
Paraneoplastic Syndromes in Hodgkin’s Lymphoma


Abstract
:1. Introduction
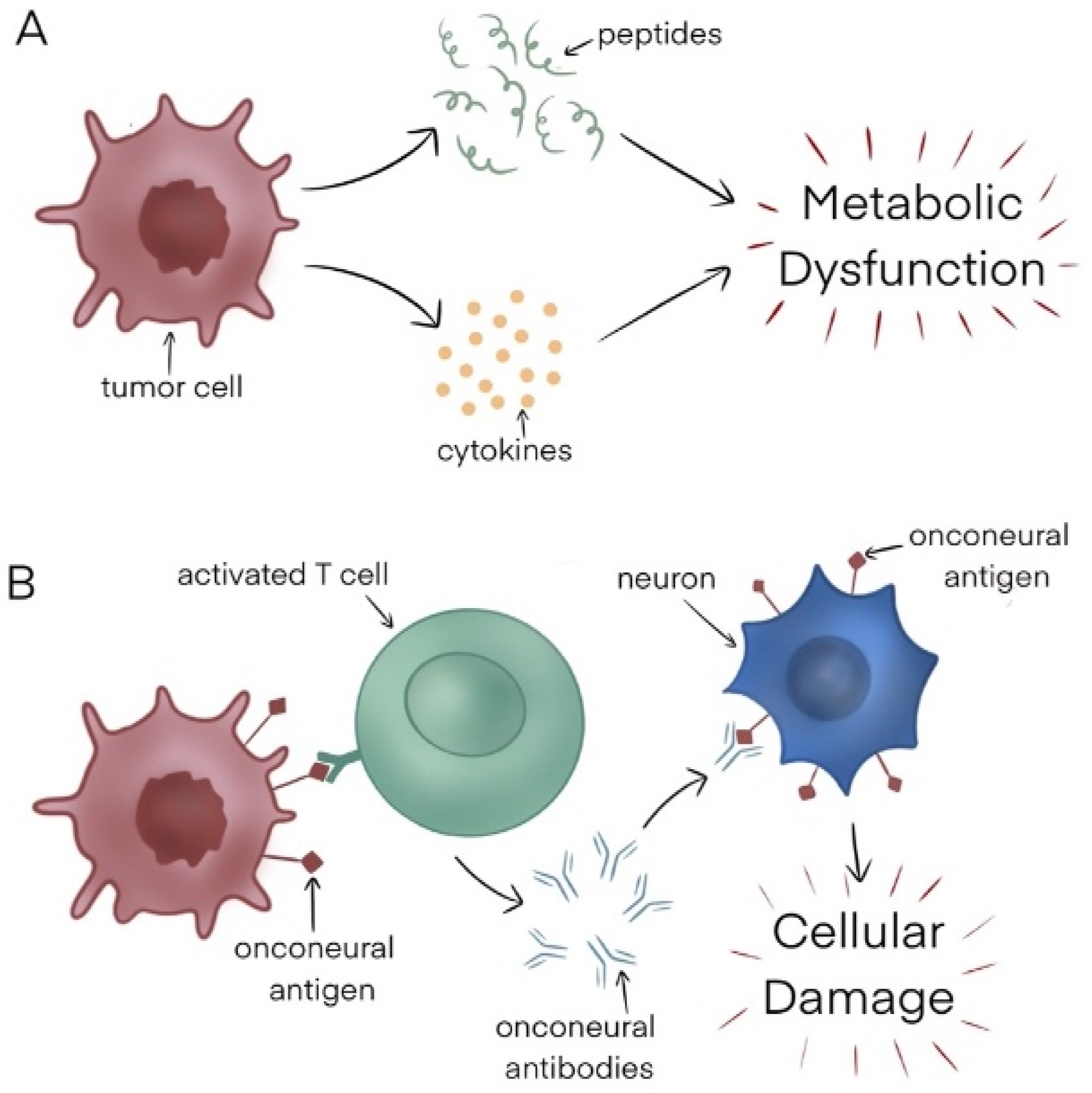
2. General Overview of Paraneoplastic Syndromes and Pathophysiology
3. Paraneoplastic Syndromes in Hodgkin Lymphoma by System
3.1. Neurological Syndromes
3.1.1. Cerebellar Degeneration
3.1.2. Limbic Encephalitis (LE)
3.1.3. Granulomatous Angiitis of the Central Nervous System
3.2. Hepatic Syndromes
3.2.1. Vanishing Bile Duct Syndrome (VBDS)
3.2.2. Paraneoplastic Intrahepatic Cholestasis
3.3. Renal Syndromes
3.4. Dermatological Syndromes
3.4.1. Eczematous Eruptions
3.4.2. Paraneoplastic Pemphigus (PNP)
3.5. Other Hematological Syndromes
Autoimmune Cytopenias (AICs)
3.6. Miscellaneous Paraneoplastic Arthritis
4. Challenges and Future Directions
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaseb, H.; Babiker, H.M. Hodgkin Lymphoma; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Graus, F.; Ariño, H.; Dalmau, J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood 2014, 123, 3230–3238. [Google Scholar] [CrossRef]
- Pelosof, L.C.; Gerber, D.E. Paraneoplastic Syndromes: An approach to diagnosis and treatment. Mayo Clin. Proc. 2010, 85, 838–854. [Google Scholar] [CrossRef] [PubMed]
- Surveillance, Epidemiology, and End Results (SEER) Program Populations. Available online: https://seer.cancer.gov/statfacts/html/hodg.html (accessed on 9 October 2023).
