Real-World Analysis of the Safety and Effectiveness of Apixaban Therapy in Cancer Patients with Venous Thromboembolism in Saudi Arabia

 ,
,
Abstract
:1. Introduction
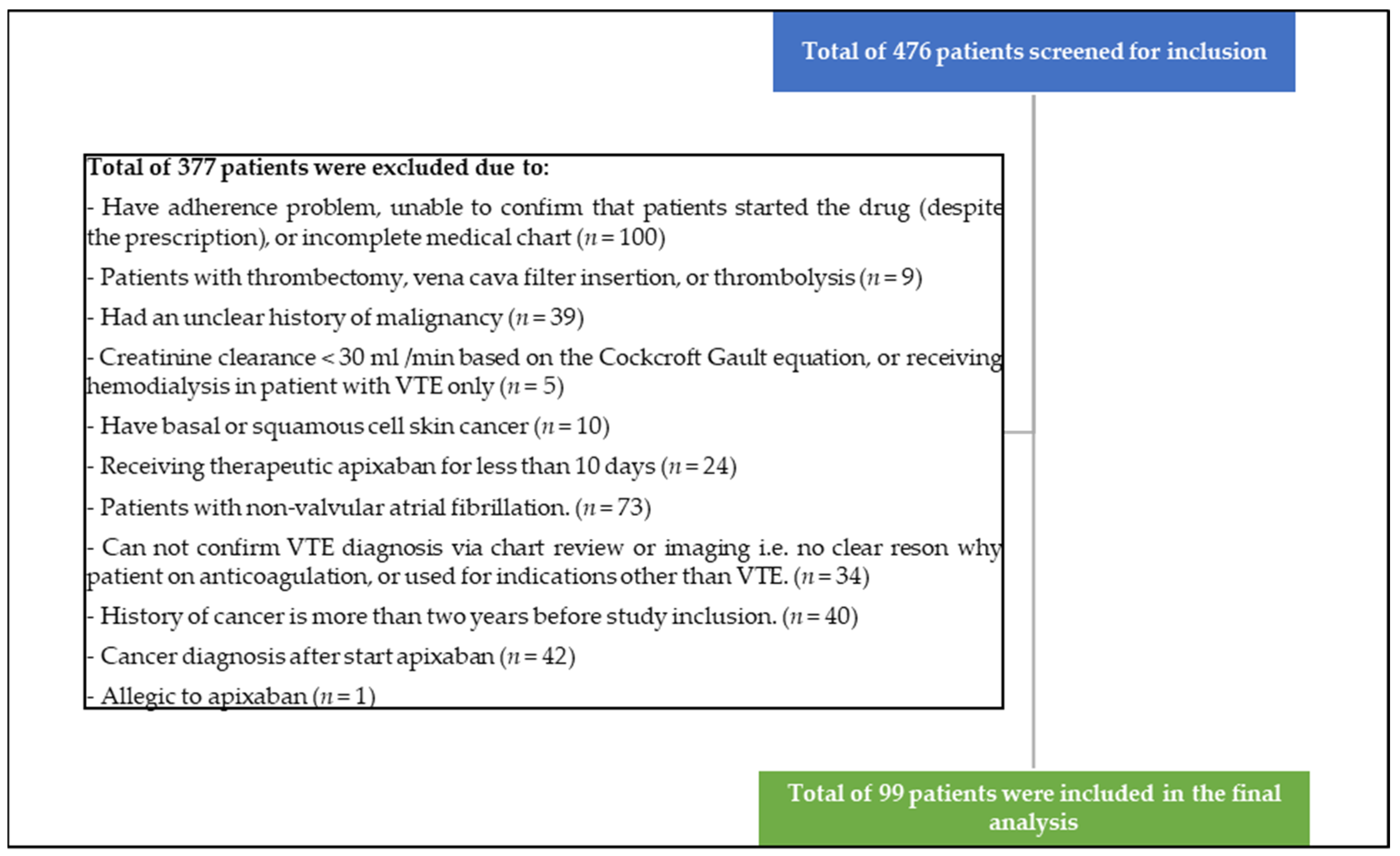
2. Materials and Methods
3. Results
3.1. Demographic and Clinical Characteristics
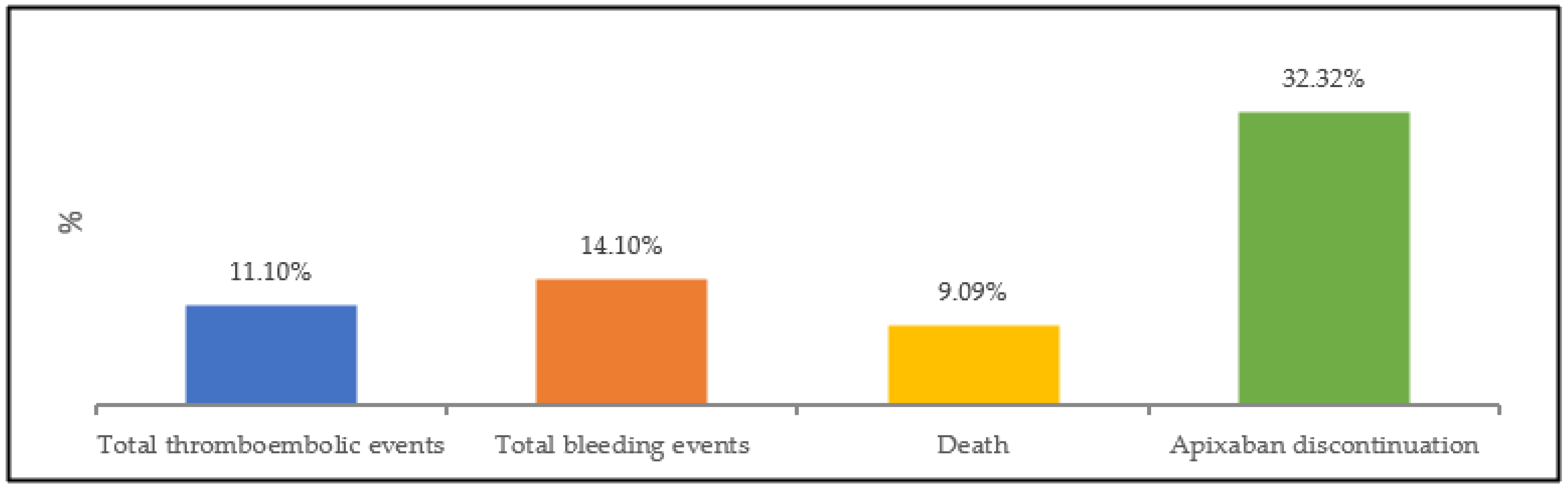
3.2. Thrombotic and Bleeding Events
3.3. Mortality and Apixaban Discontinuation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Streiff, M.B.; Holmstrom, B.; Angelini, D.; Ashrani, A.; Elshoury, A.; Fanikos, J.; Fertrin, K.Y.; Fogerty, A.E.; Gao, S.; Goldhaber, S.Z.; et al. Cancer-Associated Venous Thromboembolic Disease, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. (JNCCN) 2021, 19, 1181–1201. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, S.; Alfawzan, A.; Alswaidan, A.; Alkharaan, A.; Alabduljabar, M.; Khan, A.; Alzahrani, M. Anatomical sites and clinical characteristics of venous thromboembolism in a tertiary hospital. J. Appl. Hematol. 2020, 11, 126. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Cancer Investigators. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor with Low Molecular Weight Heparin in Patients with Cancer with Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- McBane, R.D., II; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. (JTH) 2020, 18, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Mulder, F.I.; Bosch, F.; Young, A.M.; Marshall, A.; McBane, R.D.; Zemla, T.J.; Carrier, M.; Kamphuisen, P.W.; Bossuyt, P.; Büller, H.R.; et al. Direct oral anticoagulants for cancer-associated venous thromboembolism: A systematic review and meta-analysis. Blood 2020, 136, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- McCormack, T.; Harrisingh, M.C.; Horner, D.; Bewley, S.; Guideline Committee. Venous thromboembolism in adults: Summary of updated NICE guidance on diagnosis, management, and thrombophilia testing. BMJ 2020, 369, m1565. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Carrier, M.; Ay, C.; Di Nisio, M.; Hicks, L.K.; Khorana, A.A.; Leavitt, A.D.; Lee, A.; Macbeth, F.; Morgan, R.L.; et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: Prevention and treatment in patients with cancer. Blood Adv. 2021, 5, 927–974. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.O.; Davis, K.A. Evaluation of Direct-Acting Oral Anticoagulant Use in Patients with Cancer. J. Pharm. Pract. 