
Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes

 ,
, 

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Results
2.1. Blood Pressure
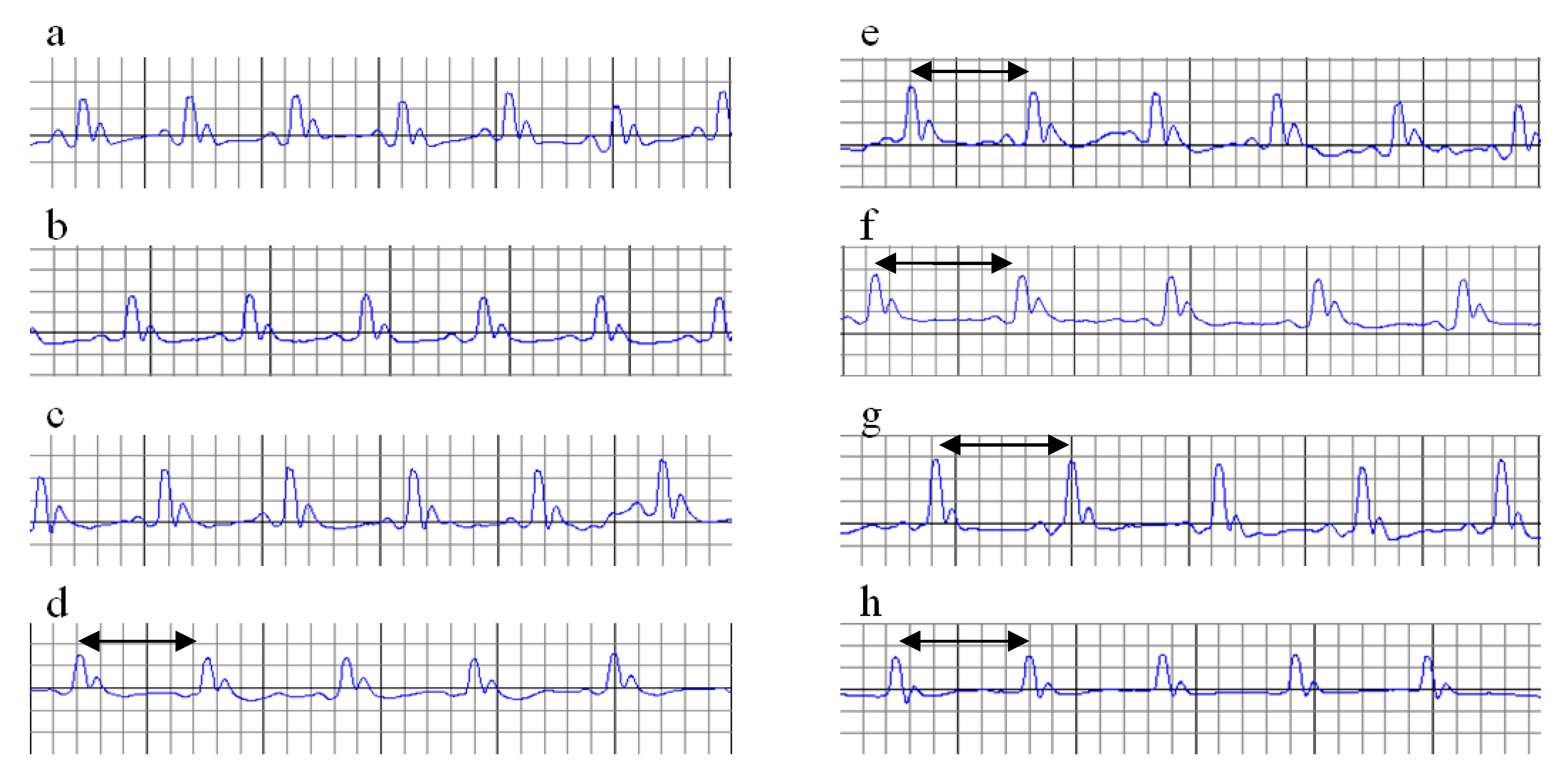
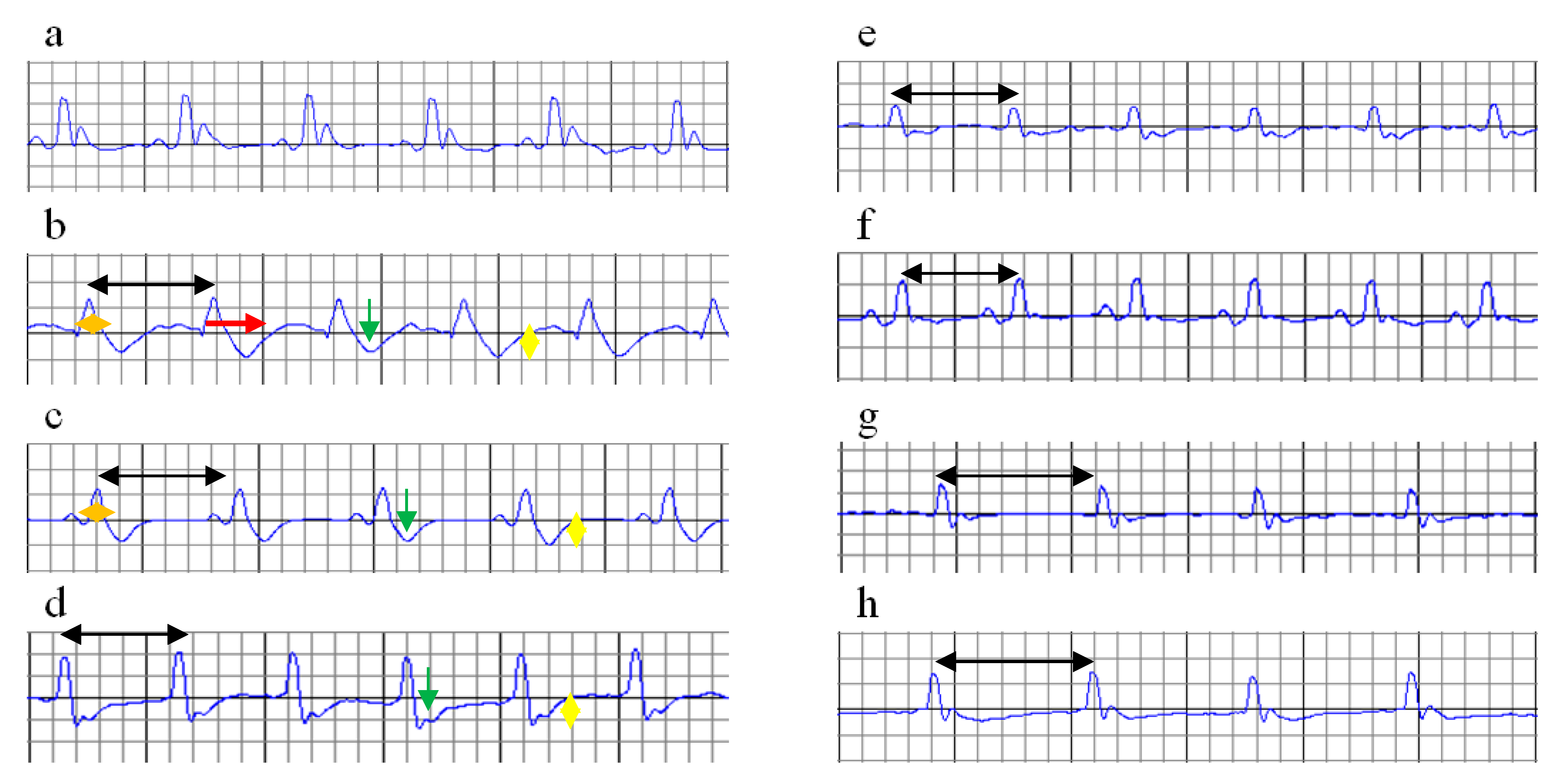
2.2. Electrocardiogram Monitoring
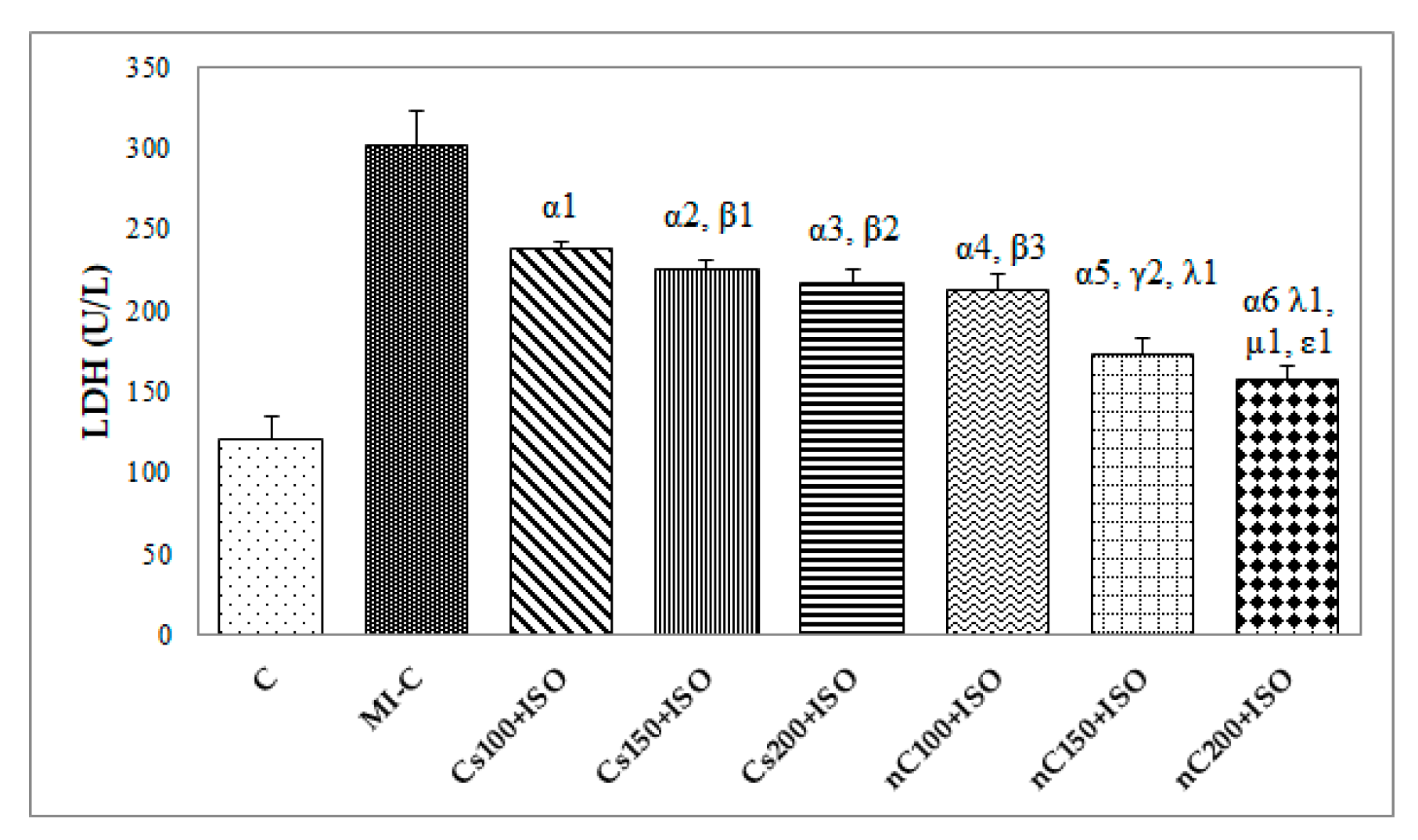
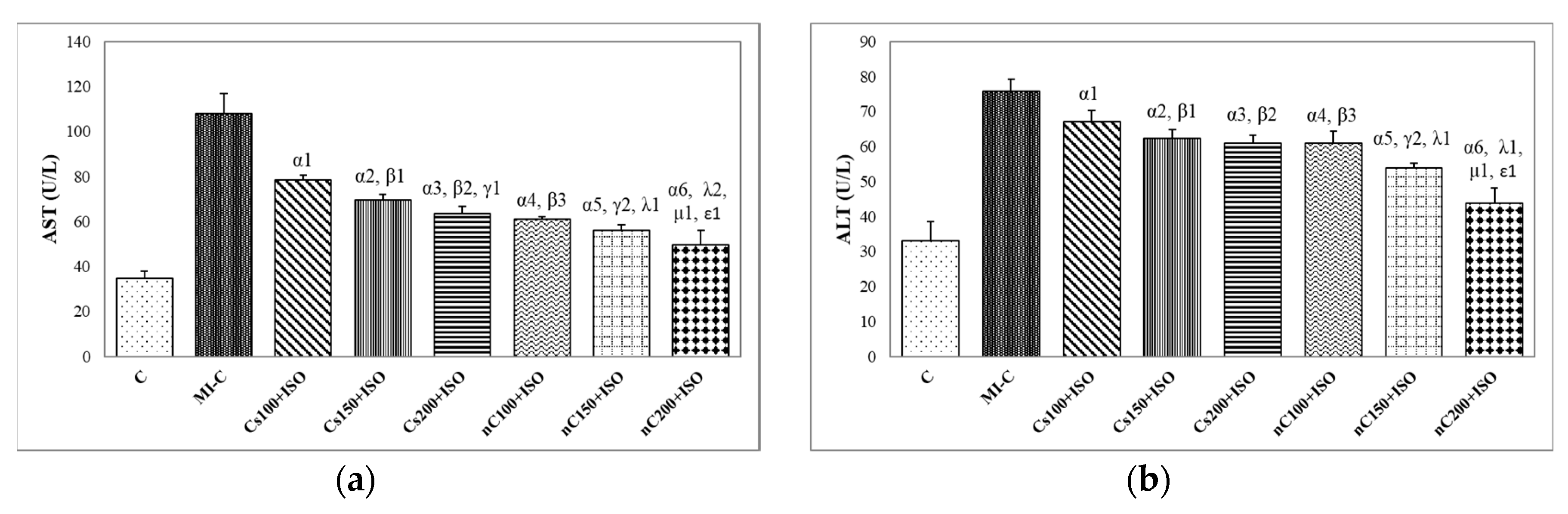
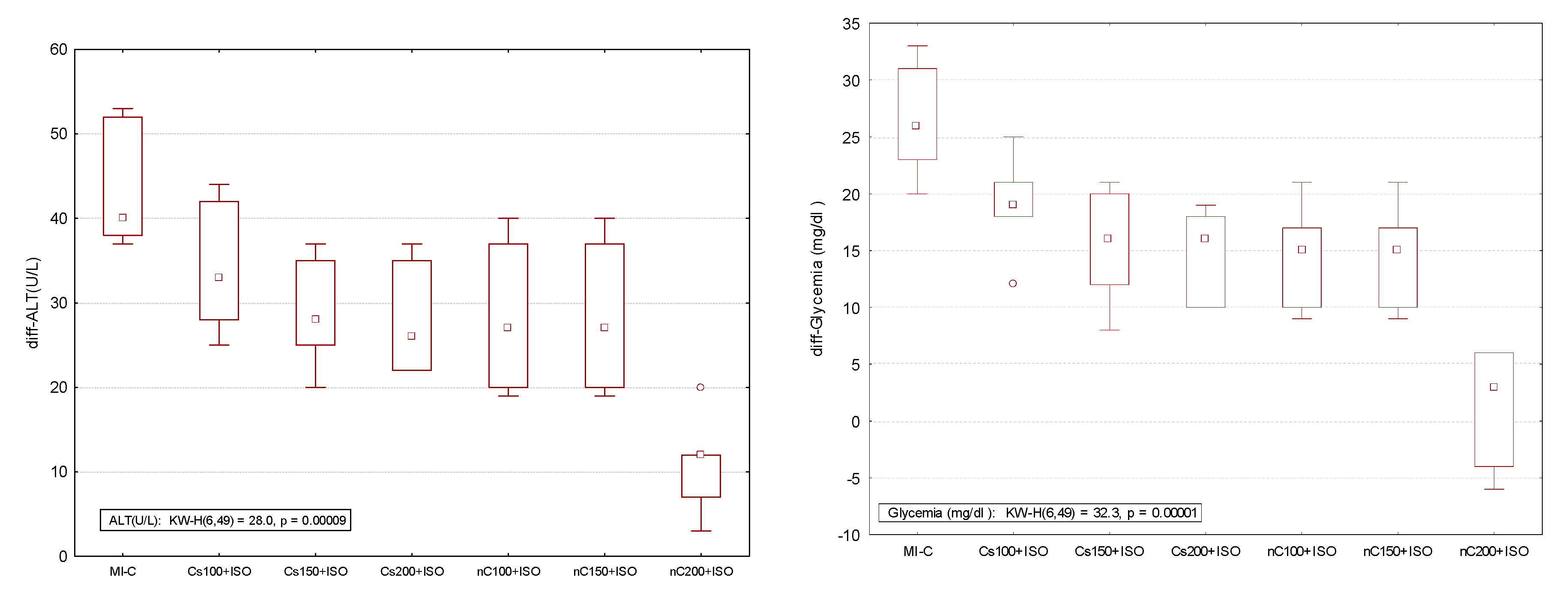
2.3. Blood Samples and Serum Analysis
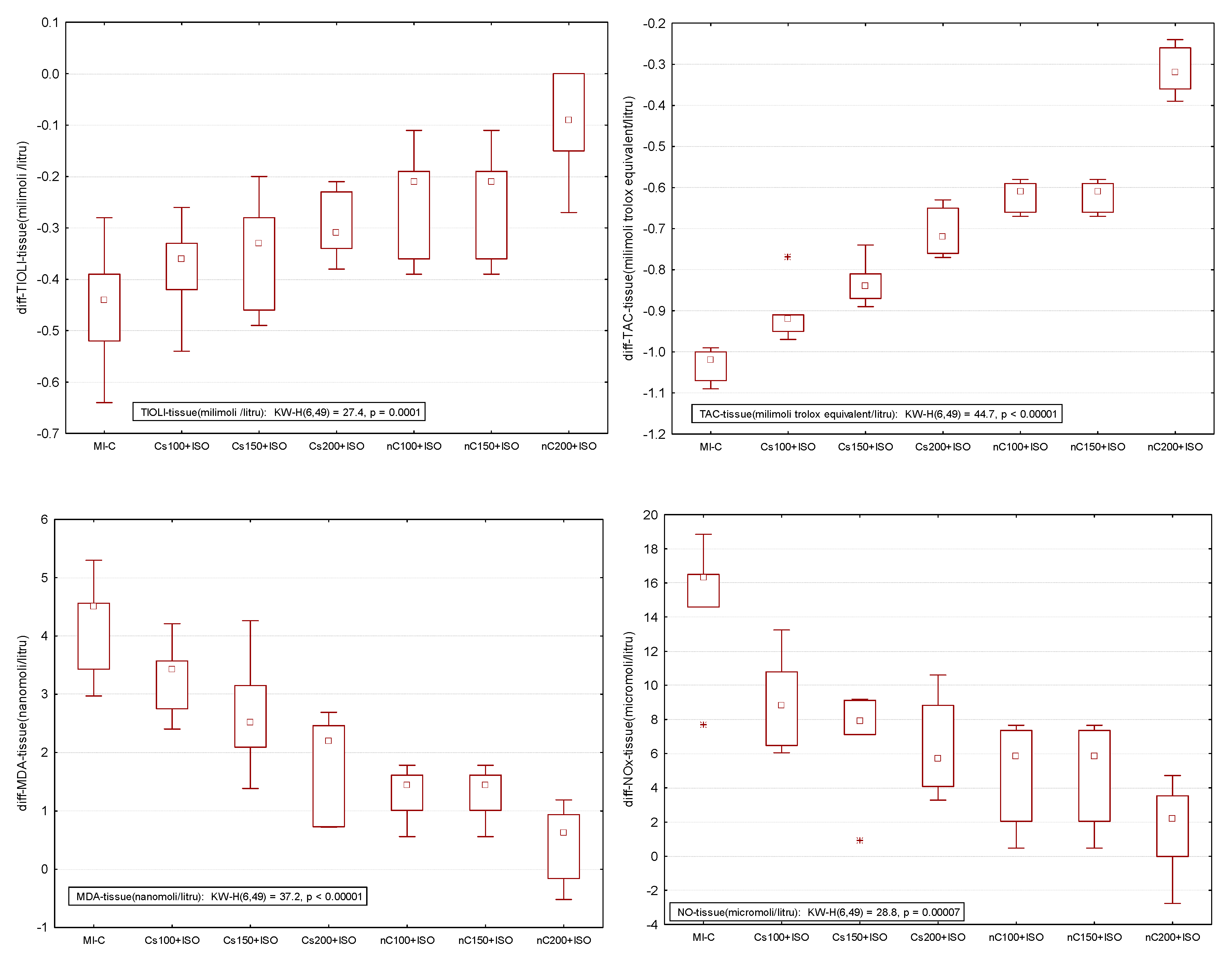
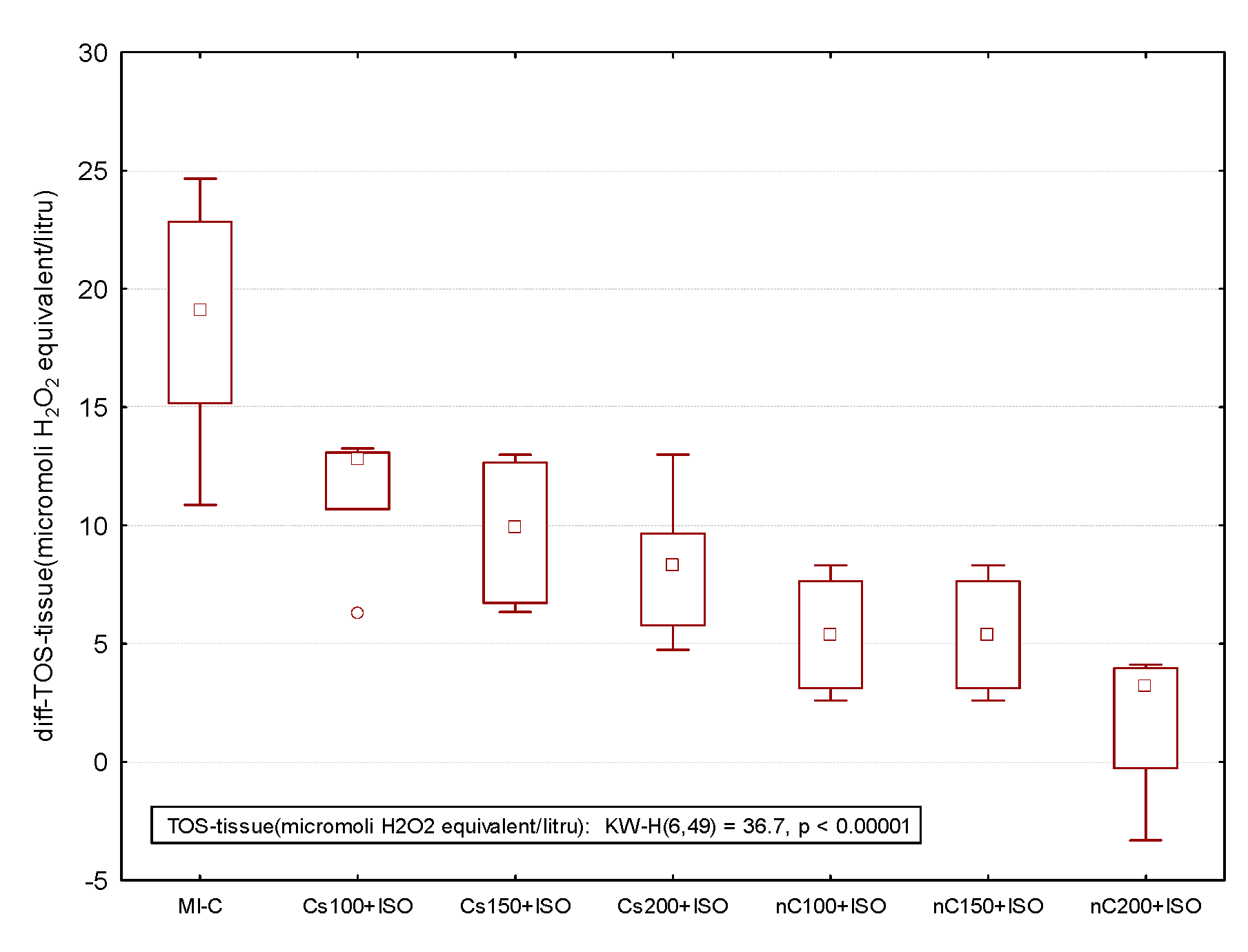
2.4. Assessment of Oxidative Stress Parameters in Myocardial Tissue
2.5. Overall Effect of Curcumin Nanoparticle Solution
3. Discussion
Study Limitations and Call for Future Researches
4. Materials and Methods
4.1. Ethics Statement
4.2. Chemicals and Reagents
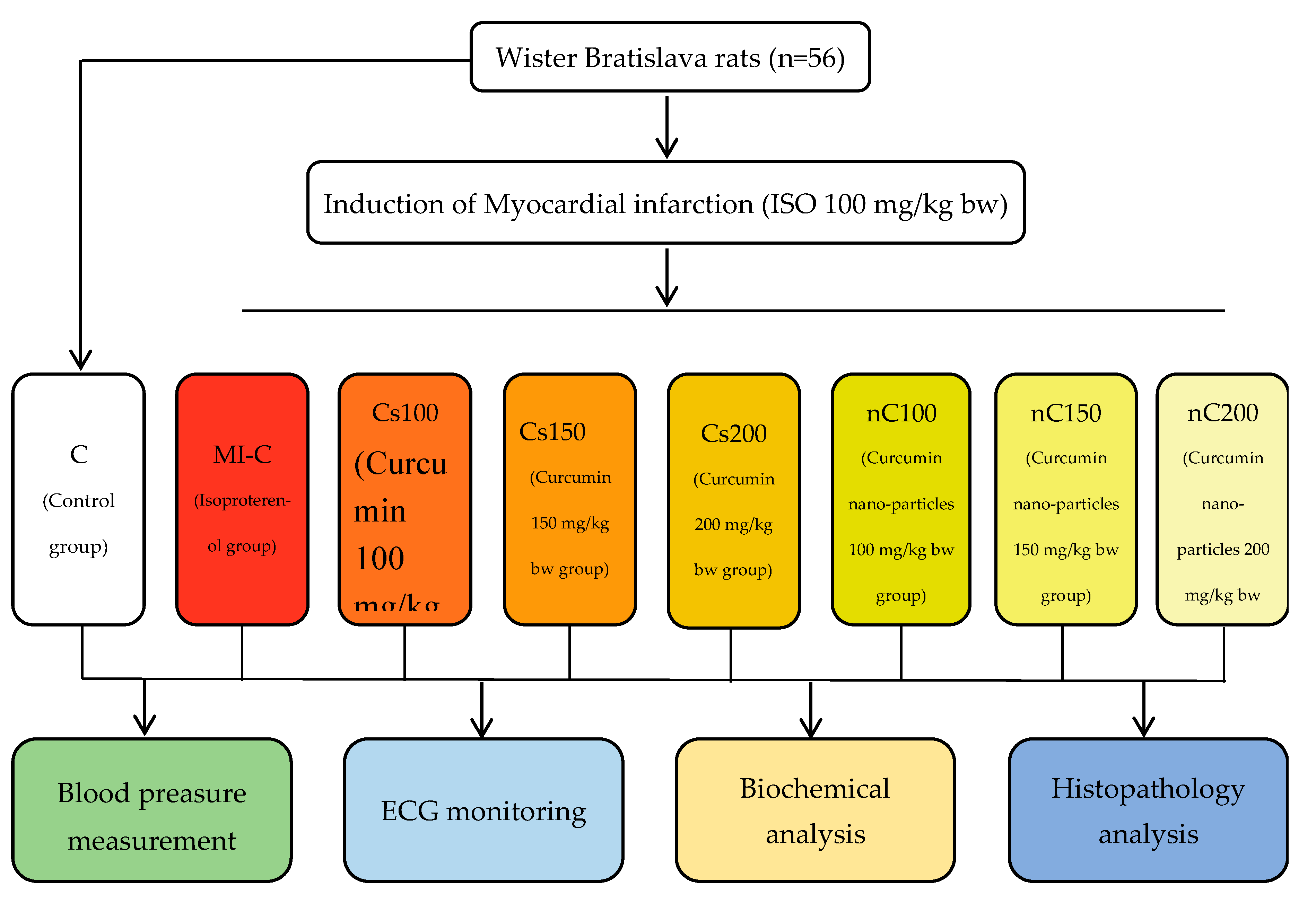
4.3. Animal Grouping
4.4. Myocardial Ischemia Induction
4.5. Blood Pressure Measurement
4.6. Electrocardiography Monitoring
4.7. Blood Samples and Serum Analysis
4.8. Preparation of Tissue Homogenate and Myocardial Oxidative Stress Evaluation
4.9. Statistical Analysis
5. Conclusionss
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Steffens, S.; Montecucco, F.; Mach, F. The inflammatory response as a target to reduce myocardial ischaemia and reperfusion injury. Thromb. Haemost. 2009, 102, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.H.; Arnaout, S.; Karrowni, W.; Dakik, H.A. The management of acute myocardial infarction in developing countries. Int. J. Cardiol. 2006, 111, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Li, H.; Wan, S.P.; Zeng, Q.T.; Cheng, L.X.; Jiang, L.L.; Peng, Y.D. Cardioprotective effects of malvidin against isoproterenol-induced myocardial infarction in rats, A mechanistic study. Med. Sci. Monit. 2017, 23, 2007–2016. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2018, 72, 2231–2264. [Google Scholar]
- Prince, P.S.; Dhanasekar, K.; Rajakumar, S. Vanillic acid prevents altered ion pumps; ions; inhibits Fas-receptor and caspase mediated apoptosis-signaling pathway and cardiomyocyte death in myocardial infarcted rats. Chem. Biol. Interact. 2015, 232, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Sharma, C.; Mahajan, U.; Patil, C.; Agrawal, Y.; Kumari, S.; Arya, D.; Ojha, S. Protective effects of cardamom in isoproterenol-induced myocardial infarction in rats. Int. J. Mol. Sci. 2015, 16, 27457–27469. [Google Scholar] [CrossRef]
- Upaganlawar, A.; Gandhi, H.; Balaraman, R. Isoproterenol induced myocardial infarction, Protective role of natural products. J. Pharmacol. Toxicol. 2011, 6, 1–7. [Google Scholar]
- Huang, H.; Geng, Q.; Yao, H.; Shen, Z.; Wu, Z.; Miao, X.; Shi, P. Protective effect of scutellarin on myocardial infarction induced by isoprenaline in rats. Iran. J. Basic Med. Sci. 2018, 21, 267–276. [Google Scholar]
