Additivity vs Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Resazurin Microplate Assay and Checkerboard Assay
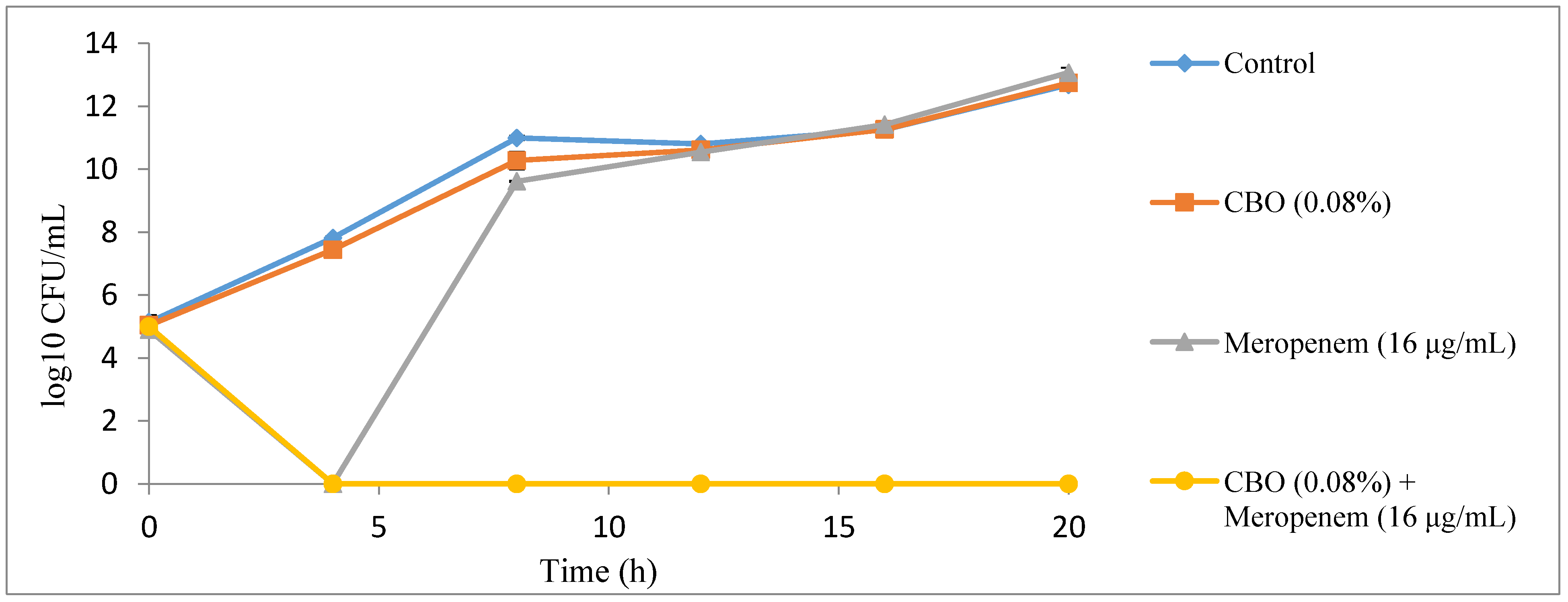
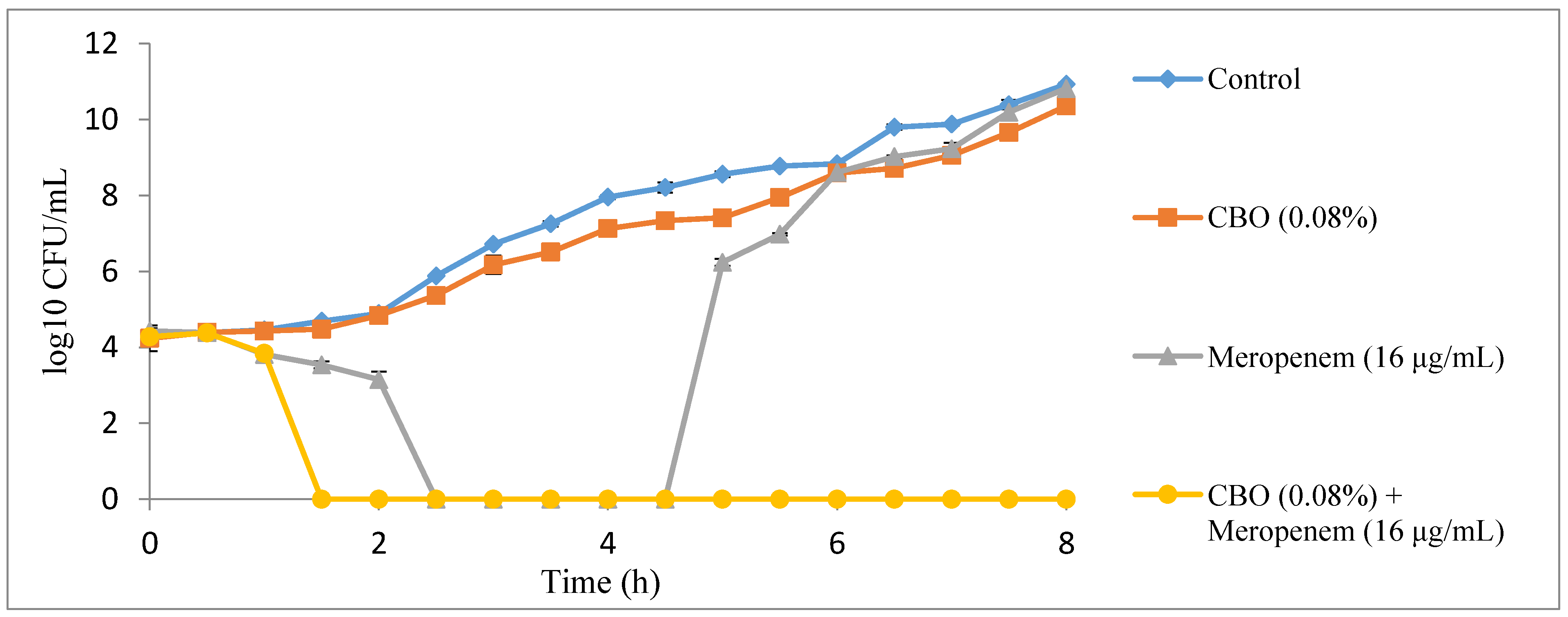
2.2. Time Kill Analysis
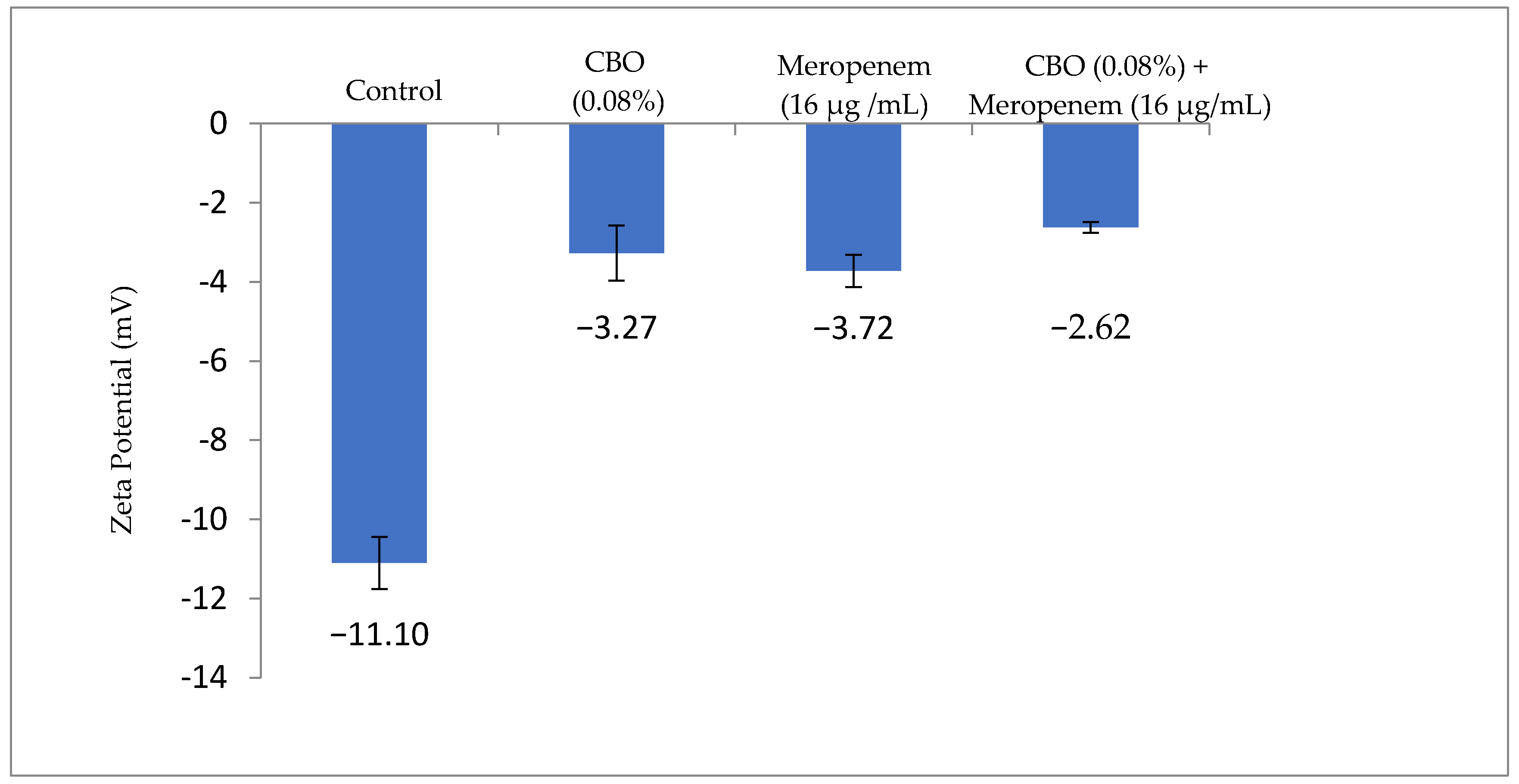
2.3. Zeta Potential Measurement
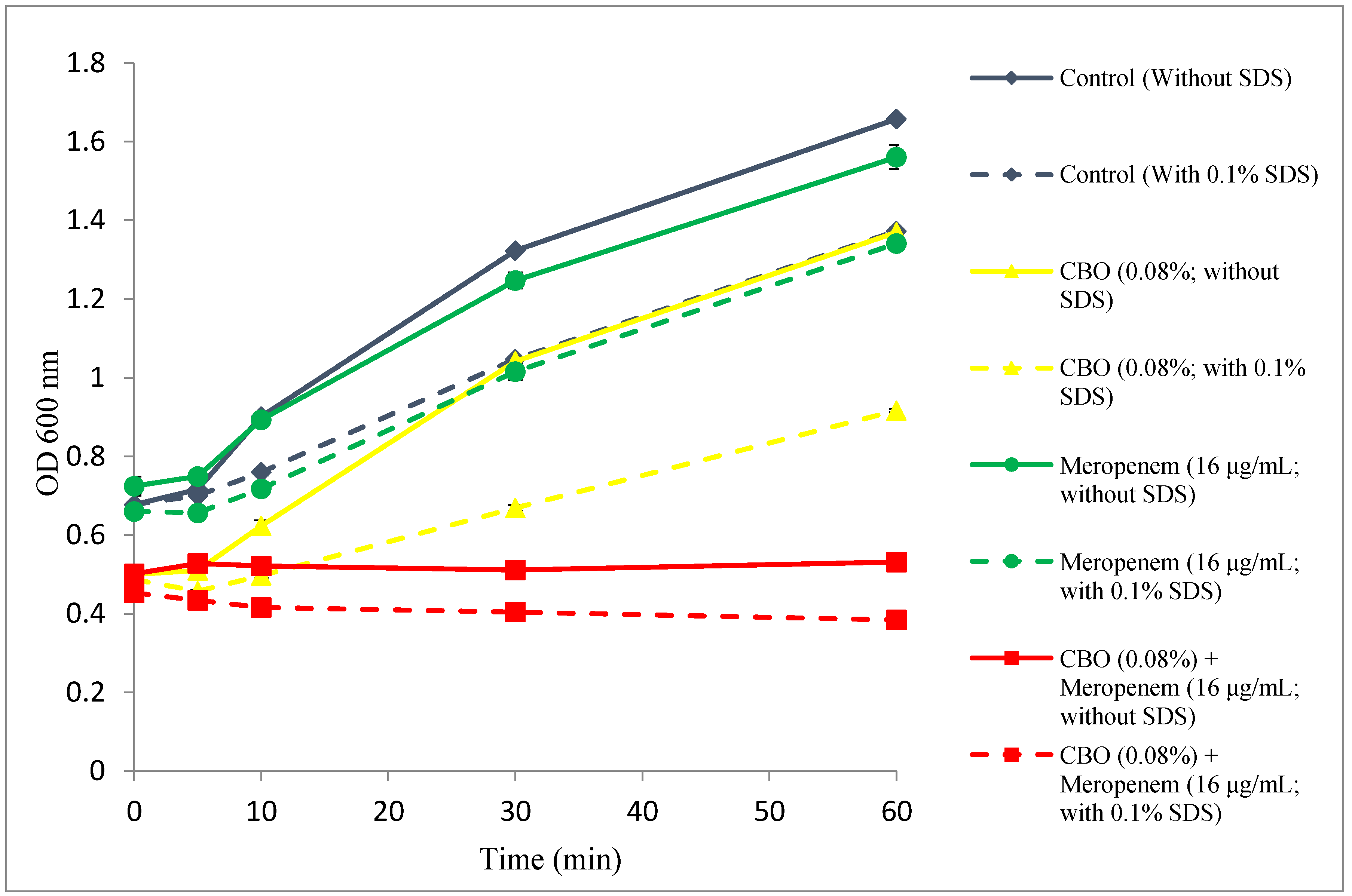
2.4. Outer Membrane Permeability Assay
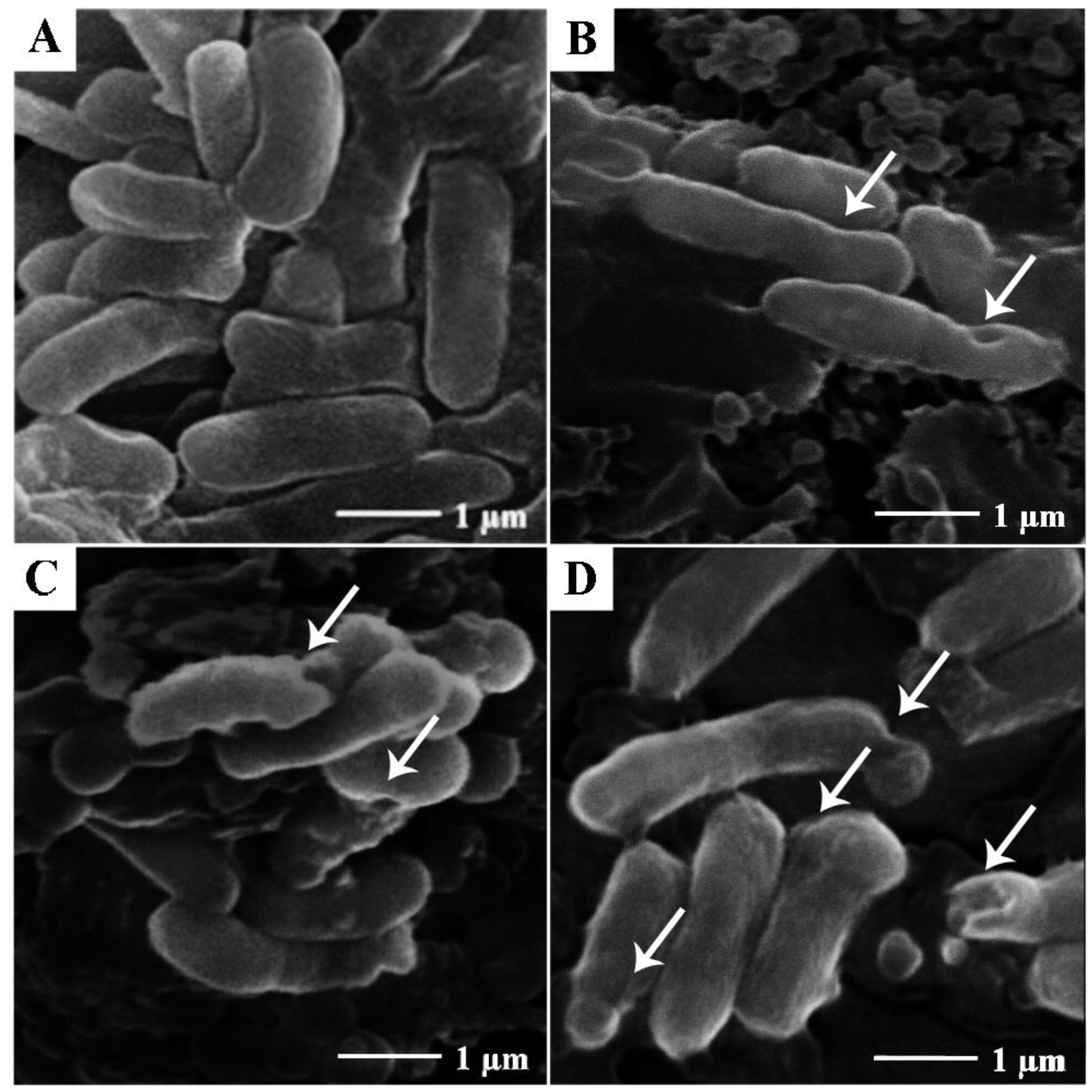
2.5. Scanning Electron Microscopy
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Essential Oils and Meropenem
5.2. Bacterial Strains and Growth Conditions
5.3. Resazurin Microplate Assay
5.4. Checkerboard Assay
5.5. Time Kill Analysis
5.6. Zeta Potential Measurement
5.7. Outer Membrane Permeability Assay
5.8. Scanning Electron Microscopy
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. Raw Data

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time (h) | K. pneumoniae BAA-1705 | |||
|---|---|---|---|---|
| Cell Number (CFU/mL) (Mean ± SD) | ||||
| Control | CBO (0.08%) | Meropenem (16 µg/mL) | CBO (0.08%) + Meropenem (16 µg/mL) | |
| 0 | 1.49 × 105 ± 7.28 × 104 | 1.10 × 105 ± 1.41 × 104 | 7.90 × 104 ± 1.27 × 104 | 1.00 × 105 ± 1.41 × 104 |
| 4 | 6.60 × 107 ± 8.49× 106 | 2.90 × 107± 1.27 × 107 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 8 | 9.95 × 1010 ± 1.48 × 1010 | 2.10 × 1010± 1.27 × 1010 | 4.15 × 109 ± 2.12 × 108 | 1.00 × 101 ± 0.00 × 100 |
| 12 | 6.35 × 1010± 7.78 × 109 | 4.25 × 1010 ± 1.48 × 1010 | 3.55 × 1010 ± 9.19 × 109 | 1.00 × 101 ± 0.00 × 100 |
| 16 | 1.85 × 1011± 4.95 × 1010 | 1.85 × 1011 ± 2.12 × 1010 | 2.65 × 1011 ± 4.95 × 1010 | 1.00 × 101 ± 0.00 × 100 |
| 20 | 4.80 × 1012 ± 2.83 × 1011 | 5.55 × 1012 ± 6.36 × 1011 | 1.21 × 1013 ± 4.10 × 1012 | 1.00 × 101 ± 0.00 × 100 |
| Time (h) | K. pneumoniae BAA-1705 | |||
|---|---|---|---|---|