- El Fakih, R.; Bajuaifer, Y.S.; Shah, A.Y.; Sulaiman, R.; Almohamady, R.; Elgohary, G.; Alothaimeen, H.S.; Aljurf, M. Paraneoplastic syndromes associated with classic Hodgkin lymphoma, a systematic literature review. Ann. Hematol. 2023, 102, 1–7. [Google Scholar] [CrossRef] [PubMed]
- de Celis Ferrari, A.C.R.; Glasberg, J.; Riechelmann, R.P. Carcinoid syndrome: Update on the pathophysiology and treatment. Clinics 2018, 73 (Suppl. S1), e490s. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Gigli, G.L.; Segatti, S.; Corazza, E.; Marini, A.; Bernardini, A.; Valent, F.; Fabris, M.; Curcio, F.; Brigo, F.; et al. Epidemiology of paraneoplastic neurological syndromes: A population-based study. J. Neurol. 2020, 267, 26–35. [Google Scholar] [CrossRef]
- Hébert, J.; Riche, B.; Vogrig, A.; Muñiz-Castrillo, S.; Joubert, B.; Picard, G.; Rogemond, V.; Psimaras, D.; Alentorn, A.; Berzero, G.; et al. Epidemiology of paraneoplastic neurologic syndromes and autoimmune encephalitides in France. Neurol.-Neuroimmunol. Neuroinflammation 2020, 7, e883. [Google Scholar] [CrossRef]
- Graus, F.; Vogrig, A.; Muñiz-Castrillo, S.; Antoine, J.-C.G.; Desestret, V.; Dubey, D.; Giometto, B.; Irani, S.R.; Joubert, B.; Leypoldt, F.; et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurol.-Neuroimmunol. Neuroinflammation 2021, 8, e1014. [Google Scholar] [CrossRef]
- Nayak, L.; Batchelor, T.T. How I treat neurologic complications in patients with lymphoid cancer. Blood 2022, 139, 1469–1478. [Google Scholar] [CrossRef]
- Trotter, J.L.; Hendin, B.A.; Osterland, C.K. Cerebellar degeneration with hodgkin disease: An immunological study. Arch. Neurol. 1976, 33, 660–661. [Google Scholar] [CrossRef] [PubMed]
- Marsili, L.; Marcucci, S.; LaPorta, J.; Chirra, M.; Espay, A.J.; Colosimo, C. Paraneoplastic Neurological Syndromes of the Central Nervous System: Pathophysiology, Diagnosis, and Treatment. Biomedicines 2023, 11, 1406. [Google Scholar] [CrossRef] [PubMed]
- Loehrer, P.A.; Zieger, L.; Simon, O.J. Update on Paraneoplastic Cerebellar Degeneration. Brain Sci. 2021, 11, 1414. [Google Scholar] [CrossRef]
- Campana, I.G.; Silva, G.D. Anti-Tr/DNER Antibody–Associated Cerebellar Ataxia: A Systematic Review. Cerebellum 2022, 21, 1085–1091. [Google Scholar] [CrossRef]
- Greene, M.; Lai, Y.; Baella, N.; Dalmau, J.; Lancaster, E. Antibodies to Delta/notch-like epidermal growth factor-related receptor in patients with anti-Tr, paraneoplastic cerebellar degeneration, and Hodgkin lymphoma. JAMA Neurol. 2014, 71, 1003–1008. [Google Scholar] [CrossRef]
- Christensen, P.B.; Gregersen, H.; Almasi, C. Anti-Tr/DNER antibody paraneoplastic cerebellar degeneration preceding a very late relapse of Hodgkin Lymphoma after 12 years. Cerebellum Ataxias 2021, 8, 14. [Google Scholar] [CrossRef]
- Galli, J.; Greenlee, J. Paraneoplastic Diseases of the Central Nervous System. F1000Research 2020, 9, 167. [Google Scholar] [CrossRef] [PubMed]
- Smitt, P.S.; Kinoshita, A.; De Leeuw, B.; Moll, W.; Coesmans, M.; Jaarsma, D.; Henzen-Logmans, S.; Vecht, C.; De Zeeuw, C.; Sekiyama, N.; et al. Paraneoplastic cerebellar ataxia due to autoantibodies against a glutamate receptor. N. Engl. J. Med. 2000, 342, 21–27. [Google Scholar] [CrossRef]
- Miske, R.; Scharf, M.; Stark, P.; Dietzel, H.; Bien, C.I.; Borchers, C.; Kermer, P.; Ott, A.; Denno, Y.; Rochow, N.; et al. Autoantibodies Against the Purkinje Cell Protein RGS8 in Paraneoplastic Cerebellar Syndrome. Neurol.-Neuroimmunol. Neuroinflammation 2021, 8, e987. [Google Scholar] [CrossRef] [PubMed]
- Arratibel, N.; Sobejano, E.; Moran, J.C.; Diaz, L.G.; Blázquez, A.; Baile, M.; Veiga, Á.; Caballero, M.D.; García-Sanz, R. A Case of Paraneoplastic Cerebellar Degeneration that Preceded the Diagnosis of Classical Hodgkin’s Lymphoma by 16 Months. Am. J. Case Rep. 2020, 21, e922342-1–e922342-5. [Google Scholar] [CrossRef] [PubMed]
- Bernal, F.; Shams’Ili, S.; Rojas-Marcos, I.; Sanchez-Valle, R.; Saiz, A.; Dalmau, J.; Honnorat, J.; Sillevis Smitt, P.S.; Graus, F. Anti-Tr antibodies as markers of paraneoplastic cerebellar degeneration and Hodgkin’s disease. Neurology 2003, 60, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Hammack, J.; Kotanides, H.; Rosenblum, M.K.; Posner, J.B. Paraneoplastic cerebellar degeneration. II. Clinical and immunologic findings in 21 patients with Hodgkin’s disease. Neurology 1992, 42, 1938–1943. [Google Scholar] [PubMed]
- Chepovetsky, J.; Duffield, A.S.; Pu, J.J. Paraneoplastic cerebellar degeneration as an early sign of classical Hodgkin lymphoma. Ann. Hematol. 2016, 95, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Rosenfeld, M.R. Paraneoplastic syndromes of the CNS. Lancet Neurol. 2008, 7, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.-C.; Lin, M.-I.; Weng, W.-C.; Lee, W.-T. Neuropsychiatric Disorders Due to Limbic Encephalitis: Immunologic Aspect. Int. J. Mol. Sci. 2020, 22, 389. [Google Scholar] [CrossRef] [PubMed]