2018, 31, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Keshishian, A.; Lee, T.; Wygant, G.; Rosenblatt, L.; Hlavacek, P.; Mardekian, J.; Wiederkehr, D.; Sah, J.; Luo, X. Effectiveness and Safety of Apixaban, Low-Molecular-Weight Heparin, and Warfarin among Venous Thromboembolism Patients with Active Cancer: A U.S. Claims Data Analysis. Thromb. Haemost. 2021, 121, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Yamada, N.; Mo, M.; Ohsawa, A.; Sato, M.; Umeyama, M.; Shima, D.; Nakamura, M. Safety and Effectiveness of Apixaban in Japanese Patients with Venous Thromboembolism in Clinical Practice- A Post-Marketing Surveillance. Circ. J. Off. J. Jpn. Circ. Soc. 2021, 85, 2201–2207. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age, years, (Mean, SD) | 58.59 (14.77) |
| Female Sex, (n, %) | 38 (38.4%) |
| Creatinine clearance category (n, %) * | |
| 30–50 mL/min | 14 (14.1%) |
| >50 mL/min | 85 (85.9%) |
| Platelets count category, (n, %) | |
| <100 × 109/L | 4 (4.0%) |
| 100–349 × 109/L | 67 (67.7%) |
| >349 × 109/L | 28 (28.3%) |
| Hemoglobin < 10 g/dL, (n, %) | 33 (33.3%) |
| Body Mass Index category, (n, %) | |
| <18.5 kg/m2 | 5 (5.1%) |
| 18.5–24.9 kg/m2 | 32 (32.3%) |
| 25–29.9 kg/m2 | 22 (22.2%) |
| >29.9 kg/m2 | 40 (40.4%) |
| Appropriate dose at baseline (n, %) | 79 (79.8%) |
| ECOG performance status category (n, %) | |
| 0 | 8 (8.33%) |
| 1 | 11 (11.5%) |
| 2 | 10 (10.4%) |
| ≧3 | 12 (12.5%) |
| Unknown | 55 (57.3%) |
| Active cancer (n, %) | 96 (97.0%) |
| Type of cancer (n, %) | |
| Solid tumor | 74 (77.1%) |
| Hematological malignancy | 22 (22.9%) |
| Recurrent locally advance or metastatic Cancer (n, %) | 69 (71.9%) |
| Qualifying diagnosis of venous thromboembolism (n, %) | |
| Proximal DVT | 36 (36.4%) |
| Distal DVT | 2 (2.0%) |
| Proximal and distal DVT | 2 (2.0%) |
| Segmental PE | 19 (19.2%) |
| Subsegmental PE | 6 (6.1%) |
| Subsegmental & Segmental PE | 10 (10.1%) |
| Proximal DVT & Segmental PE | 5 (5.1%) |
| Splanchnic (SPVT) | 9 (9.1%) |
| Superficial (SVT) | 1 (1.0%) |
| Proximal DVT & Subsegmental PE | 1 (1.0%) |
| RV thrombus | 1 (1.0%) |
| SVC thrombus | 1 (1.0%) |
| Unknown | 3 (3.0%) |
| Superficial (SVT) and unknown type of PE | 1 (1.0%) |
| Proximal DVT and unknown type of PE | 1 (1.0%) |
| Proximal DVT + SPVT + Segmental PE | 1 (1.0%) |
