
Effect of Cocoa Beverage and Dark Chocolate Intake on Lipid Profile in People Living with Normal and Elevated LDL Cholesterol: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- (i)
- Articles must be published as original research.
- (ii)
- Articles should be written in English and accessible in full-text.
- (iii)
- Articles must present data for lipid profile at baseline and at post-intervention or the change in lipid profile at post-intervention.
- (iv)
- The duration of the study should be equal or longer than 2 weeks.
- (v)
- The study must involve a comparison between a cocoa product used as a treatment, and either a non-cocoa product or a cocoa product with a negligible amount of polyphenol used as a control.
- (vi)
- The study must focus on an adult population, specifically individuals aged 18 years and above.
2.2. Exclusion Criteria
- (i)
- Studies published as editorials, review articles, conference proceedings, and commentaries.
- (ii)
- Studies that incorporated cocoa or chocolate intervention alongside other lifestyle interventions, such as exercise or weight-loss intervention.
- (iii)
- Studies that administered cocoa or chocolate supplemented with other nutrients.
- (iv)
- Studies with participants presenting significant comorbidities, including cardiovascular diseases and diabetes.
2.3. Data Extraction
2.4. Risk of Bias
2.5. Meta-Analysis
3. Results
3.1. Study Characteristics
3.2. Risk of Bias Assessment
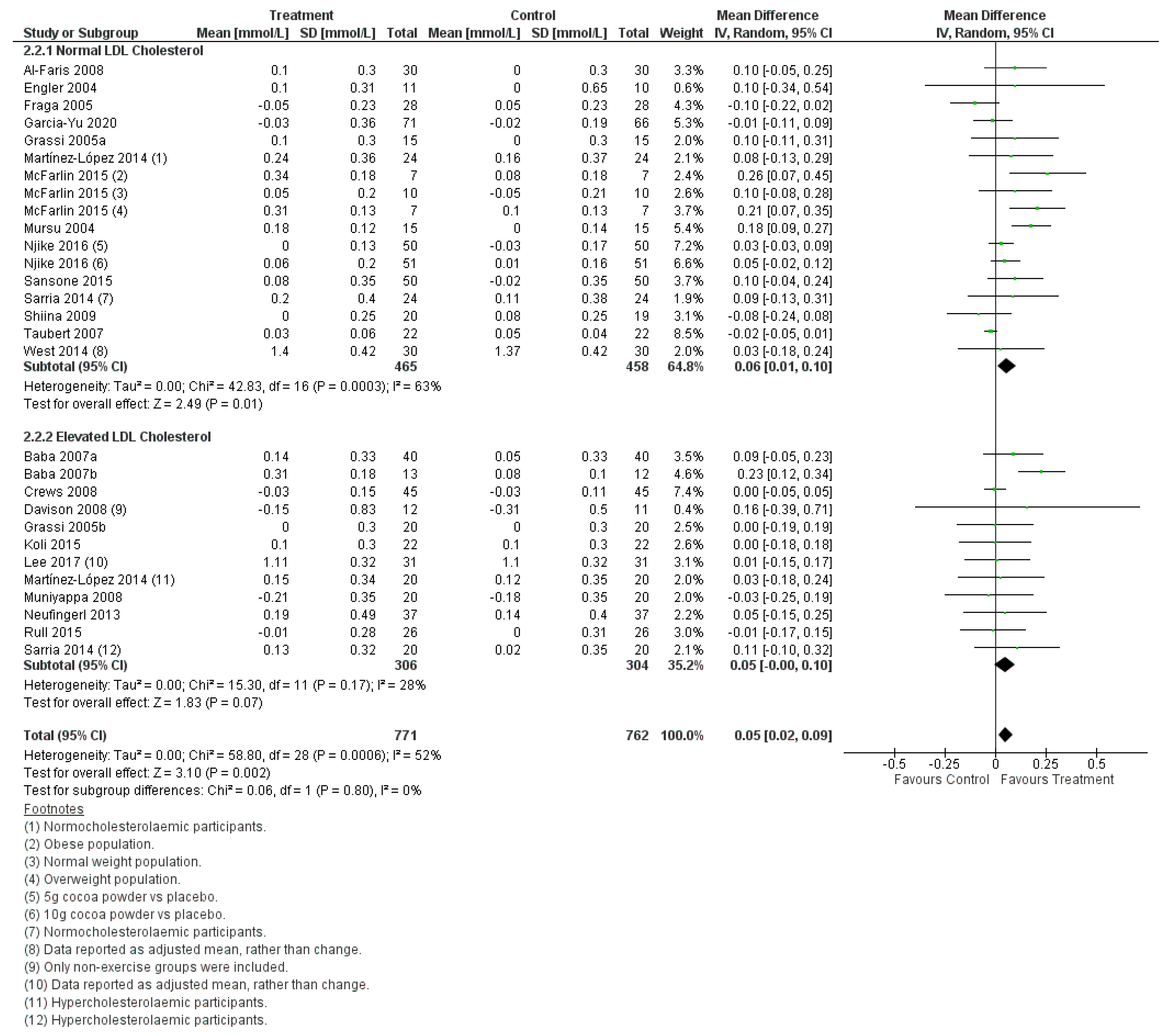
3.3. Meta-Analysis: Effect of Flavanol-Containing Cocoa Beverage and Chocolate Consumption on Lipid Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pirillo, A.; Casula, M.; Olmastroni, E.; Norata, G.D.; Catapano, A.L. Global epidemiology of dyslipidaemias. Nat. Rev. Cardiol. 2021, 18, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Barquera, S.; Pedroza-Tobias, A.; Medina, C.; Hernandez-Barrera, L.; Bibbins-Domingo, K.; Lozano, R.; Moran, A.E. Global Overview of the Epidemiology of Atherosclerotic Cardiovascular Disease. Arch. Med. Res. 2015, 46, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Finger, J.D.; Busch, M.A.; Du, Y.; Heidemann, C.; Knopf, H.; Kuhnert, R.; Lampert, T.; Mensink, G.B.; Neuhauser, H.K.; Rosario, A.S.; et al. Time Trends in Cardiometabolic Risk Factors in Adults. Dtsch. Arztebl. Int. 2016, 113, 712–719. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Bigna, J.J.; Nansseu, J.R.; Nyaga, U.F.; Balti, E.V.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Prevalence of dyslipidaemia among adults in Africa: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e998–e1007. [Google Scholar] [CrossRef] [Green Version]
- Berger, S.; Raman, G.; Vishwanathan, R.; Jacques, P.F.; Johnson, E.J. Dietary cholesterol and cardiovascular disease: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2015, 102, 276–294. [Google Scholar] [CrossRef] [Green Version]
- Schoeneck, M.; Iggman, D. The effects of foods on LDL cholesterol levels: A systematic review of the accumulated evidence from systematic reviews and meta-analyses of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1325–1338. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.; Kumar, S.; Diep Pham, H.T.; Coffey, S.; Mann, J. Dietary fibre in hypertension and cardiovascular disease management: Systematic review and meta-analyses. BMC Med. 2022, 20, 139. [Google Scholar] [CrossRef]
- Williams, B.A.; Mikkelsen, D.; Flanagan, B.M.; Gidley, M.J. “Dietary fibre”: Moving beyond the “soluble/insoluble” classification for monogastric nutrition, with an emphasis on humans and pigs. J. Anim. Sci. Biotechnol. 2019, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Jaramillo Flores, M.E. Cocoa Flavanols: Natural Agents with Attenuating Effects on Metabolic Syndrome Risk Factors. Nutrients 2019, 11, 751. [Google Scholar] [CrossRef] [Green Version]
- Febrianto, N.A.; Wang, S.; Zhu, F. Chemical and biological properties of cocoa beans affected by processing: A review. Crit. Rev. Food Sci. Nutr. 2022, 62, 8403–8434. [Google Scholar] [CrossRef] [PubMed]
- Amoah, I.; Lim, J.J.; Osei, E.O.; Arthur, M.; Tawiah, P.; Oduro, I.N.; Aduama-Larbi, M.S.; Lowor, S.T.; Rush, E. Effect of Cocoa Beverage and Dark Chocolate Consumption on Blood Pressure in Those with Normal and Elevated Blood Pressure: A Systematic Review and Meta-Analysis. Foods 2022, 11, 1962. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, Agricultural Research Service. Food Data Central. Available online: https://fdc.nal.usda.gov/index.html (accessed on 22 June 2023).