- Soto-Rincón, C.A.; Castillo-Torres, S.A.; Cantú-García, D.A.; Estrada-Bellmann, I.; Chávez-Luévanos, B.; Marfil, A. The poor insane Ophelia: Reconsidering Ophelia syndrome. Arq. Neuro-Psiquiatria 2019, 77, 828–831. [Google Scholar] [CrossRef]
- Madhavan, A.A.; Carr, C.M.; Morris, P.P.; Flanagan, E.P.; Kotsenas, A.L.; Hunt, C.H.; Eckel, L.J.; Lindell, E.P.; Diehn, F.E. Imaging Review of Paraneoplastic Neurologic Syndromes. Am. J. Neuroradiol. 2020, 41, 2176–2187. [Google Scholar] [CrossRef]
- Zrzavy, T.; Höftberger, R.; Wimmer, I.; Berger, T.; Rommer, P.; Macher, S. Longitudinal CSF Findings in Autoimmune Encephalitis—A Monocentric Cohort Study. Front. Immunol. 2021, 12, 646940. [Google Scholar] [CrossRef]
- Briani, C.; Vitaliani, R.; Grisold, W.; Honnorat, J.; Graus, F.; Antoine, J.; Bertolini, G.; Giometto, B.; Euronetwork, F.T.P. Spectrum of paraneoplastic disease associated with lymphoma. Neurology 2011, 76, 705–710. [Google Scholar] [CrossRef]
- Suri, V.; Jadhao, N.; Khan, N.; Gupta, R. Paraneoplastic cerebellar degeneration in Hodgkin′s lymphoma. Ann. Indian Acad. Neurol. 2012, 15, 205–207. [Google Scholar] [CrossRef]
- Ypma, P.F.; Wijermans, P.W.; Koppen, H.; Smitt, P.A.E.S. Paraneoplastic cerebellar degeneration preceding the diagnosis of Hodgkin’s lymphoma. Neth. J. Med. 2006, 64, 243–247. [Google Scholar]
- Shams’ili, S.; Grefkens, J.; de Leeuw, B.; van den Bent, M.; Hooijkaas, H.; van der Holt, B.; Vecht, C.; Sillevis Smitt, P. Paraneoplastic cerebellar degeneration associated with antineuronal antibodies: Analysis of 50 patients. Brain 2003, 126, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Spyridonidis, A.; Fischer, K.-G.; Glocker, F.X.; Fetscher, S.; Klisch, J.; Behringer, D. Paraneoplastic cerebellar degeneration and nephrotic syndrome preceding Hodgkin’s disease: Case report and review of the literature. Eur. J. Haematol. 2002, 68, 318–321. [Google Scholar] [CrossRef]
- Lancaster, E.; Martinez-Hernandez, E.; Titulaer, M.; Boulos, M.; Weaver, S.; Antoine, J.-C.; Liebers, E.; Kornblum, C.; Bien, C.; Honnorat, J.; et al. Antibodies to metabotropic glutamate receptor 5 in the Ophelia syndrome. Neurology 2011, 77, 1698–1701. [Google Scholar] [CrossRef]
- Zandi, M.S.; Irani, S.R.; Follows, G.; Moody, A.M.; Molyneux, P.; Vincent, A. Limbic encephalitis associated with antibodies to the NMDA receptor in Hodgkin lymphoma. Neurology 2009, 73, 2039–2040. [Google Scholar] [CrossRef] [PubMed]
- Kung, S.; Mueller, P.S.; Geda, Y.E.; Krahn, L.E. Delirium Resulting from Paraneoplastic Limbic Encephalitis Caused by Hodgkin’s Disease. Psychosomatics 2002, 43, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Hentschke, S.; Malzfeldt, E.; Salwender, H.J.; Braumann, D.; Stang, A.; Hentschke, M. Hu-antibody positive limbic encephalitis in a patient with Hodgkin lymphoma. Leuk. Lymphoma 2008, 49, 2374–2376. [Google Scholar] [CrossRef] [PubMed]
- Bernard, P.; Vinzio, S.; Talarmin, F.; Kadouri, A.; Flocard, F. Hodgkin’s disease manifesting as paraneoplastic limbic encephalitis. Rev. Med. Interne 2003, 24, 257–260. [Google Scholar] [CrossRef]
- Deodhare, S.; O’connor, P.; Ghazarian, D.; Bilbao, J.M. Paraneoplastic Limbic Encephalitis in Hodgkin’s Disease. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 1996, 23, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, T.; Gärtner, J.; Körholz, D.; Janßen, G.; Schneider, D.; Engelbrecht, V.; Göbel, U.; Lenard, H.-G. Paraneoplastic limbic encephalitis in two teenage girls. Neuropediatrics 1998, 29, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Duyckaerts, C.; Derouesne, C.; Signoret, J.L.; Gray, F.; Escourolle, R.; Castaigne, P. Bilateral and limited amygdalohippocampal lesions causing a pure amnesic syndrome. Ann. Neurol. 1985, 18, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Pfliegler, G.; Pósán, E.; Glaub, D.; Telek, B.; Rak, K. Hodgkin’s disease and memory loss: Another case of the ophelia syndrome. Br. J. Haematol. 1990, 74, 232. [Google Scholar] [CrossRef]
- Borellini, L.; Lanfranconi, S.; Bonato, S.; Trezzi, I.; Franco, G.; Torretta, L.; Bresolin, N.; Di Fonzo, A.B. Progressive Encephalomyelitis with Rigidity and Myoclonus Associated with Anti-GlyR Antibodies and Hodgkin’s Lymphoma: A Case Report. Front. Neurol. 2017, 8, 401. [Google Scholar] [CrossRef]
- Kanaparthi, S.; Aroor, S.; Mundkur, S.C.; Shashidhara, S.; Reddy, K.V. Alopecia Areata and Demyelination as Paraneoplastic Manifestation in Paediatric Hodgkin’s Lymphoma. Int. J. Hematol. Oncol. Stem Cell Res. 2018, 12, 98–102. [Google Scholar]
- Al, I.O.; Koç, B.; Bayram, C.; Paslı, E.U.; Yıldız, E.P.; Ayçiçek, A.; Çalışkan, M.; Özdemir, G.N. Variant Guillain-Barré syndrome in a patient with Hodgkin lymphoma: AMSAN. Turk. Arch. Pediatr. 2018, 53, 263–266. [Google Scholar] [CrossRef]
- Anderson, D.; Beecher, G.; Steve, T.A.; Jen, H.; Camicioli, R.; Zochodne, D.W. Neurological Nuance: Hodgkin lymphoma presenting with Guillain-BarrÉ syndrome. Muscle Nerve 2017, 55, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Milanesio, M.; Vera, S.; Sturich, A.G.; Guanchiale, L.A.; Basquiera, A.L. Hodgkin’s lymphoma: Sensitive and autonomic neuropathy as a paraneoplastic manifestation. Medicina 2023, 83, 484–488. [Google Scholar]
