



Cancers 2024, 16(1), 140; https://doi.org/10.3390/cancers16010140 - 27 Dec 2023
Viewed by 1972
Abstract
►
Show Figures
Selpercatinib is indicated for locally advanced/metastatic RET-activated solid tumors after progression or following prior systemic therapies. Until the recently published data from LIBRETTO-431 and LIBRETTO-531, there were limited effectiveness data comparing selpercatinib with other first-line treatments in RET-activated non-small cell lung
[...] Read more.
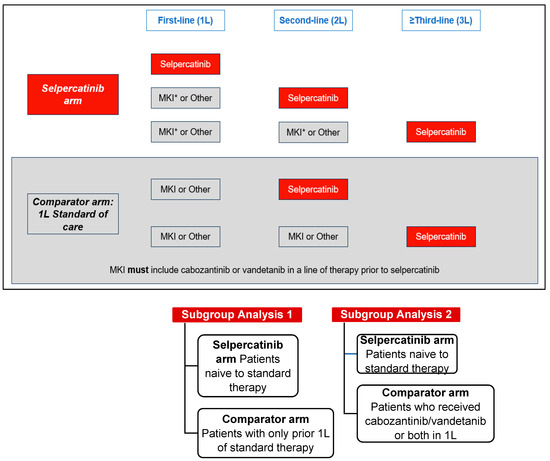
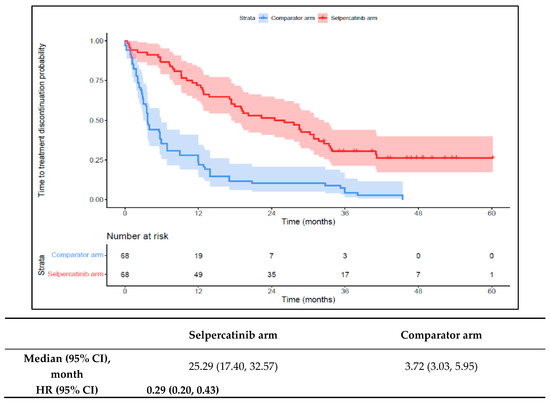
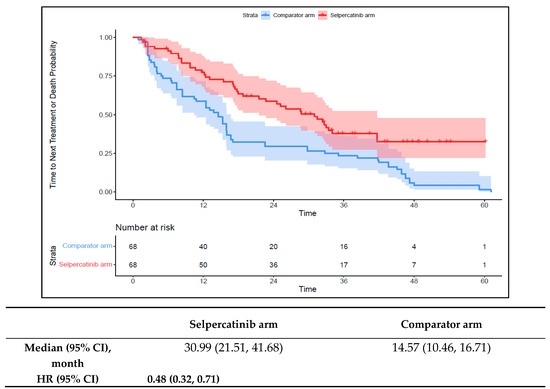
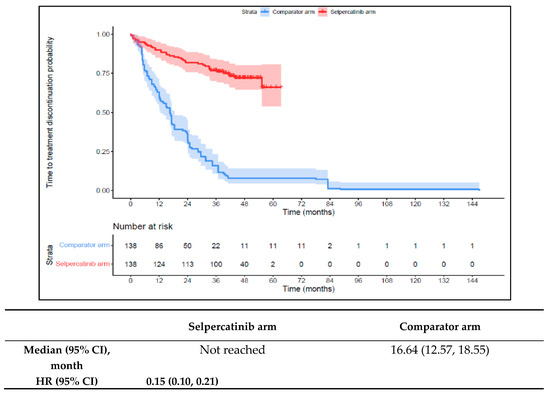
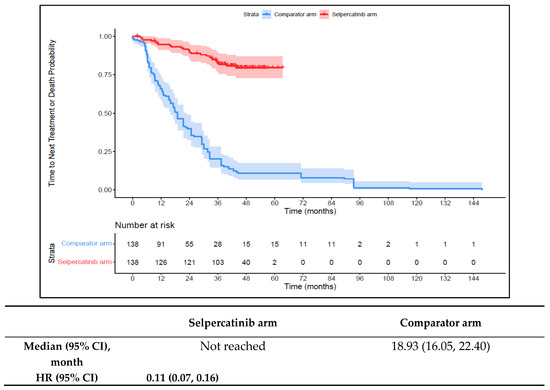
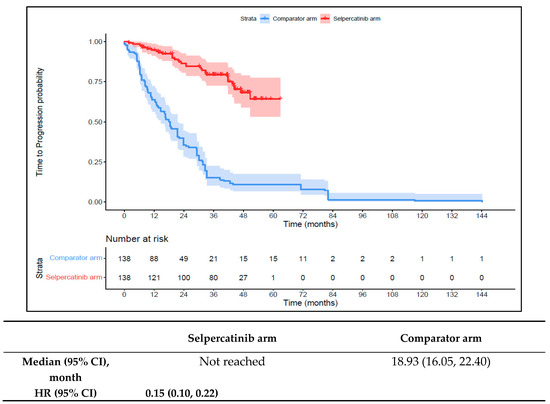
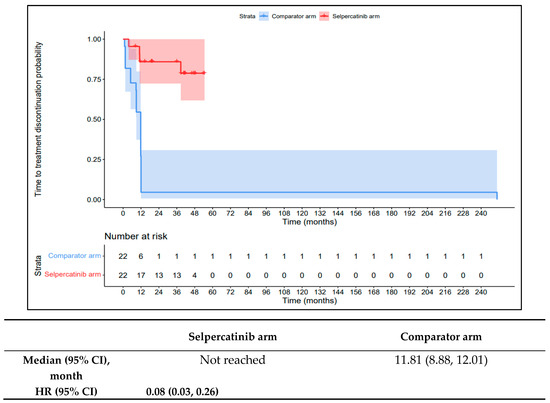
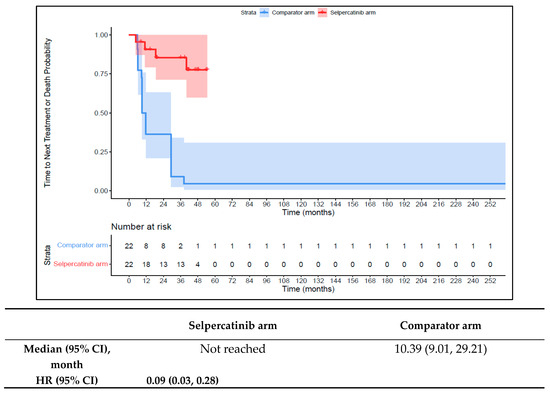
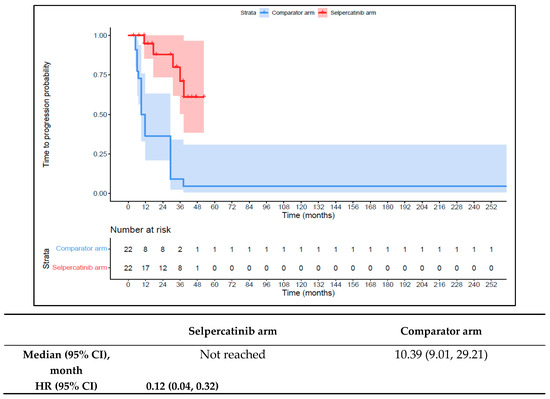
Selpercatinib is indicated for locally advanced/metastatic RET-activated solid tumors after progression or following prior systemic therapies. Until the recently published data from LIBRETTO-431 and LIBRETTO-531, there were limited effectiveness data comparing selpercatinib with other first-line treatments in RET-activated non-small cell lung cancer (NSCLC), medullary