

The Renal Manifestations of SARS-CoV-2: A Guide for Family Physicians


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Chronic Kidney Disease and COVID-19
3.2. Adult COVID-19 Patients with Acute Kidney Injury (AKI)
3.3. Adult Kidney Transplant Recipients
3.4. Glomerulonephritis in COVID-19 Patients
3.5. Pediatric COVID-19
3.6. Multisystem-Inflammatory Syndrome in Children (MIS-C) and AKI
3.7. Renal Histopathology and COVID-19
3.8. Geriatric Patients and AKI
3.9. Race and Risk of AKI
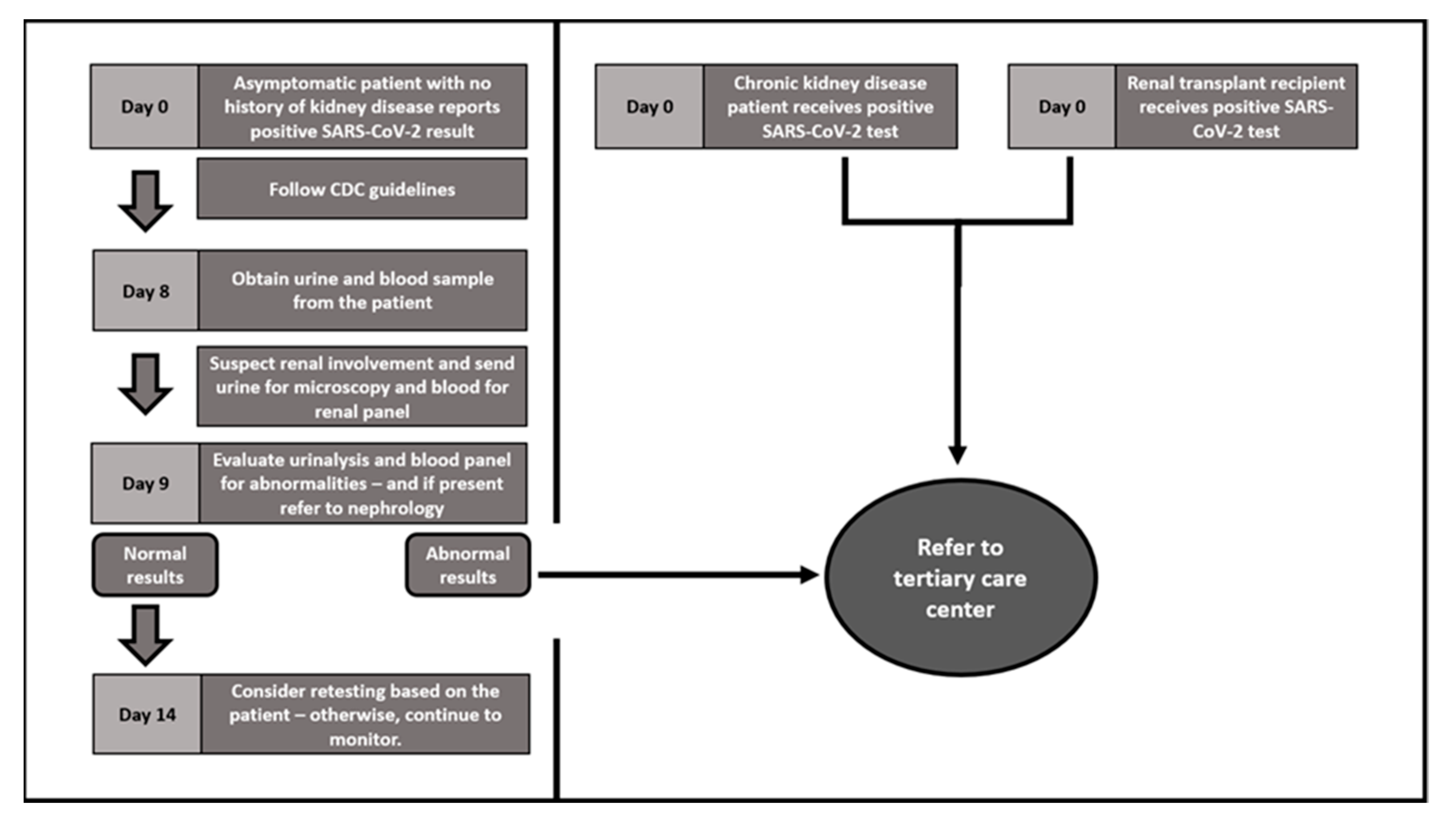
4. Triaging and Monitoring Suspected Renal Involvement
4.1. Management
4.2. Renal Function Monitoring
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.-C.; Kuo, R.-L.; Shih, S.-R. COVID-19: The First Documented Coronavirus Pandemic in History. Biomed. J. 2020, 43, 328–333. [Google Scholar] [CrossRef]
- CDC COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 9 December 2022).
