



A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Calculations
3. Results
3.1. Reliability of Observations
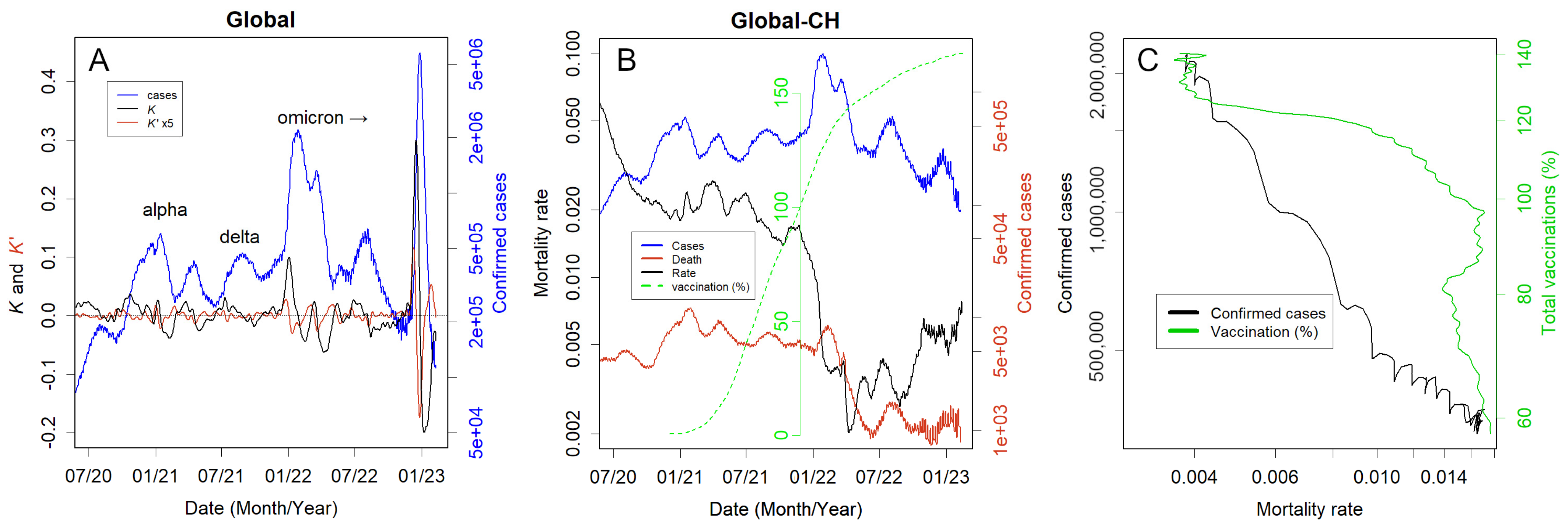
3.2. Global Data as an Example
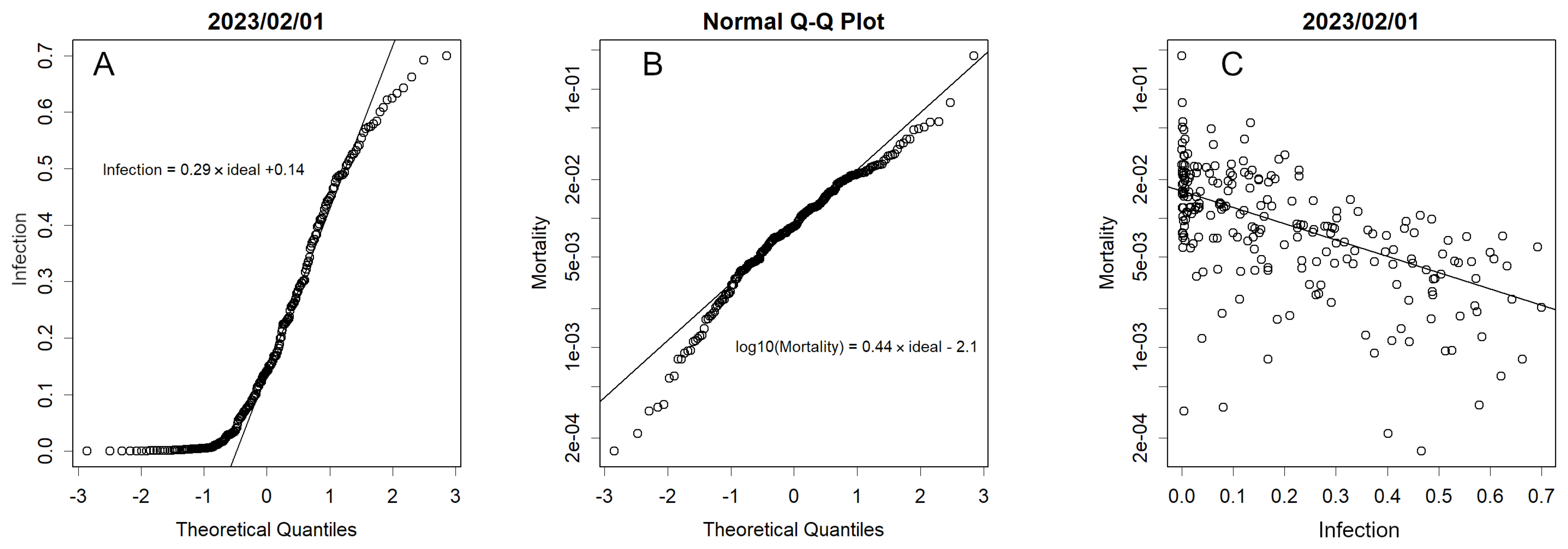
3.3. Statistical Nature of the Data
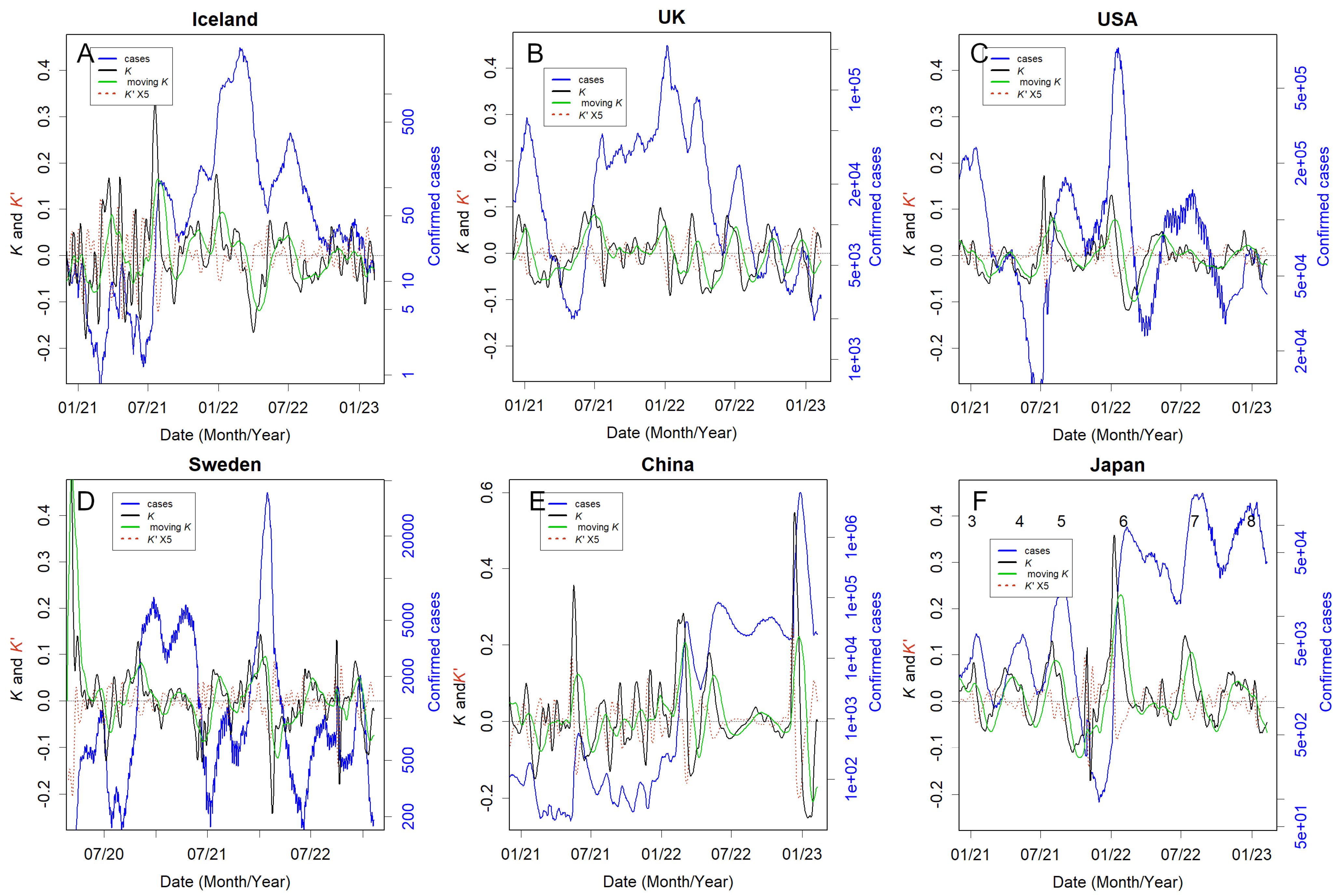
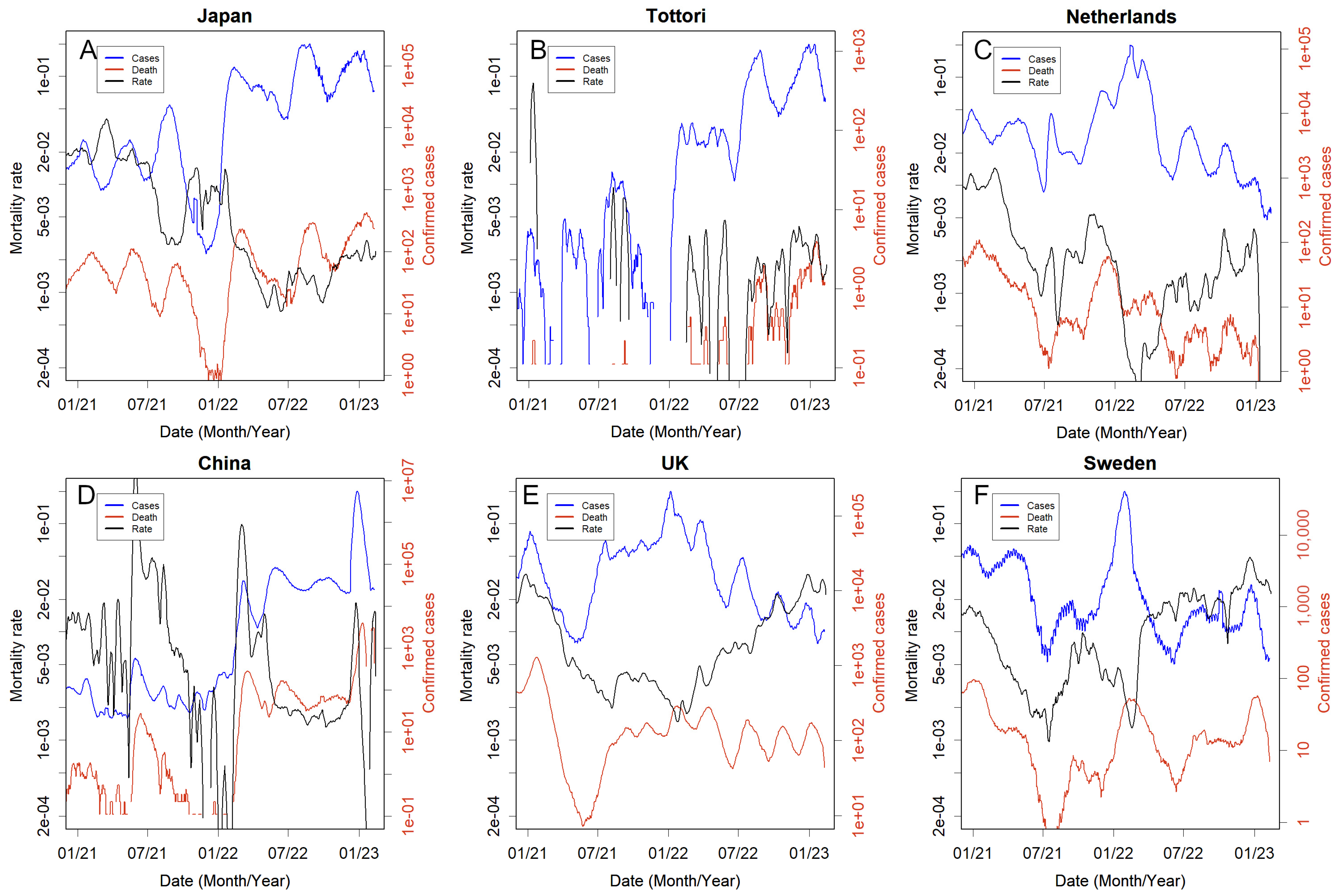
3.4. Country Responses
3.5. Countries That Took the Necessary Measures
3.6. Countries That Could Not Take the Necessary Measures or Made No Attempt to Do So
3.7. People Defended Themselves without Recourse to the Country
3.8. Countries That Relied Too Heavily on Lockdowns
3.9. Countries Where Nothing Could Be Done
3.10. What Difference Do the Policies Make?
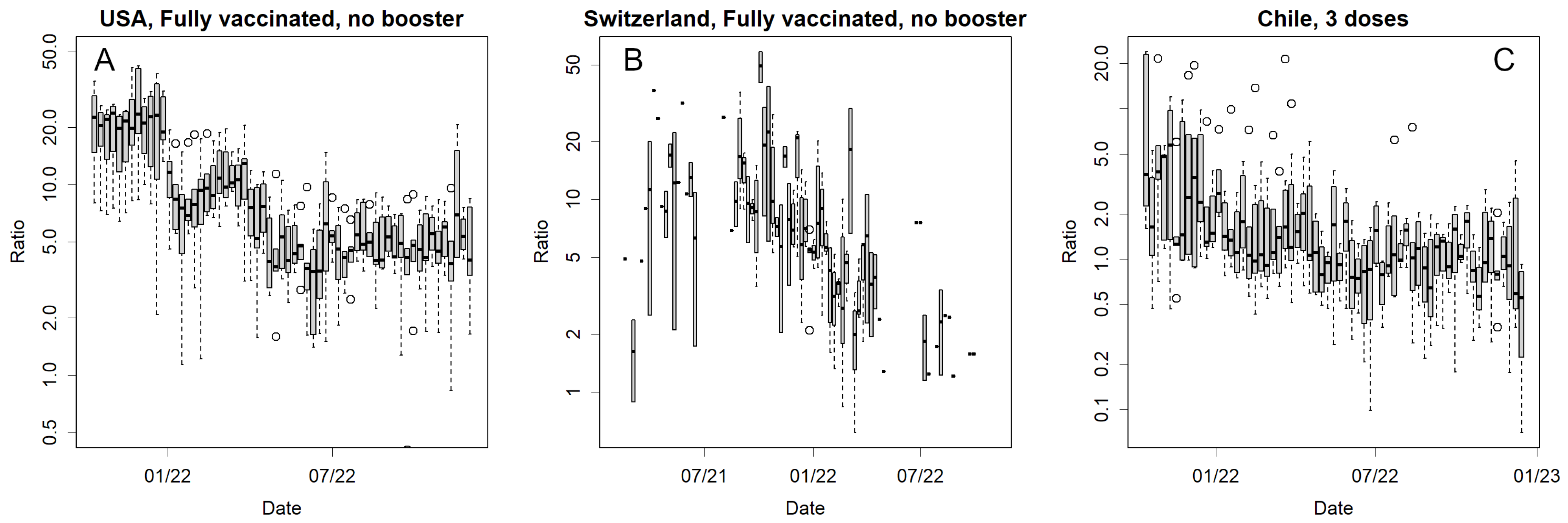
3.11. Vaccine Effectiveness on Mortality
3.12. Convergence of the Epidemics
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
