
Formulation of Chrysomycin A Cream for the Treatment of Skin Infections

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Cells and Animals
2.3. Formulation Screening
- Tefose® 63, Labrifil® M 1944 CS and 1-octadecanol were added into the vial. Then, the mixture was heated at 75 °C (600 rpm, 20 min) until complete mixing to prepare the oil phase.
- 1,2-Propanediol, purified water, and benzoic acid were added into a 2 mL Eppendorf tube, then heated with stirring at 75 °C for 20 min to prepare the water phase.
- The water phase was then added to the oil phase at 75 °C, and magnetic stirring was used for low-speed emulsification (600 rpm, 20 min). Then, the mixture was cooled down to 55 °C.
- 2-(2-Ethoxyethoxy) ethanol and chrysomycin A powder were added into a 1 mL Eppendorf tube; chrysomycin A was dispersed in 2-(2-Ethoxyethoxy) ethanol.
- The mixture of Step 4 was added to the mixture of Step 3 and emulsified at low speed with magnetic stirring at 55 °C (600 rpm, 20 min), then cooled naturally to room temperature.
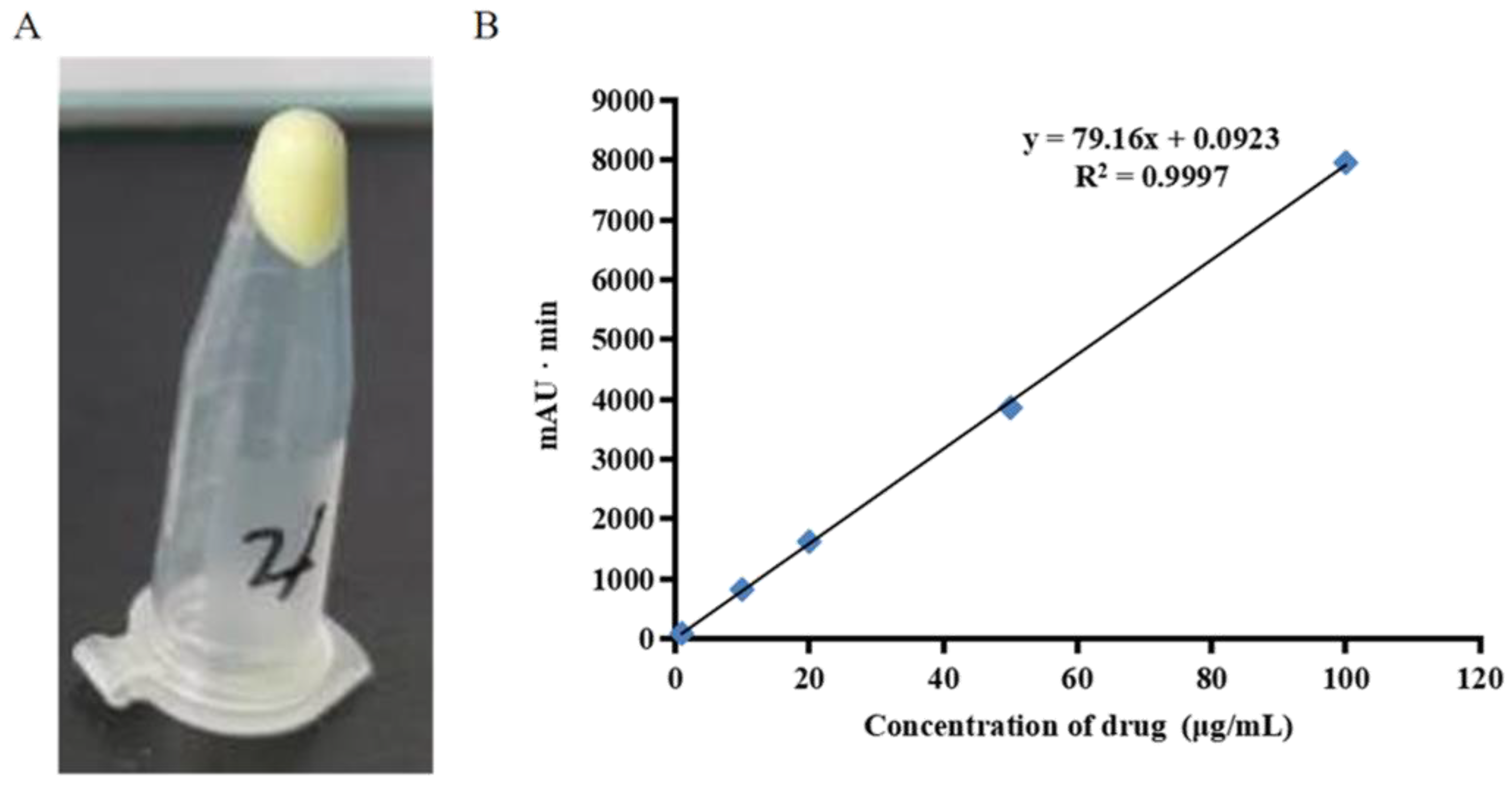
2.4. Chrysomycin A Extraction and Recovery
2.5. Stability Study
2.6. Organoleptic Appreciation
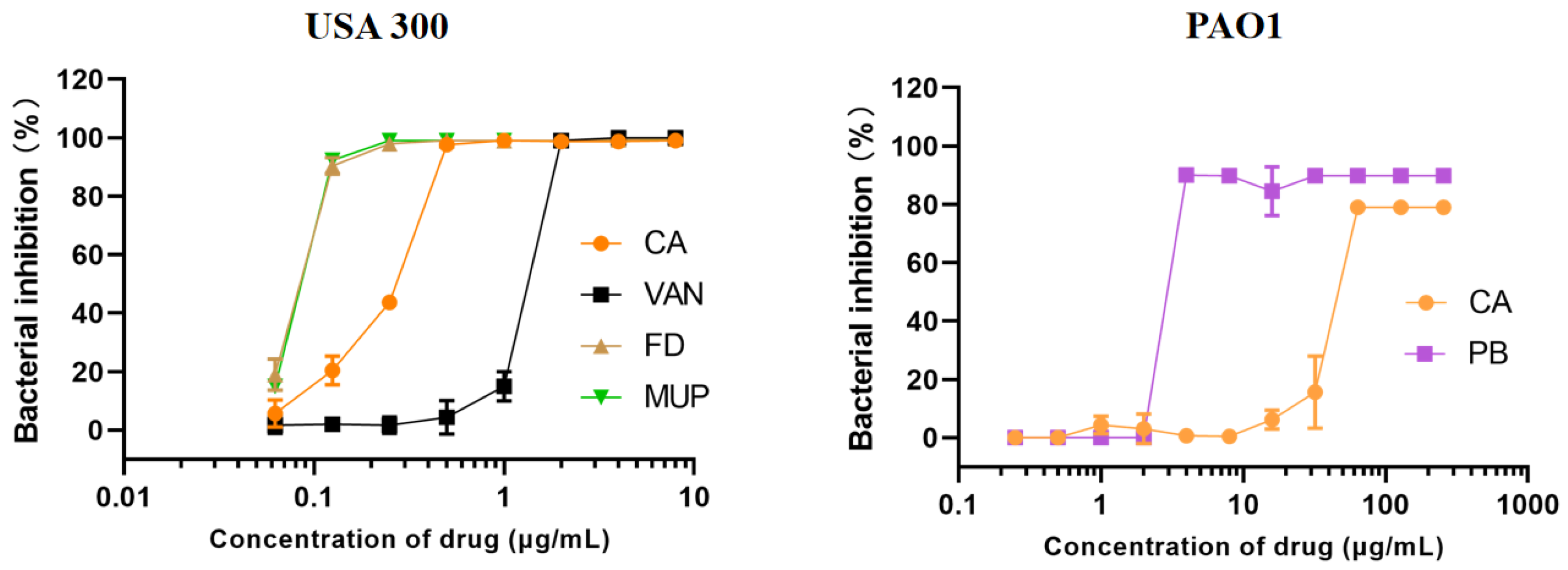
2.7. In Vitro Minimum Inhibitory Concentration of Chrysomycin A
2.8. In Vitro Antibacterial Activity of Chrysomycin A Cream
2.9. In Vivo Antibacterial Activity Evaluation of Chrysomycin A Cream
2.10. Statistical Analysis
3. Results and Discussion
