
Recycling Antibiotics into GUMBOS: A New Combination Strategy to Combat Multi-Drug-Resistant Bacteria


Abstract
:1. Introduction


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strain | Abbreviation | Characteristic |
|---|---|---|
| Escherichia coli 29522 + | EC 29522 | Clinical isolate, quality control organism |
| Escherichia coli O157:H7 43895 + | EC 43895 | EHEC, hamburger isolate (stx1+, stx2+) |
| Salmonella typhi ++ | Styphi | Fluoroquinolone resistant |
| Acinetobacter baumannii 225T2 ++ | AB 225T2 | Respiratory isolate, multi-drug resistant * |
| Acinetobacter baumannii 250 ++ | AB 250 | Skin isolate, multi-drug resistant |
| Acinetobacter baumannii 252 ++ | AB 252 | Catheter isolate, multi-drug resistant |
| Acinetobacter baumannii 254 ++ | AB 254 | Wound drain isolate, multi-drug resistant |
| Enterobacter cloacae 210T2 ++ | EC 210T2 | Pleural fluid isolate, multi-drug resistant |
| Enterobacter aerogenes 221T2 ++ | EA 221T2 | Sputum, multi-drug resistant |
| Klebsiella pneumoniae 10031 + | KP 10031 | Quality control organism |
| Klebsiella pneumoniae 50T2 ++ | KP 50T2 | Urine isolate, multi-drug resistant |
| Klebsiella pneumoniae 86T2 ++ | KP 86T2 | Pleural fluid isolate, multi-drug resistant |
| Pseudomonas aeruginosa 124T2 ++ | PA 124T2 | Respiratory: sputum isolate, β-lactam drug resistant |
| Pseudomonas aeruginosa 27853 + | PA 27853 | Blood isolate, quality control organism |
| Pseudomonas aeruginosa PSA3 ++ | PSA 3 | Urine Isolate, β-lactam drug resistant |
| Pseudomonas aeruginosa PSA4 ++ | PSA 4 | Sputum isolate, β-lactam, fluoroquinolone, carbapenem drug resistant |
| Serratia marcescens ++ | SM | Wound isolate, multi-drug resistant |
| Staphylococcus aureus 25923 + | SA 25923 | Clinical isolate |
| Streptococcus mutans35668 + | SM 35668 | Quality control organism |
| Streptococcus faecalis 19433 + | SF 19433 | Quality control organism |
| Micrococcus luteus 4698 + | ML 4698 | Quality control organism |
| Streptococcus faecalis 9790 + | SF 9790 | Quality control organism |
| Bacillus cereus 1178 + | BC 1178 | Quality control organism |