| Medical history (n, %) | |
| Hypertension | 37 (37.4%) |
| Diabetes mellitus | 36 (36.4%) |
| Heart failure | 6 (6.1%) |
| Prior ischemic stroke, TIA or MI | 13 (13.1%) |
| History of mycardial infarction, peripheral artery disease, aortic plaque | 2 (2.0%) |
| Prior gastrointistinal bleed | 10 (10.1%) |
| Type of Cancer | ||
|---|---|---|
| Solid tumor | Number | % |
| Colorectal | 13 | 13.5% |
| Lung | 3 | 3.1% |
| Breast | 15 | 15.6% |
| Genitourinary | 7 | 7.3% |
| Gynecological | 15 | 15.6% |
| Pancreatic or hepatobiliary | 10 | 10.4% |
| Upper gastrointestinal | 3 | 3.1% |
| Head and neck | 2 | 2.1% |
| Bone/Soft tissue | 5 | 5.2% |
| Other solid tumor | 1 | 1.0% |
| Hematological malignancy | Number | % |
| Multiple myeloma | 7 | 7.3% |
| Non-Hodgkin lymphoma | 9 | 9.4% |
| Hodgkin lymphoma | 3 | 3.1% |
| Acute leukemia | 1 | 1.0% |
| Chronic leukemia | 1 | 1.0% |
| Other hematological | 1 | 1.0% |
| Therapy while on apixaban | ||
| Anti-Cancer Agents | Number | % |
| Alkylating agents | 49 | 51.0% |
| Antimetabolites | 37 | 38.5% |
| Monoclonal antibodies | 32 | 33.3% |
| Anti-Androgens | 2 | 2.1% |
| Aromatase Inhibitor | 4 | 4.2% |
| Cyclin-Dependent Kinase Inhibitor | 1 | 1.0% |
| Taxanes | 17 | 17.7% |
| Hormonal therapy | 1 | 1.0% |
| Topoisomerase inhibitors | 12 | 12.5% |
| PARP Inhibitor | 1 | 1.0% |
| Anthracyclines | 15 | 15.6% |
| Vinca alkaloids | 11 | 11.5% |
| Kinase inhibitors | 4 | 4.2% |
| Immunomodulating agents | 6 | 6.3% |
| Proteasome inhibitors | 2 | 2.1% |
| Antitumor antibiotics | 4 | 4.2% |
| All-trans retinoic acid | 1 | 1.0% |
| Arsenic Trioxide | 1 | 1.0% |
| Radiation | 14 | 14.6% |
| Radiation and Anti-cancer | 11 | 11.5% |
| Other Therapy | Number | % |
| NSAID | 17 | 17.2% |
| Clopidogrel | 3 | 3.0% |
| Prior use of anticoagulation therapy | 71 | 71.7% |
| Outcome | Number | % |
|---|---|---|
| Primary efficacy outcome | ||
| Total thromboembolic events | 11 | 11.1% |
| Type of thromboembolic events | ||
| Stroke | 1 | 9.1% |
| PE | 4 | 40.0% |
| DVT | 4 | 40.0% |
| Other VTE | 1 | 10.0% |
| Thromboembolic events Sub-Type | ||
| Hemorrhagic stroke | 1 | 9.1% |
| Segmental PE | 3 | 27.3% |
| Subsegmental & Segmental PE | 1 | 9.1% |
| Proximal DVT | 4 | 36.4% |
| Superficial (SVT) | 1 | 9.1% |
| Onset of VTE since apixaban initiation | ||