- Flanagan, E.P.; Sandroni, P.; Pittock, S.J.; Inwards, D.J.; Jones, L.K. Paraneoplastic lower motor neuronopathy associated with Hodgkin lymphoma. Muscle Nerve 2012, 46, 823–827. [Google Scholar] [CrossRef]
- Johnson, M.; Maciunas, R.; Dutt, P.; Clinton, M.E.; Collins, R. Granulomatous angiitis masquerading as a mass lesion. Magnetic resonance imaging and stereotactic biopsy findings in a patient with occult Hodgkin’s disease. Surg. Neurol. 1989, 31, 49–53. [Google Scholar] [CrossRef]
- Lopez-Chiriboga, A.S.; Yoon, J.W.; Siegel, J.L.; Harriott, A.M.; Pirris, S.; Eidelman, B.H.; Freeman, W.D. Granulomatous Angiitis of the Central Nervous System Associated with Hodgkin’s Lymphoma: Case Report and Literature Review. J. Stroke Cerebrovasc. Dis. 2018, 27, e5–e8. [Google Scholar] [CrossRef]
- Delobel, P.; Brassat, D.; Danjoux, M.; Lotterie, J.-A.; Irsutti-Fjørtoft, M.; Clanet, M.; Laurent, G. Granulomatous angiitis of the central nervous system revealing Hodgkin’s disease. J. Neurol. 2004, 251, 611–612. [Google Scholar] [CrossRef] [PubMed]
- Valappil, A.; Nair, R.R.; Madhusoodhanan, S.; Narendran, A. Rhombencephalomyelitis due to possible paraneoplastic syndrome associated with Hodgkin’s lymphoma. BMJ Case Rep. 2022, 15, e249089. [Google Scholar] [CrossRef]
- Ballonoff, A.; Kavanagh, B.; Nash, R.; Drabkin, H.; Trotter, J.; Costa, L.; Rabinovitch, R. Hodgkin lymphoma-related vanishing bile duct syndrome and idiopathic cholestasis: Statistical analysis of all published cases and literature review. Acta Oncol. 2008, 47, 962–970. [Google Scholar] [CrossRef]
- Scalabrini, D.R.; Caravelli, D.; Schianca, F.C.; D’ambrosio, L.; Tolomeo, F.; Boccone, P.; Manca, A.; De Rosa, G.; Nuzzo, A.; Aglietta, M.; et al. Complete remission of paraneoplastic vanishing bile duct syndrome after the successful treatment of Hodgkin’s lymphoma: A case report and review of the literature. BMC Res. Notes 2014, 7, 529. [Google Scholar] [CrossRef]
- Iturriagagoitia, A.C.; Bastarrica, M.I.; de Equiza, E.P.; Urmeneta, J.M.Z.; Martínez-Peñuela, J.M.; Pérez, R.B. Ductal regeneration in vanishing bile duct syndrome in Hodgkin’s lymphoma. Gastroenterol. Hepatol. 2005, 28, 275–278. [Google Scholar]
- Crosbie, O.M.; Crown, J.P.; Nolan, N.P.; Murray, R.; Hegarty, J.E. Resolution of paraneoplastic bile duct paucity following successful treatment of Hodgkin’s disease. Hepatology 1997, 26, 5–8. [Google Scholar] [CrossRef]
- Yalçın, S.; Kars, A.; Sökmensüer, C.; Atahan, L. Extrahepatic Hodgkin’s Disease with Intrahepatic Cholestasis: Report of Two Cases. Oncology 1999, 57, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Ripoll, C.; Carretero, L.; Sabin, P.; Alvarez, E.; Marrupe, D.; Banares, R. Idiopathic cholestasis associated with progressive ductopenia in two patients with hodgkin’s disease. Gastroenterol. Hepatol. 2002, 25, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Barta, S.K.; Yahalom, J.; Shia, J.; Hamlin, P.A. Idiopathic cholestasis as a paraneoplastic phenomenon in Hodgkin’s lymphoma. Clin. Lymphoma Myeloma Leuk. 2006, 7, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Leeuwenburgh, I.; Lugtenburg, E.P.; van Buuren, H.R.; Zondervan, P.E.; de Man, R.A. Severe jaundice, due to vanishing bile duct syndrome, as presenting symptom of Hodgkin’s lymphoma, fully reversible after chemotherapy. Eur. J. Gastroenterol. Hepatol. 2008, 20, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Pass, A.K.; McLin, V.A.; Rushton, J.R.; Kearney, D.L.; Hastings, C.A.; Margolin, J.F. Vanishing bile duct syndrome and hodgkin disease: A case series and review of the literature. J. Pediatr. Hematol. Oncol. 2008, 30, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.-M.; Chang, C.-S.; Wu, C.-C.; Yin, H.-L. Hodgkin’s lymphoma-related vanishing bile duct syndrome: A case report and literature review. Kaohsiung J. Med. Sci. 2013, 29, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Anugwom, C.; Goetz, G.; Hassan, M. Vanishing Bile Duct Syndrome Preceding the Diagnosis of Hodgkin Lymphoma. ACG Case Rep. J. 2020, 7, e00336. [Google Scholar] [CrossRef]
- Papakonstantinou, I.; Kosmidou, M.; Papathanasiou, K.; Koumpis, E.; Kapsali, E.; Milionis, H.; Vassilakopoulos, T.P.; Papoudou-Bai, A.; Hatzimichael, E. Paraneoplastic Intrahepatic Cholestasis in Supradiaphragmatic Classical Hodgkin Lymphoma Successfully Treated with Brentuximab Vedotin: A Case Report and Review of the Literature. In Vivo 2021, 35, 1951–1957. [Google Scholar] [CrossRef]
- Sfrijan, D.; Tieranu, I.; Necula, I.; Popa, L.; Balgradean, M. Nephrotic Syndrome, Paraneoplastic Syndrome Associated to Hodgkin Lymphoma. Maedica 2016, 11, 64–67. [Google Scholar]
- Mallouk, A.; Pham, P.-C.T. Concurrent FSGS and Hodgkin’s lymphoma: Case report and literature review on the link between nephrotic glomerulopathies and hematological malignancies. Clin. Exp. Nephrol. 2006, 10, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Audard, V.; Larousserie, F.; Grimbert, P.; Abtahi, M.; Sotto, J.-J.; Delmer, A.; Boue, F.; Nochy, D.; Brousse, N.; Delarue, R.; et al. Minimal change nephrotic syndrome and classical Hodgkin’s lymphoma: Report of 21 cases and review of the literature. Kidney Int. 2006, 69, 2251–2260. [Google Scholar] [CrossRef]