thyroid cancer (MTC), and thyroid cancer (TC). This study analyzed patient data from LIBRETTO-001 and compared the outcomes (time to treatment discontinuation {TTD}, time to next treatment or death {TTNT-D}, time to progression {TTP}, and the objective response rate {ORR}) of first-line selpercatinib (selpercatinib arm) use with the outcomes of first-line standard therapies in patients who then received selpercatinib in later lines of treatment (comparator arm). Overall, the first-line selpercatinib arm had a longer TTD, TTNT-D, and TTP versus the first-line comparator arm. The hazard ratios (HRs) for TTD were 0.29 (NSCLC), 0.15 (MTC), 0.08 (TC); for TTNT-D, the HRs were 0.48 (NSCLC), 0.11 (MTC), 0.09 (TC); and for TTP, the HRs were 0.54 (NSCLC), 0.15 (MTC), and 0.12 (TC). The ORR was higher for first-line selpercatinib versus the first-line comparator (NSCLC: 85.3% vs. 39.7%; MTC: 82.6% vs. 15.2%; and TC: 81.8% vs. 31.8%). First-line selpercatinib use is associated with improved outcomes compared to first-line comparator therapies for patients with advanced/metastatic RET-activated cancers.
Full article
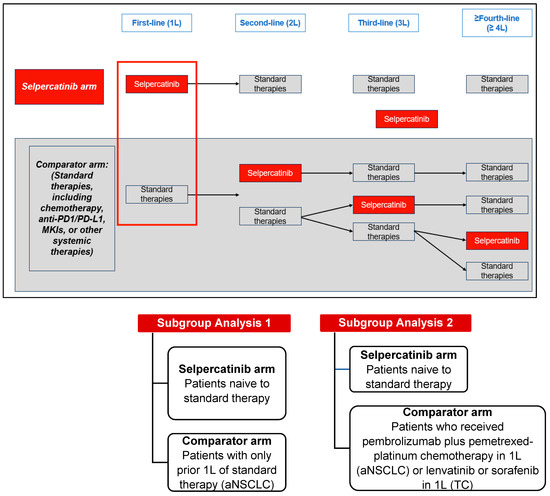
Figure 1
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}