
Perceived Barriers and Facilitators to a Healthy Diet among Cancer Survivors: A Qualitative Exploration Using the TDF and COM-B


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Design
2.3. Participant Recruitment
2.4. Materials
2.5. Healthy Diet
2.6. Researcher Characteristics and Reflexivity
2.7. Procedure
2.8. Data Analysis
2.9. Intervention Options
3. Results
3.1. Participant Demographics
3.2. Barriers and Facilitators to a Healthy Diet
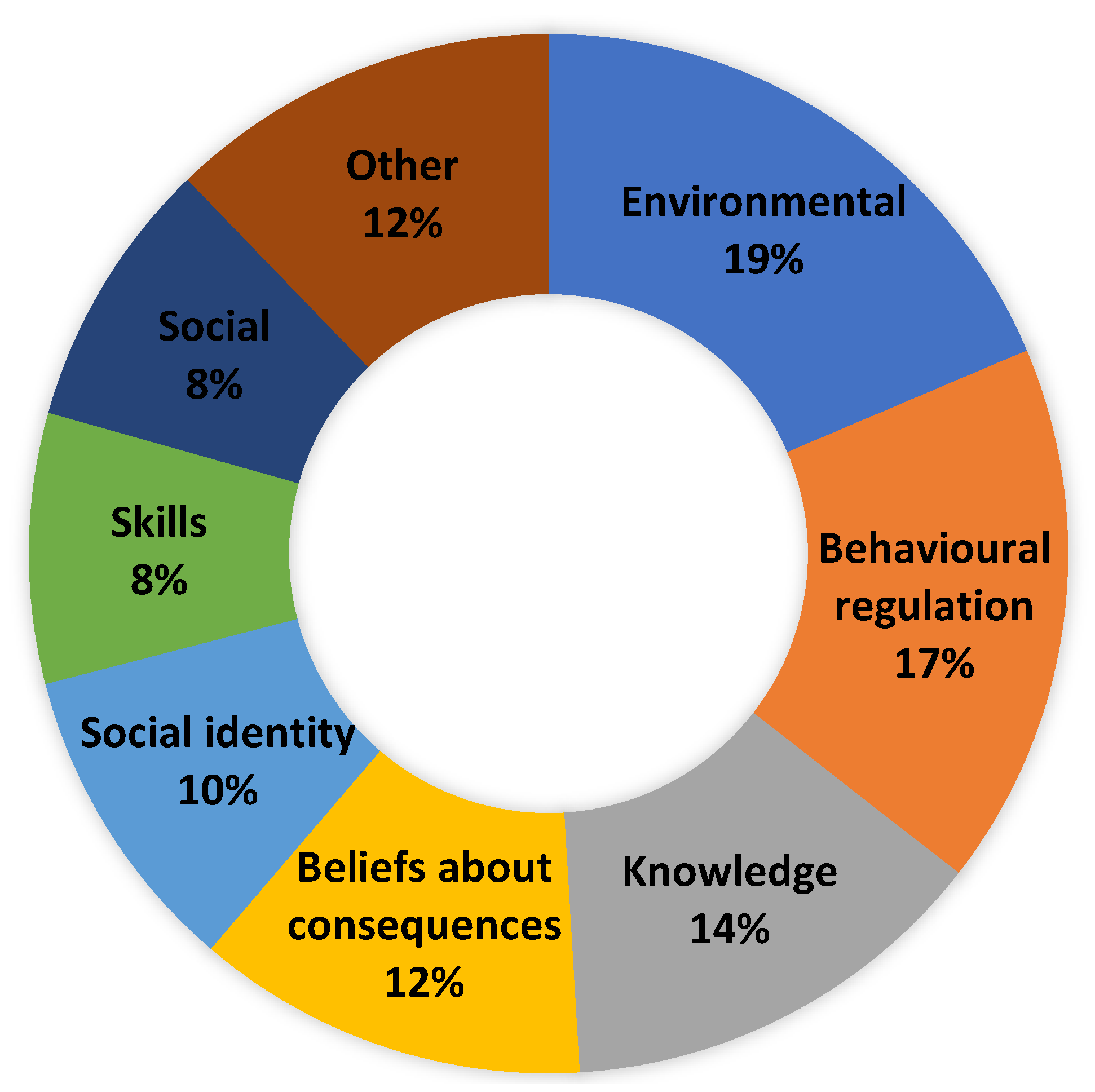
3.3. Key Domains
3.3.1. Environmental Context and Resources (Physical Opportunity)
“I’m on sick leave now, so I find I have the time to prep.”(Female, aged 46, breast cancer, 1 year post-treatment)
“I get the fresh fish comes three or four days a week from Kilybegs.”(Male, aged 69, prostate cancer, 1 year post-treatment)
“I wanted to eat properly, and then my gut was affected.”(Female, aged 67, colon, 1 year post-treatment)
“If I could get the vomiting sorted out.”(Female, aged 52, oesophagus cancer, 1 year post-treatment)
“I have no appetite at all.”(Female, aged 52, oesophagus cancer, 1 year post-treatment)
“The emphasis needs to come off weight and more on what’s your body going to be lacking after chemotherapy.”(Female, aged 53, non-Hodgkin’s Lymphoma, 1 year post-treatment)
“Definitely costs more to eat healthily.”(Female, aged 56, breast cancer, 10 years post-treatment)
“The cost of it can hinder you from eating healthily.”(Female, aged 67, colon cancer, 1 year post-treatment)
“it’s tough. You need a lot of discipline and much time as well to prepare and finish and plan.”(Male, aged 57, prostate cancer, 3 years post-treatment)
“Difficult timewise.”(Female, aged 46, breast cancer, 1 year post-treatment)
“In work, I find you slip, if you’re buying your lunches.”Female, aged 42, breast cancer, 2 years post-treatment)
“Moved into my parents’ house while I was having treatments…there are chocolates and there’s temptations here all the time so that would be my downfall.”(Female, aged 46, breast cancer, 1 year post-treatment)
3.3.2. Behavioural Regulation (Psychological Capability)
“Always have a fridge full of vegetables.”(Female, aged 61, breast cancer, 3 years post-treatment)
“Plan out some meals for the week.”(Female, aged 67, colon cancer, 1-year post-treatment)
“I have to have the balance.”(Female, aged 49, breast cancer, 14 years post-treatment)
“I think it’s also not good to be hauling ourselves over the coals if we crumble at the odd meal.”(Female, aged 34, breast cancer, 1 year post-treatment)
“I try Monday to Friday at least I am pretty strict”(Female, aged 56, breast cancer, 10 years post-treatment)
3.3.3. Knowledge (Psychological Capability)
“It is as important, if not more, as all the drugs we received along the way.”(Female, aged 34, breast cancer, 1 year post-treatment)
“It’s very important….feed my body with the proper nutrients, that are going to aid my recovery.”(Female, aged 61, breast cancer, 2 years post-treatment)