- Panda, S.; Kar, A.; Biswas, S. Preventive effect of agnucastoside C against isoproterenol-induced myocardial injury. Sci. Rep. 2017, 7, 16146. [Google Scholar] [CrossRef]
- Hosseinzadeh, L.; Behravan, J.; Mosaffa, F.; Bahrami, G.; Bahrami, A.R.; Karimi, G. Effect of curcumin on doxorubicin-induced cytotoxicity in H9c2 cardiomyoblast cells. Iran. J. Basic Med. Sci. 2011, 14, 49–56. [Google Scholar]
- Kocaadam, B.; Şanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yue, Y.; Zheng, X.; Zhang, K.; Chen, S.; Du, Z. Curcumin, inflammation, and chronic diseases, how are they linked? Molecules 2015, 20, 9183–9213. [Google Scholar] [CrossRef]
- Hatcher, H.; Planalp, R.; Cho, J.; Torti, F.; Torti, S. Curcumin, from ancient medicine to current clinical trials. Cell. Mol. Life Sci. 2008, 65, 1631–1652. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin, problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Abdollahzadeh Estakhri, M.; Shokrzadeh, M.; Jaafari, M.R.; Mohammadi, H. Organ toxicity attenuation by nanomicelles containing curcuminoids, Comparing the protective effects on tissues oxidative damage induced by diazinon. Iran. J. Basic Med. Sci. 2019, 22, 17–24. [Google Scholar] [PubMed]
- Gera, M.; Sharma, N.; Ghosh, M.; Huynh, D.L.; Lee, S.J.; Min, T.; Kwon, T.; Jeong, D.K. Nanoformulations of curcumin, an emerging paradigm for improved remedial application. Oncotarget 2017, 8, 66680. [Google Scholar] [CrossRef] [PubMed]
- Silva-Buzanello, R.A.; Souza, M.F.; Oliveira, D.A.; Bona, E.; Leimann, F.V.; Cardozo Filho, L.; de Araújo, P.H.H.; Ferreira, S.R.S.; Gonçalves, O.H. Preparation of curcumin-loaded nanoparticles and determination of the antioxidant potential of curcumin after encapsulation. Polímeros 2016, 26, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Dai, W.T.; He, Z.M.; Gao, L.; Huang, X.; Gong, J.M.; Xing, H.Y.; Chen, W.D. Fabrication and evaluation of curcumin-loaded nanoparticles based on solid lipid as a new type of colloidal drug delivery system. Indian J. Pharm. Sci. 2013, 75, 178–184. [Google Scholar]
- Ghalandarlaki, N.; Alizadeh, A.M.; Ashkani-Esfahani, S. Nanotechnology-applied curcumin for different diseases therapy. Biomed. Res. Int. 2014, 2014, 394264. [Google Scholar] [CrossRef]
- Boarescu, P.M.; Chirilă, I.; Bulboacă, A.E.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bolboacă, S.D. Effects of curcumin nanoparticles in isoproterenol-induced myocardial infarction. Oxid. Med. Cell. Longev. 2019, 2019, 7847142. [Google Scholar] [CrossRef]
