Associations between Neurocardiovascular Signal Entropy and Physical Frailty

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
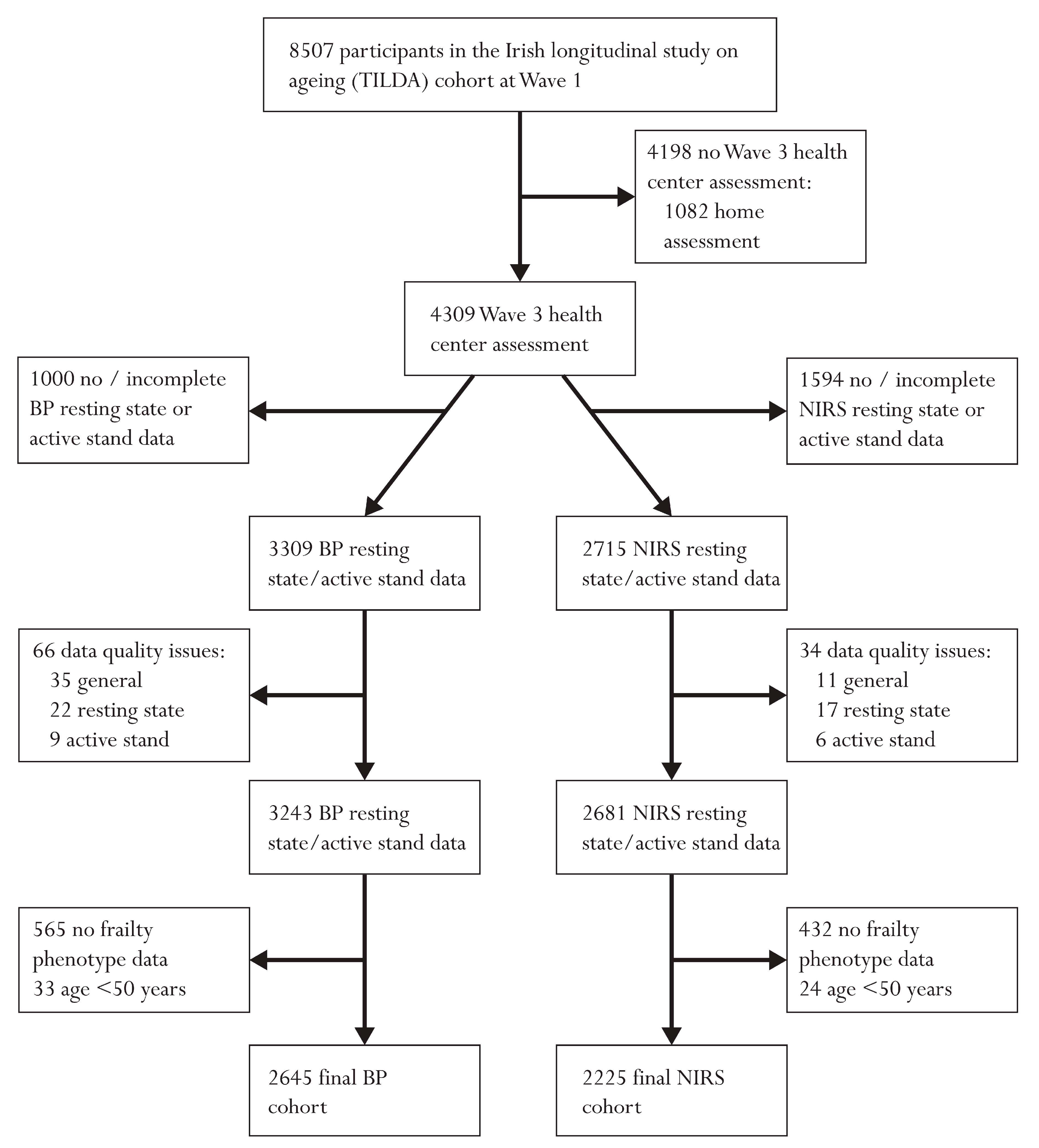
2.1. Study Population
2.2. Neurocardiovascular Measurements
2.3. Signal Processing
2.4. Entropy Analysis
2.4.1. Approximate Entropy (ApEn)
2.4.2. Sample Entropy (SampEn)
2.5. Frailty Phenotype
2.6. Other Measures
2.7. Statistical Analysis
2.8. Data Availability Statement
3. Results
3.1. Participant Characteristics
3.2. Associations of Entropy with Frailty Phenotype
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| X | ΔApEn | ΔSampEn | ||
|---|---|---|---|---|
| Resting State N = 3273–3817 | N [%] Stationary | N (%) Stationary | Mean [Range] | Mean [Range] |
| sBP | 59 (1.6%) | 921 (24.1%) | −0.1 [−2.3 to 2.6] × 10−14 | <1 × 10−32 |
| dBP | 57 (1.5%) | 879 (23.0%) | 0.1 [−1.5 to 2.0] × 10−14 | <1 × 10−32 |
| MAP | 103 (2.7%) | 690 (18.1%) | −0.1 [−2.4 to 2.8] × 10−14 | <1 × 10−32 |
| HR | 18 (0.5%) | 1958 (51.3%) | −0.1 [−2.4 to 2.3] × 10−14 | <1 × 10−32 |
| O2Hb | 8 (0.2%) | 3032 (92.6%) | 0.8 [−1.0 to 2.9] × 10−14 | <1 × 10−32 |
| HHb | 28 (0.9%) | 1835 (56.1%) | 1.1 [−0.9 to 3.2] × 10−14 | <1 × 10−32 |
| TSI | 15 (0.5%) | 2280 (69.7%) | 1.0 [−1.0 to 2.8] × 10−14 | <1 × 10−32 |
| Stand (0–60s) N = 2583–3538 | ||||
| sBP | 267 (7.6%) | 1532 (43.3%) | <1 × 10−32 | <1 × 10−32 |
| dBP | 478 (13.5%) | 1283 (36.3%) | <1 × 10−32 | <1 × 10−32 |
| MAP | 817 (23.1%) | 1871 (52.9%) | <1 × 10−32 | <1 × 10−32 |
| HR | 85 (2.5%) | 2051 (58.0%) | <1 × 10−32 | <1 × 10−32 |
| O2Hb | 94 (3.6%) | 1913 (74.1%) | <1 × 10−32 | <1 × 10−32 |
| HHb | 82 (3.2%) | 1264 (48.9%) | <1 × 10−32 | <1 × 10−32 |
| TSI | 79 (3.1%) | 885 (34.3%) | <1 × 10−32 | <1 × 10−32 |
| Stand (120–180s) N = 2583–3365 | ||||
| sBP | 23 (0.7%) | 927 (27.6%) | <1 × 10−32 | <1 × 10−32 |
| dBP | 26 (0.8%) | 850 (25.3%) | <1 × 10−32 | <1 × 10−32 |