| Cell Number (CFU/mL) (Mean ± SD) | ||||
| Control | CBO (0.08%) | Meropenem (16 µg/mL) | CBO (0.08%) + Meropenem (16 µg/mL) | |
| 0.0 | 2.25 × 104 ± 3.54 × 103 | 2.00 × 104 ± 1.41 × 104 | 2.70 × 104 ± 4.24 × 103 | 1.90 × 104 ± 1.41 × 103 |
| 0.5 | 2.50 × 104 ± 7.07 × 103 | 2.50 × 104 ± 4.24 × 103 | 2.45 × 104 ± 3.54 × 103 | 2.45 × 104 ± 7.78 × 103 |
| 1.0 | 2.90 × 104 ± 4.24 × 103 | 2.70 × 104 ± 4.24 × 103 | 6.50 × 103 ± 7.07 × 102 | 7.00 × 103 ± 1.41 × 103 |
| 1.5 | 4.90 × 104 ± 1.41 × 103 | 3.05 × 104 ± 6.36 × 103 | 3.50 × 103 ± 7.07 × 102 | 1.00 × 101 ± 0.00 × 100 |
| 2.0 | 7.75 × 104 ± 7.07 × 102 | 6.90 × 104 ± 1.41 × 103 | 1.50 × 103 ± 7.07 × 102 | 1.00 × 100 ± 0.00 × 100 |
| 2.5 | 7.60 × 105 ± 5.66 × 104 | 2.40 × 105 ± 8.49 × 104 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 3.0 | 5.20 × 106 ± 2.83 × 105 | 1.60 × 106 ± 8.49 × 105 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 3.5 | 1.80 × 107 ± 2.83 × 106 | 3.25 × 106 ± 6.36 × 105 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 4.0 | 9.05 × 107 ± 1.06 × 107 | 1.35 × 107 ± 2.12 × 106 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 4.5 | 1.65 × 108 ± 4.95 × 107 | 2.20 × 107 ± 5.66 × 106 | 1.00 × 101 ± 0.00 × 100 | 1.00 × 101 ± 0.00 × 100 |
| 5.0 | 3.65 × 108 ± 6.36 × 107 | 2.60 × 107 ± 5.66 × 106 | 1.75 × 106 ± 3.54 × 105 | 1.00 × 101 ± 0.00 × 100 |
| 5.5 | 5.90 × 108 ± 1.41 × 107 | 8.80 × 107 ± 5.66 × 106 | 9.50 × 106 ± 7.07 × 105 | 1.00 × 101 ± 0.00 × 100 |
| 6.0 | 6.80 × 108 ± 2.83 × 107 | 3.90 × 108 ± 1.41 × 107 | 4.20 × 108 ± 1.70 × 108 | 1.00 × 101 ± 0.00 × 100 |
| 6.5 | 6.30 × 109 ± 9.90 × 108 | 5.20 × 108 ± 1.13 × 108 | 1.05 × 109 ± 7.07 × 107 | 1.00 × 101 ± 0.00 × 100 |
| 7.0 | 7.55 × 109 ± 6.36 × 108 | 1.14 × 109 ± 2.26 × 108 | 1.75 × 109 ± 6.36 × 108 | 1.00 × 101 ± 0.00 × 100 |
