
Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review

 ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology
3. Insulinotropic Peptides
4. Tirzepatide
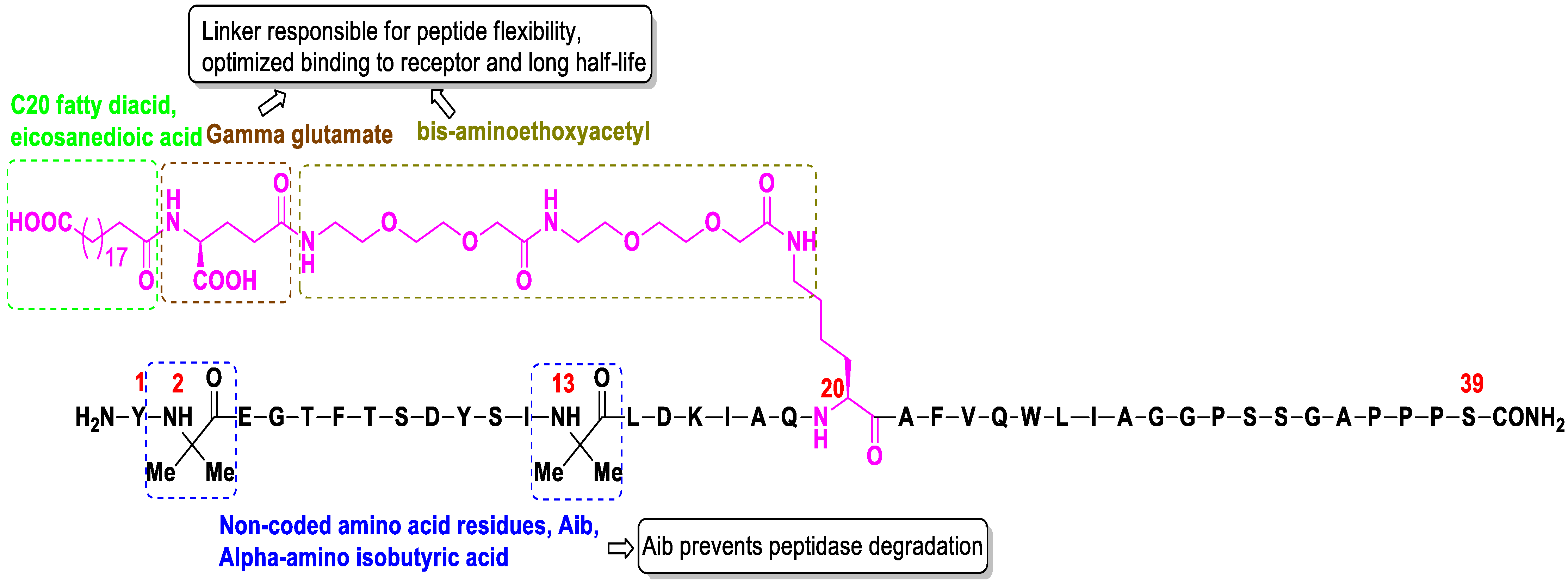
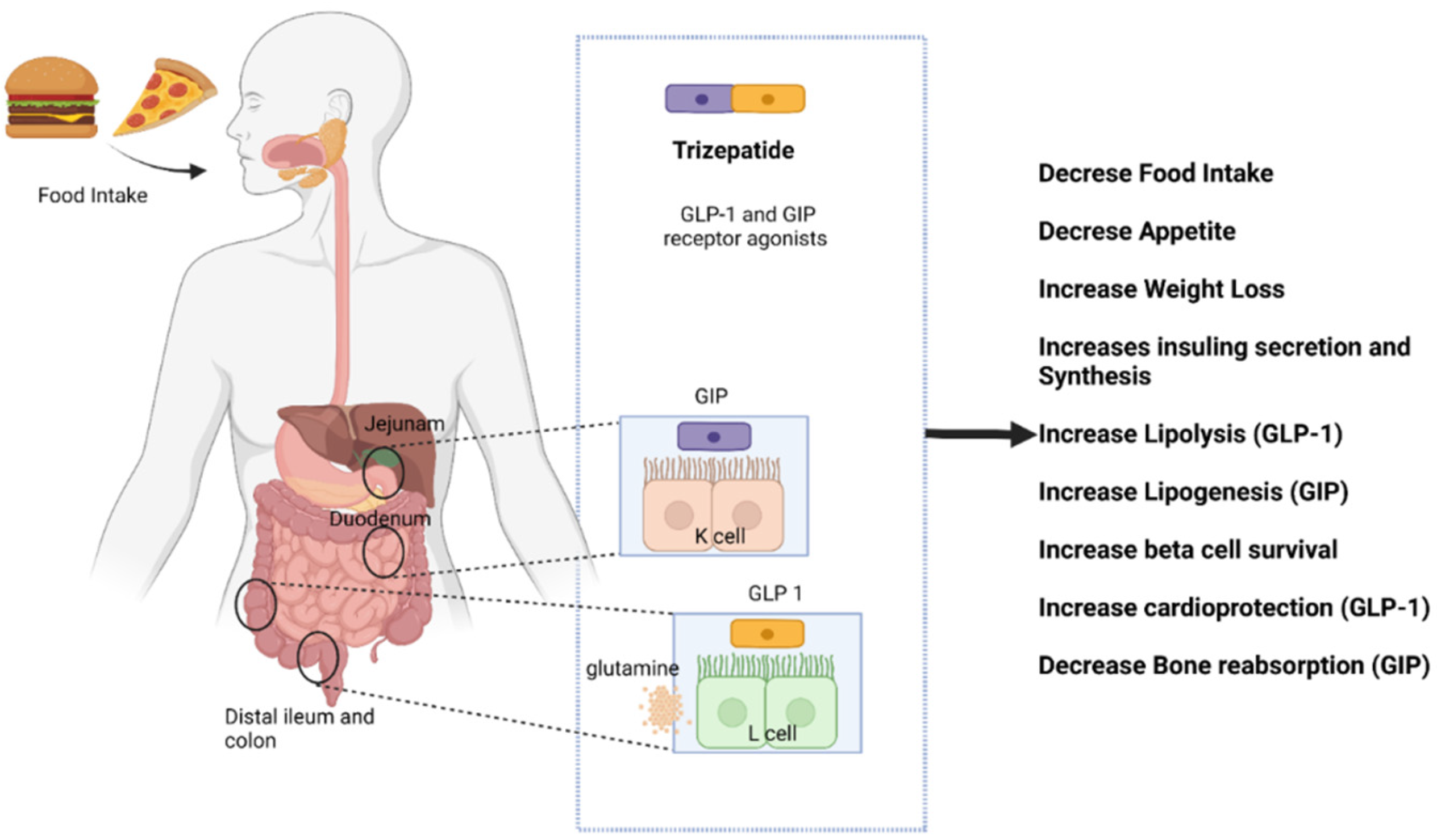
4.1. Structure and Activity
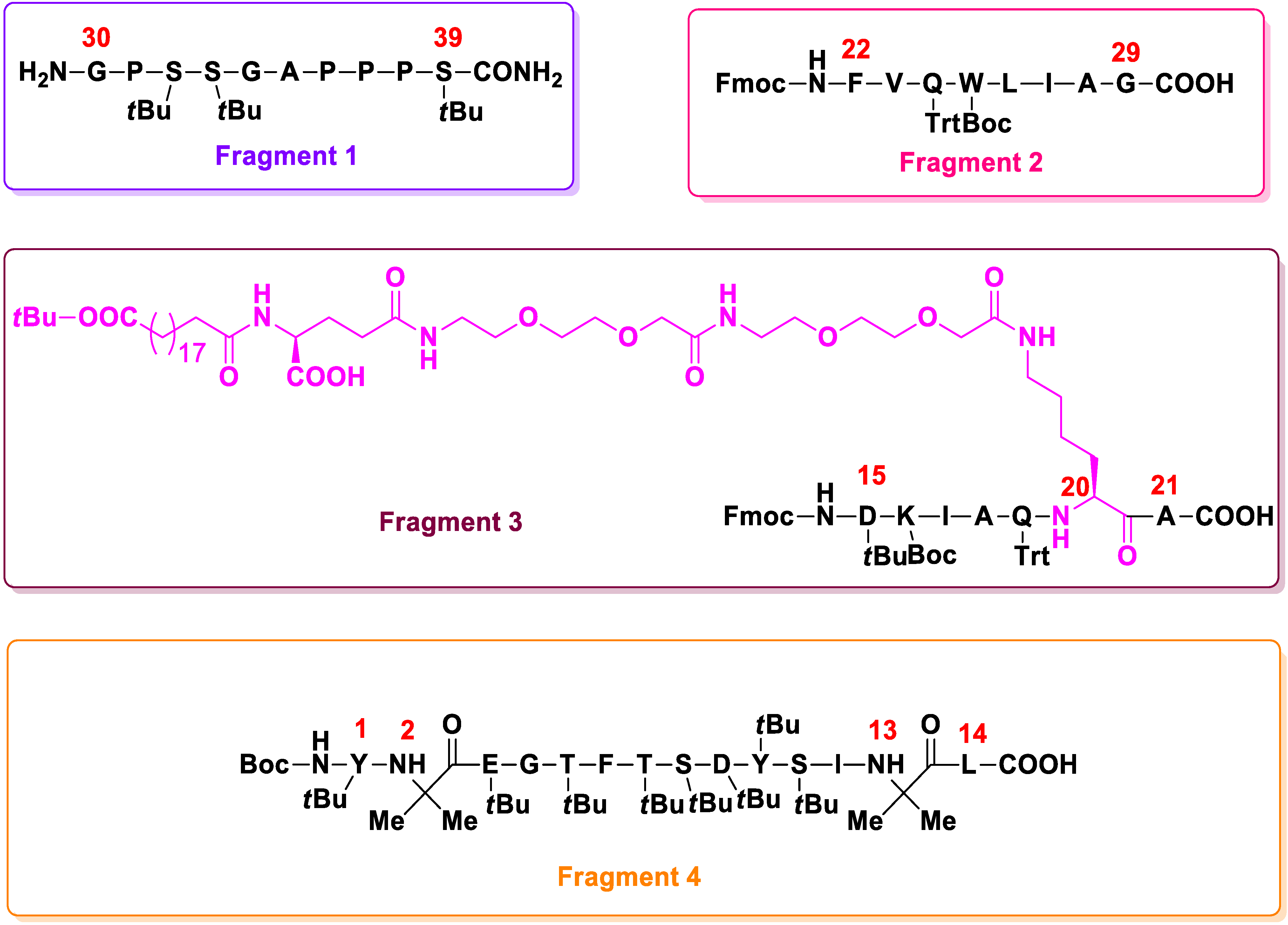
4.2. Synthesis
4.3. Clinical Development
4.4. Pharmacokinetics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Sheldon, T.A.; Wright, J. Twin epidemics of COVID-19 and non-communicable disease. BMJ 2020, 369, 2618. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Sarma, D.K.; Shubham, S.; Kumawat, M.; Verma, V.; Prakash, A.; Tiwari, R. Environmental endocrine-disrupting chemical exposure: Role in non-communicable diseases. Front. Public Health 2020, 8, 553850. [Google Scholar] [CrossRef] [PubMed]
- Mancilla, V.J.; Peeri, N.C.; Silzer, T.; Basha, R.; Felini, M.; Jones, H.P.; Phillips, N.; Tao, M.H.; Thyagarajan, S.; Vishwanatha, J.K. Understanding the interplay between health disparities and epigenomics. Front. Genet. 2020, 11, 903. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161–173. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 May 2022).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Technical Report; WHO: Geneva, Switzerland, 2000.
- Guh, P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88–120. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Diabetes, Key Facts; WHO: Geneva, Switzerland, 10 November 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 5 May 2022).