| MAP | 34 (1.0%) | 694 (20.6%) | <1 × 10−32 | <1 × 10−32 |
| HR | 14 (0.4%) | 1585 (47.1%) | <1 × 10−32 | <1 × 10−32 |
| O2Hb | 3 (0.1%) | 2266 (87.7%) | <1 × 10−32 | <1 × 10−32 |
| HHb | 22 (0.9%) | 1493 (57.8%) | <1 × 10−32 | <1 × 10−32 |
| TSI | 4 (0.2%) | 1766 (68.4%) | <1 × 10−32 | <1 × 10−32 |
Appendix B

References
- Fried, L.P.; Tangen, C.M.; Walston, J.D.; Newman, A.B.; Hirsch, C.; Gottdiener, J.S.; Seeman, T.E.; Tracy, R.P.; Kop, W.J.; Burke, G.L.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Rockwood, K.; Stadnyk, K.; Macknight, C.; McDowell, I.; Hébert, R.; Hogan, D.B. A brief clinical instrument to classify frailty in elderly people. Lancet 1999, 353, 205–206. [Google Scholar] [CrossRef]
- Speechley, M.; Tinetti, M. Falls and Injuries in Frail and Vigorous Community Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 46–52. [Google Scholar] [CrossRef]
- Winograd, C.H. Targeting strategies: An overview of criteria and outcomes. J. Am. Geriatr. Soc. 1991, 39, 25s–35s. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Olde Rikkert, M.G.M.; Melis, R.J.F. Rerouting Geriatric Medicine by Complementing Static Frailty Measures With Dynamic Resilience Indicators of Recovery Potential. Front. Physiol. 2019, 10, 723. [Google Scholar] [CrossRef]
- Maguire, F.; Romero-Ortuno, R.; O’Connor, J.; Reilly, R.; Knight, S.; Kenny, R. Orthostatic Cerebrovascular Response is Altered in Frailty: Findings from The Irish Longitudinal Study on Ageing; Journal of the American Geriatrics Society; WILEY 111 River St: Hoboken, NJ, USA, 2020; pp. S6–S7. [Google Scholar]
- Romero-Ortuno, R.; Cogan, L.; O’Shea, D.; Lawlor, B.; Kenny, R.A. Orthostatic haemodynamics may be impaired in frailty. Age Ageing 2011, 40, 576–583. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, M.D.L.; Savva, G.M.; Finucane, C.; Romero-Ortuno, R.; Fan, C.W.; Kenny, R.A. Impairments in Hemodynamic Responses to Orthostasis Associated with Frailty: Results from The Irish Longitudinal Study on Ageing (TILDA). J. Am. Geriatr. Soc. 2018, 66, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Dall, P.M.; Kerr, A. Frequency of the sit to stand task: An observational study of free-living adults. Appl. Ergon. 2010, 41, 58–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finucane, C.; O’Connell, M.D.; Fan, C.W.; Savva, G.M.; Soraghan, C.J.; Nolan, H.; Cronin, H.; Kenny, R.A. Age-related normative changes in phasic orthostatic blood pressure in a large population study: Findings from The Irish Longitudinal Study on Ageing (TILDA). Circulation 2014, 130, 1780–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, L.; Nolan, H.; Carey, D.; Reilly, R.B.; Kenny, R.A. Age and sex differences in frontal lobe cerebral oxygenation in older adults—Normative values using novel, scalable technology: Findings from the Irish Longitudinal Study on Ageing (TILDA). Arch. Gerontol. Geriatr. 2020, 87, 103988. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.D.; O’Connell, M.D.L.; Romero-Ortuno, R.; Hernández, B.; Newman, L.; Reilly, R.B.; Kenny, R.A.; Knight, S.P. Functional Analysis of Continuous, High-Resolution Measures in Aging Research: A Demonstration Using Cerebral Oxygenation Data From the Irish Longitudinal Study on Aging. Front. Hum. Neurosci. 2020, 14, 261. [Google Scholar] [CrossRef] [PubMed]
- Chon, K.H.; Scully, C.G.; Lu, S. Approximate entropy for all signals. IEEE Eng. Med. Biol. Mag. 2009, 28, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Fast Approximate Entropy. Available online: https://uk.mathworks.com/matlabcentral/fileexchange/32427-fast-approximate-entropy (accessed on 10 January 2020).
- Martínez-Cagigal, V. Sample Entropy. Available online: https://uk.mathworks.com/matlabcentral/fileexchange/69381-sample-entropy (accessed on 10 January 2020).
