Current Advances and Future Directions for Antithrombotic Treatment Strategies
(Closed)
Share This Topical Collection
Editor
Topical Collection Information
Dear Colleagues,
The last decade has seen major advances in the development and management of antithrombotic therapy, a field that is still rapidly evolving. Pivotal trials have revolutionized many aspects of antithrombotic therapy in several areas of cardiovascular disease, including atrial fibrillation, ischemic heart disease, and venous thromboembolism; however, the overarching aim remains to achieve the greatest reduction in thrombotic risk, with the minimum risk of bleeding. In the coming years, focus on high-risk patients, implementation of personalized medicine, and the inclusion of antithrombotic strategies in the context of more comprehensive and holistic treatment approaches will be some of the most intriguing challenges that we will face.
This collection aims to collect original contributions, literature reviews (including systematic reviews and meta-analysis), viewpoints, or any other kind of contribution related to the present and future development of antithrombotic strategies in the broad field of cardiovascular diseases. Submission with a particular focus on an innovative and comprehensive approach to the topic, or current unmet needs in antithrombotic strategies, are particularly encouraged.
Dr. Giulio Francesco Romiti
Collection Editor
Manuscript Submission Information
Manuscripts should be submitted online at www.mdpi.com by registering and logging in to this website. Once you are registered, click here to go to the submission form. Manuscripts can be submitted until the deadline. All submissions that pass pre-check are peer-reviewed. Accepted papers will be published continuously in the journal (as soon as accepted) and will be listed together on the collection website. Research articles, review articles as well as short communications are invited. For planned papers, a title and short abstract (about 100 words) can be sent to the Editorial Office for announcement on this website.
Submitted manuscripts should not have been published previously, nor be under consideration for publication elsewhere (except conference proceedings papers). All manuscripts are thoroughly refereed through a single-blind peer-review process. A guide for authors and other relevant information for submission of manuscripts is available on the Instructions for Authors page. Journal of Clinical Medicine is an international peer-reviewed open access semimonthly journal published by MDPI.
Please visit the Instructions for Authors page before submitting a manuscript.
The Article Processing Charge (APC) for publication in this open access journal is 2600 CHF (Swiss Francs).
Submitted papers should be well formatted and use good English. Authors may use MDPI's
English editing service prior to publication or during author revisions.
Keywords
- antithrombotics
- anticoagulants
- antiplatelets
- cardiovascular disease
- ischemic heart disease
- atrial fibrillation
- venous thromboembolism
- thromboembolic risk prevention
- bleeding risk management
Published Papers (8 papers)
Open AccessEditorial
New Paradigms in Antithrombotic Strategies: A Leap into the Future of Cardiovascular Medicine
by
Giulio Francesco Romiti
Viewed by 1496
Abstract
During the last decades, significant improvements have changed the landscape of antithrombotic treatment strategies and, more generally, the treatment of thrombotic and cardiovascular diseases [...]
Full article
Open AccessArticle
Prevalence and Rate of Resolution of Left Atrial Thrombus in Patients with Non-Valvular Atrial Fibrillation: A Two-Center Retrospective Real-World Study
by
Pompilio Faggiano, Elisabetta Dinatolo, Antonella Moreo, Benedetta De Chiara, Marco Sbolli, Francesco Musca, Antonio Curnis, Oriana Belli, Cristina Giannattasio, Cesare Tomasi, Marco Metra and Gloria Santangelo
Cited by 7 | Viewed by 2887
Abstract
Background and aim. Thromboembolic events due to left atrial appendage (LAA) thrombosis are the main complication of non-valvular atrial fibrillation (NVAF). Although anticoagulants are effective in patients with NVAF, a minimal residual thromboembolic risk persists. Little is known about the prevalence of LAA
[...] Read more.