- New COVID-19 Cases Worldwide. Available online: https://coronavirus.jhu.edu/data/new-cases (accessed on 21 December 2022).
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry Indicate a High Mortality Due to COVID-19 in Dialysis Patients and Kidney Transplant Recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cryer, M.J.; Farhan, S.; Kaufmann, C.C.; Jäger, B.; Garg, A.; Krishnan, P.; Mehran, R.; Huber, K. Prothrombotic Milieu, Thrombotic Events and Prophylactic Anticoagulation in Hospitalized COVID-19 Positive Patients: A Review. Clin. Appl. Thromb Hemost 2022, 28, 10760296221074352. [Google Scholar] [CrossRef]
- Li, Z.; Wu, M.; Yao, J.; Guo, J.; Liao, X.; Song, S.; Li, J.; Duan, G.; Zhou, Y.; Wu, X.; et al. Caution on Kidney Dysfunctions of COVID-19 Patients. MedRxiv 2020, 25. [Google Scholar] [CrossRef]
- Estimated COVID-19 Burden|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html (accessed on 6 April 2022).
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D. Acute Kidney Injury in Patients Hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Flythe, J.E.; Assimon, M.M.; Tugman, M.J.; Chang, E.H.; Gupta, S.; Shah, J.; Sosa, M.A.; Renaghan, A.D.; Melamed, M.L.; Wilson, F.P.; et al. Characteristics and Outcomes of Individuals With Pre-Existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States. Am. J. Kidney Dis. 2021, 77, 190–203. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. JASN 2021, 32, 151–160. [Google Scholar] [CrossRef]
- Fisher, M.; Neugarten, J.; Bellin, E.; Yunes, M.; Stahl, L.; Johns, T.S.; Abramowitz, M.K.; Levy, R.; Kumar, N.; Mokrzycki, M.H.; et al. AKI in Hospitalized Patients with and without COVID-19: A Comparison Study. JASN 2020, 31, 2145–2157. [Google Scholar] [CrossRef] [PubMed]
- Akilesh, S.; Nast, C.C.; Yamashita, M.; Henriksen, K.; Charu, V.; Troxell, M.L.; Kambham, N.; Bracamonte, E.; Houghton, D.; Ahmed, N.I.; et al. Multicenter Clinicopathologic Correlation of Kidney Biopsies Performed in COVID-19 Patients Presenting With Acute Kidney Injury or Proteinuria. Am. J. Kidney Dis. 2021, 77, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Shetty, A.A.; Tawhari, I.; Safar-Boueri, L.; Seif, N.; Alahmadi, A.; Gargiulo, R.; Aggarwal, V.; Usman, I.; Kisselev, S.; Gharavi, A.G.; et al. COVID-19–Associated Glomerular Disease. JASN 2021, 32, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Ilori, T.O.; Holick, M.F.; Hochberg, N.S.; Apovian, C.M. Self-Identified Race and COVID-19-Associated Acute Kidney Injury and Inflammation: A Retrospective Cohort Study of Hospitalized Inner-City COVID-19 Patients. J. Gen. Intern. Med. 2021, 36, 3487–3496. [Google Scholar] [CrossRef]
- Stewart, D.J.; Hartley, J.C.; Johnson, M.; Marks, S.D.; du Pré, P.; Stojanovic, J. Renal Dysfunction in Hospitalised Children with COVID-19. Lancet Child. Adolesc. Health 2020, 4, e28–e29. [Google Scholar] [CrossRef]
- Gonzalez Jimenez, D.; Velasco Rodríguez-Belvís, M.; Ferrer Gonzalez, P.; Domínguez Ortega, G.; Segarra, O.; Medina Benitez, E.; Garcia Tirado, D.; Garcia Romero, R.; Vecino López, R.; Crehuá-Gaudiza, E.; et al. COVID-19 Gastrointestinal Manifestations Are Independent Predictors of PICU Admission in Hospitalized Pediatric Patients. Pediatr. Infect. Dis. J. 2020, 39, e459–e462. [Google Scholar] [CrossRef] [PubMed]