“I feel like all the evidence is on the side of plant-based.”(Female, aged 62, breast cancer, 8 years post-treatment)
“There must be an alternative to that, and I haven’t got that information.”(Male, aged 51, lymphoma, 2 years post-treatment)
“I know we’re completely left on our own.”(Female, aged 37, breast cancer, 18 months post-treatment)
“There was nothing there.”(Female, aged 61, breast cancer, 2 years post-treatment)
“Want to know more about nutrition.”(Female, aged 67, colon cancer, 1 year post-treatment)
“Nice to have personalised.”(Female, aged 67, lung/bowel cancer, 2 years post-treatment)
“We should know what we should eat to get good.”(Female, aged 49, breast cancer, 14 years post-treatment)
3.3.4. Beliefs about Consequences (Reflective Motivation)
“Feed my body with the proper nutrients that are going to aid my recovery.”(Female, aged 61, breast cancer, 2 years post-treatment)
“My energy levels have improved greatly.”(Female, aged 62, breast cancer, 8 years post-treatment)
“Going to speed up your recovery.”(Female, aged 23, acute myeloid leukaemia, 9 years post-treatment)
“It’s what you want to get back to normality.”(Female, aged 55, breast cancer, 5 years post-treatment)
“To help me and fight cancer coming back.”(Female, aged 53, non-Hodgkin’s lymphoma, 1 year post-treatment)
3.3.5. Social/Professional Role or Identity (Social Opportunity)
“Whatever I pick is geared towards being healthy.”(Female, aged 67, colon cancer, 1 year post-treatment)
“You want to be as healthy as you can.”(Female, aged 23, acute myeloid leukaemia, 9 years post-treatment)
3.3.6. Social Influences (Social Opportunity)
“We all have that kind of try to eat well attitude, and I think that helps.”(Female, aged 42, breast cancer, 2 years post-treatment)
“We are on the same level, my partner, so there’s no problem there eating healthily.”(Female, aged 67, lung/bowel cancer, 2 years post-treatment)
“I think my family would be a help.”(Female, aged 62, breast cancer, 8 years post-treatment)
“I think it’s very difficult sometimes if other people and family aren’t following the same nutritional programme that you’re following.”(Female, aged 47, breast cancer, 2 years post-treatment)
“There are three teenagers in this house, so you know, it doesn’t work.”(Male, aged 51, lymphoma, 2 years post-treatment)
“If they’re not on board it’s very hard.”(Male, aged 57, prostate cancer, 3 years post-treatment)
3.3.7. Skills (Physical Capability)
“I would call myself a reasonable cook.”(Female, aged 56, breast cancer, 10 years post-treatment)
“I do have the skills.”(Female, aged 42, breast cancer, 2 years post-treatment)
3.4. Identifying Intervention Options
- (1)
- Enablement—increasing means and reducing barriers to increase capability or opportunity (e.g., behavioural support to change dietary behaviour; strategies to reduce the impact of symptoms).
- (2)
- Environmental restructuring—changing the physical environment (e.g., re-designing a work cafeteria to emphasise healthy foods, clear menu labelling, price incentives, point of purchase messaging)