- Alam, S.; Hasan, M.K.; Neaz, S.; Hussain, N.; Hossain, M.F.; Rahman, T. Diabetes mellitus: Insights from epidemiology, biochemistry, risk factors, diagnosis, complications and comprehensive management. Diabetology 2021, 2, 36–50. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, S.; Basit, A.; Chan, J.C.N.; et al. IDF Diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119–109132. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef]
- Sebire, S.J.; Toumpakari, Z.; Turner, K.M.; Cooper, A.R.; Page, A.S.; Malpass, A.; Andrews, A.R. “I’ve made this my lifestyle now”: A prospective qualitative study of motivation for lifestyle change among people with newly diagnosed type two diabetes mellitus. BMC Public Health 2018, 18, 204. [Google Scholar] [CrossRef] [Green Version]
- Ganesan, K.; Rana, M.B.M.; Sultan, S. Oral Hypoglycemic Medications; Updated 8 May 2022; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Costello, R.A.; Shivkumar, N.S. Sulfonylureas; Updated 23 February 2022; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zeynaloo, E.; Stone, L.D.; Dikici, E.; Ricordi, C.; Deo, S.K.; Bachas, L.G.; Daunert, S.; Lanzoni, G. Delivery of therapeutic agents and cells to pancreatic islets: Towards a new era in the treatment of diabetes. Mol. Aspects Med. 2022, 83, 101063–101084. [Google Scholar] [CrossRef]
- Marín-Peñalver, J.J.; Martín-Timón, I.; Sevillano-Collantes, C.; Del Cañizo-Gómez, F.J. Update on the treatment of type 2 diabetes mellitus. World J. Diabetes 2016, 7, 354–395. [Google Scholar] [CrossRef] [PubMed]
- Al-Tabakha, M.M. Future prospect of insulin inhalation for diabetic patients: The case of Afrezza versus Exubera. J. Control Release 2015, 215, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Modi, P. Diabetes beyond insulin: Review of new drugs for treatment of diabetes mellitus. Curr. Drug Discov. Technol. 2007, 4, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Tupas, G.D.; Otero, M.C.B.; Ebhohimen, I.E.; Egbuna, C.; Aslam, M. Chapter 8—Antidiabetic Lead Compounds and Targets for Drug Development. In Phytochemicals as Lead Compounds for New Drug Discovery; Egbuna, C., Kumar, S., Ifemeje, J.C., Ezzat, S.M., Kaliyaperumal, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 127–141. [Google Scholar]
- Frias, J.P.; Nauck, M.A.; Van, J.; Kutner, M.E.; Cui, X.; Benson, C.; Urva, S.; Gimeno, R.E.; Milicevic, Z.; Robins, D.; et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: A randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet 2018, 392, 2180–2193. [Google Scholar] [CrossRef]
- Frias, J.P.; Nauck, M.A.; Van, J.; Benson, C.; Bray, R.; Cui, X.; Milicevic, Z.; Urva, S.; Haupt, A.; Robins, D.A. Efficacy and tolerability of tirzepatide, a dual glucose-dependent insulinotropic peptide and glucagon-like peptide-1 receptor agonist in patients with type 2 diabetes: A 12-week, randomized, double-blind, placebo-controlled study to evaluate different dose-escalation regimens. Diabetes Obes. Metab. 2020, 22, 938–946. [Google Scholar]
- Apostolopoulos, V.; Bojarska, J.; Chai, T.-T.; Elnagdy, S.; Kaczmarek, K.; Matsoukas, J.; New, R.; Parang, K.; Lopez, O.P.; Parhiz, H.; et al. A Global review on short peptides: Frontiers and perspectives. Molecules 2021, 26, 430. [Google Scholar] [CrossRef]
- Nauck, M.A.; Meier, J.J. The incretin effect in healthy individuals and those with type 2 diabetes: Physiology, pathophysiology, and response to therapeutic interventions. Lancet Diabetes Endocrinol. 2016, 4, 525–536. [Google Scholar] [CrossRef]