- Katz, D.L.; Doughty, K.; Ali, A. Cocoa and chocolate in human health and disease. Antioxid. Redox Signal. 2011, 15, 2779–2811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, F.M.; Bearden, M.M.; Keen, C.L. Cocoa and chocolate flavonoids: Implications for cardiovascular health. J. Am. Diet. Assoc. 2003, 103, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Krauss, R.M. Public health guidelines should recommend reducing saturated fat consumption as much as possible: YES. Am. J. Clin. Nutr. 2020, 112, 13–18. [Google Scholar] [CrossRef]
- Jia, L.; Liu, X.; Bai, Y.Y.; Li, S.H.; Sun, K.; He, C.; Hui, R. Short-term effect of cocoa product consumption on lipid profile: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2010, 92, 218–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Zhang, I.; Li, A.; Manson, J.E.; Sesso, H.D.; Wang, L.; Liu, S. Cocoa flavanol intake and biomarkers for cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. J. Nutr. 2016, 146, 2325–2333. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Follmann, D.; Elliott, P.; Suh, I.L.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Vlachojannis, J.; Erne, P.; Zimmermann, B.; Chrubasik-Hausmann, S. The impact of cocoa flavanols on cardiovascular health. Phytother. Res. 2016, 30, 1641–1657. [Google Scholar] [CrossRef]
- Higgins, J.P. Commentary: Heterogeneity in meta-analysis should be expected and appropriately quantified. Int. J. Epidemiol. 2008, 37, 1158–1160. [Google Scholar] [CrossRef] [Green Version]
- McFarlin, B.K.; Venable, A.S.; Henning, A.L.; Prado, E.A.; Best Sampson, J.N.; Vingren, J.L.; Hill, D.W. Natural cocoa consumption: Potential to reduce atherogenic factors? J. Nutr. Biochem. 2015, 26, 626–632. [Google Scholar] [CrossRef]
- Martinez-Lopez, S.; Sarria, B.; Sierra-Cinos, J.L.; Goya, L.; Mateos, R.; Bravo, L. Realistic intake of a flavanol-rich soluble cocoa product increases HDL-cholesterol without inducing anthropometric changes in healthy and moderately hypercholesterolemic subjects. Food Funct. 2014, 5, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Sarria, B.; Martinez-Lopez, S.; Sierra-Cinos, J.L.; Garcia-Diz, L.; Mateos, R.; Bravo, L. Regular consumption of a cocoa product improves the cardiometabolic profile in healthy and moderately hypercholesterolaemic adults. Br. J. Nutr. 2014, 111, 122–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njike, V.Y.; Hamburg, N.; Kellogg, M.; Annapureddy, A.; Vita, J. Dose and response to cocoa (DARC): A randomized double-blind controlled trial. Clin. Trials Regul. Sci. Cardiol. 2016, 23–24, 9–15. [Google Scholar] [CrossRef]
- Al-Faris, N.A. Short-term consumption of a dark chocolate containing flavanols is followed by a significant decrease in normotensive population. Pak. J. Nutr. 2008, 7, 773–781. [Google Scholar]
- Baba, S.; Natsume, M.; Yasuda, A.; Nakamura, Y.; Tamura, T.; Osakabe, N.; Kanegae, M.; Kondo, K. Plasma LDL and HDL cholesterol and oxidized LDL concentrations are altered in normo-and hypercholesterolemic humans after intake of different levels of cocoa powder. J. Nutr. 2007, 137, 1436–1441. [Google Scholar] [CrossRef] [Green Version]
- Baba, S.; Osakabe, N.; Kato, Y.; Natsume, M.; Yasuda, A.; Kido, T.; Fukuda, K.; Muto, Y.; Kondo, K. Continuous intake of polyphenolic compounds containing cocoa powder reduces LDL oxidative susceptibility and has beneficial effects on plasma HDL-cholesterol concentrations in humans. Am. J. Clin. Nutr. 2007, 85, 709–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crews Jr, W.D.; Harrison, D.W.; Wright, J.W. A double-blind, placebo-controlled, randomized trial of the effects of dark chocolate and cocoa on variables associated with neuropsychological functioning and cardiovascular health: Clinical findings from a sample of healthy, cognitively intact older adults. Am. J. Clin. Nutr. 2008, 87, 872–880. [Google Scholar]