- (3)
- Restrictions—designed to limit access to an unhealthy substance (e.g., sugar-sweetened beverage tax, food standards within hospitals)
- (4)
- Training—imparting skills (e.g., how to cook healthier meals, how to shop for healthy food on a budget)
4. Discussion
4.1. Implications for Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hegarty, J.; Murphy, A.H.T.; O’Mahony, M.; Landers, M.; McCarthy, B.; Lehane, E.; Noonan, B.; Fitzgerald, S.; Reidy, M.; Saab, M.M.; et al. National Cancer Survivorship Needs Assessment: Living with and Beyond Cancer in Ireland; National Cancer Control Programme: Dublin, Ireland, 2019. [Google Scholar]
- Robien, K.; Demark-Wahnefried, W.; Rock, C.L. Evidence-Based Nutrition Guidelines for Cancer Survivors: Current Guidelines, Knowledge Gaps, and Future Research Directions. J. Am. Diet. Assoc. 2011, 111, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Teepen, J.C.; Kremer, L.; Ronckers, C.M.; van Leeuwen, F.E.; Hauptmann, M.; Dulmen-Den Broeder, V.; Van Der Pal, H.J.; Jaspers, M.W.; Tissing, W.J.; Den Heuvel-Eibrink, V. Long-term risk of subsequent malignant neoplasms after treatment of childhood cancer in the DCOG LATER study cohort: Role of chemotherapy. J. Clin. Oncol. 2017, 35, 2288–2298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armenian, S.H.; Xu, L.; Ky, B.; Sun, C.; Farol, L.T.; Pal, S.K.; Douglas, P.S.; Bhatia, S.; Chao, C. Cardiovascular Disease Among Survivors of Adult-Onset Cancer: A Community-Based Retrospective Cohort Study. J. Clin. Oncol. 2016, 34, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Liu, Z.; Thong, M.S.Y.; Doege, D.; Arndt, V. Higher Incidence of Diabetes in Cancer Patients Compared to Cancer-Free Population Controls: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 1808. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.W.; Suh, B.; Lim, H.; Suh, Y.-S.; Choi, Y.J.; Jeong, S.-M.; Yun, J.M.; Song, S.O.; Park, Y. Increased Risk of Osteoporotic Fracture in Postgastrectomy Gastric Cancer Survivors Compared with Matched Controls: A Nationwide Cohort Study in Korea. Am. J. Gastroenterol. 2019, 114, 1735–1743. [Google Scholar] [CrossRef]
- Bryant, A.L.; Walton, A.L.; Phillips, B. Cancer-related fatigue: Scientific progress has been made in 40 years. Clin. J. Oncol. Nurs. 2015, 19, 137–139. [Google Scholar] [CrossRef] [Green Version]
- Coa, K.I.; Epstein, J.B.; Ettinger, D.; Jatoi, A.; McManus, K.; Platek, M.E.; Price, W.; Stewart, M.; Teknos, T.N.; Moskowitz, B. The Impact of Cancer Treatment on the Diets and Food Preferences of Patients Receiving Outpatient Treatment. Nutr. Cancer 2015, 67, 339–353. [Google Scholar] [CrossRef] [Green Version]
- Boltong, A.; Keast, R. The influence of chemotherapy on taste perception and food hedonics: A systematic review. Cancer Treat. Rev. 2012, 38, 152–163. [Google Scholar] [CrossRef]
- WCRF; AIfCRD. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2. 2018. Available online: http://dietandcancerreport.org (accessed on 15 July 2022).