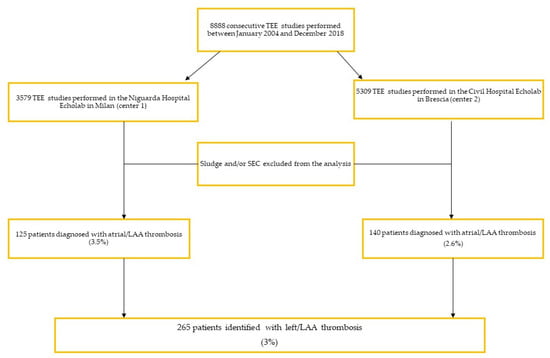
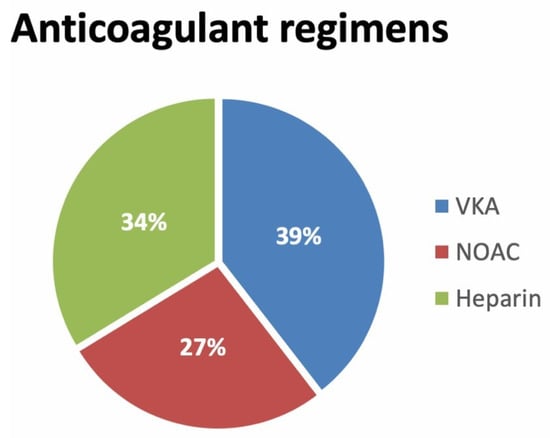
Background and aim. Thromboembolic events due to left atrial appendage (LAA) thrombosis are the main complication of non-valvular atrial fibrillation (NVAF). Although anticoagulants are effective in patients with NVAF, a minimal residual thromboembolic risk persists. Little is known about the prevalence of LAA thrombus and the rate of resolution after the recommended period of anticoagulation therapy, including vitamin K antagonists (VKA), heparin, and non-vitamin K antagonist oral anticoagulants (NOACs). Methods and results. We aimed to study the prevalence of LAA thrombus in an unselected cohort of patients undergoing transesophageal echocardiogram (TEE), and the determinants of LAA thrombus resolution. We retrospectively analyzed 8888 consecutive TEEs performed over five years in two high-volume centers and included all patients with LAA thrombus. A total of 265 patients (3%) had an LAA thrombus. Among these, 97% presented with AF. Fifty-eight percent of patients were on anticoagulants at least three weeks before the diagnosis. After the LAA thrombus diagnosis, VKAs were prescribed in 52%, heparin in 18.5%, and NOAC in 27% of patients. Among the 183 patients with repeat TEE, performed at (25–75th) 39 days (21–84), 67% showed resolution of the LAA thrombus. Although the rate of thrombus resolution was higher in patients treated with NOACs (NOACs 71%, VKA 66%, Heparin 60%) the difference between anticoagulants was statistically non-significant (VKA, OR 0.9,
p = 0.83; NOAC, OR 1.23,
p = 0.42; heparin, OR 0.69,
p = 0.35). Thus, NOACs were demonstrated to be at least as effective as other anticoagulants in the rate of LAA thrombus resolution. Upon multivariate-adjusted analysis, higher LAA emptying velocities were the only predictor of thrombus resolution. In conclusion, the majority of patients were already on anticoagulants. NOACs could be at least as effective as other anticoagulants, yielding an LAA thrombus resolution in two-thirds of patients. This may have clinical relevance, especially in patients undergoing cardioversion or catheter ablation.
Full article
►▼
Show Figures
Open AccessArticle
Anticoagulation Prior to COVID-19 Infection Has No Impact on 6 Months Mortality: A Propensity Score–Matched Cohort Study
by
Marcin Protasiewicz, Konrad Reszka, Wojciech Kosowski, Barbara Adamik, Wojciech Bombala, Adrian Doroszko, Damian Gajecki, Jakub Gawryś, Maciej Guziński, Maria Jedrzejczyk, Krzysztof Kaliszewski, Katarzyna Kilis-Pstrusinska, Bogusława Konopska, Agnieszka Kopec, Krzysztof Kujawa, Anna Langner, Anna Larysz, Weronika Lis, Lilla Pawlik-Sobecka, Joanna Gorka-Dynysiewicz, Marta Rosiek-Biegus, Agnieszka Matera-Witkiewicz, Tomasz Matys, Michał Pomorski, Mateusz Sokolski, Janusz Sokołowski, Anna Tomasiewicz-Zapolska, Katarzyna Madziarska and Ewa A Jankowskaadd
Show full author list
remove
Hide full author list
| Viewed by 2128
Abstract
The coronavirus disease 2019 (COVID-19) shows high incidence of thromboembolic events in humans. In the present study, we aimed to evaluate if anticoagulation prior to COVID-19 infection may impact clinical profile, as well as mortality rate among patients hospitalized with COVID-19. The study
[...] Read more.