| 7.5 | 2.50 × 1010 ± 7.07 × 109 | 4.55 × 109 ± 6.36 × 108 | 1.60 × 1010 ± 5.66 × 109 | 1.00 × 101 ± 0.00 × 100 |
| 8.0 | 8.45 × 1010 ± 7.78 × 109 | 2.35 × 1010 ± 9.19 × 109 | 6.55 × 1010 ± 6.36 × 109 | 1.00 × 101 ± 0.00 × 100 |
| K. pneumoniae BAA-1705 | Zeta Potential (mV) (Mean ± SD) | |||
| Control | Cinnamon Bark | Meropenem | Cinnamon Bark + Meropenem | |
| −11.10 ± 0.66 | −3.27 ± 0.70 | −3.72 ± 0.41 | −2.62 ± 0.14 | |
| Time | Treatment OD600nm ± SD (n = 3) | |||||||
|---|---|---|---|---|---|---|---|---|
| Control | CBO (0.08%) | Meropenem (16 µg/mL) | CBO (0.08%) + Meropenem (16 µg/mL) | |||||
| Without 0.1% SDS | With 0.1% SDS | Without 0.1% SDS | With 0.1% SDS | Without 0.1% SDS | With 0.1% SDS | Without 0.1% SDS | With 0.1% SDS | |
| 0 | 0.68 ± 0.027 | 0.68 ± 0.006 | 0.50 ± 0.016 | 0.49 ± 0.010 | 0.72 ± 0.025 | 0.66 ± 0.016 | 0.50 ± 0.017 | 0.45 ± 0.017 |
| 5 | 0.72 ± 0.047 | 0.70 ± 0.002 | 0.51 ± 0.007 | 0.46 ± 0.003 | 0.75 ± 0.005 | 0.66 ± 0.011 | 0.53 ± 0.008 | 0.43 ± 0.004 |
| 10 | 0.90 ± 0.007 | 0.76 ± 0.008 | 0.62 ± 0.015 | 0.50 ± 0.006 | 0.89 ± 0.013 | 0.72 ± 0.006 | 0.52 ± 0.007 | 0.42 ± 0.021 |
| 30 | 1.32 ± 0.005 | 1.05 ± 0.007 | 1.04 ± 0.004 | 0.67 ± 0.008 | 1.25 ± 0.021 | 1.02 ± 0.021 | 0.51 ± 0.015 | 0.40 ± 0.014 |
| 60 | 1.66 ± 0.007 | 1.37 ± 0.009 | 1.37 ± 0.004 | 0.92 ± 0.004 | 1.56 ± 0.031 | 1.34 ± 0.011 | 0.53 ± 0.015 | 0.38 ± 0.009 |
References
- Amábile-Cuevas, C.F. Antimicrobial Resistance in Bacteria; Horizon Bioscience: Wymondham, England, 2007. [Google Scholar]
- Yap, P.S.X.; Yang, S.K.; Lai, K.S.; Lim, S.H.E. Essential oils: The ultimate solution to antimicrobial resistance in Escherichia coli? In Escherichia coli-Recent Advances on Physiology, Pathogenesis and Biotechnological Applications; Samie, A., Ed.; Intech Open: Rijeka, Croatia, 2017. [Google Scholar]