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [Green Version]
- Winkels, R.M.; Lee, L.; Beijer, S.; Bours, M.J.; Duijnhoven, F.J.B.; Geelen, A.; Hoedjes, M.; Mols, F.; Vries, J.; Weijenberg, M.P.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research lifestyle recommendations in colorectal cancer survivors: Results of the PROFILES registry. Cancer Med. 2016, 5, 2587–2595. [Google Scholar] [CrossRef] [Green Version]
- Kałędkiewicz, E.; Szostak-Węgierek, D. Current and past adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations in survivors of breast cancer. Rocz. Panstw. Zakl. Hig. 2019, 70, 295–305. [Google Scholar] [CrossRef]
- O’Callaghan, N.; Douglas, P.; Keaver, L. Nutrition Practices among Adult Cancer Survivors Living on the Island of Ireland: A Cross-Sectional Study. Nutrients 2022, 14, 767. [Google Scholar] [CrossRef] [PubMed]
- Beeken, R.; Williams, K.; Wardle, J.; Croker, H. “What about diet?” A qualitative study of cancer survivors’ views on diet and cancer and their sources of information. Eur. J. Cancer Care 2016, 25, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.S.; Rice, N.; Kingston, E.; Kelly, A.; Reynolds, J.V.; Feighan, J.; Power, D.G.; Ryan, A.M. A national survey of oncology survivors examining nutrition attitudes, problems and behaviours, and access to dietetic care throughout the cancer journey. Clin. Nutr. ESPEN 2020, 41, 331–339. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the Crest of the Teachable Moment: Promoting Long-Term Health after the Diagnosis of Cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef] [Green Version]
- Shea–Budgell, M.; Kostaras, X.; Myhill, K.; Hagen, N. Information Needs and Sources of Information for Patients during Cancer Follow-Up. Curr. Oncol. 2014, 21, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.W.; Courneya, K.S.; Peddle-McIntyre, C.; Mackey, J.R. Oncologists’ opinions towards recommending exercise to patients with cancer: A Canadian national survey. Support. Care Cancer 2005, 13, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Ventura, E.E.; Ganz, P.A.; Bower, J.E.; Abascal, L.; Petersen, L.; Stanton, A.L.; Crespi, C. Barriers to physical activity and healthy eating in young breast cancer survivors: Modifiable risk factors and associations with body mass index. Breast Cancer Res. Treat. 2013, 142, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.D.; Brage, S.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Does the importance of dietary costs for fruit and vegetable intake vary by socioeconomic position? Br. J. Nutr. 2015, 114, 1464–1470. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.; Park, C. Barriers to physical activity and healthy diet among breast cancer survivors: A multilevel perspective. Eur. J. Cancer Care 2017, 27, e12772. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, A.J.; Day, R.S.; Taylor, W.C.; Sharma, S.V.; Sloane, R.; Snyder, D.C.; Kraus, W.E.; Demark-Wahnefried, W. Exercise among breast and prostate cancer survivors—What are their barriers? J. Cancer Surviv. 2011, 5, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Francis, J.; Eccles, M.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers. Centre for Health Services Research. 2004. Available online: https://openaccess.city.ac.uk/id/eprint/1735/1/TPB%20Manual%20FINAL%20May2004.pdf (accessed on 15 July 2022).