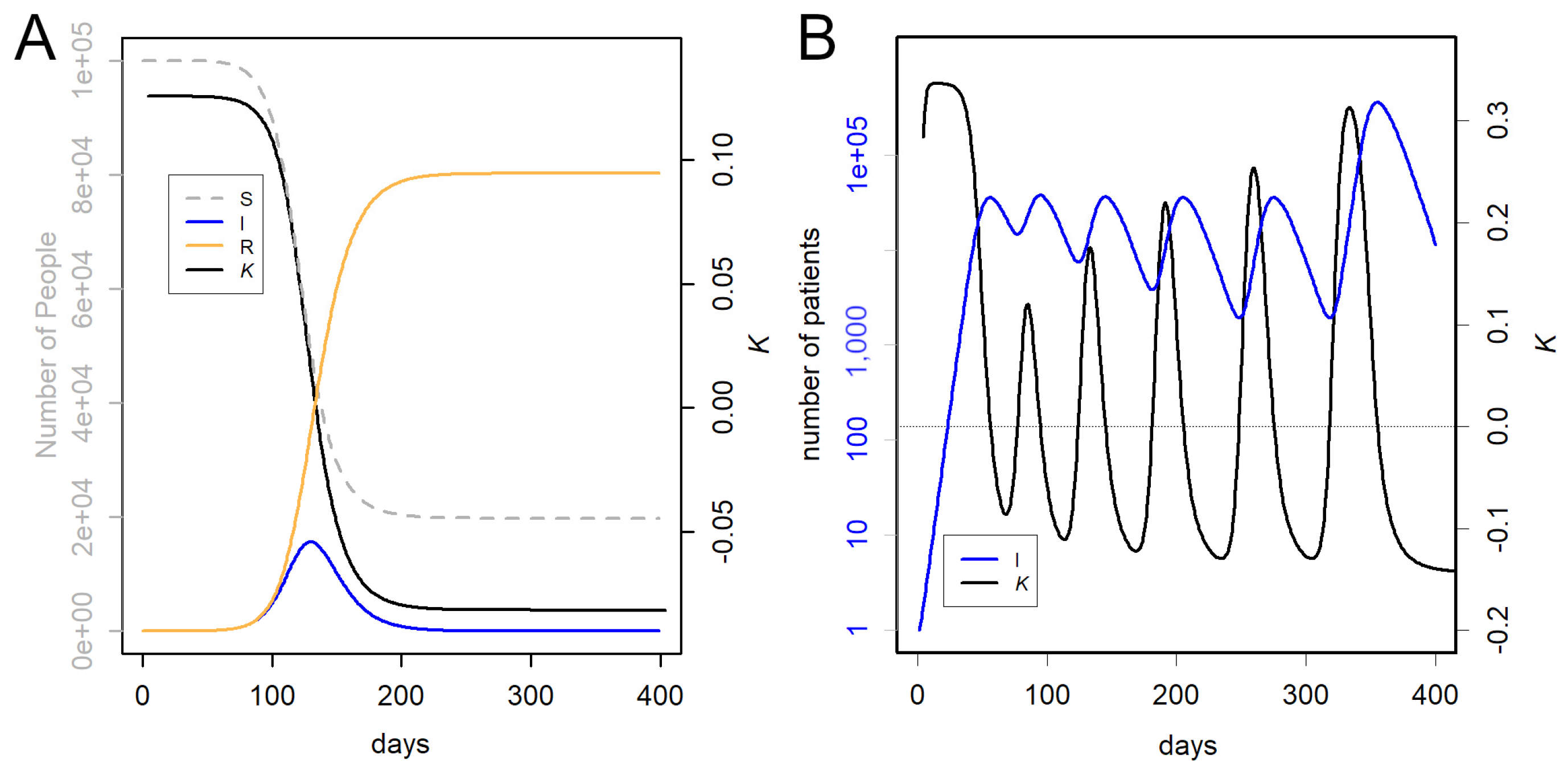
Appendix A. The Character of K

Appendix B. Statistical Tests
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/data (accessed on 22 September 2023).
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Bach, K. New Data Shows Long COVID Is Keeping as Many as 4 Million People out of Work. Brookings. Available online: https://www.brookings.edu/research/new-data-shows-long-covid-is-keeping-as-many-as-4-million-people-out-of-work/ (accessed on 22 September 2023).
- Belluck, P. Long COVID Is Keeping Significant Numbers of People out of Work, Study Finds. New York Times. Available online: https://www.nytimes.com/2023/01/24/health/long-covid-work.html (accessed on 22 September 2023).
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef] [PubMed]
- Oxford University. COVID-19 Government Response Tracker. 2023. Available online: https://www.bsg.ox.ac.uk/research/covid-19-government-response-tracker (accessed on 22 September 2023).