- Worthington, R.J.; Melander, C. Combination approaches to combat multi-drug resistant bacteria. Trends Biotechnol. 2013, 31, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Cosgrove, S.E.; Maragakis, L.L. Combination therapy for treatment of infections with gram-negative bacteria. Clin. Microbiol. Rev. 2012, 25, 450–470. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.S.; Yiap, B.C.; Ping, H.C.; Lim, S.H. Essential oils, a new horizon in combating bacterial antibiotic resistance. Open Microbiol. J. 2014, 8, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Borisy, A.A.; Elliott, P.J.; Hurst, N.W.; Lee, M.S.; Lehar, J.; Price, E.R.; Serbedzija, G.; Zimmermann, G.R.; Foley, M.A.; Stockwell, B.R.; et al. Systematic discovery of multicomponent therapeutics. Proc. Natl. Acad. Sci. USA 2003, 100, 7977–7982. [Google Scholar] [CrossRef] [PubMed]
- Lorian, V. Antibiotics in Laboratory Medicine, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; p. 889. [Google Scholar]
- Meletiadis, J.; Pournaras, S.; Roilides, E.; Walsh, T.J. Defining fractional inhibitory concentration index cutoffs for additive interactions based on self-drug additive combinations, Monte Carlo simulation analysis, and in vitro-in vivo correlation data for antifungal drug combinations against Aspergillus fumigatus. Antimicrob. Agents Chemother. 2010, 54, 602–609. [Google Scholar] [PubMed]
- Si, H.; Hu, J.; Liu, Z.; Zeng, Z.L. Antibacterial effect of oregano essential oil alone and in combination with antibiotics against extended-spectrum beta-lactamase-producing Escherichia coli. F.E.M.S. Immunol. Med. Microbiol. 2008, 53, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Van Vuuren, S.F.; Suliman, S.; Viljoen, A.M. The antimicrobial activity of four commercial essential oils in combination with conventional antimicrobials. Lett. Appl. Microbiol. 