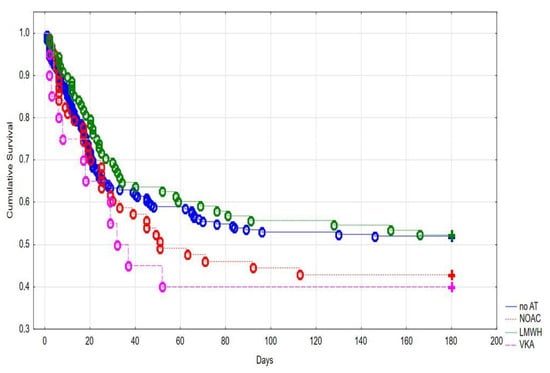
The coronavirus disease 2019 (COVID-19) shows high incidence of thromboembolic events in humans. In the present study, we aimed to evaluate if anticoagulation prior to COVID-19 infection may impact clinical profile, as well as mortality rate among patients hospitalized with COVID-19. The study was based on retrospective analysis of medical records of patients with laboratory confirmed SARS-CoV-2 infection. After propensity score matching (PSM), a group of 236 patients receiving any anticoagulant treatment prior to COVID-19 infection (AT group) was compared to 236 patients without previous anticoagulation (no AT group). In 180 days, the observation we noted comparable mortality rate in AT and no AT groups (38.5% vs. 41.1%,
p = 0.51). Similarly, we did not observe any statistically significant differences in admission in the intensive care unit (14.1% vs. 9.6%,
p = 0.20), intubation and mechanical ventilation (15.0% vs. 11.6%,
p = 0.38), catecholamines usage (14.3% vs. 13.8%,
p = 0.86), and bleeding rate (6.3% vs. 8.9%,
p = 0.37) in both groups. Our results suggest that antithrombotic treatment prior to COVID-19 infection is unlikely to be protective for morbidity and mortality in patients hospitalized with COVID-19.
Full article
►▼
Show Figures
Open AccessArticle
Effectiveness and Safety of Non-Vitamin K Oral Anticoagulants in Non-Valvular Atrial Fibrillation Patients: Results of A Real-World Study in a Metropolitan Area of Northern Italy
by
Emanuele Crocetti, Sarah Cattaneo, Walter Bergamaschi, Stefano De Servi and Antonio Giampiero Russo
Cited by 6 | Viewed by 2794
Abstract
Background: New oral anticoagulant agents (NOACs) are valid alternatives for vitamin K antagonists (VKA) in patients with non-valvular atrial fibrillation (NVAF) for stroke prevention. In clinical practice, NOACs users may differ from patients enrolled in clinical trials in age or comorbidities, and thus
[...] Read more.
Background: New oral anticoagulant agents (NOACs) are valid alternatives for vitamin K antagonists (VKA) in patients with non-valvular atrial fibrillation (NVAF) for stroke prevention. In clinical practice, NOACs users may differ from patients enrolled in clinical trials in age or comorbidities, and thus it is a critical issue to evaluate the effectiveness and safety of NOACs in the real-world. Accordingly, we assessed two-year overall mortality and hospital admissions for myocardial infarction, stroke or bleeding in patients with NVAF users of NOACs compared to warfarin-treated patients. Methods: This is a population-based retrospective new user active comparator study. All atrial fibrillation patients who were naïve and not switcher users of oral anticoagulants from January 2017 to December 2019 were included (
n = 8543). Data were obtained from the electronic health records of the Milan Agency for Health Protection, Italy. Two-year risks for overall mortality, myocardial infarction, stroke and bleeding were computed using Cox models. Age, sex, number of comorbidities, use of platelet aggregation inhibitors and Proton pump inhibitors and area of residence were used as confounding factors. We also controlled by indication bias-weighting NOACs and warfarin users based on the weights computed by a Kernel propensity score. Results: For all NOACs, we found a decrease in the risks compared with warfarin for mortality (from −25% to −49%), hospitalization for myocardial infarction (from −16% to −27%, statistically significant for apixaban, edoxaban and rivaroxaban) and ischemic stroke (from −23% to −41%, significant for dabigatran and apixaban). The risk of bleeding was decreased for rivaroxaban (−33%) and numerically but not significantly for the other NOACs. Conclusions: After two years of follow-up, in comparison with warfarin, NOACs users showed a significant reduction of overall mortality (all NOACs), hospital admission for myocardial infarction (apixaban and edoxaban), ischemic stroke (dabigatran) and bleeding (rivaroxaban).