- WHO. Strategic Preparedness, Readiness and Response Plan to End the Global COVID-19 Emergency in 2022. 2023. Available online: https://www.who.int/publications/i/item/WHO-WHE-SPP-2022.1 (accessed on 22 September 2023).
- European Centre for Disease Prevention and Control. Public Health Control Measures for COVID-19. 2023. Available online: https://www.ecdc.europa.eu/en/infectious-disease-topics/z-disease-list/covid-19/facts/public-health-control-measures-covid-19 (accessed on 22 September 2023).
- Amri, M.M.; Abed, S.A. The Data-Driven Future of Healthcare: A Review. Mesopotamian J. Big Data 2023, 2023, 68–74. [Google Scholar] [CrossRef]
- Lee, K.-S.; Eom, J.K. Systematic literature review on impacts of COVID-19 pandemic and corresponding measures on mobility. Transportation 2023. [Google Scholar] [CrossRef]
- Konishi, T. Effect of control measures on the pattern of COVID-19 Epidemics in Japan. PeerJ 2021, 9, e12215. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Taeihagh, A.; Tan, S.Y. A scoping review of the impacts of COVID-19 physical distancing measures on vulnerable population groups. Nat. Commun. 2023, 14, 599. [Google Scholar] [CrossRef]
- Xie, G.; Wang, L.; Zhang, J. How are countries responding differently to COVID-19: A systematic review of guidelines on isolation measures. Front. Public Health 2023, 11, 1190519. [Google Scholar] [CrossRef]
- Herby, J.; Jonung, L.; Hanke, S. A Literature Review and Meta-Analysis of the Effects of Lockdowns on COVID-19 Mortality; The Johns Hopkins Institute for Applied Economics, Global Health, and the Study of Business Enterprise. January 2022. Available online: https://ideas.repec.org/p/ris/jhisae/0200.html (accessed on 22 September 2023).