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Xia, Y.; Yang, C.; Zhang, L. The Review of the Major Entropy Methods and Applications in Biomedical Signal Research, International Symposium on Bioinformatics Research and Applications (ISBRA); Springer International Publishing: Beijing, China, 2018; pp. 87–100. [Google Scholar]
- Mayer, C.C.; Bachler, M.; Holzinger, A.; Stein, P.K.; Wassertheurer, S. The Effect of Threshold Values and Weighting Factors on the Association between Entropy Measures and Mortality after Myocardial Infarction in the Cardiac Arrhythmia Suppression Trial (CAST). Entropy 2016, 18, 129. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [Green Version]
- Chaves, P.H.M.; Varadhan, R.; Lipsitz, L.A.; Stein, P.K.; Windham, B.G.; Tian, J.; Fleisher, L.A.; Guralnik, J.M.; Fried, L.P. Physiological Complexity Underlying Heart Rate Dynamics and Frailty Status in Community-Dwelling Older Women. J. Am. Geriatr. Soc. 2008, 56, 1698–1703. [Google Scholar] [CrossRef]
- Rangasamy, V.; Henriques, T.S.; Xu, X.; Subramaniam, B. Preoperative Blood Pressure Complexity Indices as a Marker for Frailty in Patients Undergoing Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2020, 34, 616–621. [Google Scholar] [CrossRef]
- Takahashi, A.C.M.; Bonjorni, L.A.; Buto, M.S.S.; Vassimon-Barroso, V.; Minatel, V.; Rocha, S.M.A.; Ribeiro, F.H.M.; Montano, N.; Porta, A.; Catai, A.M. Short-term complexity of cardiovascular oscillations in frailty syndrome. In Proceedings of the 2014 8th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO), Trento, Italy, 25–28 May 2014; pp. 21–22. [Google Scholar]
- Xiong, J.; Liang, X.; Zhu, T.; Zhao, L.; Li, J.; Liu, C. A New Physically Meaningful Threshold of Sample Entropy for Detecting Cardiovascular Diseases. Entropy 2019, 21, 830. [Google Scholar] [CrossRef] [Green Version]
- Pincus, S.M.; Gladstone, I.M.; Ehrenkranz, R.A. A regularity statistic for medical data analysis. J. Clin. Monit. 1991, 7, 335–345. [Google Scholar] [CrossRef]
- Parvaneh, S.; Howe, C.; Toosizadeh, N.; Honarvar, B.; Slepian, M.J.; Fain, M.; Mohler, J.; Najafi, B. Regulation of Cardiac Autonomic Nervous System Control across Frailty Statuses: A Systematic Review. Gerontology 2015, 62, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef]
- Travers, J.; Romero-Ortuno, R.; Bailey, J.; Cooney, M.-T. Delaying and reversing frailty: A systematic review of primary care interventions. Br. J. Gen. Pract. 2019, 69, e61–e69. [Google Scholar] [CrossRef]
- Donoghue, O.A.; McGarrigle, C.A.; Foley, M.; Fagan, A.; Meaney, J.; Kenny, R.A. Cohort Profile Update: The Irish Longitudinal Study on Ageing (TILDA). Int. J. Epidemiol. 2018, 47, 1398–1398l. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Cronin, H.; O’Regan, C.; Kamiya, Y.; Savva, G.M.; Whelan, B.; Kenny, R. Cohort Profile: The Irish Longitudinal Study on Ageing. Int. J. Epidemiol. 2011, 40, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Whelan, B.J.; Savva, G.M. Design and Methodology of the Irish Longitudinal Study on Ageing. J. Am. Geriatr. Soc. 2013, 61, S265–S268. [Google Scholar] [CrossRef]
- Jasper, H.H. The ten twenty electrode system of the international federation. Electroencephalogr. Clin. Neurophysiol. 1958, 10, 371–375. [Google Scholar]
- Ferrari, M.; Quaresima, V. Near Infrared Brain and Muscle Oximetry: From the Discovery to Current Applications. J. Near Infrared Spectrosc. 2012, 20, 1–14. [Google Scholar] [CrossRef]
- O’Connor, J.D.; O’Connell, M.D.L.; Nolan, H.; Newman, L.; Knight, S.P.; Kenny, R.A. Impact of Standing Speed on the Peripheral and Central Hemodynamic Response to Orthostasis: Evidence From the Irish Longitudinal Study on Ageing. Hypertension 2020, 75, 524–531. [Google Scholar] [CrossRef]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The Appropriate Use of Approximate Entropy and Sample Entropy with Short Data Sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef]
- Delgado-Bonal, A.; Marshak, A. Approximate Entropy and Sample Entropy: A Comprehensive Tutorial. Entropy 2019, 21, 541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortelano, M.; Reilly, R.B.; Castells, F.; Cervigón, R. Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults with Orthostatic Intolerance. Entropy 2018, 20, 860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turianikova, Z.; Javorka, K.; Baumert, M.; Calkovska, A.; Javorka, M. The effect of orthostatic stress on multiscale entropy of heart rate and blood pressure. Physiol. Meas. 2011, 32, 1425–1437. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, A.M.; Finucane, C.; Savva, G.M.; Robertson, I.H.; Kenny, R.A. Sustained Attention and Frailty in the Older Adult Population. J. Gerontol. Ser. B 2014, 69, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Peklar, J.; O’Halloran, A.M.; Maidment, I.D.; Henman, M.C.; Kenny, R.A.; Kos, M. Sedative load and frailty among community-dwelling population aged ≥65 years. J. Am. Med. Dir. Assoc. 2015, 16, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; O’Regan, C.; Cronin, H.; Kenny, R.A. Using Timed Up-and-Go to Identify Frail Members of the Older Population. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 68, 441–446. [Google Scholar] [CrossRef]
- Donoghue, O.; O’Connell, M.; Kenny, R. Walking to Wellbeing: Physical Activity, Social Participation and Psychological Health in Irish Adults Aged 50 Years or Older. 2016. Available online: https://tilda.tcd.ie/publications/reports/pdf/ReportPhysicalActivity.pdf (accessed on 3 October 2020).