| Methicillin-resistant Staphylococcus aureus | CA-MRSA 2 | Wound isolate, vancomycin susceptible |
| Methicillin-resistan ++CA-MRSA 2 Staphylococcus aureus ++ CA-MRSA 1 | CA-MRSA 1 | Prosthetic joint infection isolate, vancomycin susceptible |
2. Results and Discussion
2.1. Aqueous Solubility, Dissolution and Theoretical Intestinal Absorption
| Antimicrobial Agent a | Solubility, mg/mL | Dissolution Rate (k), min−1 | Permeability Coefficients, cm/s (SD) | Log Permeability Coefficients | % HIA c |
|---|---|---|---|---|---|
| CHX Ac | 10 | na b | 9.39 × 10−7 (±0.87) | −6.10 | 77.4 |
| CHX Amp | 0.126 | 0.0188 | 4.03 × 10−6 (±1.03) | −5.39 | 101.9 |
| CHX Carb | 0.055 | 0.0022 | 3.67 × 10−6 (±0.074) | −5.43 | 100.4 |
| CHX Ceph | 0.079 | 0.0037 | 4.98 × 10−6 (±0.082) | −5.30 | 105.5 |
| CHX Oxa | 0.166 | 0.0189 | 4.91 × 10−6 (±0.17) | −5.31 | 105.3 |
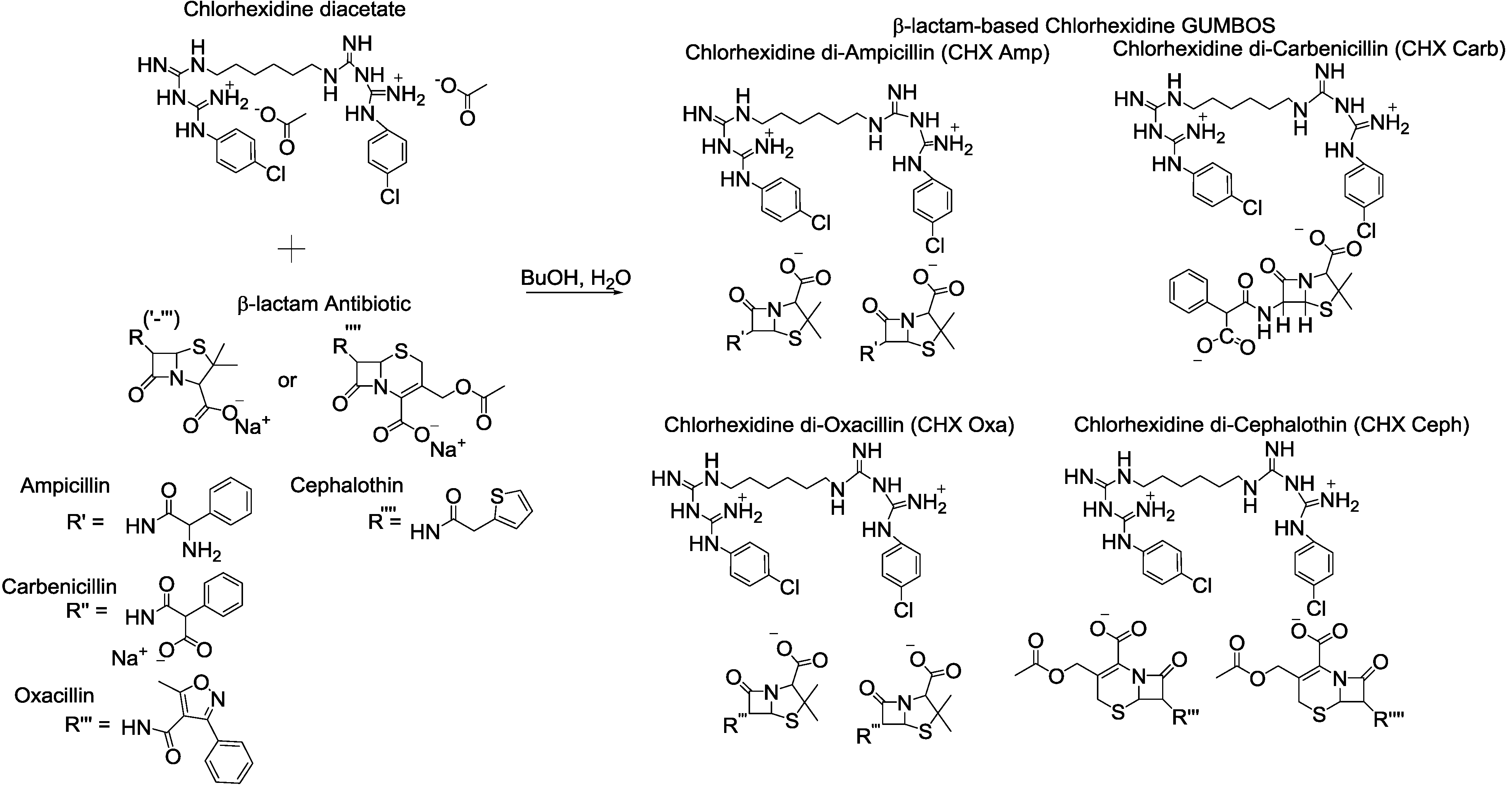
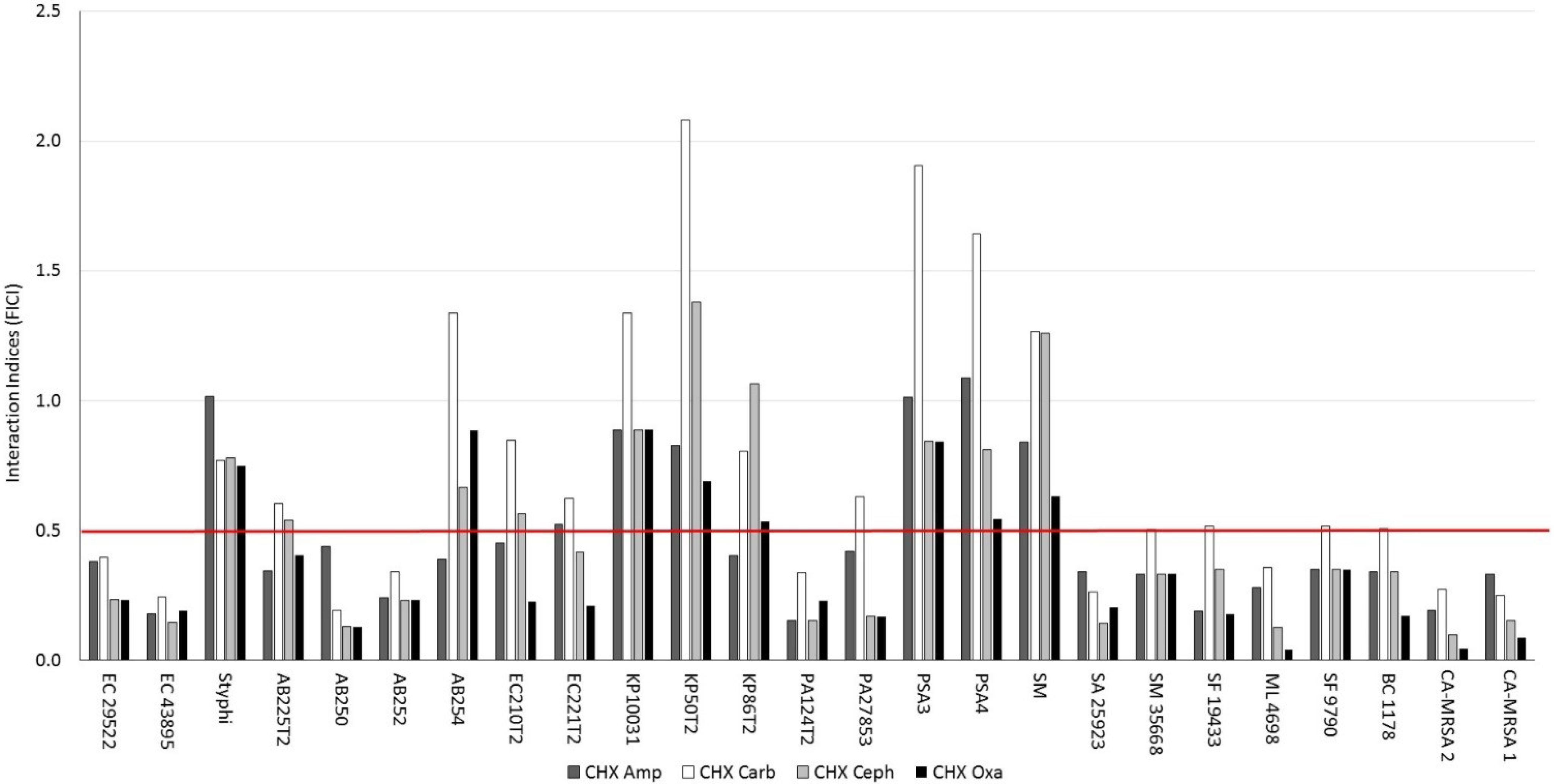
2.2. Antibacterial Activities of β-Lactam-Based Chlorhexidine GUMBOS
| Antibacterial Agent b | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Gram-Positive Bacteria | Amp | Carb | Ceph | Oxa | CHX Ac | CHX Amp | CHX Carb | CHX Ceph | CHX Oxa |
| SA 25923 | 2 | 13 | 125 | 125 | 1 | 0.9 | 0.5 | 0.4 | 0.5 |
| SM 35668 | 0.8 | 94 | 104 | 98 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 |
| SF 19433 | 0.2 | 0.1 | 0.1 | 0.1 | 0.8 | 0.4 | 0.8 | 0.8 | 0.4 |
| ML 4698 | 625 | >1250 | >1250 | >1250 | 0.8 | 0.6 | 0.5 | 0.3 | 0.1 |
| SF 9790 | 625 | >1250 | >1250 | >1250 | 0.8 | 0.8 | 0.8 | 0.8 | 0.8 |
| BC 1178 | 625 | >1250 | >1250 | >1250 | 0.4 | 0.4 | 0.4 | 0.4 | 0.2 |
| CA-MRSA 2 | 625 | >1250 | >1250 | >1250 | 1 | 0.8 | 0.7 | 0.4 | 0.2 |
| CA-MRSA 1 | >1250 | >1250 | >1250 | >1250 | 0.7 | 0.7 | 0.3 | 0.3 | 0.2 |
| Antibacterial Agent b | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Gram-Negative Bacteria | Amp | Carb | Ceph | Oxa | CHX Ac | CHX Amp | CHX Carb | CHX Ceph | CHX Oxa |
| EC 29522 | >1250 | >1250 | >1250 | >1250 | 0.3 | 0.3 | 0.2 | 0.2 | 0.2 |
| EC 43895 | >1250 | >1250 | >1250 | >1250 | 0.2 | 0.1 | 0.1 | 0.1 | 0.1 |