- Müller, T.D.; Finan, B.; Bloom, S.R.; D’Alessio, D.; Drucker, D.J.; Flatt, P.R.; Fritsche, A.; Gribble, F.; Grill, H.J.; Habaner, J.F.; et al. Glucagon-like peptide 1 (GLP-1). Mol. Metab. 2019, 30, 72–130. [Google Scholar] [CrossRef]
- Gupta, S.; Sen, U. More than just an enzyme: Dipeptidyl peptidase-4 (DPP-4) and its association with diabetic kidney remodelling. Pharmacol. Res. 2019, 147, 104391–104403. [Google Scholar] [CrossRef]
- Frías, J.P. Tirzepatide: A glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) dual agonist in development for the treatment of type 2 diabetes. Expert Rev. Endocrinol. Metab. 2020, 15, 379–394. [Google Scholar] [CrossRef]
- Andreadis, P.; Karagiannis, T.; Malandris, K.; Avgerinos, I.; Liakos, A.; Manolopoulos, A.; Beklari, E.; Matthews, D.R.; Tsapas, A. Semaglutide for type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes. Metab. 2018, 20, 2255–2263. [Google Scholar] [CrossRef]
- Bokvist, B.K.; Coskun, T.; Cummins, R.C.; Alsina-Fernandez, J. GIP and GLP-1 Co-Agonist Compounds. U.S. Patent 947478, 25 October 2016. [Google Scholar]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide once weekly for the treatment of obesity. N. Engl. J. Med. 2022, 11, 127. [Google Scholar] [CrossRef]
- Wang, L. Designing a dual GLP-I R/GIPR agonist from tirzepatide: Comparing residues between tirzepatide, GLP-I, and GIP. Drug Des. Dev. Ther. 2022, 16, 1547–1560. [Google Scholar] [CrossRef] [PubMed]
- Cosku, T.; Sloop, K.W.; Loghin, C.; Alsina-Fernandez, J.; Urva, S.; Bokvist, K.B.; Cui, X.; Briere, D.A.; Cabrera, O.; Roell, W.C.; et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol. Metab. 2018, 18, 3–14. [Google Scholar] [CrossRef]
- Østergaard, S.; Paulsson, J.F.; Kofoed, J.; Zosel, F.; Olsen, J.; Jeppesen, C.B.; Spetzler, J.; Ynddal, L.; Schleiss, L.G.; Christoffersen, B.Ø.; et al. The effect of fatty diacid acylation of human PYY3-36 on Y2 receptor potency and half-life in minipigs. Sci. Rep. 2021, 11, 21179–21194. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Willard, F.S.; Feng, D.; Alsina-Fernandez, J.; Chen, Q.; Vieth, M.; Ho, J.D.; Showalter, A.D.; Stutsman, C.; Ding, L.; et al. Structural determinants of dual incretin receptor agonism by tirzepatide. Proc. Natl. Acad. Sci. USA 2022, 119, 211650611–211650622. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.; Chan, J.C.N. The emerging role of incretins and twincretins. Nat. Rev. Endocrinol. 2021, 18, 73–74. [Google Scholar] [CrossRef]
- Fisman, E.Z.; Tenenbaum, A. The dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist tirzepatide: A novel cardiometabolic therapeutic prospect. Cardiovasc. Diabetol. 2022, 20, 225–230. [Google Scholar] [CrossRef]
- Nowak, M.; Nowak, W.; Grzeszczak, W. Tirzepatide-a dual GIP/GLP-1 receptor agonist—A new antidiabetic drug with potential metabolic activity in the treatment of type 2 diabetes. Endokrynol. Pol. 2022, 1–11. [Google Scholar] [CrossRef]
- Starling, S. GIP-GLP1 receptor agonist shows promise. Nat. Rev. Endocrinol. 2022, 18, 391. [Google Scholar] [CrossRef]