- Basalely, A.; Gurusinghe, S.; Schneider, J.; Shah, S.S.; Siegel, L.B.; Pollack, G.; Singer, P.; Castellanos-Reyes, L.J.; Fishbane, S.; Jhaveri, K.D.; et al. Acute Kidney Injury in Pediatric Patients Hospitalized with Acute COVID-19 and Multisystem Inflammatory Syndrome in Children Associated with COVID-19. Kidney Int. 2021, 100, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.; Chakraborty, R.; Mawby, I.; Agarwal, N.; Sethi, S.; Forbes, M. Critical Analysis of Acute Kidney Injury in Pediatric COVID-19 Patients in the Intensive Care Unit. Pediatr. Nephrol. 2021, 36, 2627–2638. [Google Scholar] [CrossRef]
- Xu, H.; Garcia-Ptacek, S.; Annetorp, M.; Bruchfeld, A.; Cederholm, T.; Johnson, P.; Kivipelto, M.; Metzner, C.; Religa, D.; Eriksdotter, M. Acute Kidney Injury and Mortality Risk in Older Adults with COVID-19. J. Nephrol. 2021, 34, 295–304. [Google Scholar] [CrossRef]
- Yuasa, B.K.; Magalhães, L.E.; Oliveira, P.G.S.d.; Yokota, L.G.; Cardoso, P.A.; Zamoner, W.; Balbi, A.L.; Ponce, D. Acute Kidney Injury in Elderly Patients With Coronavirus Infectious Disease: A Study of Incidence, Risk Factors, and Prognosis in Brazil. Front. Nephrol. 2022, 2. [Google Scholar] [CrossRef]
- Elias, M.; Pievani, D.; Randoux, C.; Louis, K.; Denis, B.; Delion, A.; Le Goff, O.; Antoine, C.; Greze, C.; Pillebout, E.; et al. COVID-19 Infection in Kidney Transplant Recipients: Disease Incidence and Clinical Outcomes. J. Am. Soc. Nephrol. 2020, 31, 2413–2423. [Google Scholar] [CrossRef]
- Mohan, S.; King, K.L.; Husain, S.A.; Schold, J.D. COVID-19–Associated Mortality among Kidney Transplant Recipients and Candidates in the United States. CJASN 2021, 16, 1695–1703. [Google Scholar] [CrossRef]
- Monfared, A.; Akhondzadeh, L.; Mousazadeh, M.; Jafari, A.; Khosravi, M.; Lebadi, M.; Aghajanzadeh, P.; Haghdar-Saheli, Y.; Movassaghi, A.; Ramezanzadeh, E.; et al. COVID-19 in Renal Transplant Recipients and General Population: A Comparative Study of Clinical, Laboratory, and Radiological Features, Severity, and Outcome. Virol. J. 2021, 18, 243. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update 2022. Kidney Int. Suppl. (2011) 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.E.; Benn, E.K.T.; Astha, V.; Okhawere, K.E.; Korn, T.G.; Nkemdirim, W.; Rambhia, A.; Ige, O.A.; Funchess, H.; Mihalopoulos, M.; et al. Association between Chronic Kidney Disease and COVID-19-Related Mortality in New York. World J. Urol. 2021, 39, 2987–2993. [Google Scholar] [CrossRef] [PubMed]
- Jdiaa, S.S.; Mansour, R.; El Alayli, A.; Gautam, A.; Thomas, P.; Mustafa, R.A. COVID-19 and Chronic Kidney Disease: An Updated Overview of Reviews. J. Nephrol. 2022, 35, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute Kidney Injury and Chronic Kidney Disease as Interconnected Syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Braun, F.; Lütgehetmann, M.; Pfefferle, S.; Wong, M.N.; Carsten, A.; Lindenmeyer, M.T.; Nörz, D.; Heinrich, F.; Meißner, K.; Wichmann, D.; et al. SARS-CoV-2 Renal Tropism Associates with Acute Kidney Injury. Lancet 2020, 396, 597–598. [Google Scholar] [CrossRef]