- Grimm, D.; Elsner, D.; Schunkert, H.; Pfeifer, M.; Griese, D.; Bruckschlegel, G.; Muders, F.; Riegger, G.A.J.; Kromer, E.P. Development of heart failure following isoproterenol administration in the rat, role of the renin-angiotensin system. Cardiovasc. Res. 1998, 37, 91–100. [Google Scholar] [CrossRef]
- Kilinç, E.; Kaygisiz, Z.; Benek, B.S.; Gümüştekin, K. Effects and mechanisms of curcumin on the hemodynamic variablesof isolated perfused rat hearts. Turk. J. Med. Sci. 2016, 46, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Balea, Ş.S.; Pârvu, A.E.; Pop, N.; Marín, F.Z.; Pârvu, M. Polyphenolic Compounds; Antioxidant; and Cardioprotective Effects of Pomace Extracts from Fetească Neagră Cultivar. Oxid. Med. Cell. Longev. 2018, 2018, 8194721. [Google Scholar] [CrossRef] [PubMed]
- Králová, E.; Mokran, T.; Murin, J.; Stankovicova, T. Electrocardiography in two models of isoproterenol-induced left ventricular remodeling. Physiol. Res. 2008, 57, S83–S89. [Google Scholar] [PubMed]
- Collins, P.; Billings, C.G. Isoprenaline-induced changes in regional myocardial perfusion in the pathogenesis of myocardial necrosis. Br. J. Exp. Pathol. 1976, 5, 637–644. [Google Scholar]
- Shipsey, S.J.; Bryant, S.M.; Hart, G. Effects of hypertrophy on regional action potential characteristics in the rat left ventricle, a cellular basis for T-wave inversion? Circulation 1997, 96, 2061–2068. [Google Scholar] [CrossRef] [PubMed]
- Nirmala, C.; Puvanakrishnan, R. Protective role of curcumin against isoproterenol induced myocardial infarction in rats. Mol. Cell. Biochem. 1996, 159, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Helson, L.; Shopp, G.; Bouchard, A.; Majeed, M. Liposome mitigation of curcumin inhibition of cardiac potassium delayed-rectifier current. J. Recept. Ligand Channel Res. 2012, 11, 1–8. [Google Scholar] [CrossRef]
- Hu, C.W.; Sheng, Y.; Zhang, Q.; Liu, H.B.; Xie, X.; Ma, W.C.; Huo, R.; Dong, D.-L. Curcumin inhibits hERG potassium channels in vitro. Toxicol Lett 2012, 11, 192–196. [Google Scholar] [CrossRef]
- Ranjan, A.P.; Mukerjee, A.; Helson, L.; Vishwanatha, J.K. Mitigating prolonged QT interval in cancer nanodrug development for accelerated clinical translation. J. Nanobiotechnol. 2013, 11, 40. [Google Scholar] [CrossRef]
- Sedláková, E.; Rácz, O.; Lovásová, E.; Beòaèka, R.; Kurpas, M.; Chmelárová, A.; Sedlák, J.; Studenèan, M. Markers of oxidative stress in acute myocardial infarction treated by percutaneous coronary intervention. Open Med. 2009, 4, 26–31. [Google Scholar] [CrossRef]
- Bulboacă, A.E.; Bolboacă, S.D.; Stănescu, I.C.; Sfrângeu, C.A.; Bulboacă, A.C. Preemptive analgesic and antioxidative effect of curcumin for experimental migraine. Biomed. Res. Int. 2017, 2017, 4754701. [Google Scholar] [CrossRef] [PubMed]