- Davison, K.; Coates, A.; Buckley, J.; Howe, P. Effect of cocoa flavanols and exercise on cardiometabolic risk factors in overweight and obese subjects. Int. J. Obes. 2008, 32, 1289–1296. [Google Scholar] [CrossRef] [Green Version]
- Engler, M.B.; Engler, M.M.; Chen, C.Y.; Malloy, M.J.; Browne, A.; Chiu, E.Y.; Kwak, H.-K.; Milbury, P.; Paul, S.M.; Blumberg, J. Flavonoid-rich dark chocolate improves endothelial function and increases plasma epicatechin concentrations in healthy adults. J. Am. Coll. Nutr. 2004, 23, 197–204. [Google Scholar] [CrossRef]
- Fraga, C.G.; Actis-Goretta, L.; Ottaviani, J.I.; Carrasquedo, F.; Lotito, S.B.; Lazarus, S.; Schmitz, H.H.; Keen, C.L. Regular consumption of a flavanol-rich chocolate can improve oxidant stress in young soccer players. Clin. Dev. Immunol. 2005, 12, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Yu, I.A.; Garcia-Ortiz, L.; Gomez-Marcos, M.A.; Rodriguez-Sanchez, E.; Agudo-Conde, C.; Gonzalez-Sanchez, J.; Maderuelo-Fernandez, J.A.; Recio-Rodriguez, J.I. Effects of cocoa-rich chocolate on blood pressure, cardiovascular risk factors, and arterial stiffness in postmenopausal women: A randomized clinical trial. Nutrients 2020, 12, 1758. [Google Scholar] [CrossRef] [PubMed]
- Grassi, D.; Lippi, C.; Necozione, S.; Desideri, G.; Ferri, C. Short-term administration of dark chocolate is followed by a significant increase in insulin sensitivity and a decrease in blood pressure in healthy persons. Am. J. Clin. Nutr. 2005, 81, 611–614. [Google Scholar] [CrossRef] [Green Version]
- Grassi, D.; Necozione, S.; Lippi, C.; Croce, G.; Valeri, L.; Pasqualetti, P.; Desideri, G.; Blumberg, J.B.; Ferri, C. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension 2005, 46, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koli, R.; Kohler, K.; Tonteri, E.; Peltonen, J.; Tikkanen, H.; Fogelholm, M. Dark chocolate and reduced snack consumption in mildly hypertensive adults: An intervention study. Nutr. J. 2015, 14, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Berryman, C.E.; West, S.G.; Chen, C.O.; Blumberg, J.B.; Lapsley, K.G.; Preston, A.G.; Fleming, J.A.; Kris-Etherton, P.M. Effects of Dark Chocolate and Almonds on Cardiovascular Risk Factors in Overweight and Obese Individuals: A Randomized Controlled-Feeding Trial. J. Am. Heart Assoc. 2017, 6, e005162. [Google Scholar] [CrossRef] [Green Version]
- Muniyappa, R.; Hall, G.; Kolodziej, T.L.; Karne, R.J.; Crandon, S.K.; Quon, M.J. Cocoa consumption for 2 wk enhances insulin-mediated vasodilatation without improving blood pressure or insulin resistance in essential hypertension. Am. J. Clin. Nutr. 2008, 88, 1685–1696. [Google Scholar] [CrossRef] [Green Version]
- Mursu, J.; Voutilainen, S.; Nurmi, T.; Rissanen, T.H.; Virtanen, J.K.; Kaikkonen, J.; Nyyssonen, K.; Salonen, J.T. Dark chocolate consumption increases HDL cholesterol concentration and chocolate fatty acids may inhibit lipid peroxidation in healthy humans. Free Radic. Biol. Med. 2004, 37, 1351–1359. [Google Scholar] [CrossRef]
- Neufingerl, N.; Zebregs, Y.E.; Schuring, E.A.; Trautwein, E.A. Effect of cocoa and theobromine consumption on serum HDL-cholesterol concentrations: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 1201–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rull, G.; Mohd-Zain, Z.N.; Shiel, J.; Lundberg, M.H.; Collier, D.J.; Johnston, A.; Warner, T.D.; Corder, R. Effects of high flavanol dark chocolate on cardiovascular function and platelet aggregation. Vascul. Pharmacol. 2015, 71, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Sansone, R.; Rodriguez-Mateos, A.; Heuel, J.; Falk, D.; Schuler, D.; Wagstaff, R.; Kuhnle, G.G.; Spencer, J.P.; Schroeter, H.; Merx, M.W.; et al. Cocoa flavanol intake improves endothelial function and Framingham Risk Score in healthy men and women: A randomised, controlled, double-masked trial: The Flaviola Health Study. Br. J. Nutr. 2015, 114, 1246–1255. [Google Scholar] [CrossRef] [PubMed]