- Dutta, D.; Surana, V.; Singla, R.; Aggarwal, S.; Sharma, M. Efficacy and safety of novel twincretin tirzepatide a dual GIP and GLP-1 receptor agonist in the management of type-2 diabetes: A cochrane meta-analysis. Indian J. Endocrinol. Metab. 2021, 25, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Pelle, M.C.; Provenzano, M.; Zaffina, I.; Pujia, R.; Giofrè, F.; Lucà, S.; Andreucci, M.; Sciacqua, A.; Arturi, F. Role of a dual glucose-dependent insulinotropic peptide (GIP)/glucagon-like peptide-1 receptor agonist (twincretin) in glycemic control: From pathophysiology to treatment. Life 2022, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, T.; Avgerinos, I.; Liakos, A.; Del Prato, S.; Matthews, D.R.; Tsapas, A.; Bekiari, E. Management of type 2 diabetes with the dual GIP/GLP-1 receptor agonist tirzepatide: A systematic review and meta-analysis. Diabetologia 2022, 1–11. [Google Scholar] [CrossRef]
- Willard, F.S.; Douros, J.D.; Gabe, M.B.; Showalter, A.D.; Wainscott, D.B.; Suter, T.M.; Capozzi, M.E.; van der Welden, W.J.C.; Stutsman, C.; Cardona, G.R.; et al. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight 2020, 5, e140532–e140549. [Google Scholar] [CrossRef]
- Scheen, A.J. Add-on value of trizepatide versus semaglutide. Lancet Diabetes Endocrinol. 2022, 10, 377–378. [Google Scholar] [CrossRef]
- Gastaldelli, A.; Cusi, K.; Lando, L.F.; Bray, R.; Brouwers, B.; Rodriguez, A. Effect of trizepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): A substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol. 2022, 10, 393–406. [Google Scholar] [CrossRef]
- Ahangarpour, M.; Kavianinia, I.; Harris, P.W.; Brimble, M.A. Photo-induced radical thiol-ene chemistry: A versatile toolbox for peptide-based drug design. Chem. Soc. Rev. 2021, 50, 898–944. [Google Scholar] [CrossRef]
- Targher, G. Tirzepatide adds hepatoprotection to its armoury. Lancet Diabetes Endocrinol. 2022, 10, 374–375. [Google Scholar] [CrossRef]
- Zhao, F.; Zhou, Q.; Cong, Z.; Hang, K.; Zou, X.; Zhang, C.; Chen, Y.; Dai, A.; Liang, A.; Ming, Q.; et al. Structural insight into multiplexed pharmacological actions of trizepatide and peptide 20 at the GIP, GLP-1 or glucagon receptors. Nat. Commun. 2022, 13, 1057–1073. [Google Scholar] [CrossRef]
- Heise, T.; Mari, A.; DeVries, J.H.; Urva, S.; Li, J.; Pratt, E.J.; Coskun, T.; Thomas, M.K.; Mather, K.J.; Haupt, A.; et al. Effects of subcutaneous tirzepatide versus placebo or semaglutide on pancreatic islet function and insulin sensitivity in adults with type 2 diabetes: A multicentre, randomised, double-blind, parallel-arm, phase 1 clinical trial. Lancet Diabetes Endocrinol. 2022, 10, 418–429. [Google Scholar] [CrossRef]
- Chipkin, S.R. Tirzepatide for patients with type 2 diabetes. JAMA 2022, 327, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Frederick, M.O.; Boyse, R.A.; Braden, T.M.; Calvin, J.R.; Campbell, B.M.; Changi, S.M.; Coffin, S.R.; Condon, C.; Gowran, O.; McClary, J.; et al. Kilogram-scale GMP manufacture of tirzepatide using a hybrid SPPS/LPPS approach with continuous manufacturing. Org. Process Res. Dev. 2021, 25, 1628–1636. [Google Scholar] [CrossRef]
- May, S.A.; Johnson, M.D.; Buser, J.Y.; Campbell, A.N.; Frank, S.A.; Haeberle, B.D.; Hoffman, P.C.; Lambertus, G.R.; McFarland, A.D.; Moher, E.D.; et al. Development and manufacturing GMP scale-up of a continuous ir-catalyzed homogeneous reductive amination reaction. Org. Process Res. Dev. 2016, 20, 1870–1898. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, Z.; Lin, S.; Jin, H.; Gao, S.; Zhu, Y.; Jin, J. Nanoparticle-templated nanofiltration membranes for ultrahigh performance desalination. Nat. Commun. 2018, 9, 2004–2013. [Google Scholar] [CrossRef] [PubMed]