- Rahnavard, M.; Hassanpour, M.; Ahmadi, M.; Heidarzadeh, M.; Amini, H.; Javanmard, M.Z.; Nouri, M.; Rahbarghazi, R.; Safaie, N. Curcumin ameliorated myocardial infarction by inhibition of cardiotoxicity in the rat model. J. Cell. Biochem. 2019, 120, 11965–11972. [Google Scholar] [CrossRef] [PubMed]
- Nabofa, W.E.; Alashe, O.O.; Oyeyemi, O.T.; Attah, A.F.; Oyagbemi, A.A.; Omobowale, T.O.; Adedapo, A.A.; Alada, A.R.A. Cardioprotective Effects of Curcumin-Nisin Based Poly Lactic Acid Nanoparticle on Myocardial Infarction in Guinea Pigs. Sci. Rep. 2018, 8, 16649. [Google Scholar] [CrossRef]
- Cebova, M.; Rehakova, R.; Kosutova, M.; Pechanova, O. Simvastatin Does Not Affect Nitric Oxide Generation Increased by Sesame Oil in Obese Zucker Rats. Oxid. Med. Cell. Longev. 2018, 2018, 5413423. [Google Scholar] [CrossRef]
- Kurian, G.A.; Rajagopal, R.; Vedantham, S.; Rajesh, M. The role of oxidative stress in myocardial ischemia and reperfusion injury and remodeling, revisited. Oxid. Med. Cell. Longev. 2016, 2016, 1656450. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Park, H.J.; Joo, S.Y.; Hong, M.H.; Kim, K.H.; Hong, Y.J.; Park, H.W.; Jeong, M.H.; Cho, J.G.; Park, G.C.; et al. The protective effect of curcumin on myocardial ischemia-reperfusion injury. Korean Circ. J. 2008, 38, 353–359. [Google Scholar]
- Yu, H.; Li, J.; Shi, K.; Huang, Q. Structure of modified ε-polylysine micelles and their application in improving cellular antioxidant activity of curcuminoids. Food Funct. 2011, 2, 373–380. [Google Scholar] [CrossRef]
- Mohajeri, M.; Sadeghizadeh, M.; Najafi, F.; Javan, M. Polymerized nano-curcumin attenuates neurological symptoms in EAE model of multiple sclerosis through down regulation of inflammatory and oxidative processes and enhancing neuroprotection and myelin repair. Neuropharmacology 2015, 99, 156–167. [Google Scholar] [CrossRef]
- Ellidag, H.Y.; Eren, E.; Yılmaz, N.; Cekin, Y. Oxidative stress and ischemia-modified albumin in chronic ischemic heart failure. Redox Rep. 2014, 19, 118–123. [Google Scholar] [CrossRef]
- Bas, H.A.; Aksoy, F.; Icli, A.; Varol, E.; Dogan, A.; Erdogan, D.; Ersoy, I.; Arslan, A.; Ari, H.; Bas, N.; et al. The association of plasma oxidative status and inflammation with the development of atrial fibrillation in patients presenting with ST elevation myocardial infarction. Scand. J. Clin. Lab. Investig. 2017, 77, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Eser, A.; Hizli, D.; Haltas, H.; Namuslu, M.; Kosus, A.; Kosus, N.; Kafali, H. Effects of curcumin on ovarian ischemia-reperfusion injury in a rat model. Biomed. Rep. 2015, 3, 807–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adeoye, B.O.; Ajibade, T.O.; Oyagbemi, A.A.; Omobowale, T.O.; Yakubu, M.A.; Adedapo, A.D.; Ayodele, A.E.; Adedapo, A.A. Cardioprotective effects and antioxidant status of Andrographis paniculata in isoproterenol-induced myocardial infarction in rats. JOMPED 2019, 3, 1–12. [Google Scholar] [CrossRef]