- Hale, E. How Taiwan Used Simple Tech to Help Contain COVID-19. BBC. Available online: https://www.bbc.com/news/business-60461732 (accessed on 22 September 2023).
- Kolbert, E. How Iceland Beat the Coronavirus. The New Yorker. Available online: https://www.newyorker.com/magazine/2020/06/08/how-iceland-beat-the-coronavirus (accessed on 22 September 2023).
- Mackenzie, J. How Iceland Clamped down to Conquer Coronavirus. BBC. Available online: https://www.bbc.com/news/world-europe-56412790 (accessed on 22 September 2023).
- Aljazeera. WHO Says China’s Zero-COVID Strategy Unsustainable. Available online: https://www.aljazeera.com/news/2022/5/10/who-says-chinas-zero-covid-strategy-unsustainable (accessed on 22 September 2023).
- Cowling, B. The impact of ending ‘zero COVID’ in China. Nat. Med. 2023, 29, 302. [Google Scholar] [CrossRef]
- Deutsche Welle. Coronavirus: New Zealand Abandons ‘Zero-COVID’ Strategy. Available online: https://www.dw.com/en/coronavirus-digest-new-zealand-drops-zero-covid-strategy/a-59396717 (accessed on 22 September 2023).
- BBC. Why Has Australia Switched Tack on COVID Zero? Available online: https://www.bbc.com/news/world-australia-58406526 (accessed on 22 September 2023).
- Frans, E. Did Sweden’s Controversial COVID Strategy Pay off? In Many Ways It Did—But It Let the Elderly down. The Conversation. Available online: https://theconversation.com/did-swedens-controversial-covid-strategy-pay-off-in-many-ways-it-did-but-it-let-the-elderly-down-188338 (accessed on 22 September 2023).
- Sobczak, M.; Pawliczak, R. Factors That Affect the COVID-19 Pandemic in Summer 2022 Compared to Summer 2021. Int. J. Environ. Res. Public Health 2022, 19, 12561. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef]
- Khazaei, Y.; Küchenhoff, H.; Hoffmann, S.; Syliqi, D.; Rehms, R. Using a Bayesian hierarchical approach to study the association between non-pharmaceutical interventions and the spread of COVID-19 in Germany. Sci. Rep. 2023, 13, 18900. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, A.; Speich, B.; Mentré, F.; Rueegg, C.S.; Belhadi, D.; Assoumou, L.; Burdet, C.; Murthy, S.; Dodd, L.E.; Wang, Y.; et al. Effects of remdesivir in patients hospitalised with COVID-19: A systematic review and individual patient data meta-analysis of randomised controlled trials. Lancet Respir. Med. 2023, 11, 453–464. [Google Scholar] [CrossRef]
- Külper-Schiek, W.; Piechotta, V.; Pilic, A.; Batke, M.; Dreveton, L.S.; Geurts, B.; Koch, J.; Köppe, S.; Treskova, M.; Vygen-Bonnet, S.; et al. Facing the Omicron variant-how well do vaccines protect against mild and severe COVID-19? Third interim analysis of a living systematic review. Front. Immunol. 2022, 13, 940562. [Google Scholar] [CrossRef]
- Kissler, S.M.; Fauver, J.R.; Mack, C.; Tai, C.G.; Breban, M.I.; Watkins, A.E.; Samant, R.M.; Anderson, D.J.; Metti, J.; Khullar, G.; et al. Viral Dynamics of SARS-CoV-2 Variants in Vaccinated and Unvaccinated Persons. N. Engl. J. Med. 2021, 385, 2489–2491. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, A. Omicron Variant Could be an Antigenic Shift of SARS-CoV-2. Qeios 2023. [Google Scholar] [CrossRef]
- Azim Majumder, M.A.; Razzaque, M.S. Repeated vaccination and ‘vaccine exhaustion’: Relevance to the COVID-19 crisis. Expert Rev. Vaccines 2022, 21, 1011–1014. [Google Scholar] [CrossRef]
- Gao, F.X.; Wu, R.X.; Shen, M.Y.; Huang, J.J.; Li, T.T.; Hu, C.; Luo, F.Y.; Song, S.Y.; Mu, S.; Hao, Y.N.; et al. Extended SARS-CoV-2 RBD booster vaccination induces humoral and cellular immune tolerance in mice. iScience 2022, 25, 105479. [Google Scholar] [CrossRef]
- Irrgang, P.; Gerling, J.; Kocher, K.; Lapuente, D.; Steininger, P.; Habenicht, K.; Wytopil, M.; Beileke, S.; Schäfer, S.; Zhong, J.; et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci. Immunol. 2023, 8, eade2798. [Google Scholar] [CrossRef]
- Kiszel, P.; Sík, P.; Miklós, J.; Kajdácsi, E.; Sinkovits, G.; Cervenak, L.; Prohászka, Z. Class switch towards spike protein-specific IgG4 antibodies after SARS-CoV-2 mRNA vaccination depends on prior infection history. Sci. Rep. 2023, 13, 13166. [Google Scholar] [CrossRef]
- Uversky, V.N.; Redwan, E.M.; Makis, W.; Rubio-Casillas, A. IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein. Vaccines 2023, 11, 991. [Google Scholar] [CrossRef] [PubMed]
- Konishi, T. COVID-19 Epidemics Monitored Through the Logarithmic Growth Rate and SIR Model. J. Clin. Immunol. Microbiol. 2022, 3, 1–45. [Google Scholar] [CrossRef]
- Konishi, T. Progressing adaptation of SARS-CoV-2 to humans. Chem-Bio Inform. J. 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Konishi, T. Continuous mutation of SARS-CoV-2 during migration via three routes at the beginning of the pandemic. PeerJ 2022, 10, e12681. [Google Scholar] [CrossRef] [PubMed]
- Konishi, T. SARS-CoV-2 mutations among minks show reduced lethality and infectivity to humans. PLoS ONE 2021, 16, e0247626. [Google Scholar] [CrossRef] [PubMed]
- Konishi, T. Mutations in SARS-CoV-2 are on the increase against the acquired immunity. PLoS ONE 2022, 17, e0271305. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan. New Corona Vaccination Results. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/vaccine_sesshujisseki.html (accessed on 22 September 2023).