| Styphi | >1250 | >1250 | >1250 | >1250 | 0.2 | 0.2 | 0.1 | 0.1 | 0.1 |
| AB 225T2 | >1250 | >1250 | >1250 | >1250 | 12 | 12 | 15 | 20 | 15 |
| AB 250 | >1250 | >1250 | >1250 | >1250 | 20 | 24 | 7 | 7 | 7 |
| AB 252 | >1250 | >1250 | >1250 | >1250 | 29 | 20 | 20 | 20 | 20 |
| AB 254 | >1250 | >1250 | >1250 | >1250 | 4 | 4 | 10 | 7 | 10 |
| EC 210T2 | >1250 | >1250 | >1250 | >1250 | 15 | 20 | 24 | 24 | 10 |
| EA 221T2 | >1250 | >1250 | >1250 | >1250 | 16 | 24 | 20 | 20 | 10 |
| KP 10031 | 27 | 22 | 29 | 17 | 5 | 13 | 13 | 13 | 13 |
| KP 50T2 | 540 | 270 | 270 | 215 | 5 | 12 | 20 | 20 | 10 |
| KP 86T2 | 14 | 28 | 28 | 28 | 6 | 7 | 10 | 20 | 10 |
| PA 124T2 | 10 | 10 | 10 | 5 | 22 | 10 | 15 | 10 | 15 |
| PA 27853 | 28 | 28 | 28 | 28 | 6 | 8 | 8 | 3 | 3 |
| PSA 3 | 32 | 39 | 27 | 45 | 4 | 12 | 15 | 10 | 10 |
| PSA 4 | >1250 | >1250 | >1250 | >1250 | 6 | 20 | 20 | 15 | 10 |
| SM | >1250 | >1250 | >1250 | >1250 | 9 | 22 | 22 | 32 | 16 |
| CHX Amp | 1 CHX:2 Amp | CHX Carb | 1 CHX:1 Carb | CHX Ceph | 1 CHX:2 Ceph | CHX Oxa | 1 CHX:2 Oxa | |
|---|---|---|---|---|---|---|---|---|
| SA 25923 | ||||||||
| MIC | 0.9 | 2.4 | 0.5 | 18.8 | 0.4 | 9.4 | 0.5 | 2.0 |
| FICI b | 0.3 | 0.2 | 0.3 | 7.1 | 0.1 | 3.4 | 0.2 | 1.3 |
| Effect | syn | syn | syn | ant | syn | add | syn | add |
| KP 10031 | ||||||||
| MIC | 12.5 | 37.5 | 12.5 | 37.5 | 12.5 | 18.8 | 12.5 | 18.8 |
| FICI | 0.9 | 2.7 | 1.3 | 2.7 | 0.9 | 1.5 | 0.9 | 2.0 |
| Effect | add | add | add | add | add | add | add | add |
| PA 27853 | ||||||||
| MIC | 7.8 | 18.8 | 7.8 | 18.8 | 3.1 | 9.4 | 3.1 | 18.8 |
| FICI | 0.4 | 1.3 | 0.6 | 1.5 | 0.2 | 0.8 | 0.2 | 1.5 |
| Effect | syn | add | add | add | syn | add | syn | add |
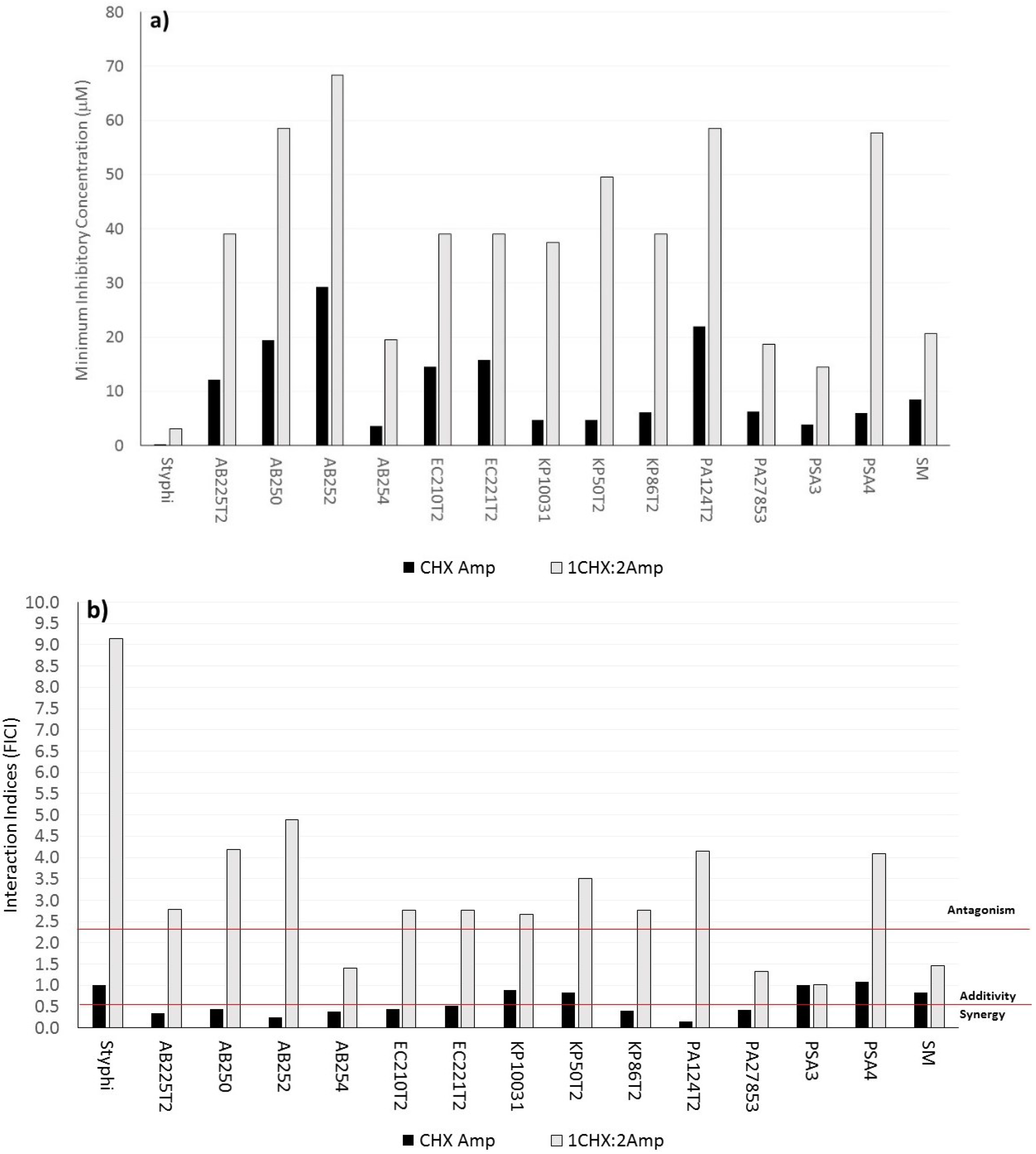
2.3. Comparison of Antibacterial Activity between Reacted β-Lactam-Based Chlorhexidine GUMBOS and Its Unreacted Mixtures


2.4. Cytotoxicity and Therapeutic Indices of Chlorhexidine and β-Lactam Antibiotics in Combination and as GUMBOS
| Antibacterial Agents a | Cervical | Fibroblasts | Endothelial |
|---|---|---|---|
| CHX Ac | 43 ± 3 | 47 ± 2 | 80 ± 3 |
| 1 CHX:2 Amp | 76 ± 4 | 43 ± 2 | 67 ± 11 |