- Gagliano, R.G.; Costanzi, J.J.; Beathard, G.A.; Sarles, H.E.; Bell, J.D. The nephrotic syndrome associated with neoplasia: An unusual paraneoplastic syndrome. Report of a case and review of the literature. Am. J. Med. 1976, 60, 1026–1031. [Google Scholar] [CrossRef]
- Lien, Y.-H.H.; Lai, L.-W. Pathogenesis, diagnosis and management of paraneoplastic glomerulonephritis. Nat. Rev. Nephrol. 2011, 7, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.P.; Krzesinski, J.-M.; Launay-Vacher, V.; Sprangers, B. Onco-nephrology: Core Curriculum 2015. Am. J. kidney Dis. Off. J. Natl. Kidney Found. 2015, 66, 869–883. [Google Scholar] [CrossRef]
- Nagaharu, K.; Sugimoto, Y.; Kawakami, K. A Rare Case of Immunotactoid Glomerulopathy Associated with Hodgkin Lymphoma. Case Rep. Nephrol. 2021, 2021, 5527966. [Google Scholar] [CrossRef] [PubMed]
- Jonkers, J.; Weening, J.J.; van der Valk, M.; Bobeldijk, R.; Berns, A. Overexpression of Frat1 in transgenic mice leads to glomerulosclerosis and nephrotic syndrome, and provides direct evidence for the involvement of Frat1 in lymphoma progression. Oncogene 1999, 18, 5982–5990. [Google Scholar] [CrossRef]
- Doussis-Anagnostopoulou, I.A.; Talks, K.L.; Turley, H.; Debnam, P.; Tan, D.C.; Mariatos, G.; Gorgoulis, V.; Kittas, C.; Gatter, K.C. Vascular endothelial growth factor (VEGF) is expressed by neoplastic Hodgkin–Reed–Sternberg cells in Hodgkin’s disease. J. Pathol. 2002, 197, 677–683. [Google Scholar] [CrossRef]
- Newcom, S.R.; Gu, L. Transforming growth factor beta 1 messenger RNA in Reed-Sternberg cells in nodular sclerosing Hodgkin’s disease. J. Clin. Pathol. 1995, 48, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Riesco Martínez, M.C.; Muñoz Martín, A.J.; Zamberk Majlis, P.; Adeva Alfonso, J.; Sabin Domínguez, P.; García Alfonso, P.; Pérez Fernández, R. Acquired ichthyosis as a paraneoplastic syndrome in Hodgkin’s disease. Clin. Transl. Oncol. 2009, 11, 552–553. [Google Scholar] [CrossRef] [PubMed]
- Didona, D.; Fania, L.; Didona, B.; Eming, R.; Hertl, M.; Di Zenzo, G. Paraneoplastic Dermatoses: A Brief General Review and an Extensive Analysis of Paraneoplastic Pemphigus and Paraneoplastic Dermatomyositis. Int. J. Mol. Sci. 2020, 21, 2178. [Google Scholar] [CrossRef]
- de Souza, P.K.; Amorim, R.O.; Sousa, L.S.; Batista, M.D. Dermatological manifestations of hematologic neoplasms. Part II: Nonspecific skin lesions/paraneoplastic diseases. An. Bras. Dermatol. 2023, 98, 141–158. [Google Scholar] [CrossRef]
- Asad, U.; Austin, B.; Sturgeon, A.; Stetson, C. Paraneoplastic eczematous eruption associated with Hodgkin’s lymphoma. Bayl. Univ. Med. Cent. Proc. 2019, 32, 587–588. [Google Scholar] [CrossRef] [PubMed]
- Kappius, R.H.; Ufkes, N.A.T.B. Paraneoplastic Pemphigus; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Marjon, P.; Kim, B.; Lazic, T.; Cernik, C.; Rathore, R. Paraneoplastic Pemphigus (PNP) As a Presenting Finding in a Patient with Hodgkin’s Lymphoma. Blood 2011, 118, 4864. [Google Scholar] [CrossRef]
- Váróczy, L.; Gergely, L.; Zeher, M.; Szegedi, G.; Illés, A. Malignant lymphoma-associated autoimmune diseases—A descriptive epidemiological study. Rheumatol. Int. 2002, 22, 233–237. [Google Scholar] [CrossRef]
- Lechner, K.; Chen, Y.-A. Paraneoplastic autoimmune cytopenias in Hodgkin lymphoma. Leuk. Lymphoma 2010, 51, 469–474. [Google Scholar] [CrossRef]
- Poponea, N.; Suede, M.; Muhsin Chisti, M. Idiopathic Thrombocytopenia Purpura Masking Hodgkin Disease: A Paraneoplastic Syndrome or Simply a Mere Association. Case Rep. Oncol. 2017, 10, 1116–1120. [Google Scholar] [CrossRef]
- Erlij, D.; Calderón, B.; Rivera, A.; Mella, C.; Valladares, X.; Roessler, E.; Rivera, M.T.; Méndez, G. Polyarthritis and membranoproliferative glomerulonephritis as paraneoplastic manifestation of hodgkin’s lymphoma: A Case Report and Literature Review. Reumatol. Clin. 2016, 12, 282–284. [Google Scholar] [CrossRef]
- Aruch, D.B.; Mims, M.P. Paraneoplastic nephrotic syndrome and inflammatory arthritis at diagnosis in hodgkin lymphoma. Clin. Lymphoma Myeloma Leuk. 2013, 13, 77–79. [Google Scholar] [CrossRef]
- Jurkovic, J.; Cirone, M. Mucocutaneous Paraneoplastic Syndrome Secondary to Classical Hodgkin’s Lymphoma. Clin. Prac. Cases Emerg. Med. 2019, 3, 160–161. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Lim, S.W. Alopecia areata as a paraneoplastic syndrome of Hodgkin’s lymphoma: A case report. Mol. Clin. Oncol. 2014, 2, 596–598. [Google Scholar] [CrossRef] [PubMed]
- Villafranca, J.J.A.; Siles, M.G.; Casanova, M.; Goitia, B.T.; Domínguez, A.R. Paraneoplastic pruritus presenting with Hodgkin’s lymphoma: A case report. J. Med. Case Rep. 2014, 8, 300. [Google Scholar] [CrossRef] [PubMed]