- Timlin, D.; McCormack, J.M.; Simpson, E.E. Using the COM-B model to identify barriers and facilitators towards adoption of a diet associated with cognitive function (MIND diet). Public Health Nutr. 2020, 24, 1657–1670. [Google Scholar] [CrossRef] [PubMed]
- Al Rawahi, S.H.; Asimakopoulou, K.; Newton, J.T. Factors related to reducing free sugar intake among white ethnic adults in the UK: A qualitative study. BDJ Open 2018, 4, 17024. [Google Scholar] [CrossRef] [Green Version]
- Bentley, M.R.; Mitchell, N.; Sutton, L.; Backhouse, S.H. Sports nutritionists’ perspectives on enablers and barriers to nutritional adherence in high performance sport: A qualitative analysis informed by the COM-B model and theoretical domains framework. J. Sports Sci. 2019, 37, 2075–2085. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Moore, S.E.; Appleton, K.M.; Cupples, M.E.; Erwin, C.; Kee, F.; Prior, L.; Young, I.S.; McKinley, M.C.; Woodside, J.V. Development of a peer support intervention to encourage dietary behaviour change towards a Mediterranean diet in adults at high cardiovascular risk. BMC Public Health 2018, 18, 1194. [Google Scholar] [CrossRef] [PubMed]
- Rohde, A.; Duensing, A.; Dawczynski, C.; Godemann, J.; Lorkowski, S.; Brombach, C. An App to Improve Eating Habits of Adolescents and Young Adults (Challenge to Go): Systematic Development of a Theory-Based and Target Group–Adapted Mobile App Intervention. JMIR mHealth uHealth 2019, 7, e11575. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, D.P. Considerations in the choice of interobserver reliability estimates. J. Appl. Behav. Anal. 1977, 10, 103–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Veen, M.R.; Mols, F.; Bours, M.J.L.; Weijenberg, M.P.; Kampman, E.; Beijer, S. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention is associated with better health–related quality of life among long-term colorectal cancer survivors: Results of the PROFILES registry. Support. Care Cancer 2019, 27, 4565–4574. [Google Scholar] [CrossRef] [Green Version]
- Fraser, G.E. Vegetarian diets: What do we know of their effects on common chronic diseases? Am. J. Clin. Nutr. 2009, 89, 1607S–1612S. [Google Scholar] [CrossRef] [Green Version]
- Pimentel, D.; Pimentel, M. Sustainability of meat-based and plant-based diets and the environment. Am. J. Clin. Nutr. 2003, 78, 660S–663S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baroni, L.; Cenci, L.; Tettamanti, M.; Berati, M. Evaluating the environmental impact of various dietary patterns combined with different food production systems. Eur. J. Clin. Nutr. 2006, 61, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.K.; Park, S.Y.; Choi, G. Facilitators and Barriers to Adoption of a Healthy Diet in Survivors of Colorectal Cancer. J. Nurs. Scholarsh. 2019, 51, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Arroyave, W.D.; Clipp, E.C.; Miller, P.E.; Jones, L.W.; Ward, D.S.; Bonner, M.J.; Rosoff, P.M.; Snyder, D.C.; Demark-Wahnefried, W. Childhood Cancer Survivors’ Perceived Barriers to Improving Exercise and Dietary Behaviors. Oncol. Nurs. Forum 2008, 35, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Raber, M.; Crawford, K.; Baranowski, T.; Sharma, S.V.; Schick, V.; Markham, C.; Roth, M.; Wakefield, C.E.; Chandra, J. Meal planning values impacted by the cancer experience in families with school-aged survivors—A qualitative exploration and recommendations for intervention development. Support. Care Cancer 2019, 28, 1305–1313. [Google Scholar] [CrossRef]
- Bagnall, A.-M.; Radley, D.; Jones, R.; Gately, P.; Nobles, J.; Van Dijk, M.; Blackshaw, J.; Montel, S.; Sahota, P. Whole systems approaches to obesity and other complex public health challenges: A systematic review. BMC Public Health 2019, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Park, S.; Choi, G.-S. Association of support from family and friends with self-leadership for making long-term lifestyle changes in patients with colorectal cancer. Eur. J. Cancer Care 2018, 27, e12846. [Google Scholar] [CrossRef]