- Baba, S.P.; Bhatnagar, A. Role of thiols in oxidative stress. Curr. Opin. Toxicol. 2018, 7, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.L.; Luis, P.B.; Varuzza, P.V.; Joseph, A.I.; Presley, S.H.; Chaturvedi, R.; Schneider, C. The anti-inflammatory activity of curcumin is mediated by its oxidative metabolites. J. Biol. Chem. 2017, 292, 21243–21252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandur, S.K.; Ichikawa, H.; Pandey, M.K.; Kunnumakkara, A.B.; Sung, B.; Sethi, G.; Aggarwal, B.B. Role of pro-oxidants and antioxidants in the anti-inflammatory and apoptotic effects of curcumin (diferuloylmethane). Free Radic. Biol. Med. 2007, 43, 568–580. [Google Scholar] [CrossRef] [Green Version]
- Surekha, R.H.; Srikanth, B.B.; Jharna, P.; Ramachandra, R.V.; Dayasagar, R.V.; Jyothy, A. Oxidative stress and total antioxidant status in myocardial infarction. Singap. Med. J. 2007, 48, 137–142. [Google Scholar]
- Matabudul, D.; Pucaj, K.; Bolger, G.; Vcelar, B.; Majeed, M.; Helson, L. Tissue distribution of (Lipocurc™) liposomal curcumin and tetrahydrocurcumin following two-and eight-hour infusions in beagle dogs. Anticancer Res. 2012, 32, 4359–4364. [Google Scholar]
- Bulboacă, A.E.; Bolboacă, S.D.; Stănescu, I.C.; Sfrângeu, C.A.; Porfire, A.; Tefas, L.; Bulboacă, A.C. The effect of intravenous administration of liposomal curcumin in addition to sumatriptan treatment in an experimental migraine model in rats. Int. J. Nanomed. 2018, 13, 3093–3103. [Google Scholar] [CrossRef]
- Arenja, N.; Reichlin, T.; Drexler, B.; Oshima, S.; Denhaerynck, K.; Haaf, P.; Potocki, M.; Breidthardt, T.; Noveanu, M.; Stelzig, C.; et al. Sensitive cardiac troponin in the diagnosis and risk stratification of acute heart failure. J. Intern. Med. 2012, 271, 598–607. [Google Scholar] [CrossRef]
- Lofthus, D.M.; Stevens, S.R.; Armstrong, P.W.; Granger, C.B.; Mahaffey, K.W. Pattern of liver enzyme elevations in acute ST-elevation myocardial infarction. Coron. Artery Di 2012, 23, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, M.E.A. Protective Effect of Curcumin against Isoproterenol-Induced Myocardial Infarction in Adult Male Albino Rat. Egypt. J. Anat. 2011, 34, 15–29. [Google Scholar] [CrossRef]
- Yu, Y.P.; Huang, X.M.; Fu, Y.F. Curcumin protects H9c2 cardiomyocyte against ischemia/reperfusion injury through inactivation of glycogen synthase kinase-3. Int. J. Clin. Exp. Pathol. 2016, 9, 3226–3232. [Google Scholar]
- Bulboacă, A.E.; Porfire, A.S.; Tefas, L.R.; Boarescu, P.M.; Bolboacă, S.D.; Stănescu, I.C.; Bulboacă, A.C.; Dogaru, G. Liposomal Curcumin is Better than Curcumin to Alleviate Complications in Experimental Diabetic Mellitus. Molecules 2019, 24, 846. [Google Scholar] [CrossRef]