- Orme, J.G.; Reis, J.; Herz, E.J. Factorial and discriminant validity of the center for epidemiological studies depression (CES-D) scale. J. Clin. Psychol. 1986, 42, 28–33. [Google Scholar] [CrossRef]
- Ewing, J.A. Detecting alcoholism. The CAGE questionnaire. JAMA 1984, 252, 1905–1907. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E.; Allen, N.B. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol. Aging 1997, 12, 277–287. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Porta, A.; Castiglioni, P.; Di Rienzo, M.; Bari, V.; Bassani, T.; Marchi, A.; Takahashi, A.C.M.; Tobaldini, E.; Montano, N.; Catai, A.M.; et al. Short-term complexity indexes of heart period and systolic arterial pressure variabilities provide complementary information. J. Appl. Physiol. 2012, 113, 1810–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catai, A.; Takahashi, A.; Perseguini, N.; Milan, J.; Minatel, V.; Rehder-Santos, P.; Marchi, A.; Bari, V.; Porta, A. Effect of the Postural Challenge on the Dependence of the Cardiovascular Control Complexity on Age. Entropy 2014, 16, 6686–6704. [Google Scholar] [CrossRef] [Green Version]
- Porta, A.; Gnecchi-Ruscone, T.; Tobaldini, E.; Guzzetti, S.; Furlan, R.; Montano, N. Progressive decrease of heart period variability entropy-based complexity during graded head-up tilt. J. Appl. Physiol. 2007, 103, 1143–1149. [Google Scholar] [CrossRef]
- Wejer, D.; Graff, B.; Makowiec, D.; Budrejko, S.; Struzik, Z.R. Complexity of cardiovascular rhythms during head-up tilt test by entropy of patterns. Physiol. Meas. 2017, 38, 819–832. [Google Scholar] [CrossRef] [PubMed]
- Buto, M.S.D.S.; Catai, A.M.; De Vassimon-Barroso, V.; Gois, M.; Porta, A.; Takahashi, A.C.D.M. Baroreflex sensitivity in frailty syndrome. Braz. J. Med. Biol. Res. 2019, 52, e8079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberger, A. Non-linear dynamics for clinicians: Chaos theory, fractals, and complexity at the bedside. Lancet 1996, 347, 1312–1314. [Google Scholar] [CrossRef]
- De Lucia, C.; Eguchi, A.; Koch, W.J. New Insights in Cardiac β-Adrenergic Signaling During Heart Failure and Aging. Front. Pharmacol. 2018, 9, 904. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M255–M263. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, M.D.; Savva, G.M.; Fan, C.W.; Kenny, R.A. Orthostatic hypotension, orthostatic intolerance and frailty: The Irish Longitudinal Study on Aging-TILDA. Arch. Gerontol. Geriatr. 2015, 60, 507–513. [Google Scholar] [CrossRef]