Full article
Open AccessReview
A Review of Current and Future Antithrombotic Strategies in Surgical Patients—Leaving the Graduated Compression Stockings Behind?
by
Amulya Khatri, Matthew Machin, Aditya Vijay, Safa Salim, Joseph Shalhoub and Alun Huw Davies
Cited by 6 | Viewed by 3709
Abstract
Venous thromboembolism (VTE) remains an important consideration within surgery, with recent evidence looking to refine clinical guidance. This review provides a contemporary update of existing clinical evidence for antithrombotic regimens for surgical patients, providing future directions for prophylaxis regimens and research. For moderate
[...] Read more.
Venous thromboembolism (VTE) remains an important consideration within surgery, with recent evidence looking to refine clinical guidance. This review provides a contemporary update of existing clinical evidence for antithrombotic regimens for surgical patients, providing future directions for prophylaxis regimens and research. For moderate to high VTE risk patients, existing evidence supports the use of heparins for prophylaxis. Direct oral anticoagulants (DOACs) have been validated within orthopaedic surgery, although there remain few completed randomised controlled trials in other surgical specialties. Recent trials have also cast doubt on the efficacy of mechanical prophylaxis, especially when adjuvant to pharmacological prophylaxis. Despite the ongoing uncertainty in higher VTE risk patients, there remains a lack of evidence for mechanical prophylaxis in low VTE risk patients, with a recent systematic search failing to identify high-quality evidence. Future research on rigorously developed and validated risk assessment models will allow the better stratification of patients for clinical and academic use. Mechanical prophylaxis’ role in modern practice remains uncertain, requiring high-quality trials to investigate select populations in which it may hold benefit and to explore whether intermittent pneumatic compression is more effective. The validation of DOACs and aspirin in wider specialties may permit pharmacological thromboprophylactic regimens that are easier to administer.
Full article
Open AccessReview
Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis
by
Giulio Francesco Romiti, Bernadette Corica, Gregory Y. H. Lip and Marco Proietti
Cited by 66 | Viewed by 6533
Abstract
Background: In patients with COVID-19, cardiovascular complications are common and associated with poor prognosis. Among these, an association between atrial fibrillation (AF) and COVID-19 has been described; however, the extent of this relationship is unclear. The aim of this study is to investigate
[...] Read more.