- Batlle, D.; Soler, M.J.; Sparks, M.A.; Hiremath, S.; South, A.M.; Welling, P.A.; Swaminathan, S.; on behalf of the COVID-19 and ACE2 in Cardiovascular, L. Acute Kidney Injury in COVID-19: Emerging Evidence of a Distinct Pathophysiology. JASN 2020, 31, 1380–1383. [Google Scholar] [CrossRef]
- Lee, S.A.; Cozzi, M.; Bush, E.L.; Rabb, H. Distant Organ Dysfunction in Acute Kidney Injury: A Review. Am. J. Kidney Dis 2018, 72, 846–856. [Google Scholar] [CrossRef]
- Klomjit, N.; Alexander, M.P.; Fervenza, F.C.; Zoghby, Z.; Garg, A.; Hogan, M.C.; Nasr, S.H.; Minshar, M.A.; Zand, L. COVID-19 Vaccination and Glomerulonephritis. Kidney Int. Rep. 2021, 6, 2969–2978. [Google Scholar] [CrossRef]
- Moore, D. COVID-19 Vaccine for Children and Adolescents|Canadian Paediatric Society. Available online: https://cps.ca/en/documents//position//covid-19-vaccine-for-children-and-adolescents/ (accessed on 13 April 2022).
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA 2021, 325, 1074–1087. [Google Scholar] [CrossRef]
- Teoh, C.W.; Gaudreault-Tremblay, M.-M.; Blydt-Hansen, T.D.; Goldberg, A.; Arora, S.; Feber, J.; Langlois, V.; Ruhl, M.; Phan, V.; Morgan, C.; et al. Management of Pediatric Kidney Transplant Patients During the COVID-19 Pandemic: Guidance From the Canadian Society of Transplantation Pediatric Group. Can. J. Kidney Health Dis. 2020, 7, 2054358120967845. [Google Scholar] [CrossRef]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; et al. COVID-19–Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef] [PubMed]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal Histopathological Analysis of 26 Postmortem Findings of Patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.A.; Markowitz, G.S.; Valeri, A.; Appel, G.B. Collapsing Glomerulopathy. Semin. Nephrol. 2003, 23, 209–218. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why Does COVID-19 Disproportionately Affect Older People? Aging (Albany NY) 2020, 12, 9959–9981. [Google Scholar] [CrossRef]
- Bowe, B.; Cai, M.; Xie, Y.; Gibson, A.K.; Maddukuri, G.; Al-Aly, Z. Acute Kidney Injury in a National Cohort of Hospitalized US Veterans with COVID-19. Clin. J. Am. Soc. Nephrol. CJASN 2020, null, null. [Google Scholar] [CrossRef] [PubMed]
- CDC Risk for COVID-19 Infection, Hospitalization, and Death By Race/Ethnicity. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 9 December 2022).
- Qeadan, F.; VanSant-Webb, E.; Tingey, B.; Rogers, T.N.; Brooks, E.; Mensah, N.A.; Winkfield, K.M.; Saeed, A.I.; English, K.; Rogers, C.R. Racial Disparities in COVID-19 Outcomes Exist despite Comparable Elixhauser Comorbidity Indices between Blacks, Hispanics, Native Americans, and Whites. Sci. Rep. 2021, 11, 8738. [Google Scholar] [CrossRef] [PubMed]
- Kabarriti, R.; Brodin, N.P.; Maron, M.I.; Guha, C.; Kalnicki, S.; Garg, M.K.; Racine, A.D. Association of Race and Ethnicity With Comorbidities and Survival Among Patients With COVID-19 at an Urban Medical Center in New York. JAMA Netw. Open 2020, 3, e2019795. [Google Scholar] [CrossRef] [PubMed]
- Wiley, Z.; Kubes, J.N.; Cobb, J.; Jacob, J.T.; Franks, N.; Plantinga, L.; Lea, J. Age, Comorbid Conditions, and Racial Disparities in COVID-19 Outcomes. J. Racial Ethn. Health Disparities 2022, 9, 117–123. [Google Scholar] [CrossRef]
- CDC Labs. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 21 December 2022).