- Our World in Data. How Do Death Rates from COVID-19 Differ between People Who Are Vaccinated and Those Who Are Not? Available online: https://ourworldindata.org/covid-deaths-by-vaccination (accessed on 22 September 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://cran.r-project.org/ (accessed on 22 September 2023).
- Qasmieh, S.A.; Robertson, M.M.; Teasdale, C.A.; Kulkarni, S.G.; Jones, H.E.; McNairy, M.; Borrell, L.N.; Nash, D. The prevalence of SARS-CoV-2 infection and long COVID in US adults during the BA.4/BA.5 surge. June–July 2022. Prev. Med. 2023, 169, 107461. [Google Scholar] [CrossRef]
- Park, S.; Marcus, G.M.; Olgin, J.E.; Carton, T.; Hamad, R.; Pletcher, M.J.; Consortium, C.-C.S.S. Unreported SARS-CoV-2 Home Testing and Test Positivity. JAMA Netw. Open 2023, 6, e2252684. [Google Scholar] [CrossRef]
- Stowe, J.; Andrews, N.; Kirsebom, F.; Ramsay, M.; Bernal, J.L. Effectiveness of COVID-19 vaccines against Omicron and Delta hospitalisation, a test negative case-control study. Nat. Commun. 2022, 13, 5736. [Google Scholar] [CrossRef]
- Kuhlmann, C.; Mayer, C.K.; Claassen, M.; Maponga, T.; Burgers, W.A.; Keeton, R.; Riou, C.; Sutherland, A.D.; Suliman, T.; Shaw, M.L.; et al. Breakthrough infections with SARS-CoV-2 omicron despite mRNA vaccine booster dose. Lancet 2022, 399, 625–626. [Google Scholar] [CrossRef]
- Staff, T. Israeli Trial, World’s First, Finds 4th Dose ‘Not Good Enough’ against Omicron. The Times of Israel. Available online: https://www.timesofisrael.com/israeli-trial-worlds-first-finds-4th-dose-not-good-enough-against-omicron/ (accessed on 22 September 2023).
- Centers for Disease Control and Prevention; U.S. Department of Health and Human Services. Transmission-Based Precautions. Available online: https://www.cdc.gov/infectioncontrol/basics/transmission-based-precautions.html (accessed on 22 September 2023).
- Chu, V.T.; Schwartz, N.G.; Donnelly, M.A.P.; Chuey, M.R.; Soto, R.; Yousaf, A.R.; Schmitt-Matzen, E.N.; Sleweon, S.; Ruffin, J.; Thornburg, N.; et al. Comparison of Home Antigen Testing with RT-PCR and Viral Culture During the Course of SARS-CoV-2 Infection. JAMA Intern. Med. 2022, 182, 701–709. [Google Scholar] [CrossRef]
- Wakita, M.; Idei, M.; Saito, K.; Horiuchi, Y.; Yamatani, K.; Ishikawa, S.; Yamamoto, T.; Igawa, G.; Hinata, M.; Kadota, K.; et al. Comparison of the clinical performance and usefulness of five SARS-CoV-2 antibody tests. PLoS ONE 2021, 16, e0246536. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Okazaki, K.; Kitai, Y.; Shinohara, K.; Yukawa, S.; Noguchi, T.; Tanaka, M.; Matsumura, Y.; Nishiyama, Y.; Nagao, M. Comparison of six antibody assays and two combination assays for COVID-19. Virol. J. 2022, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Corona Virus Resource Center; Johns Hopkins University & Medicine. Taiwan. Available online: https://coronavirus.jhu.edu/region/taiwan (accessed on 22 September 2023).
- Parker, C.F.; Stern, E.K. The Trump Administration and the COVID-19 crisis: Exploring the warning-response problems and missed opportunities of a public health emergency. Public Adm. 2022, 100, 616–632. [Google Scholar] [CrossRef] [PubMed]
- Head, M. Boris Johnson’s Pandemic Legacy—Where He Went Wrong Managing COVID. The Conversation. (and Some Things He Got Right). Available online: https://theconversation.com/boris-johnsons-pandemic-legacy-where-he-went-wrong-managing-covid-and-some-things-he-got-right-189666 (accessed on 22 September 2023).
- Hamada, K.; Miki, I. Hotel Patients in COVID-19 Complain of a Harsh and Anxious Life under House Arrest: “If My Condition Suddenly Changes Here, I’m Afraid I Won’t Survive”. Business Insider. Available online: https://www.businessinsider.jp/post-211965 (accessed on 22 September 2023).
- Takata, N. East Japan Pref. to Pay over $50K to Family of COVID-19 Patient Found Dead after Systemic Flaw. Mainichi Shinbun. Available online: https://mainichi.jp/english/articles/20210907/p2a/00m/0na/005000c (accessed on 22 September 2023).
- Ministry of Health, Labour and Welfare, Japan. A Survey of the Actual Antibody Retention Rate of Novel Coronavirus Using Residual Blood Samples for Testing at the Time of Blood Donation. Available online: https://www.mhlw.go.jp/content/10906000/001070846.pdf (accessed on 22 September 2023).