- Swamy, A.V.; Gulliaya, S.; Thippeswamy, A.; Koti, B.C.; Manjula, D.V. Cardioprotective effect of curcumin against doxorubicin-induced myocardial toxicity in albino rats. Indian J. Pharmacol. 2012, 44, 73–77. [Google Scholar] [CrossRef]
- Ishihara, M. Acute hyperglycemia in patients with acute myocardial infarction. Circ. J. 2012, 76, 563–567. [Google Scholar] [CrossRef]
- Ceriello, A. Acute hyperglycaemia, a ‘new’ risk factor during myocardial infarction. Eur. Heart J. 2004, 26, 328–331. [Google Scholar] [CrossRef]
- Wickenberg, J.; Ingemansson, S.L.; Hlebowicz, J. Effects of Curcuma longa (turmeric) on postprandial plasma glucose and insulin in healthy subjects. Nutr, J. 2010, 9, 43. [Google Scholar] [CrossRef]
- Fang, M.; Jin, Y.; Bao, W.; Gao, H.; Xu, M.; Wang, D.; Wang, X.; Yao, P.; Liu, L. In vitro characterization and in vivo evaluation of nanostructured lipid curcumin carriers for intragastric administration. Int. J. Nanomed. 2012, 7, 5395–5404. [Google Scholar] [CrossRef] [Green Version]
- Tanwar, V.; Sachdeva, J.; Golechha, M.; Kumari, S.; Arya, D.S. Curcumin Protects Rat Myocardium Against Isoproterenol-Induced Ischemic Injury, Attenuation of Ventricular Dysfunction Through Increased Expression of Hsp27 Alongwith Strengthening Antioxidant Defense System. J. Cardiovasc. Pharmacol. 2010, 55, 377–384. [Google Scholar] [CrossRef]
- Garvin, A.M.; Jackson, M.A.; Korzick, D.H. Inhibition of programmed necrosis limits infarct size through altered mitochondrial and immune responses in the aged female rat heart. Am. J Physiol. Heart Circ. Physiol. 2018, 315, H1434–H1442. [Google Scholar] [CrossRef] [PubMed]
- Ravichandran, R. Pharmacokinetic study of nanoparticulate curcumin, oral formulation for enhanced bioavailability. J. Biomater. Nanobiotechnol. 2013, 4, 291–299. [Google Scholar] [CrossRef]
- Soraya, H.; Khorrami, A.; Garjani, A.; Maleki-Dizaji, N.; Garjani, A. Acute treatment with metformin improves cardiac function following isoproterenol induced myocardial infarction in rats. Pharmacol. Rep. 2012, 64, 1476–1484. [Google Scholar] [CrossRef]
- Boarescu, P.M.; Chirilă, I.; Bulboacă, A.E.; Pârvu, A.; Gheban, D.; Sorana, S.D. Isoproterenol Induced Myocardial Infarction in Rats, Dose Identification. Clujul Med. 2018, 91, S39–S40. [Google Scholar]
- Joe, B.; Nagaraju, A.; Gowda, L.R.; Basrur, V.; Lokesh, B.R. Mass-spectrometric identification of T-kininogen I/thiostatin as an acute-phase inflammatory protein suppressed by curcumin and capsaicin. PLoS ONE 2014, 9, e107565. [Google Scholar] [CrossRef] [PubMed]