| CHX Amp | 149 ± 8 | 48 ± 3 | 109 ± 6 |
| 1 CHX:1 Carb | 58 ± 3 | 51 ± 4 | 59 ± 4 |
| CHX Carb | 44 ± 2 | 48 ± 7 | 73 ± 10 |
| 1 CHX:2 Ceph | 65 ± 6 | 52 ± 6 | 103 ± 14 |
| CHX Ceph | 79 ± 2 | 52 ± 5 | 150 ± 13 |
| 1 CHX:2 Oxa | 92 ± 3 | 44 ± 4 | 92 ± 7 |
| CHX Oxa | 139 ± 8 | 48 ± 4 | 97 ± 16 |

2.5. Limitations
3. Experimental Section
3.1. Antibacterial Agents
3.2. Synthesis of β-Lactam-Based Chlorhexidine GUMBOS
3.3. Bacterial Strains
3.4. Media
3.5. Minimum Inhibitory Concentrations and Synergy Experiments
3.6. Interaction Indices and Synergy Testing
3.7. Dissolution Profile Measurement
3.8. In Vivo Prediction of Intestinal Permeability Coefficients and Absorption
3.9. Mammalian Cytotoxicity
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Boucher, H.W.; Talbot, G.H.; Bradley, J.S.; Edwards, J.E.; Gilbert, D.; Rice, L.B.; Scheld, M.; Spellberg, B.; Bartlett, J. Bad bugs, no drugs: No ESKAPE! An update from the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1–12. [Google Scholar] [CrossRef]
- Hogberg, L.D.; Heddini, A.; Cars, O. The global need for effective antibiotics: Challenges and recent advances. Trends Pharmacol. Sci. 2010, 31, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R. The use of systemic antibiotics in the treatment of chronic wounds. Dermatol. Ther. 2006, 19, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.; Nailor, M.D. Combination antibiotic therapy for empiric and definitive treatment of Gram-negative infections: Insights from the Society of Infectious Diseases Pharmacists. Pharmacotherpy 2011, 31, 1073–1084. [Google Scholar] [CrossRef]
- Ahmad, I.; Aqil, F. New Strategies Combating Bacterial Infection; John Wiley & Sons: Weinhem, Germany, 2009; p. 384. [Google Scholar]
- Tängdén, T. Combination antibiotic therapy for multidrug-resistant Gram-negative bacteria. Upsala J. Med. Sci. 2014, 119, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, M.; Mehrgan, H.; Hadji-Nejad, S. Enhancement of vancomycin activity by phenothiazines against vancomycin-resistant Enterococcus faecium in vitro. Basic Clin. Pharmacol. Toxicol. 