2009, 48, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Karpanen, T.J.; Worthington, T.; Hendry, E.R.; Conway, B.R.; Lambert, P.A. Antimicrobial efficacy of chlorhexidine digluconate alone and in combination with eucalyptus oil, tea tree oil and thymol against planktonic and biofilm cultures of Staphylococcus epidermidis. J. Antimicrob. Chemother. 2008, 62, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Chovanova, R.; Mikulasova, M.; Vaverkova, S. In vitro antibacterial and antibiotic resistance modifying effect of bioactive plant extracts on methicillin-resistant Staphylococcus epidermidis. Int. J. Microbiol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.S.; Lim, S.H.; Hu, C.P.; Yiap, B.C. Combination of essential oils and antibiotics reduce antibiotic resistance in plasmid-conferred multidrug resistant bacteria. Phytomedicine 2013, 20, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Doern, C.D. When does 2 plus 2 equal 5? A review of antimicrobial synergy testing. J. Clin. Microbiol. 2014, 52, 4124–4128. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.S.; Krishnan, T.; Chan, K.G.; Lim, S.H. Antibacterial mode of action of Cinnamomum verum bark essential oil, alone and in combination with piperacillin, against a multi-drug-resistant Escherichia coli strain. J. Microbiol. Biotechnol. 2015, 25, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.S.; Krishnan, T.; Yiap, B.C.; Hu, C.P.; Chan, K.G.; Lim, S.H. Membrane disruption and anti-quorum sensing effects of synergistic interaction between Lavandula angustifolia (lavender oil) in combination with antibiotic against plasmid-conferred multi-drug-resistant Escherichia coli. J. Appl. Microbiol. 2014, 116, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Odds, F.C. Synergy, antagonism, and what the chequerboard puts between them. J. Antimicrob. Chemother. 2003, 52, 1. [Google Scholar] [CrossRef] [PubMed]