- Satia, J.A.; Walsh, J.F.; Pruthi, R.S. Health Behavior Changes in White and African American Prostate Cancer Survivors. Cancer Nurs. 2009, 32, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Beagan, B.L.; Chapman, G.E. Family Influences on Food Choice: Context of Surviving Breast Cancer. J. Nutr. Educ. Behav. 2004, 36, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.S.; Martin, R.M.; Renehan, A.G.; Cade, J.; Copson, E.R.; Cross, A.J.; Grimmett, C.; Keaver, L.; King, A.; Riboli, E.; et al. Cancer survivorship, excess body fatness and weight-loss intervention—Where are we in 2020? Br. J. Cancer 2021, 124, 1057–1065. [Google Scholar] [CrossRef]
- Szinay, D.; Perski, O.; Jones, A.; Chadborn, T.; Brown, J.; Naughton, F. Perceptions of Factors Influencing Engagement with Health and Well-being Apps in the United Kingdom: Qualitative Interview Study. JMIR mHealth uHealth 2021, 9, e29098. [Google Scholar] [CrossRef]
- Swartz, J.J.; Dowray, S.; Braxton, D.; Mihas, P.; Viera, A.J. Simplifying healthful choices: A qualitative study of a physical activity based nutrition label format. Nutr. J. 2013, 12, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mete, R.; Shield, A.; Murray, K.; Bacon, R.; Kellett, J. What is healthy eating? A qualitative exploration. Public Health Nutr. 2019, 22, 2408–2418. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.; Drake, T.; Vollmer, R.L. A qualitative research study comparing nutrition advice communicated by registered Dietitian and non-Registered Dietitian bloggers. J. Commun. Health 2020, 13, 55–63. [Google Scholar] [CrossRef]
- De Leo, A.; Bayes, S.; Bloxsome, D.; Butt, J. Exploring the usability of the COM-B model and Theoretical Domains Framework (TDF) to define the helpers of and hindrances to evidence-based practice in midwifery. Implement. Sci. Commun. 2021, 2, 7. [Google Scholar] [CrossRef]
- Whittenbury, K.; Kroll, L.; Dubicka, B.; Bull, E.R. Exploring barriers and facilitators for mental health professionals delivering behavioural activation to young people with depression: Qualitative study using the Theoretical Domains Framework. BJPsych Open 2022, 8, e38. [Google Scholar] [CrossRef] [PubMed]
- Lucci, V.-E.M.; McKay, R.C.; McBride, C.B.; McGrath, M.S.; Willms, R.; Gainforth, H.L.; Claydon, V.E. Barriers and facilitators to changing bowel care practices after spinal cord injury: A Theoretical Domains Framework approach. Spinal Cord 2022, 60, 664–673. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| COM-B | Domain (Definition) * | Theoretical Constructs Represented within Each Domain * | Interview Prompt Questions |
|---|---|---|---|
| Psychological Capability | Knowledge (An awareness of the existence of something) | Knowledge (including knowledge of condition/scientific rationale); Procedural knowledge; Schemas, mindsets and illness representations | What is your understanding of a healthy diet for someone with cancer? |
| Physical Capability | Skills (An ability or proficiency acquired through practice) | Skills; Competence/Ability/Skills assessment; practice/skills development; Interpersonal skills; Coping strategies | Do you feel you have the necessary skills e.g., preparing/cooking/eating to eat a diet that promotes health? |
| Psychological Capability | Memory, attention and decision processes (The ability to retain information, focus selectively on aspects of the environment and choose between alternatives) | Memory; Attention; Attention control; Decision making; Cognitive overload/tiredness | To what extent is eating a diet that promotes health something you normally do? Are there any situations that make it difficult for you to remember to do this? |
| Psychological Capability | Behavioural regulation (Anything aimed at managing or changing objectively observed or measured actions) | Self-monitoring; Breaking habit; Action planning | To what extent do you monitor whether you are eating foods that promote health? |
| Social Opportunity | Social/professional role or identity (A coherent set of behaviours and displayed personal qualities of an individual in a social or work setting) | Professional identity; Professional role; Social identity; Identity; Professional boundaries; Professional confidence; Group identity; Leadership; Organisational commitment | In general, do you think of yourself as someone who maintains a healthy diet? |