- Shiina, Y.; Funabashi, N.; Lee, K.; Murayama, T.; Nakamura, K.; Wakatsuki, Y.; Daimon, M.; Komuro, I. Acute effect of oral flavonoid-rich dark chocolate intake on coronary circulation, as compared with non-flavonoid white chocolate, by transthoracic Doppler echocardiography in healthy adults. Int. J. Cardiol. 2009, 131, 424–429. [Google Scholar] [CrossRef]
- Taubert, D.; Roesen, R.; Lehmann, C.; Jung, N.; Schömig, E. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide: A randomized controlled trial. JAMA 2007, 298, 49–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, S.G.; McIntyre, M.D.; Piotrowski, M.J.; Poupin, N.; Miller, D.L.; Preston, A.G.; Wagner, P.; Groves, L.F.; Skulas-Ray, A.C. Effects of dark chocolate and cocoa consumption on endothelial function and arterial stiffness in overweight adults. Br. J. Nutr. 2014, 111, 653–661. [Google Scholar] [CrossRef] [Green Version]
- Di Angelantonio, E.; Sarwar, N.; Perry, P.; Kaptoge, S.; Ray, K.K.; Thompson, A.; Wood, A.M.; Lewington, S.; Sattar, N.; Packard, C.J.; et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009, 302, 1993–2000. [Google Scholar] [CrossRef] [Green Version]
- Rosa Cde, O.; Dos Santos, C.A.; Leite, J.I.; Caldas, A.P.; Bressan, J. Impact of nutrients and food components on dyslipidemias: What is the evidence? Adv. Nutr. 2015, 6, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Feldman, F.; Koudoufio, M.; Desjardins, Y.; Spahis, S.; Delvin, E.; Levy, E. Efficacy of Polyphenols in the Management of Dyslipidemia: A Focus on Clinical Studies. Nutrients 2021, 13, 672. [Google Scholar] [CrossRef]
- Marz, W.; Kleber, M.E.; Scharnagl, H.; Speer, T.; Zewinger, S.; Ritsch, A.; Parhofer, K.G.; von Eckardstein, A.; Landmesser, U.; Laufs, U. HDL cholesterol: Reappraisal of its clinical relevance. Clin. Res. Cardiol. 2017, 106, 663–675. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.B.; Hurst, W.J.; Flannigan, N.; Ou, B.; Lee, C.Y.; Smith, N.; Stuart, D.A. Survey of commercially available chocolate- and cocoa-containing products in the United States. 2. Comparison of flavan-3-ol content with nonfat cocoa solids, total polyphenols, and percent cacao. J. Agric. Food Chem. 2009, 57, 9169–9180. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.; Amoah, I.; Diep, T.; Jalili-Moghaddam, S. Determinants and suitability of carotenoid reflection score as a measure of carotenoid status. Nutrients 2020, 12, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darand, M.; Hajizadeh Oghaz, M.; Hadi, A.; Atefi, M.; Amani, R. The effect of cocoa/dark chocolate consumption on lipid profile, glycemia, and blood pressure in diabetic patients: A meta-analysis of observational studies. Phytother. Res. 2021, 35, 5487–5501. [Google Scholar] [CrossRef] [PubMed]
- Tokede, O.A.; Gaziano, J.M.; Djousse, L. Effects of cocoa products/dark chocolate on serum lipids: A meta-analysis. Eur. J. Clin. Nutr. 2011, 65, 879–886. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutrient | Cocoa Powder, Unsweetened | Cocoa Butter | Dark Chocolate |
|---|---|---|---|
| Water (g/100 g) | 3 | 0 | 1.37 |
| Ash (g/100 g) | 5.8 | 0 | 2.32 |
| Total lipid (fat) (g/100 g) | 13.7 | 100 | 42.6 |
| Total dietary fibre (g/100 g) | 37 | 0 | 10.9 |
| Protein (g/100 g) | 19.6 | 0 | 7.79 |
| Carbohydrate, by difference (g/100 g) | 57.9 | 0 | 45.9 |
| Energy (kcal/100 g) | 228 | 884 | 598 |
| Calcium (mg/100 g) | 128 | 0 | 73 |
| Magnesium (mg/100 g) | 499 | 0 | 228 |
| Phosphorus (mg/100 g) | 734 | 0 | 308 |
| Potassium (mg/100 g) | 1520 | 0 | 715 |
| Sodium (mg/100 g) | 21 | 0 | 20 |