- Papp-Wallace, K.M.; Endimiani, A.; Taracila, M.A.; Bonomo, R.A. Carbapenems: Past, present, and future. Antimicrob. Agents Chemother. 2011, 55, 4943–4960. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.S.; Yusoff, K.; Maziah, M. Extracellular matrix as the early structural marker for Centella asiatica embryogenic tissues. Biol. Plant 2011, 55, 549–553. [Google Scholar] [CrossRef]
- Verma, P. Methods for Determining Bactericidal Activity and Antimicrobial Interactions; CRC Press: Boca Raton, FL, USA, 2007; pp. 275–298. [Google Scholar]
- Sands, M.; McCarter, Y.; Sanchez, W. Synergy testing of multidrug resistant Acinetobacter baumanii against tigecycline and polymyxin using an E-test methodology. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 521–522. [Google Scholar] [CrossRef] [PubMed]
- Wai, S.N.; Mizunoe, Y.; Takade, A.; Yoshida, S. A comparison of solid and liquid media for resuscitation of starvation- and low-temperature-induced nonculturable cells of Aeromonas hydrophila. Arch. Microbiol. 2000, 173, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, X.; Wang, Y.; Jiang, P.; Quek, S. Antibacterial activity and mechanism of cinnamon essential oil against Escherichia coli and Staphylococcus aureus. Food Control 2016, 59, 282–289. [Google Scholar] [CrossRef]
- Sopirala, M.M.; Mangino, J.E.; Gebreyes, W.A.; Biller, B.; Bannerman, T.; Balada-Llasat, J.M.; Pancholi, P. Synergy testing by Etest, microdilution checkerboard, and time-kill methods for pan-drug-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2010, 54, 4678–4683. [Google Scholar] [CrossRef] [PubMed]