2010, 107, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Jeyaseeli, L.; Dasgupta, A.; Dastidar, S.G.; Molnar, J.; Amaral, L. Evidence of significant synergism between antibiotics and the antipsychotic, antimicrobial drug flupenthixol. Eur. J. Clin. Microbiol. Infect Dis. 2012, 31, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Carson, C.F.; Riley, T.V. Non-antibiotic therapies for infectious diseases. Commun. Dis. Intell. 2003, 27 (Suppl.), S143–S146. [Google Scholar]
- Chattopadhyay, D.; Das, S.K.; Patra, A.R.; Bhattacharya, S.K. Non-antibiotics—An alternative for microbial resistance: Scope and hope. In New Strategies Combating Bacterial Infection; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2009; pp. 89–125. [Google Scholar]
- Kristiansen, J.E.; Hendricks, O.; Delvin, T.; Butterworth, T.S.; Aagaard, L.; Christensen, J.B.; Flores, V.C.; Keyzer, H. Reversal of resistance in microorganisms by help of non-antibiotics. J. Antimicrob. Chemother. 2007, 59, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.; Dastidar, S.G.; Fanning, S.; Kristiansen, J.E.; Molnar, J.; Pages, J.M.; Schelz, Z.; Spengler, G.; Viveiros, M.; Amaral, L. Potential role of non-antibiotics (helper compounds) in the treatment of multidrug-resistant Gram-negative infections: Mechanisms for their direct and indirect activities. Int. J. Antimicrob. Agents 2008, 31, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Ejim, L.; Farha, M.A.; Falconer, S.B.; Wildenhain, J.; Coombes, B.K.; Tyers, M.; Brown, E.D.; Wright, G.D. Combinations of antibiotics and nonantibiotic drugs enhance antimicrobial efficacy. Nat. Chem. Biol. 2011, 7, 348–350. [Google Scholar] [CrossRef] [PubMed]
- Trumic, E.; Pranjic, N.; Begic, L.; Becic, F.; Asceric, M. Idiosyncratic adverse reactions of most frequent drug combinations longterm use among hospitalized patients with polypharmacy. Med. Arch. 2012, 66, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Safdar, N.; Kethireddy, S.; Chateau, D. A survival benefit of combination antibiotic therapy for serious infections associated with sepsis and septic shock is contingent only on the risk of death: A meta-analytic/meta-regression study. Crit. Care Med. 2010, 38, 1651–1664. [Google Scholar] [CrossRef] [PubMed]