- Pei, S.; Hinshaw, M.A. Palisaded Neutrophilic Granulomatous Dermatitis Leading to Diagnosis of Hodgkin Lymphoma: Report of Rare Case and Literature Review of Paraneoplastic Granulomatous Dermatitides. Am. J. Dermatopathol. 2019, 41, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Tabata, M.M.; Novoa, R.A.; Martires, K.J. Paraneoplastic granulomatous dermatitis in a patient with Hodgkin’s disease: A diagnostic pitfall. BMJ Case Rep. 2018, 2018, bcr2018224961. [Google Scholar] [CrossRef] [PubMed]
- Farruggia, P.; Trizzino, A.; Maringhini, S.; Grigoli, A.; Sapia, C.; D’alessandro, M.; Tropia, S.; D’angelo, P. Hodgkin lymphoma and nephrotic syndrome in childhood. Indian J. Pediatr. 2010, 77, 1147–1149. [Google Scholar] [CrossRef] [PubMed]
- Deacon, A.J.; Goetz, N.N.; Weber, N.; Clouston, A.; Gonsalkorala, E.; Baskerville, C.; Leggett, B. Relapsed nodular lymphocyte-predominant Hodgkin lymphoma presenting as severe paraneoplastic hepatitis: A case report. J. Med. Case Rep. 2023, 17, 269. [Google Scholar] [CrossRef] [PubMed]
- Gutmann, B.; Crivellaro, C.; Mitterer, M.; Zingerle, H.; Egarter-Vigl, E.; Wiedermann, C.J. Paraneoplastic stiff-person syndrome, heterotopic soft tissue ossification and gonarthritis in a HLA B27-positive woman preceding the diagnosis of Hodgkin’s lymphoma. Haematologica 2006, 91 (Suppl. S12), ECR59. [Google Scholar]
- Villano, F.; Peixoto, A.; Riva, E.; Di Matteo, C.; Díaz, L. Digital Ischemia as an Unusual Manifestation of Hodgkin’s Lymphoma. Case Rep. Hematol. 2018, 2018, 1980749. [Google Scholar] [CrossRef]
- AlRasbi, S.; Al-Badi, A.H.; Al Alawi, A.M. Paraneoplastic acral vascular syndrome: Case presentation and literature review. BMJ Case Rep. 2021, 14, e237258. [Google Scholar] [CrossRef] [PubMed]
- Valencia-Sanchez, C.; Zekeridou, A. Paraneoplastic Neurological Syndromes and Beyond Emerging with the Introduction of Immune Checkpoint Inhibitor Cancer Immunotherapy. Front. Neurol. 2021, 12, 642800. [Google Scholar] [CrossRef] [PubMed]
- Duong, S.L.; Prüss, H. Paraneoplastic Autoimmune Neurological Syndromes and the Role of Immune Checkpoint Inhibitors. Neurotherapeutics 2022, 19, 848–863. [Google Scholar] [CrossRef] [PubMed]
- Farina, A.; Birzu, C.; Elsensohn, M.-H.; Picca, A.; Muñiz-Castrillo, S.; Vogrig, A.; Villagrán-García, M.; Ciano-Petersen, N.L.; Massacesi, L.; Hervier, B.; et al. Neurological outcomes in immune checkpoint inhibitor-related neurotoxicity. Brain Commun. 2023, 5, fcad169. [Google Scholar] [CrossRef]
- Binks, S.; Uy, C.; Honnorat, J.; Irani, S.R. Paraneoplastic neurological syndromes: A practical approach to diagnosis and management. Prac. Neurol. 2021, 22, 19–31. [Google Scholar] [CrossRef]


{kind=link}
| Antibodies | Risk of Association with Cancer | Associated Syndrome |
|---|---|---|
| Anti-Tr(DNER) | High risk | Cerebellar degeneration |
| Anti-Hu | High risk | Limbic encephalitis |
| Anti-NMDA | Intermediate risk | Limbic encephalitis |
| Anti-mGluR5 | Intermediate risk | Limbic encephalitis |
| Anti-mGluR1 | Low risk | Cerebellar degeneration |
| Syndrome | Author(s) | Age and Sex of Patient(s) | Treatment Received | Clinical Outcome |
|---|---|---|---|---|
| Cerebellar degeneration | Arratibel et al. [20] | 44-year-old male | IVIG initially but without clinical improvement, followed by ABVD with improvement | Complete resolution of HL with partial improvement in neurological symptoms |
| Briani et al. [29] | 16 patients (12 male and 4 female) with a mean age of 49 years (range 16–73) | Various treatments including combinations of chemotherapy for HL, IVIG, steroids, and plasmapheresis | 8 patients had partial resolution of neurological syndrome after treatment of tumor. 2 patients died | |
| Bernal et al. [21] | 28 patients (22 male and 6 female) with a median age of 16 (range 14–75) | Not mentioned | Complete remission of ataxia in three, partial in one; the rest of the patients stable, with bad functional status or worse | |
| Suri et al. [30] | 54-year-old male | ABVD | Partial resolution of neurological syndrome | |
| Ypma et al. [31] | 34-year-old male | EBVP | Complete resolution of HL and partial resolution of neurological syndrome | |
| Shams’ili et al. [32] | 31-year-old | Antitumor treatment | Complete resolution of HL | |
| 19-year-old | Antitumor treatment, steroid, and plasma exchange | Complete resolution of HL and functional deficits | ||
| Spyridonidis et al. [33] | 20-year-old male | Procarbazine, etoposide, doxorubicin, cyclophosphamide, bleomycin, prednisone, and field irradiation | Complete resolution of HL and no improvement in neurological syndrome | |
| Chepovetsky et al. [23] | 68-year-old male | IVIG and CHOP | Partial resolution of HL and no improvement in neurological syndrome | |
| Smitt et al. [18] | 19-year-old female | MOPP-ABV, followed by subtotal nodal irradiation, IVIG, and plasmapheresis | Complete resolution of HL and neurological syndrome | |
| 49-year-old female | Plasmapheresis | Complete resolution of HL and no improvement in neurological syndrome | ||