- CNBC. China Says COVID Outbreak Has Infected 80% of Population. Available online: https://www.cnbc.com/2023/01/21/china-says-covid-outbreak-has-infected-80percent-of-population.html (accessed on 22 September 2023).
- Yong, N. China COVID: More Than 88 Million People in Henan Infected, Official Says. BBC. Available online: https://www.bbc.com/news/world-asia-china-64208127 (accessed on 22 September 2023).
- The Guardian. 90% of People in China Province Infected with COVID, Says Local Health Official. Available online: https://www.theguardian.com/world/2023/jan/09/life-is-moving-forward-china-enters-new-phase-in-covid-fight-as-borders-open (accessed on 22 September 2023).
- NHK. COVID-19: What Will Change with the All-Knowing Review? Available online: https://www.nhk.or.jp/shutoken/newsup/20220825b.html (accessed on 1 December 2023).
- Murata, T. High Death Toll in 8th Wave “Caused by More Infections Than Reported” Volunteer Expert Analysis. Mainichi shimbun. Available online: https://mainichi.jp/articles/20230222/k00/00m/040/380000c (accessed on 22 September 2023).
- Ministry of Health, Labour and Welfare, Japan. Preliminary Vital Statistics. January 2023. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/s2023/dl/202301.pdf (accessed on 22 September 2023).
- Yomiuri Shinbun. Corona Deaths Somehow the Most in Osaka, 3 Factors Compared to Tokyo… Prefectures Continue to Be at the Mercy of Mutant Stocks. Available online: https://www.yomiuri.co.jp/national/20220904-OYT1T50064/ (accessed on 22 September 2023).
- J-Cast News. Australia Amassed Nearly 20,000 More Deaths Last Year Than Expected, and Experts Say COVID-19 Is Largely to Blame. Available online: https://www.1news.co.nz/2023/03/06/experts-blame-covid-after-nearly-20000-extra-australian-deaths/ (accessed on 1 December 2023).
- The Guardian. COVID Temporarily Reduced Australia’s Average Life Expectancy and Lifted Death Rates to Historic Highs. Available online: https://www.theguardian.com/australia-news/2023/jan/06/covid-reduced-australias-average-life-expectancy-and-lifted-death-rates-to-historic-highs (accessed on 22 September 2023).
- Pandemic. Excess Severity in Australia and New Zealand. Available online: https://pandem-ic.com/excess-severity-in-australia-and-new-zealand/ (accessed on 22 September 2023).
- Clark-Dow, E. Deaths in New Zealand up by 10% in 2022, Impacted by COVID-19. Available online: https://www.stuff.co.nz/national/health/300811491/deaths-in-new-zealand-up-by-10-in-2022-impacted-by-covid19 (accessed on 22 September 2023).
- Ministry of Health, Labour and Welfare, Japan. Number of Positive Cases and Deaths from Novel Coronavirus Infection by Age Group—Also Examining Vaccination by Age Group. July 2021. Available online: https://www.mhlw.go.jp/content/10900000/000826597.pdf (accessed on 22 September 2023).
- Konishi, T. Re-Evaluation of the Evolution of Influenza H1 Viruses Using Direct PCA. Sci. Rep. 2019, 9, 19287. [Google Scholar] [CrossRef]
- Deng, J.; Ma, Y.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3335. [Google Scholar] [CrossRef]
- Human Right Watch. China: Free ‘White Paper’ Protesters. Available online: https://www.hrw.org/news/2023/01/26/china-free-white-paper-protesters (accessed on 22 September 2023).
- Chaudhary, N.; Weissman, D.; Whitehead, K.A. mRNA vaccines for infectious diseases: Principles, delivery and clinical translation. Nat. Rev. Drug Discov. 2021, 20, 817–838. [Google Scholar] [CrossRef]
- Payne, J.R.; Bose, S.; Kubiak, R.W.; Nolen, L.D. Evaluation of mortality risk after COVID-19 vaccination, Utah 2021. Vaccine 2023, 41, 2996–3002. [Google Scholar] [CrossRef]
- WHO. Interim Statement on COVID-19 Vaccines in the Context of the Circulation of the Omicron SARS-CoV-2 Variant from the WHO Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC). 2022. Available online: https://www.who.int/news/item/11-01-2022-interim-statement-on-covid-19-vaccines-in-the-context-of-the-circulation-of-the-omicron-sars-cov-2-variant-from-the-who-technical-advisory-group-on-covid-19-vaccine-composition (accessed on 22 September 2023).
- Wisnivesky, J.P.; Govindarajulu, U.; Bagiella, E.; Goswami, R.; Kale, M.; Campbell, K.N.; Meliambro, K.; Chen, Z.; Aberg, J.A.; Lin, J.J. Association of Vaccination with the Persistence of Post-COVID Symptoms. J. Gen. Intern. Med. 2022, 37, 1748–1753. [Google Scholar] [CrossRef]
- Reardon, S. Long COVID risk falls only slightly after vaccination, huge study shows. Nature 2022. Available online: https://www.nature.com/articles/d41586-022-01453-0 (accessed on 22 September 2023). [CrossRef]
- Roberts, H.A.; Clark, D.A.; Kalina, C.; Sherman, C.; Brislin, S.; Heitzeg, M.M.; Hicks, B.M. To vax or not to vax: Predictors of anti-vax attitudes and COVID-19 vaccine hesitancy prior to widespread vaccine availability. PLoS ONE 2022, 17, e0264019. [Google Scholar] [CrossRef] [PubMed]
- Jonson, A.G.; Linde, L.; Ali, A.R.; DeSantis, A.; Shi, M.; Adam, C.; Armstrong, B.; Armstrong, B.; Asbell, M.; Auche, S.; et al. COVID-19 Incidence and Mortality Among Unvaccinated and Vaccinated Persons Aged ≥ 12 Years by Receipt of Bivalent Booster Doses and Time Since Vaccination. MMWR Cent. Dis. Control. Prev. 2023, 72, 145–152. [Google Scholar] [CrossRef]
- Hotez, P.J. Will anti-vaccine activism in the USA reverse global goals? Nat. Rev. Immunol. 2022, 22, 525–526. [Google Scholar] [CrossRef] [PubMed]
- Nikkei Shinbun. Corona Vaccinations for the Elderly to Begin in May, Ministry of Health, Labor, and Welfare Japan. Available online: https://www.nikkei.com/article/DGXZQOUA221560S3A220C2000000/ (accessed on 22 September 2023).