- Hagihara, M.; Crandon, J.L.; Nicolau, D.P. The efficacy and safety of antibiotic combination therapy for infections caused by Gram-positive and Gram-negative organisms. Expert Opin. Drug Saf. 2012, 11, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Marcus, R.; Paul, M.; Elphick, H.; Leibovici, L. Clinical implications of β-lactam-aminoglycoside synergism: Systematic review of randomised trials. Int. J. Antimicrob. Agents 2011, 37, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Brunkhorst, F.M.; Oppert, M.; Marx, G.; Bloos, F.; Ludewig, K.; Putensen, C.; Nierhaus, A.; Jaschinski, U.; Meier-Hellmann, A.; Weyland, A.; et al. Effect of empirical treatment with moxifloxacin and meropenem vs meropenem on sepsis-related organ dysfunction in patients with severe sepsis: A randomized trial. JAMA 2012, 307, 2390–2399. [Google Scholar]
- Ho, J.; Tambyah, P.A.; Paterson, D.L. Multi-resistant Gram-negative infections: A global perspective. Curr. Opin. Infect Dis. 2010, 23, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Pena-Miller, R.; Lahnemann, D.; Schulenburg, H.; Ackermann, M.; Beardmore, R. The optimal deployment of synergistic antibiotics: A control-theoretic approach. J. R. Soc. Interface 2012, 9, 2488–2502. [Google Scholar] [CrossRef] [PubMed]
- Warner, I.M.; El-Zahab, B.; Siraj, N. Perspectives on moving ionic liquid chemistry into the solid phase. Anal. Chem. 2014, 86, 7184–7191. [Google Scholar] [CrossRef] [PubMed]
- Warner, I.M.; Tesfai, A.; El-Zahab, B.M.; Bwambok, D.; Baker, G.A.; Fakayode, S.O.; Lowry, M.; Tolocka, M.P.; de Rooy, S. Frozen Ionic Liquid Microparticles and Nanoparticles, and Methods for Their Synthesis and Use. U.S. Patent 2,008,086,065, 8 September 2011. [Google Scholar]