- Min, T.; Bain, S.C. The role of tirzepatide, dual GIP and GLP-1 receptor agonist, in the management of type 2 diabetes: The SURPASS clinical trials. Diabetes Ther. 2021, 12, 143–157. [Google Scholar] [CrossRef]
- Ludvik, B.; Giorgino, F.; Jódar, E.; Frias, J.P.; Landó, L.F.; Brown, K.; Bray, R.; Rodríguez, A. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): A randomised, open-label, parallel-group, phase 3 trial. Lancet 2021, 398, 583–598. [Google Scholar] [CrossRef]
- Frías, J.P.; Davies, M.J.; Rosenstock, J.; Pérez Manghi, F.C.; Fernández Landó, L.; Bergman, B.K.; Liu, B.; Cui, X.; Brown, K. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N. Engl. J. Med. 2021, 385, 503–515. [Google Scholar] [CrossRef]
- Apostolopoulos, V.; Bojarska, J.; Chai, T.-T.; Feehan, J.; Kaczmarek, K.; Matsoukas, J.M.; Paredes Lopez, O.; Saviano, M.; Skwarczynski, M.; Smith-Carpenter, J.; et al. New advances in short peptides: Looking forward. Molecules 2022, 27, 3635. [Google Scholar] [CrossRef]
- Apostolopoulos, V.; Bojarska, J.; Feehan, J.; Matsoukas, J.; Wolf, W. Smart therapies for pandemics: A potential of short peptides. Front. Pharmacol. 2022; accepted. [Google Scholar] [CrossRef]
- Ohwaki, K.; Furihata, K.; Mimura, M.; Oura, T.; Imaoka, T. 1024-P: Effect of tirzepatide, a dual GIP and GLP-1 receptor agonist, on glycemic control and body weight in Japanese patients with T2DM. Diabetes 2019, 68 (Suppl. S1). [Google Scholar] [CrossRef]
- Furihata, K.; Mimura, H.; Urva, S.; Oura, T.; Ohwaki, K.; Imaoka, T. A phase 1 multiple-ascending dose study of tirzepatide in Japanese participants with type 2 diabetes. Diabetes Obes. Metab. 2022, 24, 239–246. [Google Scholar] [CrossRef]
- Thomas, M.K.; Nikooienejad, A.; Bray, R.; Cui, X.; Wilson, J.; Duffin, K.; Milicevic, Z.; Haupt, A.; A Robins, D. Dual GIP and GLP-1 receptor agonist tirzepatide improves beta-cell function and insulin sensitivity in type 2 diabetes. J. Clin. Endocrinol. Metab. 2021, 106, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Dahl, D.; Onishi, Y.; Norwood, P.; Huh, R.; Bray, R.; Patel, H.; Rodríguez, Á. Effect of subcutaneous tirzepatide vs. placebo added to titrated insulin glargine on glycemic control in patients with type 2 diabetes: The SURPASS-5 randomized clinical trial. JAMA 2022, 327, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Mullard, A. Lilly’s tirzepatide secures first approval in diabetes, paving path for dual-acting hormone mimetics. Nat. Rev. Drug Discov. 2022, 21, 480. [Google Scholar] [CrossRef] [PubMed]
- Moura, F.A.; Scirica, B.M.; Ruff, C.T. Tirzepatide for diabetes: On track to SURPASS current therapy. Nat. Med. 2022, 28, 450–451. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chavda, V.P.; Ajabiya, J.; Teli, D.; Bojarska, J.; Apostolopoulos, V. Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review. Molecules 2022, 27, 4315. https://doi.org/10.3390/molecules27134315
Chavda VP, Ajabiya J, Teli D, Bojarska J, Apostolopoulos V. Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review. Molecules. 2022; 27(13):4315. https://doi.org/10.3390/molecules27134315
Chicago/Turabian StyleChavda, Vivek P., Jinal Ajabiya, Divya Teli, Joanna Bojarska, and Vasso Apostolopoulos. 2022. "Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review" Molecules 27, no. 13: 4315. https://doi.org/10.3390/molecules27134315
APA StyleChavda, V. P., Ajabiya, J., Teli, D., Bojarska, J., & Apostolopoulos, V. (2022). Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review. Molecules, 27(13), 4315. https://doi.org/10.3390/molecules27134315