| Authors | Country of Study | Age (Years) | BMI (kg/m2) | Sample Size | Study Design | Baseline LDL-C a | Intervention Duration (Weeks) | Control | Intervention | Daily Dose of Polyphenol (mg) | Daily Dose of Flavanol (mg) | Daily Dose of Epicatechin (mg) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Al-Faris [29] | Saudi Arabia | 21 ± 2 | 19.4 ± 0.4 – 22.0 ± 1.5 | 89 | C, PT | Normal | 2 | White Chocolate | Dark chocolate | 500 | — | 4 | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Baba et al. [30] | Japan | 49 ± 9 | 24.2 ± 3.5 | 160 | DB, P, CT | Elevated | 4 | Placebo | Cocoa powder | — | — | 64.5/96.7/129 | ↑ HDL-C after cocoa intervention. No significant difference between doses. ≠∆ TC, LDL-C, and TG. |
| Baba et al. [31] | Japan | 38 ± 5 | 22.1 ± 1.0 | 25 | R, C, PT | Elevated | 12 | 12 g sugar | Cocoa powder + 12 g sugar | — | — | 98 | ↑ HDL-C (cocoa vs. control). ≠∆ TC, LDL-C, TG. |
| Crews Jr et al. [32] | USA | 69 ± 9–69 ± 8 | 25.2 ± 3.4 – 25.5 ± 3.6 | 90 | R, DB, PC, PT | Elevated | 6 | Placebo | Dark chocolate bar and cocoa beverage | — | — | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Davison et al. [33] | Australia | 44 ± 4–46 ± 4 | 32.8 ± 1.1 – 34.5 ± 1.8 | 49 | R, DB, PC, FPT | Elevated | 12 | LF (36 mg flavanol) cocoa beverage | HF cocoa beverage | — | 902 | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Engler et al. [34] | USA | 32 ± 3–33 ± 3 | 21.9 ± 1.6 – 23.2 ± 1.7 | 21 | R, DB, PC, PT | Normal | 2 | LF chocolate (trace amount epicatechin) | Dark chocolate bar | — | — | 46 | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Fraga et al. [35] | Argentina | 18 ± 1 | 24.1 ± 0.2 | 28 | R, C, CT | Normal | 2 | Cocoa butter chocolate | Flavanol-containing milk chocolate | — | 168 | 39 | ↓ TC and LDL-C (flavanol cocoa milk chocolate not cocoa butter chocolate) ≠∆ TG and HDL |
| Garcia-Yu et al. [36] | Spain | 57 ± 4 | 25.6 ± 3.1 – 25.7 ± 3.8 | 137 | R, DB, C, PT | Normal | 26 | No product | Chocolate | 65.5 | — | 26.1 | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Grassi et al. [37] | Italy | 34 ± 8 | 22.6 ± 3.0 | 15 | R, CT | Normal | 2 | White chocolate | Dark chocolate | 500 | — | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Grassi et al. [38] | Italy | 44 ± 8 | 25.4 ± 1.7 | 20 | R, CT | Elevated | 2 | White chocolate | Dark chocolate | — | 88 | 66 | ↓ TC (Dark chocolate not white chocolate) ↓ LDL-C (Dark chocolate compared with white chocolate). ≠∆ HDL-C and TG. |
| Koli et al. [39] | Finland | 46 ± 8 | 27.7 ± 3.7 | 22 | R, C, CT | Elevated | 8 | Reduced snack intake | Replaced snack intake with dark chocolate | — | 603 | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Lee et al. [40] | USA | 46 ± 10 | 29.6 ± 2.8 | 31 | R, SB, C, CT | Elevated | 4 | No product | Cocoa powder + dark chocolate | — | — | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Martinez-Lopez et al. [26] | Spain | 26 ± 6 (NC group); 30 ± 10 (HC group) | 23 ± 3 (NC group); 24 ± 3 (HC group) | 24 (NC group); 20 (HC group) | NR, C, CT | Normal (NC group); Elevated (HC group) | 4 | Milk | Cocoa powder + milk | — | 45.3 | 18.9 | ↑ HDL-C (both cocoa and milk groups). No significant difference between groups. ≠∆ TC, LDL-C, and TG. |
| McFarlin et al. [25] | USA | 21 ± 2–22 ± 3 | 21.6 ± 1.9 (NW group); 27.0 ± 1.4 (OW group); 34.9 ± 3.0 (OB group) | 24 | R, DB, PC, CT | Normal (all NW, OW, and OB groups) | 4 | Placebo | Chocolate | — | 640 | 48 | ↑ HDL-C (chocolate compared to placebo). ≠∆ TC, and TG. |
| Muniyappa et al. [41] | USA | 51 ± 7 | 33.2 ± 6.3 | 20 | R, DB, PC, CT | Elevated | 2 | Placebo | Cocoa beverage | 902 | — | 174 | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Mursu et al. [42] | Finland | 19–49 | 21.5 ± 2.9 – 24.1 ± 3.5 | 45 | NR, PT | Normal | 3 | White Chocolate | Dark Chocolate | 274/418 | — | 151.5/227 | ↑ HDL-C (Dark chocolate compared to white chocolate). ≠∆ TC, LDL-C, and TG. |