- Magut, P.K.S.; Das, S.; Fernand, V.E.; Losso, J.; McDonough, K.; Naylor, B.M.; Aggarwal, S.; Warner, I.M. Tunable cytotoxicity of rhodamine 6G via anion variations. J. Am. Chem. Soc. 2013, 135, 15873–15879. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.R.; Li, M.; Jadeja, R.; El-Zahab, B.; Hayes, D.; Hobden, J.A.; Janes, M.E.; Warner, I.M. Minimizing human infection from Escherichia coli O157:H7 using GUMBOS. J. Antimicrob. Chemother. 2013, 68, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Binnemans, K. Ionic liquids. Chem. Rev. 2006, 105, 4128–4204. [Google Scholar]
- Bica, K.; Rijksen, C.; Nieuwenhuyzen, M.; Rogers, R.D. In search of pure liquid salt forms of aspirin: Ionic liquid approaches with acetylsalicylic acid and salicylic acid. Phys. Chem. Chem. Phys. 2010, 12, 2011–2017. [Google Scholar] [CrossRef] [PubMed]
- Hough-Troutman, W.L.; Smiglak, M.; Rodriguez, H.; Swatloski, R.P.; Spear, S.K.; Daly, D.T.; Pernak, J.; Grisel, J.E.; Carliss, R.D.; Soutullo, M.D.; et al. The third evolution of ionic liquids: Active pharmaceutical ingredients. New J. Chem. 2007, 31, 1429–1436. [Google Scholar]
- Rodríguez, H.; Bica, K.; Rogers, R.D. Ionic liquid technology: A potential new platform for the pharmaceutical industry. Trop. J. Pharm. Res. 2008, 7, 1011–1012. [Google Scholar]
- Kraus, C.A. The ion-pair concept, its evolution and some applications. J. Phys. Chem. 1956, 60, 129–141. [Google Scholar] [CrossRef]
- Hancock, R.E.; Wong, P.G. Compounds which increase the permeability of the Pseudomonas aeruginosa outer membrane. Antimicrob. Agents Chemother. 1984, 26, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Helander, I.M.; Latva-Kala, K.; Lounatmaa, K. Permeabilizing action of polyethyleneimine on Salmonella typhimurium involves disruption of the outer membrane and interactions with lipopolysaccharide. Microbiology 1998, 144, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Lengsfeld, C.S.; Pitera, D.; Manning, M.; Randolph, T.W. Dissolution and partitioning behavior of hydrophobic ion-paired compounds. Pharm. Res. 2002, 19, 1572–1576. [Google Scholar] [CrossRef] [PubMed]
- Hough-Troutman, W.L.; Smiglak, M.; Griffin, S.; Reichert, W.M.; Mirska, I.; Jodynis-Leibert, J.; Adamska, T.; Nawrot, J.; Stasiewicz, M.; Rogers, R.D.; et al. Ionic liquids with dual biological function: Sweet and anti-microbial, hydrophobic quaternary ammonium-based salts. New J. Chem. 2009, 33, 26–33. [Google Scholar]