| Christensen et al. [16] | 76-year-old male | IVIG, gemcitabine, liposomal doxorubicin, and radiotherapy | Complete resolution of HL and partial resolution of neurological syndrome | |
| Limbic encephalitis | Briani et al. [29] | 45-year-old male | Not mentioned | Complete resolution of neurological syndrome after treatment of tumor |
| Lancaster et al. [34] | 46-year-old female | ABVD and steroids | Partial resolution of HL and complete resolution of seizures and altered mentation | |
| 15-year-old male | IVIG and radiotherapy | Complete resolution of HL and neurological syndrome | ||
| Zandi et al. [35] | 49-year-old male | Steroids, IVIG, plasmapheresis, and chemotherapy (regimen not mentioned) | Progression of HL and partial resolution of neurological syndrome | |
| Kung et al. [36] | 53-year-old female | ABVD | Complete resolution of neurological syndrome | |
| Hentschke et al. [37] | 61-year-old male | ABVD | Partial resolution of HL and partial resolution of neurological syndrome | |
| Bernard et al. [38] | 59-year-old female | MOPP-ABV and radiotherapy | Complete resolution of HL and partial resolution of neurological syndrome | |
| Deodhare et al. [39] | 23-year-old male | Steroids and ABVD | Complete resolution of HL and partial resolution of neurological syndrome | |
| Rosenbaum et al. [40] | 13-year-old female | Chemotherapy (regimen not mentioned) | Partial resolution of HL and no improvement in neurological syndrome | |
| 16-year-old female | Cisplatin, etoposide, and ifosfamide | Partial resolution of HL and partial resolution of neurological syndrome | ||
| Duyckaerts et al. [41] | 36-year-old male | Steroids, procarbazine, chlormethine chlorhydrate, and vincristine sulfate | Death | |
| Pfliegler et al. [42] | 33-year-old male | MOPP followed by ABVD | Complete resolution of HL and complete resolution of neurological syndrome | |
| PEMS | Briani et al. [29] | 59-year-old female | Not mentioned | Partial resolution of neurological syndrome after treatment of tumor |
| 84-year-old male | Not mentioned | Not mentioned | ||
| PERM | Borellini et al. [43] | 60-year-old male | Prednisone and ABVD | Complete resolution of HL and partial resolution of neurological syndrome |
| Pontine myelinolysis | Kanaparthi et al. [44] | 11-year-old male | ABVD | Partial resolution of HL and partial resolution of neurological syndrome |
| GBS | Odaman Al et al. [45] | 13-year-old female | ABVD, IVIG, and steroids | Partial resolution of HL and partial resolution of neurological syndrome |
| Anderson et al. [46] | 34-year-old male | IVIG and ABVD | Partial resolution of HL and partial resolution of neurological syndrome | |
| CIDP | Briani et al. [29] | Males aged 48 and 62 years | Not mentioned | One patient had complete resolution of HL and partial resolution of neurological syndrome |
| Sensory neuropathy | Briani et al. [29] | 61-year-old male | Not mentioned | Not mentioned |
| Milanesio et al. [47] | 36-year-old female | ABVD | Complete resolution of HL and partial resolution of neurological syndrome | |
| Sensory neuronopathy | Briani et al. [29] | 29-year-old female | Not mentioned | Not mentioned |
| Myotonia | Briani et al. [29] | 70-year-old female | Not mentioned | Partial resolution of neurological syndrome after treatment of tumor |
| Lower motor neuropathy | Flangan et al. [48] | 31-year-old female | IVIG, steroids, ABVD, radiation, ICE, and ASCT | Complete resolution of HL and partial resolution of neurological syndrome |
| GACNS | Johnson et al. [49] | 49-year-old female | BCVPP and whole-brain radiation therapy | Complete resolution of HL and partial resolution of neurological syndrome |
| Lopez-Chiriboga et al. [50] | 25-year-old female | ABVD | Partial resolution of HL and partial resolution of neurological syndrome | |
| Delobel et al. [51] | 26-year-old female | Prednisone, ABVD, and radiotherapy | Complete resolution of HL and complete resolution of neurological syndrome | |
| Rhomboencephalomyelitis | Valappil et al. [52] | Female in her 50s | Not available | Not available |
| Author(s) | Patient Age in Years | Sex | Treatment Received | Clinical Outcome |
|---|---|---|---|---|
| Córdoba et al. [55] | 17 | Male | Modified regimen of bleomycin, cyclophosphamide, dacarbazine, and methylprednisolone | Complete remission of HL |
| Crosbie et al. [56] | 21 | Female | Modified regimen of mustine (10 mg), vincristine (1 mg), and procarbazine (50 mg, once monthly) | Complete resolution of HL |
| Yalçin et al. [57] | 47 | Female | Vincristine, bleomycin, cyclophosphamide, and prednisone for 2 cycles, followed by 8 weeks of radiotherapy | Symptomatic resolution of PNS and normalization of bilirubin levels |
| Ripoll et al. [58] | 28 | Female | C-MOPP regimen followed by radiotherapy | Death |
| 23 | Female | Once cycle of C-MOPP, followed by ABVD a few months later, followed by radiotherapy | Complete resolution of HL | |
| Barta et al. [59] | 41 | Male | 2 weeks of prednisone followed by radiotherapy | Complete resolution of HL |
| Leeuwenburgh et al. [60] | 17 | Male | MOPP regimen, followed by a reduced regimen of P(V)AG | Complete resolution of HL |