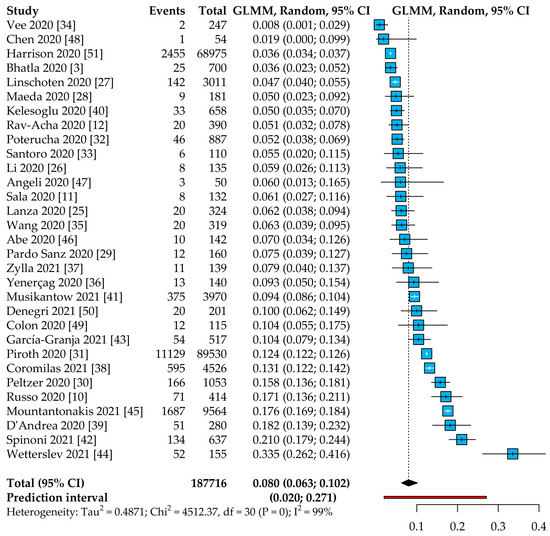
Background: In patients with COVID-19, cardiovascular complications are common and associated with poor prognosis. Among these, an association between atrial fibrillation (AF) and COVID-19 has been described; however, the extent of this relationship is unclear. The aim of this study is to investigate the epidemiology of AF in COVID-19 patients and its impact on all-cause mortality. Methods: A systematic review and meta-analysis were performed and reported according to PRISMA guidelines, and a protocol for this study was registered on PROSPERO (CRD42021227950). PubMed and EMBASE were systematically searched for relevant studies. A random-effects model was used to estimate pooled odds ratios (OR) and 95% confidence intervals (CI). Results: Overall, 31 studies were included in the analysis, with a total number of 187,716 COVID-19 patients. The prevalence of AF was found to be as high as 8% of patients with COVID-19 (95% CI: 6.3–10.2%, 95% prediction intervals (PI): 2.0–27.1%), with a high degree of heterogeneity between studies; a multiple meta-regression model including geographical location, age, hypertension, and diabetes showed that these factors accounted for more than a third of the heterogeneity. AF COVID-19 patients were less likely to be female but more likely older, hypertensive, and with a critical status than those without AF. Patients with AF showed a significant increase in the risk of all-cause mortality (OR: 3.97, 95% CI: 2.76–5.71), with a high degree of heterogeneity. A sensitivity analysis focusing on new-onset AF showed the consistency of these results. Conclusions: Among COVID-19 patients, AF is found in 8% of patients. AF COVID-19 patients are older, more hypertensive, and more likely to have a critical status. In COVID-19 patients, AF is associated with a 4-fold higher risk of death. Further studies are needed to define the best treatment strategies to improve the prognosis of AF COVID-19 patients.
Full article
►▼
Show Figures
Open AccessArticle
Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study
by
Lorène Zerah, Dominique Bonnet-Zamponi, Aya Ajrouche, Jean-Philippe Collet, Yann De Rycke and Florence Tubach
Cited by 1 | Viewed by 2157
Abstract
With the increase in prevalence of cardiovascular diseases, multimorbidity, and medical progress, oral antithrombotic (AT) combinations are increasingly prescribed. The aims of this study were to estimate the incidence of oral AT combinations, their appropriateness (defined as indications compliant with guidelines), and the
[...] Read more.
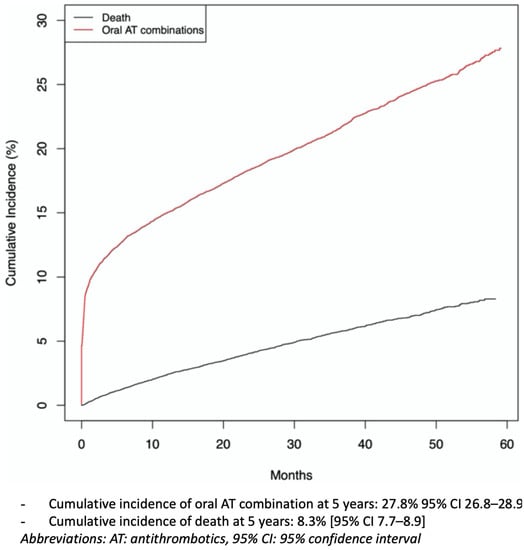
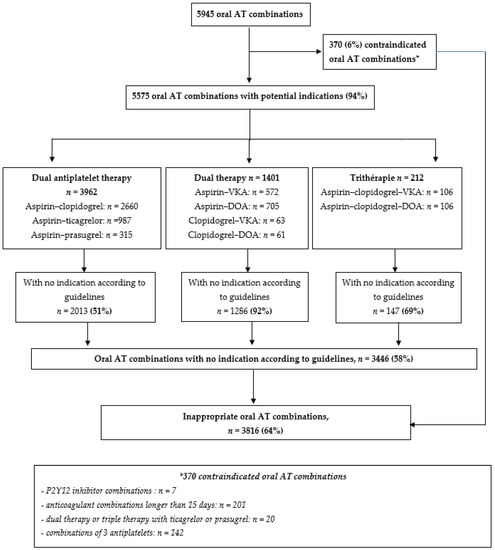
With the increase in prevalence of cardiovascular diseases, multimorbidity, and medical progress, oral antithrombotic (AT) combinations are increasingly prescribed. The aims of this study were to estimate the incidence of oral AT combinations, their appropriateness (defined as indications compliant with guidelines), and the related risk of major bleeding (i.e., leading to hospitalization) or death, among new users. We conducted a 5-year historical cohort study, using the French national healthcare database, including all individuals ≥ 45 years old with a first delivery