- Anslyn, E.V.; Dougherty, D.A. Modern Physical Organic Chemistry; University Science Books: Sausalito, CA, USA, 2006. [Google Scholar]
- Jencks, W.P. Catalysis in Chemistry and Enzymology; McGraw-Hill: New York, NY, USA, 1969. [Google Scholar]
- Kaiser, N.; Klein, D.; Karanja, P.; Greten, Z.; Newman, J. Inactivation of chlorhexidine gluconate on skin by incompatible alcohol hand sanitizing gels. Am. J. Infect. Control 2009, 37, 569–573. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, G.; Russell, A.D. Antiseptics and disinfectants: Activity, action, and resistance. Clin. Microbiol. Rev. 1999, 12, 147–179. [Google Scholar] [PubMed]
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound healing dressings and drug delivery systems: A review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Hoey, C. Topical antimicrobial therapy for treating chronic wounds. Clin. Infect Dis. 2009, 49, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Sample Availability: Samples of the compounds are available from the authors.
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cole, M.R.; Hobden, J.A.; Warner, I.M. Recycling Antibiotics into GUMBOS: A New Combination Strategy to Combat Multi-Drug-Resistant Bacteria. Molecules 2015, 20, 6466-6487. https://doi.org/10.3390/molecules20046466
Cole MR, Hobden JA, Warner IM. Recycling Antibiotics into GUMBOS: A New Combination Strategy to Combat Multi-Drug-Resistant Bacteria. Molecules. 2015; 20(4):6466-6487. https://doi.org/10.3390/molecules20046466
Chicago/Turabian StyleCole, Marsha R., Jeffery A. Hobden, and Isiah M. Warner. 2015. "Recycling Antibiotics into GUMBOS: A New Combination Strategy to Combat Multi-Drug-Resistant Bacteria" Molecules 20, no. 4: 6466-6487. https://doi.org/10.3390/molecules20046466
APA StyleCole, M. R., Hobden, J. A., & Warner, I. M. (2015). Recycling Antibiotics into GUMBOS: A New Combination Strategy to Combat Multi-Drug-Resistant Bacteria. Molecules, 20(4), 6466-6487. https://doi.org/10.3390/molecules20046466