| Pass et al. [61] | 12 | Male | A modified MOPP-ABV regimen, followed by radiation therapy | Complete resolution of HL |
| 10 | Male | Nitrogen mustard and prednisone, followed by the Stanford V regimen, which was given along with rituximab and IVIG for IgG deficiency | Partial resolution of HL followed by death due to aspiration secondary to status epilepticus | |
| Wong et al. [62] | 38 | Male | Reduced ABVD, followed by cyclophosphamide, followed by autologous hematopoietic stem cell transplant with a conditioning regimen consisting of bischloroethylnitrosourea, etoposide, cytosine arabinoside, and melphalan | Complete resolution of HL |
| Anugwom et al. [63] | 27 | Female | Radiotherapy, high-dose dexamethasone, and a modified chemotherapy regimen consisting of rituximab, gemcitabine, and cisplatin, followed by ABVD | Complete resolution of HL |
| Syndromes | Author(s) | Patient Age in Years | Sex | Treatment Received | Clinical Outcome |
|---|---|---|---|---|---|
| Mucocutaneous PNS | Jurkovic et al. [86] | 39 | Male | Not reported | Not reported |
| Alopecia areata | Kanaparthi et al. [44] | 11 | Male | ABVD | Partial resolution of HL |
| Gong et al. [87] | 46 | Male | Topical and intralesional corticosteroids steroids, followed by ABVD | Complete resolution of HL and near-complete resolution of PNS | |
| Paraneoplastic pruritis | Villafranca et al. [88] | 20 | Female | In chronological order: ABVD, GDP, hematopoietic stem cell transplant, gemcitabine–inorelbine, everolimus, CVP, GDP, bendamustine, GVD, cyclophosphamide–vinblastine–celecoxib, lenalidomide–cyclophosphamide, high-dose dexamethasone, brentuximab vedotin, oral etoposide, carboplatin–gemcitabine, thalidomide, and dexamethasone. Aprepitant and dexamethasone used specifically for PNS | Partial response of PNS, mostly with aprepitant, and partial response of HLwhich progressed and ultimately led to death by lymphoma-related airway compression |
| Granulomatous dermatitis | Pei et al. [89] | 47 | Female | Chemotherapy. Regimen not reported | Not reported |
| Tabata et al. [90] | 73 | Male | Etoposide, prednisone, doxorubicin, and cyclophosphamide. Clobetasol ointment and intralesional triamcinolone used specifically for PNS | Near-complete resolution of HL and partial resolution of PNS with plaque softening | |
| Acquired ichthyosis | Riesco Martinez et al. [75] | 80 | Male | Dose-reduced COPP | Partial resolution of PNS |
| Paraneoplastic pemphigus | Marjon et al. [80] | 76 | Male | Prednisone, followed by GVD | Partial resolution of PNS |
| Nephrotic syndrome | Aruch et al. [85] | 38 | Male | Dexamethasone, followed by ABVD | Complete resolution of HL and PNS |
| Spyridonidis et al. [33] | 20 | Male | Prednisone, followed by procarbazine, etoposide, doxorubicin, cyclophosphamide, bleomycin, and prednisone along with irradiation | Complete resolution of HL and PNS | |
| Sfrijan et al. [65] | 9 | Male | OEPA along with irradiation | Complete resolution of HL and PNS | |
| Farruggia et al. [91] | 11 | Male | Prednisone, followed by COPP/ABV and irradiation | Complete resolution of HL and PNS | |
| 17 | Female | ||||
| Paraneoplastic hepatitis | Deacon et al. [92] | 28 | Male | Prednisolone, followed by rituximab and cyclophosphamide, followed by prednisone, followed by dose-reduced R-CHOP | Complete resolution of HL and near-complete resolution of PNS with persistence of splenomegaly |
| Immune thrombocytopenia purpura | Poponea et al. [83] | 74 | Female | ABVD | Complete resolution of PNS and partial resolution of HL |
| Stiff person syndrome | Gutmann et al. [93] | 55 | Female | ABVD | Complete resolution of HL and partial response of PNS with resolution of muscular hyperactivity but persistence of muscle weakness |
| PAVS | Villano et al. [94] | 45 | Male | Corticosteroids and IV cyclophosphamide, followed by ABVD | Complete resolution of HL and PNS—although digital ischemia had occurred by the time chemotherapy was started, resulting in amputation of 3/8 distal phalanges |
| AlRasbi et al. [95] | 65 | Male | Dacarbazin, doxorubicin, and vinblastine, followed by bendamustine and dacarbazine | Near-complete resolution of HL and PNS with persistence of dry gangrene of one phalange |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jadoon, Y.; Patil, G.; Loke, C.; Bhardwaj, P.V. Paraneoplastic Syndromes in Hodgkin’s Lymphoma. Lymphatics 2024, 2, 25-42. https://doi.org/10.3390/lymphatics2010003
Jadoon Y, Patil G, Loke C, Bhardwaj PV. Paraneoplastic Syndromes in Hodgkin’s Lymphoma. Lymphatics. 2024; 2(1):25-42. https://doi.org/10.3390/lymphatics2010003
Chicago/Turabian StyleJadoon, Yamna, Goutham Patil, Chandravathi Loke, and Prarthna V. Bhardwaj. 2024. "Paraneoplastic Syndromes in Hodgkin’s Lymphoma" Lymphatics 2, no. 1: 25-42. https://doi.org/10.3390/lymphatics2010003
APA StyleJadoon, Y., Patil, G., Loke, C., & Bhardwaj, P. V. (2024). Paraneoplastic Syndromes in Hodgkin’s Lymphoma. Lymphatics, 2(1), 25-42. https://doi.org/10.3390/lymphatics2010003