- Bulboacă, A.; Bolboacă, S.D.; Suci, S. Protective effect of curcumin in fructose-induced metabolic syndrome and in streptozotocin-induced diabetes in rats. Iran. J. Basic Med. Sci. 2016, 19, 585–593. [Google Scholar] [PubMed]
- Konopelski, P.; Ufnal, M. Electrocardiography in rats, a comparison to human. Physiol. Res. 2016, 65, 717–725. [Google Scholar]
Sample Availability The experimental data will not be publicly available until the associated Ph.D. thesis is published but can be obtained upon request addressed to Paul-Mihai Boarescu (e-mail: [email protected]). |















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group abb. | Day 0 (baseline) | Day 12 (before ISO Administration) | Day 15 (after ISO Administration) | |||
|---|---|---|---|---|---|---|
| SBP (mmHg) | DBP (mmHg) | SBP (mmHg) | DBP (mmHg) | SBP (mmHg) | DBP (mmHg) | |
| C | 136.29 (4.92) | 68.43 (2.88) | 136.29 (2.81) | 68.71 (1.80) | 136.00 (3.74) | 69.57 (2.88) |
| MI-C | 137.14 (2.41) | 68.86 (2.12) | 135.00 (4.73) | 68.29 (2.14) | 137.00 (4.65) | 70.43 (2.37) |
| Cs100+ISO | 136.14 (5.58) | 69.57 (2.37) | 138.85 (2.91) | 69.42 (2.81) | 138.71 (4.03) | 67.86 (4.38) |
| Cs150+ISO | 134.57 (3.60) | 66.14 (2.34) | 134.57 (5.25) | 66.42 (3.69) | 134.43 (4.28) | 69.00 (1.41) |
| Cs200+ISO | 134.71 (3.54) | 68.29 (1.50) | 135.71 (6.67) | 66.29 (2.98) | 133.00 (2.08) | 69.57 (1.81) |
| nC100+ISO | 136.00 (3.60) | 68.57 (1.90) | 134.85 (3.33) | 68.00 (2.58) | 136.00 (4.97) | 68.57 (2.44) |
| nC150+ISO | 136.28 (3.64) | 67.14 (3.80) | 134.43 (5.47) | 67.57 (2.43) | 134.00 (8.29) | 70.71 (3.64) |
| nC200+ISO | 136.14 (2.85) | 67.71 (2.87) | 136.14 (4.29) | 68.85 (1.57) | 137.14 (2.97) | 69.71 (2.06) |
| Group abb. | RR(ms) | HR(b/min) | PR(ms) | QRS(ms) | QT(ms) | QTc(ms) | ST(mV) |
|---|---|---|---|---|---|---|---|
| C | 210 (5.74) | 285 (7.73) | 43 (2.99) | 35 (3.55) | 75 (3.78) | 64 (3.40) | 0.11 (0.04) |
| MI-C | 204 (11.56) | 294 (16.49) | 44 (2.99) | 36 (3.25) | 75 (4.82) | 65 (4.97) | 0.10 (0.01) |
| Cs100+ISO | 211 (9.27) | 285 (12.37) | 44 (3.68) | 36 (3.41) | 76 (4.86) | 64 (3.15) | 0.10 (0.03) |
| Cs150+ISO | 211 (8.38) | 285 (10.96) | 44 (2.91) | 37 (4.76) | 76 (5.16) | 64 (3.70) | 0.10 (0.03) |
| Cs200+ISO | 206 (9.04) | 292 (13.09) | 42 (2.23) | 37 (3.15) | 77 (4.11) | 66 (4.30) | 0.11 (0,03) |
| nC100+ISO | 209 (8.51) | 288 (11.53) | 41 (1.63) | 34 (1.15) | 75 (2.91) | 63 (3.43) | 0.12 (0.03) |
| nC150+ISO | 210 (4.69) | 286 (6.43) | 41 (1.51) | 36 (3.26) | 73 (2.81) | 62 (2.61) | 0.11 (0.03) |
| nC200+ISO | 209 (7.63) | 288 (10.91) | 43 (1.95) | 36 (2.43) | 77 (1.72) | 66 (2.19) | 0.10 (0.01) |
| Group abb. | RR (ms) | HR (b/min) | PR (ms) | QRS (ms) | QT (ms) | QTc (ms) | ST (mV) |
|---|---|---|---|---|---|---|---|