| Reflective Motivation | Beliefs about capabilities (Acceptance of the truth, reality, or validity about an ability, talent, or facility that a person can put to constructive use) | Self-confidence; Perceived competence; Self-efficacy; Perceived behavioural control; Beliefs; Self-esteem; Empowerment; Professional confidence | How difficult/easy would it be for you to eat a diet that promotes health? Prompt: What are the barriers to consuming a diet that promotes health? Prompt: What are the facilitators to consuming a diet that promotes health? |
| Reflective Motivation | Optimism (The confidence that things will happen for the best or that desired goals will be attained) | Optimism; Pessimism; Unrealistic optimism; Identity | Are you confident that any barriers you may have to eating a diet that promotes health can be solved? |
| Reflective Motivation | Beliefs about consequences (Acceptance of the truth, reality, or validity about outcomes of a behaviour in a given situation) | Beliefs; Outcome expectancies; Characteristics of outcome expectancies; Anticipated regret; Consequents | What do you think are the benefits or drawbacks of eating a diet that promotes health? |
| Reflective Motivation | Intentions (A conscious decision to perform a behaviour/act in a certain way) | Stability of intentions; Stages of change model; Transtheoretical model and stages of change | To what extent do you intend to follow a diet that promotes health? |
| Reflective Motivation | Goals (Mental representations of outcomes or end states that an individual wants to achieve) | Goals (distal/proximal); Goal priority; Goal/target setting; Goals (autonomous/controlled); Action planning; Implementation intention | Are there any strategies you have put in place to ensure you can implement a diet that promotes health? |
| Automatic Motivation | Reinforcement (Increasing the probability of a response by arranging a dependent relationship, or contingency, between the response and a given stimulus) | Rewards (proximal/distal, valued/not valued, probable/improbable); Incentives; Punishment; Consequents; Reinforcement; Contingencies; Sanctions | Are there any incentives for you to eat a diet that promotes health? |
| Automatic Motivation | Emotion (A complex reaction pattern, involving experiential, behavioural, and physiological elements, by which the individual attempts to deal with a personally significant matter or event) | Fear; Anxiety; Affect; Stress; Depression; Positive/negative affect; Burn-out | How would eating a diet to promote health make you feel do you think? |
| Physical Opportunity | Environmental context and resources (Any circumstance of a person’s situation or environment that discourages or encourages the development of skills and abilities, independence, social competence, and adaptive behaviour) | Environmental stressors; Resources/material resources; Organisational culture/climate; Salient events/critical incidents; Person x environment interaction; Barriers and facilitators | What factors help or hinder you eating foods that promote health? e.g., budget, time |
| Social Opportunity | Social influences (Those interpersonal processes that can cause individuals to change their thoughts, feelings, or behaviours) | Social pressure; Social norms; Group conformity; Social comparisons; Group norms; Social support; Power; Intergroup conflict; Alienation; Group identity; Modelling | To what extent do/would your family or friends help or hinder you eating a diet that promotes health? |
| Respondents Characteristics | n (%) Mean ± SD |
|---|---|
| Gender | |
| Male | 3 (15.0) |
| Female | 17 (85.0) |
| Age (years) | 51.3 ± 11.9 |
| Education | |
| Post Leaving Certificate (PLC), Diploma or Cert | 7 (35.0) |
| Bachelor’s degree | 8 (40.0) |
| Graduate Degree (Master’s or PhD) | 5 (25.0) |
| Employment | |
| Part-time employment | 2 (10.0) |
| Full-time employment | 13 (65.0) |
| Homemaker | 1 (5.0) |
| Unemployed | 1 (5.0) |
| Retired | 3 (15.0) |
| Clinical Characteristics | n (%) |