of oral ATs between 1 January 2013 and 31 December 2017. The cumulative incidence of oral AT combinations was estimated with the Fine and Gray method, taking into account the competitive risk of death. We compared the cumulative incidence of major bleeding according to the type of oral AT treatment initiated at study entry (monotherapy or oral AT combinations). During the study period, 22,220 individuals were included (mean (SD) age 68 (12) years). The cumulative incidence of oral AT combinations at 5 years was 27.8% (95% confidence interval (CI) 26.8–28.9). Overall, 64% of any oral AT combinations did not comply with guidelines. The cumulative incidence of major bleeding and death in the whole cohort at 5 years was 4.1% (95% CI 3.7–4.6) and 10.8% (95% CI 10.1–11.6), respectively. Risk of major bleeding increased among individuals with oral AT combinations versus oral AT monotherapy at study entry (subdistribution hazard ratio sHR: 2.16 (1.01–4.63)); with no difference in terms of death. The use of oral AT combinations among oral AT users is frequent, often inappropriately prescribed, and associated with an increased risk of major bleeding.
Full article
►▼
Show Figures
Open AccessReview
Gut Microbiota and the Quality of Oral Anticoagulation in Vitamin K Antagonists Users: A Review of Potential Implications
by
Anny Camelo-Castillo, José Miguel Rivera-Caravaca, Esteban Orenes-Piñero, Inmaculada Ramírez-Macías, Vanessa Roldán, Gregory Y. H. Lip and Francisco Marín
Cited by 14 | Viewed by 6876
Abstract
The efficacy and safety of vitamin K antagonists (VKAs) as oral anticoagulants (OACs) depend on the quality of anticoagulation control, as reflected by the mean time in therapeutic range (TTR). Several factors may be involved in poor TTR such as comorbidities, high inter-individual
[...] Read more.
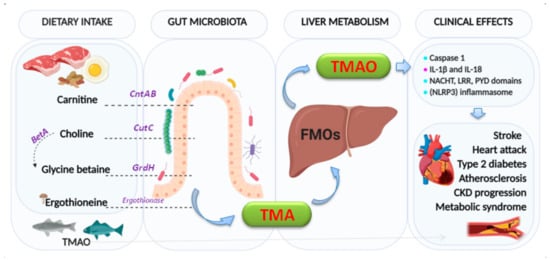
The efficacy and safety of vitamin K antagonists (VKAs) as oral anticoagulants (OACs) depend on the quality of anticoagulation control, as reflected by the mean time in therapeutic range (TTR). Several factors may be involved in poor TTR such as comorbidities, high inter-individual variability, interacting drugs, and non-adherence. Recent studies suggest that gut microbiota (GM) plays an important role in the pathogenesis of cardiovascular diseases, but the effect of the GM on anticoagulation control with VKAs is unknown. In the present review article, we propose different mechanisms by which the GM could have an impact on the quality of anticoagulation control in patients taking VKA therapy. We suggest that the potential effects of GM may be mediated first, by an indirect effect of metabolites produced by GM in the availability of VKAs drugs; second, by an effect of vitamin K-producing bacteria; and finally, by the structural modification of the molecules of VKAs. Future research will help confirm these hypotheses and may suggest profiles of bacterial signatures or microbial metabolites, to be used as biomarkers to predict the quality of anticoagulation. This could lead to the design of intervention strategies modulating gut microbiota, for example, by using probiotics.
Full article
►▼
Show Figures







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}