| within 0–3 months | 7 | 63.6% |
| 3–6 months | 3 | 27.3% |
| Primary safety outcome | ||
| Total bleeding events | 14 | 14.1% |
| Type of bleed events | ||
| Major bleed | 3 | 21.4% |
| Clinically relevant non major bleed | 8 | 57.1% |
| Clinically NON relevant non major bleed | 3 | 21.4% |
| Bleeding Location: | ||
| Fatal | 1 | 7.1% |
| Abdominal | 1 | 7.1% |
| Cutaneous | 1 | 7.1% |
| Hematuria | 4 | 28.6% |
| Upper airways | 1 | 7.1% |
| Upper GI | 3 | 21.4% |
| Lower GI | 1 | 7.1% |
| Undetermined site | 1 | 7.1% |
| Stoma | 1 | 7.1% |
| Mortality | ||
| Death | 9 | 9.09% |
| Reason of death: | ||
| Cancer related | 5 | 55.6% |
| Cardiovascular related | 1 | 11.1% |
| Other | 2 | 22.2% |
| Unknown reason | 1 | 11.1% |
| Apixaban discontinuation | 32 | 32.32% |
| Reasons of Apixaban discontinuation: | ||
| Thrombosis or bleed event | 12 | 12.1% |
| Death | 7 | 7.1% |
| Thrombocytopenia | 2 | 2.0% |
| High bleeding risk | 1 | 1.0% |
| Unknown reason | 4 | 4.0% |
| Completed VTE treatment duration | 4 | 4.0% |
| Suspect thrombosis or bleed event | 2 | 2.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alabdelmuhsin, L.; Alwethairi, M.; Almadani, O.; Althunian, T.A.; Badreldin, H.A. Real-World Analysis of the Safety and Effectiveness of Apixaban Therapy in Cancer Patients with Venous Thromboembolism in Saudi Arabia. J. Vasc. Dis. 2023, 2, 102-111. https://doi.org/10.3390/jvd2010008
Alabdelmuhsin L, Alwethairi M, Almadani O, Althunian TA, Badreldin HA. Real-World Analysis of the Safety and Effectiveness of Apixaban Therapy in Cancer Patients with Venous Thromboembolism in Saudi Arabia. Journal of Vascular Diseases. 2023; 2(1):102-111. https://doi.org/10.3390/jvd2010008
Chicago/Turabian StyleAlabdelmuhsin, Lolwa, Metab Alwethairi, Ohoud Almadani, Turki A. Althunian, and Hisham A. Badreldin. 2023. "Real-World Analysis of the Safety and Effectiveness of Apixaban Therapy in Cancer Patients with Venous Thromboembolism in Saudi Arabia" Journal of Vascular Diseases 2, no. 1: 102-111. https://doi.org/10.3390/jvd2010008
APA StyleAlabdelmuhsin, L., Alwethairi, M., Almadani, O., Althunian, T. A., & Badreldin, H. A. (2023). Real-World Analysis of the Safety and Effectiveness of Apixaban Therapy in Cancer Patients with Venous Thromboembolism in Saudi Arabia. Journal of Vascular Diseases, 2(1), 102-111. https://doi.org/10.3390/jvd2010008