| Primary tumour | |
| Breast Cancer | 12 (60.0) |
| Hematologic | 3 (15.0) |
| Bowel and Colon Cancer | 3 (15.0) |
| Prostate Cancer | 2 (10.0) |
| Oesophageal | 1 (5.0) |
| Years since treatment finished | |
| 1–2 | 5 (25.0) |
| 3–5 | 10 (50.0) |
| 6–10 | 2 (10.0) |
| >10 | 3 (15.0) |
| Completed treatments | |
| Chemotherapy | 17 (85.0) |
| Radiotherapy | 10 (50.0) |
| Hormone Therapy | 8 (40.0) |
| Surgery | 16 (80.0) |
| BMI (kg/m²) | 27.5 ± 6.5 |
| Facilitators | Barriers | |||||
|---|---|---|---|---|---|---|
| TDF Domain + (definition) Definitions as per Atkins et al., 2017 [35] | Frequency of mentions relating to codes | Participants who contributed to each domain | % Mention | Frequency of mentions relating to codes | Participants who contributed to each domain | % Mention |
| 1. Knowledge (An awareness of the existence of something) | 21 | 14 | 12.1 | 11 | 7 | 17.2 |
| 2. Skills * (An ability or proficiency acquired through practice) | 20 | 20 | 11.5 | 0 | 0 | 0 |
| 3. Social/professional role and identity * (A coherent set of behaviours and displayed personal qualities of an individual in a social or work setting) | 23 | 20 | 13.3 | 0 | 0 | 0 |
| 4. Beliefs about capabilities (Acceptance of the truth, reality or validity about an ability, talent or facility that a person can put to constructive use) | 1 | 1 | 0.6 | 3 | 3 | 4.7 |
| 5. Optimism (The confidence that things will happen for the best or that desired goals will be attained) | 0 | 0 | 0 | 0 | 0 | 0 |
| 6. Beliefs about consequences * (Acceptance of the truth, reality, or validity about outcomes of a behaviour in a given situation) | 29 | 14 | 16.8 | 0 | 0 | 0 |
| 7. Reinforcement (Increasing the probability of a response by arranging a dependent relationship, or contingency, between the response and a given stimulus) | 0 | 0 | 0 | 0 | 0 | 0 |
| 8. Intentions (A conscious decision to perform a behaviour or a resolve to act in a certain way) | 14 | 8 | 8.1 | 0 | 0 | 0 |
| 9. Goals (Mental representations of outcomes or end states that an individual wants to achieve) | 0 | 0 | 0 | 0 | 0 | 0 |
| 10. Memory, attention and decision processes (The ability to retain information, focus selectively on aspects of the environment and choose between two or more alternatives) | 0 | 0 | 0 | 1 | 1 | 1.6 |
| 11. Environmental context and resources * (Any circumstance of a person’s situation or environment that discourages or encourages the development of skills and abilities, independence, social competence and adaptive behaviour) | 9 | 7 | 5.2 | 35 | 17 | 54.7 |
| 12. Social influences * (Those interpersonal processes that can cause individuals to change their thoughts, feelings, or behaviours) | 13 | 11 | 7.5 | 7 | 7 | 11 |
| 13. Emotion (A complex reaction pattern, involving experiential, behavioural, and physiological elements, by which the individual attempts to deal with a personally significant matter or event) | 3 | 3 | 1.7 | 7 | 6 | 11 |
| 14. Behavioural regulation * (Anything aimed at managing or changing objectively observed or measured actions) | 40 | 20 | 23.1 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keaver, L.; Douglas, P.; O’Callaghan, N. Perceived Barriers and Facilitators to a Healthy Diet among Cancer Survivors: A Qualitative Exploration Using the TDF and COM-B. Dietetics 2023, 2, 123-139. https://doi.org/10.3390/dietetics2010010
Keaver L, Douglas P, O’Callaghan N. Perceived Barriers and Facilitators to a Healthy Diet among Cancer Survivors: A Qualitative Exploration Using the TDF and COM-B. Dietetics. 2023; 2(1):123-139. https://doi.org/10.3390/dietetics2010010
Chicago/Turabian StyleKeaver, Laura, Pauline Douglas, and Niamh O’Callaghan. 2023. "Perceived Barriers and Facilitators to a Healthy Diet among Cancer Survivors: A Qualitative Exploration Using the TDF and COM-B" Dietetics 2, no. 1: 123-139. https://doi.org/10.3390/dietetics2010010
APA StyleKeaver, L., Douglas, P., & O’Callaghan, N. (2023). Perceived Barriers and Facilitators to a Healthy Diet among Cancer Survivors: A Qualitative Exploration Using the TDF and COM-B. Dietetics, 2(1), 123-139. https://doi.org/10.3390/dietetics2010010