- Roe, L.; Normand, C.; Wren, M.-A.; Browne, J.; O’Halloran, A.M. The impact of frailty on healthcare utilisation in Ireland: Evidence from the Irish longitudinal study on ageing. BMC Geriatr. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Mesin, L. Estimation of Complexity of Sampled Biomedical Continuous Time Signals Using Approximate Entropy. Front. Physiol. 2018, 9, 710. [Google Scholar] [CrossRef] [PubMed]
- Magagnin, V.; Bassani, T.; Bari, V.; Turiel, M.; Maestri, R.; Pinna, G.D.; Porta, A. Non-stationarities significantly distort short-term spectral, symbolic and entropy heart rate variability indices. Physiol. Meas. 2011, 32, 1775–1786. [Google Scholar] [CrossRef] [PubMed]



| BP Cohort (n = 2645) | NIRS Cohort (n = 2225) | |
|---|---|---|
| Age [years] | 64.3 (SD: 7.7, range: [50–93]) | 64.3 (SD: 7.7, range: [50–93]) |
| Sex [% (n)] | Female: 53.0% (1401) | Female: 52.3% (1163) |
| Education [% (n)] | ||
| Primary/none | 16.5% (436) | 16.5% (368) |
| Secondary | 39.9% (1055) | 40.1% (891) |
| Third/higher | 43.6% (1154) | 43.4% (966) |
| Frailty Phenotype [% (n)] | ||
| Non-frail | 59.1% (1564) | 59.5% (1325) |
| Pre-frail | 37.2% (984) | 36.7% (816) |
| Frail | 3.7% (97) | 3.8% (84) |
| Disability [% (n)] | ||
| Number of ADL disabilities | ||
| Non-frail | ||
| 0 | 98.9% (1547) | 98.9% (1310) |
| 1 | 1.0% (15) | 1.0% (13) |
| +2 | 0.1% (2) | 0.1% (2) |
| Pre-frail | ||
| 0 | 96.1% (946) | 96.3% (786) |
| 1 | 2.3% (23) | 2.1% (17) |
| +2 | 1.6% (15) | 1.6% (13) |
| Frail | ||
| 0 | 79.4% (77) | 78.6% (66) |
| 1 | 13.4% (13) | 15.5% (13) |
| +2 | 7.2% (7) | 5.9% (5) |
| No. of Cardiovascular Conditions a [% (n)] | ||
| 0 | 40.4% (1069) | 40.6% (904) |
| 1 | 35.6% (942) | 35.9% (768) |
| 2+ | 24.0% (634) | 23.5% (523) |
| Self-reported diabetic [%] | 6.8% (179) | 6.5% (144) |
| Antihypertensive medications b [% (n)] | 37.7% (997) | 37.2% (827) |
| CAGE alcohol scale | ||
| CAGE < 2 | 76.7% (2029) | 77.2% (1718) |
| CAGE ≥ 2 | 12.4% (328) | 12.3% (274) |
| No response | 10.9% (288) | 10.5% (233) |
| Smoker [% (n)] | ||
| Never | 47.9% (1268) | 48.0% (1067) |
| Past | 42.6% (1127) | 42.5% (945) |
| Current | 9.5% (250) | 9.5% (213) |
| CESD [% (n)] | ||
| Non-depressed (CESD < 9) | 89.1% (2358) | 89.3% (1986) |
| Depressed (CESD ≥ 9) | 10.9% (287) | 10.7% (239) |
| Time to stand [seconds] | 7.2 (SD: 2.8, range: [2–27]) | 7.2 (SD: 2.8, range: [2–26]) |
| ApEn | Non-Frail (N = 1325–1564) | Pre-Frail (N = 816–984) | Frail (N = 84–97) |
|---|---|---|---|