| Neufingerl et al. [43] | Netherlands | 53 ± 9–56 ± 8 | 23.8 ± 2.5 – 24.9 ± 3.1 | 143 | R, DB, PC, FPT | Elevated | 4 | Placebo | Cocoa beverage | — | 325 | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Njike et al. [28] | USA | 53 ± 11–54 ± 10 | 29.9 ± 4.2 – 30.7 ± 5.0 | 122 | R, DB, C, MLSPT | Normal | 8 | Placebo | Chocolate and cocoa powder | — | 257/514 | 24/46 | ≠∆ TC and LDL-C. ↑ HDL-C (High dose cocoa compared with baseline, no significant difference between groups). ↑ TG (Low dose cocoa compared with baseline, no significant difference between groups). |
| Rull et al. [44] | UK | 55 ± 8 | 26.6 ± 2.8 | 32 | R, DB, PC, CT | Elevated | 6 | LF dark chocolate (88 mg flavanol) | HF dark chocolate | — | 1064 | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Sansone et al. [45] | Germany | 44 ± 9–45 ± 8 | 25 ± 3 – 26 ± 3 | 100 | R, DB, PC, PT | Normal | 4 | Placebo beverage + theobromine + caffeine | Fruit-flavored cocoa beverage | — | 900 | 128 | ↓ TC, LDL-C and ↑ HDL-C (Cocoa beverage compared to placebo.) |
| Sarria et al. [27] | Spain | 26 ± 6 – 38 ± 8 (NC group); 25 ± 7 – 36 ± 11 (HC group) | 22.0 ± 2.6 – 24.1 ± 3.6 (NC group); 22.4 ± 2.3 – 26.2 ± 4.2 (HC group) | 24 (NC group); 20 (HC group) | R, C, CT | Normal (NC group); Elevated (HC group) | 4 | Milk | Cocoa + milk | 416 | — | — | ↑ HDL-C (cocoa compared to milk) ≠∆ TC, LDL-C, and TG. |
| Shiina et al. [46] | Japan | 30 ± 4 | 22.6 ± 2.0 | 39 | R, SB, PT | Normal | 2 | White Chocolate | Dark chocolate | 550 | — | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Taubert et al. [47] | Germany | 64 ± 5 | 24.0 ± 1.6 | 44 | R, SB, C, PT | Normal | 18 | White Chocolate | Dark chocolate | 30 | — | 5.1 | ≠∆ TC, HDL-C, LDL-C, and TG. |
| West et al. [48] | USA | 53 ± 2 | 27.8 ± 3.9 | 30 | R, DB, PC, CT | Normal | 4 | LF chocolate (43 mg flavanol) + placebo beverage | Dark chocolate + cocoa beverage | — | 814 | — | ≠∆ TC, HDL-C, LDL-C, and TG. |
| Subgroups | WMD (95% CI) mmol/L | p-Value | I2 (%) | n | Subgroup Differences (p-Value) |
|---|---|---|---|---|---|
| Intervention Duration | |||||
| Total Cholesterol | |||||
| ≤4 weeks | −0.06 [−0.15, 0.03] | 0.22 | 48 | 20 | |
| >4 weeks | 0.07 [0.02, 0.11] | 0.002 a | 0 | 9 | |
| Overall | −0.03 [−0.09, 0.03] | 0.33 | 45 | 29 | 0.02 a |
| HDL Cholesterol | |||||
| ≤4 weeks | 0.07 [0.03, 0.12] | 0.002 | 30 | 20 | |
| >4 weeks | 0.03 [−0.02, 0.07] | 0.21 | 61 | 9 | |
| Overall | 0.05 [0.02, 0.09] | 0.002 | 52 | 29 | 0.16 |
| LDL Cholesterol | |||||
| ≤4 weeks | −0.08 [−0.16, 0.00] | 0.06 | 0 | 17 | |
| >4 weeks | 0.01 [−0.07, 0.09] | 0.83 | 38 | 8 | |
| Overall | −0.03 [−0.08, 0.03] | 0.32 | 22 | 25 | 0.13 |
| Triglycerides | |||||
| ≤4 weeks | −0.02 [−0.07, 0.04] | 0.56 | 0 | 19 | |
| >4 weeks | −0.03 [−0.09, 0.03] | 0.33 | 16 | 9 | |
| Overall | −0.02 [−0.06, 0.01] | 0.16 | 0 | 28 | 0.77 |
| Food Matrices | |||||
| Total Cholesterol | |||||
| Beverage | −0.05 [−0.17, 0.07] | 0.40 | 0 | 10 | |
| Chocolate | −0.04 [−0.15, 0.06] | 0.41 | 70 | 14 | |
| Beverage+Chocolate | −0.01 [−0.11, 0.08] | 0.79 | 0 | 5 | |
| Overall | −0.03 [−0.09, 0.03] | 0.33 | 45 | 29 | 0.86 |
| HDL Cholesterol | |||||
| Beverage | 0.11 [0.06, 0.17] | <0.001 | 0 | 10 | |
| Chocolate | 0.05 [−0.01, 0.11] | 0.10 | 67 | 14 | |
| Beverage+Chocolate | 0.02 [−0.01, 0.06] | 0.19 | 0 | 5 | |
| Overall | 0.05 [0.02, 0.09] | 0.002 | 52 | 29 | 0.03 |
| LDL Cholesterol | |||||
| Beverage | −0.07 [−0.19, 0.05] | 0.27 | 0 | 9 | |
| Chocolate | −0.04 [−0.14, 0.05] | 0.39 | 42 | 11 | |
| Beverage+Chocolate | −0.03 [−0.13, 0.07] | 0.58 | 12 | 5 | |
| Overall | −0.03 [−0.08, 0.03] | 0.32 | 22 | 25 | 0.10 |
| Triglycerides | |||||
| Beverage | 0.01 [−0.07, 0.10] | 0.75 | 0 | 9 | |
| Chocolate | −0.03 [−0.07, 0.01] | 0.12 | 0 | 14 | |