| C | 207 (6.35) | 291 (8.93) | 43 (2.93) | 36 (2.93) | 76 (1.63) | 65 (1.71) | 0.11 (0.02) |
| MI-C | 210 (6,34) | 286 (8.55) | 44 (1.46) | 36 (3.04) | 77 (3.39) | 65 (3.73) | 0.10 (0.01) |
| Cs100+ISO | 213 (5.40) | 282 (7.21) | 43 (1.51) | 35 (2.29) | 78 (2.37) | 65 (2.58) | 0.09 (0.03) |
| Cs150+ISO | 218 (3.72) | 275 (4.69) | 43 (1.57) | 37 (2.41) | 75 (2,69) | 62 (2.30) | 0.10 (0.02) |
| Cs200+ISO | 225 (7.62) | 267 (8.92) | 43 (2.12) | 36 (3.15) | 76 (3,35) | 61 (3.25) | 0.10 (0.02) |
| nC100+ISO | 225 (2.37) | 266 (2.79) | 42 (1.27) | 35 (1.89) | 75 (4,06) | 61 (3.32) | 0.11 (0.02) |
| nC150+ISO | 232 (1.99) | 258 (2.21) | 43 (2.04) | 35 (1.72) | 75 (2,73) | 60 (2.11) | 0.10 (0.02) |
| nC200+ISO | 244 (3.27) | 246 (3.29) | 44 (2.76) | 35 (2.23) | 78 (1.99) | 61 (1.76) | 0.10 (0.03) |
| Group abb. | RR (ms) | HR (b/min) | PR (ms) | QRS (ms) | QT (ms) | QTc (ms) | ST (mm) |
|---|---|---|---|---|---|---|---|
| C | 205 (3.60) | 292 (5.11) | 42 (1.91) | 35 (3.67) | 75 (1.51) | 64 (1.28) | 0.11 (0.04) |
| MI-C | 177 (4.75) | 339 (9.12) | 45 (2.79) | 50 (2.37) | 114 (7.46) | 105 (7.3) | −0.06 (0.03) |
| Cs100+ISO | 207 (3.35) | 290 (4.68) | 43 (1.50) | 49 (1.11) | 107 (2.87) | 91 (2.97) | −0.04 (0.01) |
| Cs150+ISO | 212 (3.10) | 284 (4.14) | 42 (3.34) | 41 (2.07) | 103 (2.94) | 87 (2.61) | −0.03 (0.02) |
| Cs200+ISO | 219 (2.56) | 274 (3.18) | 44 (2.34) | 39 (1.27) | 98 (2.61) | 81 (2.5) | −0.01 (0.01) |
| nC100+ISO | 227 (3.15) | 265 (3.75) | 42 (2.43) | 37 (2.04) | 96 (3.34) | 78 (2.37) | 0 (0.02) |
| nC150+ISO | 235 (3.21) | 256 (3.51) | 44 (2.98) | 37 (1.21) | 87 (3.86) | 69 (3,06) | 0.01 (0.01) |
| nC200+ISO | 248 (3.55) | 242 (3.48) | 43 (2.06) | 35 (1.35) | 82 (3.95) | 64 (2.91) | 0.04 (0.02) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Râjnoveanu, R.-M.; Bolboacă, S.D. Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules 2019, 24, 2802. https://doi.org/10.3390/molecules24152802
Boarescu P-M, Boarescu I, Bocșan IC, Pop RM, Gheban D, Bulboacă AE, Nicula C, Râjnoveanu R-M, Bolboacă SD. Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules. 2019; 24(15):2802. https://doi.org/10.3390/molecules24152802
Chicago/Turabian StyleBoarescu, Paul-Mihai, Ioana Boarescu, Ioana Corina Bocșan, Raluca Maria Pop, Dan Gheban, Adriana Elena Bulboacă, Cristina Nicula, Ruxandra-Mioara Râjnoveanu, and Sorana D. Bolboacă. 2019. "Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes" Molecules 24, no. 15: 2802. https://doi.org/10.3390/molecules24152802
APA StyleBoarescu, P. -M., Boarescu, I., Bocșan, I. C., Pop, R. M., Gheban, D., Bulboacă, A. E., Nicula, C., Râjnoveanu, R. -M., & Bolboacă, S. D. (2019). Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules, 24(15), 2802. https://doi.org/10.3390/molecules24152802