| Resting State | Mean (SD, [Range]) | Mean (SD, [Range]) | Mean (SD, [Range]) |
| sBP | 0.52 (0.07, [0.26–0.98]) | 0.54 (0.08, [0.22–0.77]) | 0.56 (0.08, [0.31–0.75]) |
| dBP | 0.45 (0.08, [0.20–0.96]) | 0.47 (0.09, [0.22–0.78]) | 0.50 (0.11, [0.29–0.83]) |
| MAP | 0.46 (0.08, [0.17–1.01]) | 0.48 (0.08, [0.22–0.79]) | 0.52 (0.09, [0.30–0.80]) |
| HR | 0.49 (0.09, [0.02–0.81]) | 0.49 (0.09, [0.05–0.77]) | 0.51 (0.10, [0.29–0.77]) |
| O2Hb | 0.44 (0.07, [0.16–0.68]) | 0.45 (0.07, [0.18–0.65]) | 0.46 (0.07, [0.23–0.60]) |
| HHb | 0.43 (0.07, [0.09–0.65]) | 0.43 (0.07, [0.16–0.64]) | 0.45 (0.07, [0.27–0.60]) |
| TSI | 0.39 (0.06, [0.12–0.62]) | 0.40 (0.07, [0.11–0.63]) | 0.41 (0.06, [0.28–0.54]) |
| Stand (0–60s) | |||
| sBP | 0.44 (0.07, [0.20–0.97]) | 0.46 (0.08, [0.21–0.80]) | 0.48 (0.08, [0.33–0.70]) |
| dBP | 0.40 (0.07, [0.17–0.90]) | 0.42 (0.09, [0.19–0.83]) | 0.45 (0.10, [0.25–0.76]) |
| MAP | 0.41 (0.08, [0.17–0.93]) | 0.43 (0.08, [0.18–0.82]) | 0.45 (0.09, [0.30–0.80]) |
| HR | 0.45 (0.08, [0.07–0.80]) | 0.46 (0.09, [0.18–0.95]) | 0.49 (0.11, [0.23–0.81]) |
| O2Hb | 0.79 (0.12, [0.36–1.37]) | 0.80 (0.12, [0.32–1.34]) | 0.79 (0.14 [0.38–1.08]) |
| HHb | 0.69 (0.14, [0.21–1.37]) | 0.70 (0.15, [0.30–1.36]) | 0.69 (0.14, [0.40–0.99]) |
| TSI | 0.77 (0.12, [0.40–1.39]) | 0.79 (0.12, [0.41–1.33]) | 0.79 (0.12, [0.53–1.08]) |
| Stand (120–180s) | |||
| sBP | 0.55 (0.07, [0.29–1.04]) | 0.56 (0.07, [0.33–0.84]) | 0.58 (0.07, [0.39–0.78]) |
| dBP | 0.49 (0.08, [0.27–1.02]) | 0.50 (0.09, [0.26–0.85]) | 0.53 (0.10, [0.32–0.84]) |
| MAP | 0.51 (0.07, [0.22–1.01]) | 0.52 (0.08, [0.26–0.81]) | 0.54 (0.09, [0.28–0.84]) |
| HR | 0.49 (0.08, [0.02–0.88]) | 0.50 (0.09, [0.23–0.85]) | 0.52 (0.11, [0.20–0.79]) |
| O2Hb | 0.91 (0.12, [0.43–1.40]) | 0.91 (0.12, [0.55–1.37]) | 0.92 (0.13 [0.50–1.12]) |
| HHb | 0.87 (0.14, [0.40–1.42]) | 0.88 (0.14, [0.42–1.36]) | 0.90 (0.11, [0.62–1.18]) |
| TSI | 0.92 (0.11, [0.50–1.34]) | 0.92 (0.11, [0.59–1.34]) | 0.95 (0.11, [0.60–1.15]) |
| SampEn | Non-Frail (N = 1325–1564) | Pre-Frail (N = 816–984) | Frail (N = 84–97) |
|---|---|---|---|
| Resting State | Mean (SD, [Range]) | Mean (SD, [Range]) | Mean (SD, [Range]) |
| sBP | 0.49 (0.13, [0.07–1.41]) | 0.51 (0.14, [0.08–0.93]) | 0.55 (0.14, [0.15–0.87]) |
| dBP | 0.39 (0.13, [0.06–1.34]) | 0.41 (0.13, [0.06–0.95]) | 0.45 (0.16, [0.18–0.99]) |
| MAP | 0.40 (0.13, [0.05–1.27]) | 0.43 (0.14, [0.08–0.84]) | 0.48 (0.15, [0.15–0.89]) |
| HR | 0.44 (0.15, [0.01–1.00]) | 0.44 (0.16, [0.02–1.03]) | 0.46 (0.19, [0.08–0.99]) |