| Beverage+Chocolate | 0.01 [−0.23, 0.25] | 0.94 | 57 | 5 | |
| Overall | −0.02 [−0.06, 0.01] | 0.16 | 0 | 28 | 0.64 |
| Daily Dose of Polyphenols | |||||
| Total Cholesterol | |||||
| <500 mg | 0.08 [0.04, 0.12] | <0.001 a | 0 | 5 | |
| ≥500 mg | 0.10 [−0.07, 0.26] | 0.27 | 0 | 4 | |
| Overall | 0.08 [0.03, 0.12] | <0.001 a | 0 | 9 | 0.86 |
| HDL Cholesterol | |||||
| <500 mg | 0.06 [−0.04, 0.15] | 0.23 | 77 | 5 | |
| ≥500 mg | 0.02 [−0.07, 0.12] | 0.69 | 11 | 4 | |
| Overall | 0.04 [−0.02, 0.11] | 0.21 | 62 | 9 | 0.93 |
| LDL Cholesterol | |||||
| <500 mg | 0.06 [0.03, 0.10] | <0.001 a | 0 | 5 | |
| ≥500 mg | 0.00 [−0.16, 0.16] | 0.99 | 0 | 4 | |
| Overall | 0.06 [0.02, 0.10] | 0.001 a | 0 | 9 | 0.46 |
| Triglycerides | |||||
| <500 mg | −0.01 [−0.06, 0.03] | 0.52 | 0 | 5 | |
| ≥500 mg | −0.04 [−0.18, 0.10] | 0.55 | 0 | 4 | |
| Overall | −0.02 [−0.06, 0.02] | 0.42 | 0 | 9 | 0.71 |
| Daily Dose of Flavanols | |||||
| Total Cholesterol | |||||
| <900 mg | −0.08 [−0.21, 0.04] | 0.17 | 66 | 12 | |
| ≥900 mg | −0.11 [−0.37, 0.15] | 0.85 | 0 | 3 | |
| Overall | −0.08 [−0.19, 0.02] | 0.12 | 58 | 15 | 0.85 |
| HDL Cholesterol | |||||
| <900 mg | 0.05 [0.00, 0.10] | 0.04 | 37 | 12 | |
| ≥900 mg | 0.06 [−0.05, 0.16] | 0.27 | 0 | 3 | |
| Overall | 0.05 [0.01, 0.09] | 0.02 | 20 | 15 | 0.18 |
| LDL Cholesterol | |||||
| <900 mg | −0.05 [−0.16, 0.06] | 0.36 | 28 | 10 | |
| ≥900 mg | −0.12 [−0.38, 0.14] | 0.37 | 0 | 2 | |
| Overall | −0.06 [−0.15, 0.04] | 0.23 | 16 | 12 | 0.64 |
| Triglycerides | |||||
| <900 mg | −0.03 [−0.12, 0.05] | 0.45 | 26 | 12 | |
| ≥900 mg | −0.03 [−0.25, 0.19] | 0.80 | 0 | 2 | |
| Overall | −0.04 [−0.11, 0.04] | 0.34 | 7 | 14 | 0.97 |
| Daily Dose of Epicatechin | |||||
| Total Cholesterol | |||||
| <100 mg | −0.05 [−0.15, 0.04] | 0.26 | 70 | 14 | |
| ≥100 mg | −0.04 [−0.23, 0.15] | 0.71 | 0 | 4 | |
| Overall | −0.05 [−0.13, 0.03] | 0.25 | 63 | 18 | 0.86 |
| HDL Cholesterol | |||||
| <100 mg | 0.06 [0.01, 0.11] | 0.02 | 65 | 14 | |
| ≥100 mg | 0.12 [0.04, 0.19] | 0.002 | 0 | 4 | |
| Overall | 0.07 [0.02, 0.12] | 0.003 | 55 | 18 | 0.22 |
| LDL Cholesterol | |||||
| <100 mg | −0.05 [−0.14, 0.05] | 0.35 | 57 | 11 | |
| ≥100 mg | −0.15 [−0.33, 0.04] | 0.12 | 0 | 4 | |
| Overall | −0.06 [−0.14, 0.03] | 0.17 | 49 | 15 | 0.34 |
| Triglycerides | |||||
| <100 mg | −0.04 [−0.09, 0.02] | 0.20 | 26 | 14 | |
| ≥100 mg | 0.03 [−0.21, 0.27] | 0.79 | 0 | 3 | |
| Overall | −0.03 [−0.08, 0.02] | 0.19 | 13 | 17 | 0.58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amoah, I.; Lim, J.J.; Osei, E.O.; Arthur, M.; Cobbinah, J.C.; Tawiah, P. Effect of Cocoa Beverage and Dark Chocolate Intake on Lipid Profile in People Living with Normal and Elevated LDL Cholesterol: A Systematic Review and Meta-Analysis. Dietetics 2023, 2, 215-236. https://doi.org/10.3390/dietetics2030017
Amoah I, Lim JJ, Osei EO, Arthur M, Cobbinah JC, Tawiah P. Effect of Cocoa Beverage and Dark Chocolate Intake on Lipid Profile in People Living with Normal and Elevated LDL Cholesterol: A Systematic Review and Meta-Analysis. Dietetics. 2023; 2(3):215-236. https://doi.org/10.3390/dietetics2030017
Chicago/Turabian StyleAmoah, Isaac, Jia Jiet Lim, Emmanuel Ofori Osei, Michael Arthur, Jesse Charles Cobbinah, and Phyllis Tawiah. 2023. "Effect of Cocoa Beverage and Dark Chocolate Intake on Lipid Profile in People Living with Normal and Elevated LDL Cholesterol: A Systematic Review and Meta-Analysis" Dietetics 2, no. 3: 215-236. https://doi.org/10.3390/dietetics2030017
APA StyleAmoah, I., Lim, J. J., Osei, E. O., Arthur, M., Cobbinah, J. C., & Tawiah, P. (2023). Effect of Cocoa Beverage and Dark Chocolate Intake on Lipid Profile in People Living with Normal and Elevated LDL Cholesterol: A Systematic Review and Meta-Analysis. Dietetics, 2(3), 215-236. https://doi.org/10.3390/dietetics2030017