- NHK. Why? New COVID-19 Vaccines Expired and Discarded One after Another. Available online: https://www3.nhk.or.jp/news/html/20220428/k10013603311000.html (accessed on 22 September 2023).
- Nikkei Shinbun. Corona Reserve Fund of 12 Trillion Yen, 90% of the Use of Which Cannot Be Tracked. Transparency Is an Issue. Available online: https://www.nikkei.com/article/DGXZQOUA143WV0U2A410C2000000/ (accessed on 22 September 2023).
- J-Cast News. Corona Budget of 16 Trillion Yen Is a Suspicious Destination. Huge Facilities Are Not Used, and Benefit Fraud Is Frequent. Available online: https://www.j-cast.com/trend/2022/05/31438429.html?p=all (accessed on 22 September 2023).
- Zhou, P.; Shi, Z.-L. SARS-CoV-2 spillover events. Science 2021, 371, 120–122. [Google Scholar] [CrossRef]
- Hyogo Medical Practitioners Association. The State’s New COVID-19 Response Filled with Scientific Neglect. Available online: http://www.hhk.jp/hyogo-hokeni-shinbun/backnumber/2022/1015/100002.php (accessed on 22 September 2023).
- Fraiman, J.; Erviti, J.; Jones, M.; Greenland, S.; Whelan, P.; Kaplan, R.M.; Doshi, P. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine 2022, 40, 5798–5805. [Google Scholar] [CrossRef]
- Imai, M.; Watanabe, T.; Hatta, M.; Das, S.C.; Ozawa, M.; Shinya, K.; Zhong, G.; Hanson, A.; Katsura, H.; Watanabe, S.; et al. Experimental adaptation of an influenza H5 HA confers respiratory droplet transmission to a reassortant H5 HA/H1N1 virus in ferrets. Nature 2012, 486, 420–428. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med. 2022, 28, 2398–2405. [Google Scholar] [CrossRef]
- Normandin, E.; Rudy, M.; Barkas, N.; Schaffner, S.F.; Levine, Z.; Padera, R.F.; Babadi, M.; Mukerji, S.S.; Park, D.J.; MacInnis, B.L.; et al. High-depth sequencing characterization of viral dynamics across tissues in fatal COVID-19 reveals compartmentalized infection. Nat. Commun. 2023, 14, 574. [Google Scholar] [CrossRef]
- Sumi, T.; Harada, K. Immune response to SARS-CoV-2 in severe disease and long COVID-19. iScience 2022, 25, 104723. [Google Scholar] [CrossRef]
- Tokyo Shinbun. The Division over Masks? The Government Says It’s a Personal Decision… But Can It Be Removed in Japan, a Society of Peer Pressure? Available online: https://www.tokyo-np.co.jp/article/228322 (accessed on 22 September 2023).
- TBS. Behind Prime Minister Kishida’s Decision to “No Masks by G7”. Available online: https://newsdig.tbs.co.jp/articles/-/299633?display=1 (accessed on 22 September 2023).
- Ministry of Health, Labour and Welfare, Japan. Wearing a Mask Is Based on Personal Discretion. Available online: https://www.mhlw.go.jp/content/001056979.pdf (accessed on 22 September 2023).
- Mainichi Shinbun. Death Toll to Be Announced in 2 Months at the Earliest, MHLW Due to Transition of COVID-19 to Category 5. Available online: https://mainichi.jp/articles/20230326/ddm/001/040/122000c (accessed on 22 September 2023).
- Ollila, H.; Partinen, M.; Koskela, J.; Borghi, J.; Savolainen, R.; Rotkirch, A.; Laine, L.T. Face masks to prevent transmission of respiratory infections: Systematic review and meta-analysis of randomized controlled trials on face mask use. PLoS ONE 2022, 17, e0271517. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; Westhuizen, H.-M.V.D.; Delft, A.V.; Price, A.; Fridman, L.; Tang, L.H.; et al. An evidence review of face masks against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yuan, K.; Sun, Y.-K.; Zheng, Y.-B.; Xu, Y.-Y.; Su, S.-Z.; Zhang, Y.-X.; Zhong, Y.; Wang, Y.-J.; Tian, S.-S.; et al. Efficacy and practice of facemask use in general population: A systematic review and meta-analysis. Transl. Psychiatry 2022, 12, 49. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konishi, T. A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate. COVID 2024, 4, 130-150. https://doi.org/10.3390/covid4020012
Konishi T. A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate. COVID. 2024; 4(2):130-150. https://doi.org/10.3390/covid4020012
Chicago/Turabian StyleKonishi, Tomokazu. 2024. "A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate" COVID 4, no. 2: 130-150. https://doi.org/10.3390/covid4020012
APA StyleKonishi, T. (2024). A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate. COVID, 4(2), 130-150. https://doi.org/10.3390/covid4020012