- SARS-CoV-2 Tests, Selection and Interpretation. Available online: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/clinical-guidance/covid-19-testing-guidance/sars-cov-2-tests-selection-and-interpretation/ (accessed on 21 December 2022).
- Clinical Course|Clinical Care Considerations|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/clinical-considerations-course.html (accessed on 21 December 2022).
- CDC Healthcare Workers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/outpatient-treatment-overview.html (accessed on 21 December 2022).
- Clinical Management of Adults Summary. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management-of-adults/clinical-management-of-adults-summary/ (accessed on 21 December 2022).
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 21 December 2022).
- CDC Interim Clinical Considerations for COVID-19 Treatment in Outpatients. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/outpatient-treatment-overview.html (accessed on 21 December 2022).
- El-Khoury, J.M.; Hoenig, M.P.; Jones, G.R.D.; Lamb, E.J.; Parikh, C.R.; Tolan, N.V.; Wilson, F.P. AACC Guidance Document on Laboratory Investigation of Acute Kidney Injury. J. Appl. Lab. Med. 2021, 6, 1316–1337. [Google Scholar] [CrossRef] [PubMed]
- Chaudhri, I.; Moffitt, R.; Taub, E.; Annadi, R.R.; Hoai, M.; Bolotova, O.; Yoo, J.; Dhaliwal, S.; Sahib, H.; Daccueil, F.; et al. Association of Proteinuria and Hematuria with Acute Kidney Injury and Mortality in Hospitalized Patients with COVID-19. KBR 2020, 45, 1018–1032. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Population | Authors/Year of Publication | Study Design | Sample Size—Test Result/Site of the Study | Sex | Mean Age | Presenting Signs and Symptoms | Comorbidities | Clinical Course |
|---|---|---|---|---|---|---|---|---|
| Adult | Zhou et al. 2020 [5] | Retrospective cohort | 191 + *, MC | F38%–M62% | 56 years | Fever 94%, Cough 79% | HTN 30%, DM 19%, CVD 8%, COPD 3%, CKD 1%, Other 23% | Respiratory failure 54%, Acute cardiac injury 17%, AKI 15%, RRT 10% |
| Adult | Li et al. 2020 [7] | Retrospective cohort | 193 +, MC | F49%–M51% | 57 years | Fever 89%, Cough 69% | CVD 36%, Endocrine20%, Respiratory14%, GI 10% | ARDS 28%, AKI 28%, Acute cardiac injury 12%, RRT 7% |
| Adult | Hirsch et al. 2020 [9] | Retrospective cohort | 5449 +, MC | F39.9%–M60.1% | 64 years | N/A | HTN 55.7%, DM 33.0%, Obesity 27.1%, CVD 11% | AKI 36.6%, 90% of patients with AKI required mechanical ventilation |
| Adult | Flythe et al. 2021 [10] | Retrospective cohort | 4264 +, MC | F 46%–M54% | 65 years | Shortness of breath 69%, Cough 62%, Fever 56% | HTN 87%, DM 63%, CVD 28%, Asthma 23% | Mortality in underlying renal disease 50% |
| Adult | Chan et al. 2021 [11] | Retrospective cohort | 3993 +, SC | F43%–M57% | 64 years | N/A | HTN 38%, DM 26%, CKD 11%, CHF 13% | AKI 46%, RRT 19%, Proteinuria 84%, Hematuria 81%, Leukocytoria 60% |
| Adult | Fisher et al. 2020 [12] | Retrospective cohort | 3345 +/1265 - **, MC | F46%–M54% | 64 years | Higher respiratory and pulse rates AKI. | DM 27%, CKD 12%, Obesity 20% | AKI 56.9% |
| Adult | Akilesh et al. 2020 [13] | Case series | 17 +, MC | F50%–M50% | 54 years | N/A | N/A | ATI 82%, RRT 47% |
| Adult | Shetty et al. 2020 [14] | Case series | 6 +, SC | F50%–M50% | 56 years | Fever (66%) | N/A | N/A |