- Van der Mei, H.C.; de Vries, J.; Busscher, H.J. Hydrophobic and electrostatic cell surface properties of thermophilic dairy streptococci. Appl. Environ. Microbiol. 1993, 59, 4305–4312. [Google Scholar] [PubMed]
- Nazari, M.; Kurdi, M.; Heerklotz, H. Classifying surfactants with respect to their effect on lipid membrane order. Biophys. J. 2012, 102, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Vaara, M. Agents that increase the permeability of the outer membrane. Microbiol. Rev. 1992, 56, 395–411. [Google Scholar] [PubMed]
- Scandorieiro, S.; de Camargo, L.C.; Lancheros, C.A.; Yamada-Ogatta, S.F.; Nakamura, C.V.; de Oliveira, A.G.; Andrade, C.G.; Duran, N.; Nakazato, G.; Kobayashi, R.K. Synergistic and additive effect of oregano essential oil and biological silver nanoparticles against multidrug-resistant bacterial strains. Front. Microbiol. 2016, 7, 760. [Google Scholar] [CrossRef] [PubMed]
- Ali, B.; Al-Wabel, N.A.; Shams, S.; Ahamad, A.; Khan, S.A.; Anwar, F. Essential oils used in aromatherapy: A systemic review. Asian Pac. J. Trop. Biomed. 2015, 5, 601–611. [Google Scholar] [CrossRef]
- Halder, S.; Yadav, K.K.; Sarkar, R.; Mukherjee, S.; Saha, P.; Haldar, S.; Karmakar, S.; Sen, T. Alteration of Zeta potential and membrane permeability in bacteria: A study with cationic agents. SpringerPlus 2015, 4, 672. [Google Scholar] [CrossRef] [PubMed]
- Hemaiswarya, S.; Kruthiventi, A.K.; Doble, M. Synergism between natural products and antibiotics against infectious diseases. Phytomedicine 2008, 15, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Marri, L.; Dallai, R.; Marchini, D. The novel antibacterial peptide ceratotoxin A alters permeability of the inner and outer membrane of Escherichia coli K-12. Curr. Microbiol. 1996, 33, 40–43. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds cinnamon bark (Cinnamomum verum), marjoram (Origanum majorana), peppermint (Mentha x piperita) and tea tree (Melaleuca alternifolia) are available from the authors. |