| O2Hb | 0.34 (0.14, [0.01–0.71]) | 0.35 (0.14, [0.05–0.78]) | 0.38 (0.14, [0.07–0.67]) |
| HHb | 0.31 (0.13, [0.03–0.80]) | 0.32 (0.14, [0.04–0.72]) | 0.36 (0.14, [0.12–0.62]) |
| TSI | 0.26 (0.10, [0.03–0.72]) | 0.27 (0.11, [0.03–0.74]) | 0.28 (0.11, [0.06–0.52]) |
| Stand (0–60 s) | |||
| sBP | 0.30 (0.12, [0.04–1.26]) | 0.32 (0.13, [0.04–0.98]) | 0.35 (0.14, [0.12–0.82]) |
| dBP | 0.20 (0.11, [0.03–1.03]) | 0.22 (0.14, [0.04–1.03]) | 0.28 (0.16, [0.03–0.87]) |
| MAP | 0.24 (0.11, [0.04–1.11]) | 0.26 (0.13, [0.04–0.92]) | 0.30 (0.15, [0.05–0.99]) |
| HR | 0.31 (0.14, [0.02–1.08]) | 0.33 (0.17, [0.03–1.21]) | 0.40 (0.21, [0.03–1.05]) |
| O2Hb | 0.73 (0.37, [0.04–2.69]) | 0.74 (0.39, [0.01–2.70]) | 0.68 (0.38, [0.03–1.54]) |
| HHb | 0.44 (0.33, [0.02–2.88]) | 0.47 (0.35, [0.01–2.80]) | 0.44 (0.29, [0.03–1.30]) |
| TSI | 0.61 (0.36, [0.07–2.73]) | 0.64 (0.36, [0.06–2.63]) | 0.67 (0.36, [0.12–1.67]) |
| Stand (120–180 s) | |||
| sBP | 0.52 (0.13, [0.14–1.28]) | 0.53 (0.13, [0.10–1.13]) | 0.57 (0.14, [0.27–0.96]) |
| dBP | 0.43 (0.13, [0.10–1.57]) | 0.44 (0.14, [0.10–1.10]) | 0.50 (0.19, [0.13–1.17]) |
| MAP | 0.47 (0.13, [0.06–1.50]) | 0.48 (0.14, [0.09–0.99]) | 0.51 (0.16, [0.11–1.07]) |
| HR | 0.42 (0.14, [0.01–1.06]) | 0.44 (0.16, [0.03–1.12]) | 0.47 (0.19, [0.08–0.98]) |
| O2Hb | 1.16 (0.38, [0.06–2.77]) | 1.16 (0.39, [0.09–2.57]) | 1.15 (0.39, [0.09–1.91]) |
| HHb | 0.89 (0.42, [0.07–2.80]) | 0.93 (0.45, [0.06–2.60]) | 0.97 (0.42, [0.12–2.05]) |
| TSI | 1.08 (0.36, [0.15–2.58]) | 1.08 (0.37, [0.15–2.78]) | 1.18 (0.36, [0.28–2.18]) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knight, S.P.; Newman, L.; O’Connor, J.D.; Davis, J.; Kenny, R.A.; Romero-Ortuno, R. Associations between Neurocardiovascular Signal Entropy and Physical Frailty. Entropy 2021, 23, 4. https://doi.org/10.3390/e23010004
Knight SP, Newman L, O’Connor JD, Davis J, Kenny RA, Romero-Ortuno R. Associations between Neurocardiovascular Signal Entropy and Physical Frailty. Entropy. 2021; 23(1):4. https://doi.org/10.3390/e23010004
Chicago/Turabian StyleKnight, Silvin P., Louise Newman, John D. O’Connor, James Davis, Rose Anne Kenny, and Roman Romero-Ortuno. 2021. "Associations between Neurocardiovascular Signal Entropy and Physical Frailty" Entropy 23, no. 1: 4. https://doi.org/10.3390/e23010004
APA StyleKnight, S. P., Newman, L., O’Connor, J. D., Davis, J., Kenny, R. A., & Romero-Ortuno, R. (2021). Associations between Neurocardiovascular Signal Entropy and Physical Frailty. Entropy, 23(1), 4. https://doi.org/10.3390/e23010004