| Adult | Charoenngam et al. 2022 [15] | Retrospective cohort study | 1424 +, SC | F44%–M56% | 56 years | N/A | DM 32.3%, HTN 53%, Dyslipidemia 35% | AKI in Black patients 39.4%, in white patients 23.1% |
| Pediatric | Stewart et al. 2020 [16] | Retrospective cohort | 56 +, SC | F33%–M67% | 9 years | Fever 88%, Abdominal pain 46%, Diarrhea 73% | Underlying comorbidities 56% | AKI 35% |
| Pediatric | Gonzalez et al. 2020 [17] | Observational study | 101 +, MC | F43%–M57% | 9 years | Fever 61.86%, GI 14% | Oncologic 6%, Psychiatric 4%, Hematologic 4%, Cardiac 3% | Those with GI symptoms had higher risk of PICU admission |
| Pediatric | Basalely et al. 2021 [18] | Retrospective cohort | 152 +, MC | F49%–M51% | 8 years | GI 70%, Fever 78%, Rash 35% | Asthma 10%, Congenital heart disease 6.7%, Cancer 5% | AKI 11.8% of the entire cohort, AKI 18.2% in MIS-C cohort |
| Pediatric | Raina et al. 2022 [19] | Retrospective cohort | 2546 +, MC | F49%–M51% | 5 years | Respiratory 49%, Circulatory 33%, GI 21%, Hematologic 17.6%, Renal 11.7% | CVD 58.8%, Hematology 45.3% | AKI 10.8% |
| Geriatric | Xu et al. 2021 [20] | Retrospective cohort | 1191, + and -, MC | F57%–M43% | 83 years | N/A | HTN 40%, DM 37%, Dementia 30% | AKI 29% in +, 18% in - |
| Geriatric | Yuasa 2022 [21] | Retrospective cohort | 181 +, SC | F44%–M56% | 72 years | N/A | HTN73%, DM 45%, CVD 26%, Obesity 20.99% | AKI 56.9% |
| Kidney transplants | Elias et al. 2020 [22] | Prospective cohort | 1216, + and -, MC | F44%–M56% | 56 years | N/A | N/A | AKI 42%, RRT 7% |
| Kidney transplants | Mohan et al. 2021 [23] | Retrospective cohort | 190481 + and -, MC | F36%–M64% | 65 years | N/A | Obesity 52%, DM 69% | Mortality 16% |
| Kidney transplants | Monfared et al. 2021 [24] | Case–control | 64 +,SC | F29%–M71% | 51 years | Fever 73.9%, Cough 73.9% | HTN 87%, DM 47%, IHD 17.4% | N/A |
| Age Group | [Creatinine] mg/dl | |
|---|---|---|
| Lower (LLRI) # | Upper (ULRI) ## | |
| 0–<14 days | 0.3051 | 0.9153 |
| 14 days–<1 year | 0.1582 | 0.3842 |
| 1–<3 years | 0.1695 | 0.3503 |
| 3–<5 years | 0.2599 | 0.4181 |
| 5–<7 years | 0.2825 | 0.4746 |
| 7–<9 years | 0.3390 | 0.5424 |
| 9–<11 years | 0.3164 | 0.6641 |
| 11 years | 0.4068 | 0.7232 |
| 12 years | 0.4068 | 0.7571 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrissey, A.P.; Elzinad, N.; Hayek, C.E.; Lotfollahzadeh, S.; Chitalia, V.C. The Renal Manifestations of SARS-CoV-2: A Guide for Family Physicians. Int. J. Transl. Med. 2023, 3, 81-94. https://doi.org/10.3390/ijtm3010007
Morrissey AP, Elzinad N, Hayek CE, Lotfollahzadeh S, Chitalia VC. The Renal Manifestations of SARS-CoV-2: A Guide for Family Physicians. International Journal of Translational Medicine. 2023; 3(1):81-94. https://doi.org/10.3390/ijtm3010007
Chicago/Turabian StyleMorrissey, Austin P., Nagla Elzinad, Chris El Hayek, Saran Lotfollahzadeh, and Vipul C. Chitalia. 2023. "The Renal Manifestations of SARS-CoV-2: A Guide for Family Physicians" International Journal of Translational Medicine 3, no. 1: 81-94. https://doi.org/10.3390/ijtm3010007
APA StyleMorrissey, A. P., Elzinad, N., Hayek, C. E., Lotfollahzadeh, S., & Chitalia, V. C. (2023). The Renal Manifestations of SARS-CoV-2: A Guide for Family Physicians. International Journal of Translational Medicine, 3(1), 81-94. https://doi.org/10.3390/ijtm3010007