| Combinations of Essential Oils and Meropenem | K. pneumoniae BAA-1705 | Type of Interaction | |||
|---|---|---|---|---|---|
| MICO | MICC | FICI | FICIc | ||
| Cinnamon Bark-Meropenem Cinnamon Bark (%) | 0.16 | 0.08 | 0.50 | 1.00 | Additive |
| Meropenem (μg/mL) | 32 | 16 | 0.50 | ||
| Marjoram-Meropenem Marjoram (%) | 1.25 | 0.63 | 0.50 | 0.56 | Additive |
| Meropenem (μg/mL) | 32 | 2 | 0.06 | ||
| Peppermint-Meropenem Peppermint (%) | 1.25 | 0.63 | 0.50 | 0.56 | Additive |
| Meropenem (μg/mL) | 32 | 2 | 0.06 | ||
| Tea Tree-Meropenem Tea Tree (%) | 1.25 | 0.63 | 0.50 | 0.52 | Additive |
| Meropenem (μg/mL) | 32 | 0.5 | 0.02 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.-K.; Yusoff, K.; Mai, C.-W.; Lim, W.-M.; Yap, W.-S.; Lim, S.-H.E.; Lai, K.-S. Additivity vs Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy. Molecules 2017, 22, 1733. https://doi.org/10.3390/molecules22111733
Yang S-K, Yusoff K, Mai C-W, Lim W-M, Yap W-S, Lim S-HE, Lai K-S. Additivity vs Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy. Molecules. 2017; 22(11):1733. https://doi.org/10.3390/molecules22111733
Chicago/Turabian StyleYang, Shun-Kai, Khatijah Yusoff, Chun-Wai Mai, Wei-Meng Lim, Wai-Sum Yap, Swee-Hua Erin Lim, and Kok-Song Lai. 2017. "Additivity vs Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy" Molecules 22, no. 11: 1733. https://doi.org/10.3390/molecules22111733
APA StyleYang, S. -K., Yusoff, K., Mai, C. -W., Lim, W. -M., Yap, W. -S., Lim, S. -H. E., & Lai, K. -S. (2017). Additivity vs Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy. Molecules, 22(11), 1733. https://doi.org/10.3390/molecules22111733