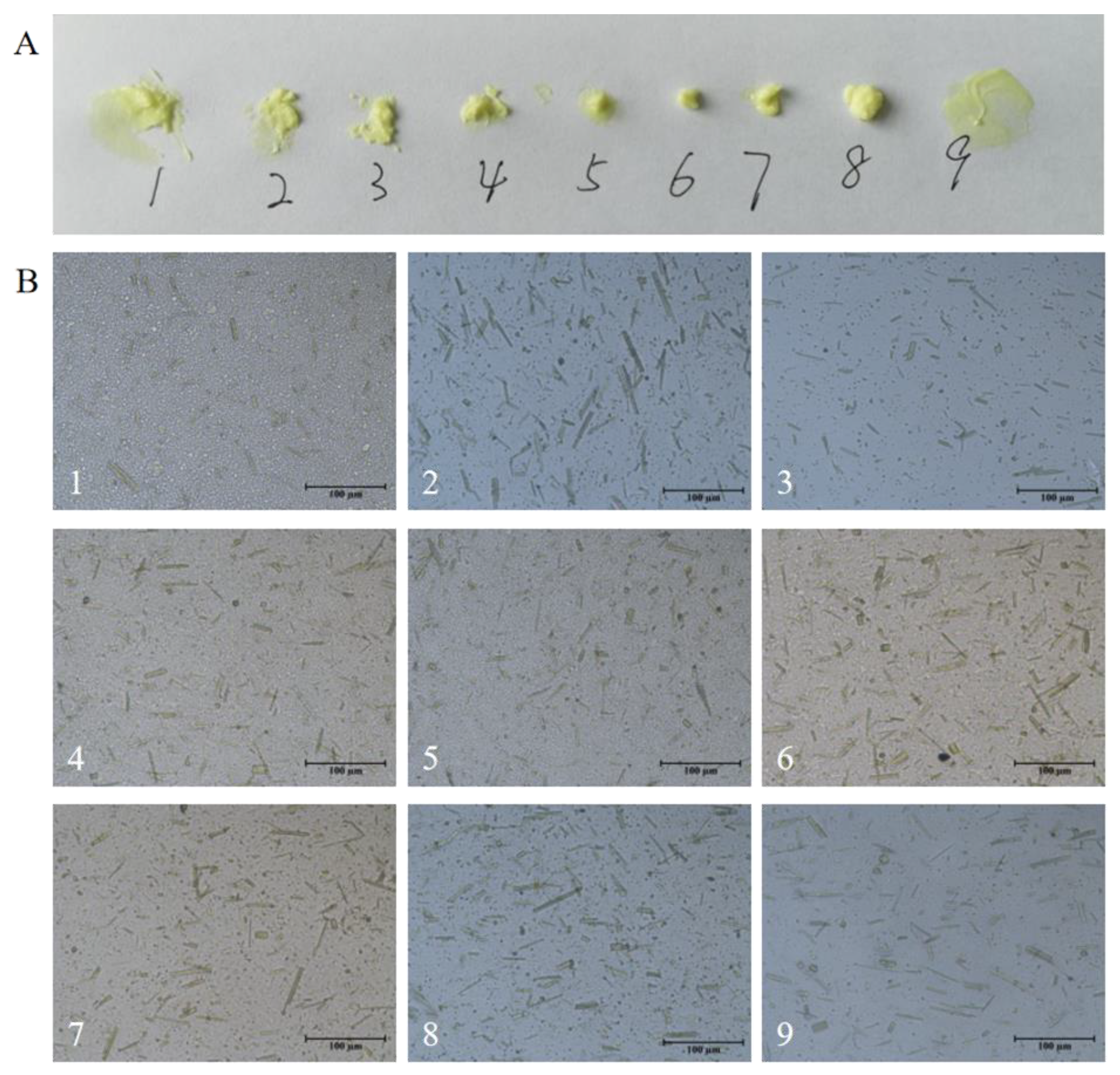
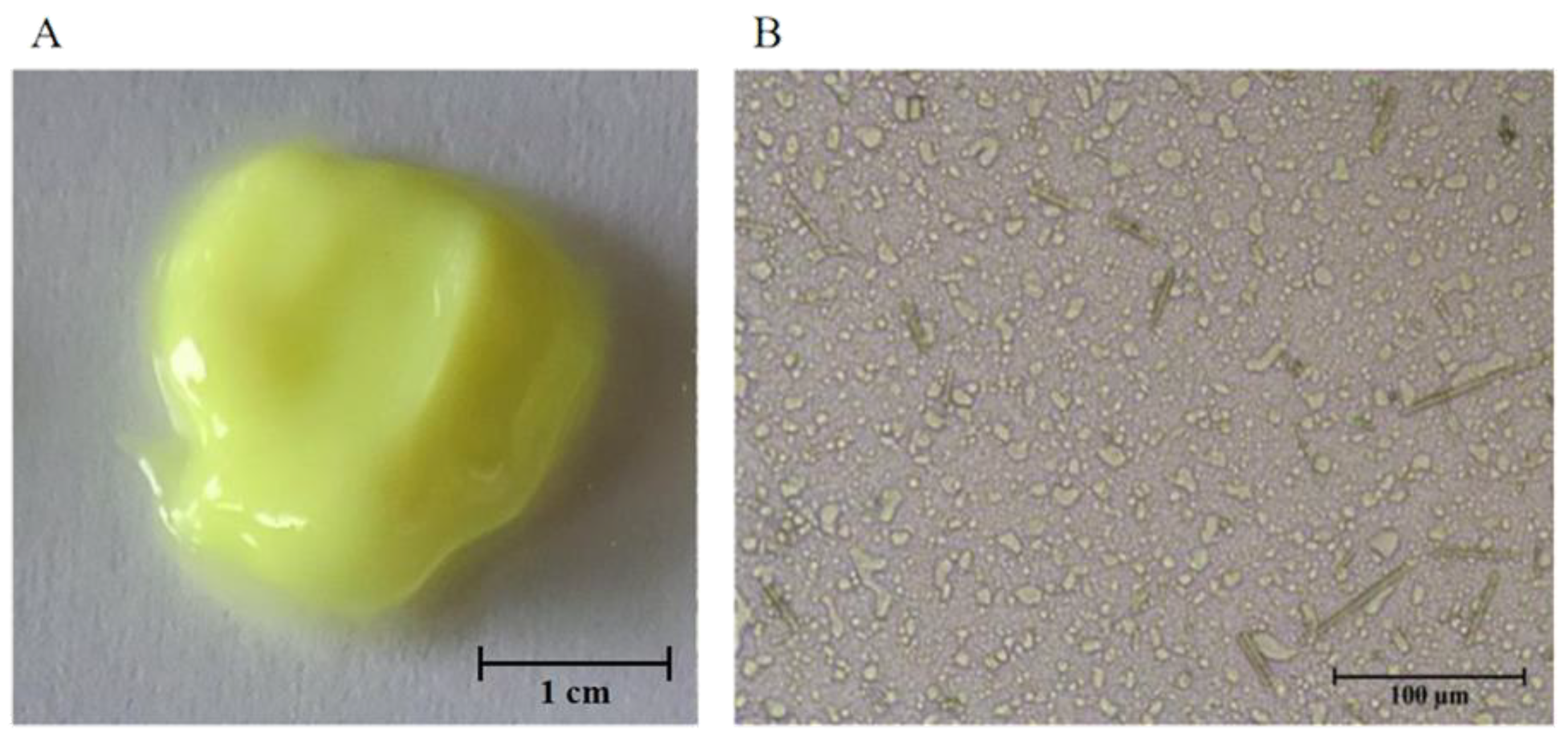
3.1. Formation of CA Cream
- Tefose® 63, Labrifil® M 1944 CS, and 1-octadecanol were added into the vial. Then, the mixture was heated at 75 °C (600 rpm, 20 min) until complete mixing to prepare the oil phase.
- 1,2-propanediol, purified water, and benzoic acid were added into a 2 mL Eppendorf tube, then heated by stirring at 75 °C for 20 min to prepare the water phase.
- The water phase was then added to the oil phase at 75 °C, and magnetic stirring was used for low-speed emulsification (600 rpm, 20 min). After that, the handled homogenizer was used for 5 min, and the mixture was cooled down to 55 °C.
- 2-(2-Ethoxyethoxy) ethanol and chrysomycin A powder were added into a 1 mL Eppendorf tube; chrysomycin A was dispersed in 2-(2-ethoxyethoxy) ethanol.
- The mixture of Step 4 was added to the mixture of Step 3 and emulsify at low speed with magnetic stirring at 55 °C (600 rpm, 20 min). After that, the handled homogenizer was used for 5 min. Finally, the product was cooled to room temperature.
- (1)
- Influence on stability: B > A > C > D;
- (2)
- Influence on spreading: D > B > C > A;
- (3)
- Influence on appearance: D > B > A = C;
- (4)
- The higher the B content, the better performance of the cream;
- (5)
- The lower the A, C, and D content, the better performance of the cream.
3.2. Organoleptic Appreciation
3.3. Stability Study
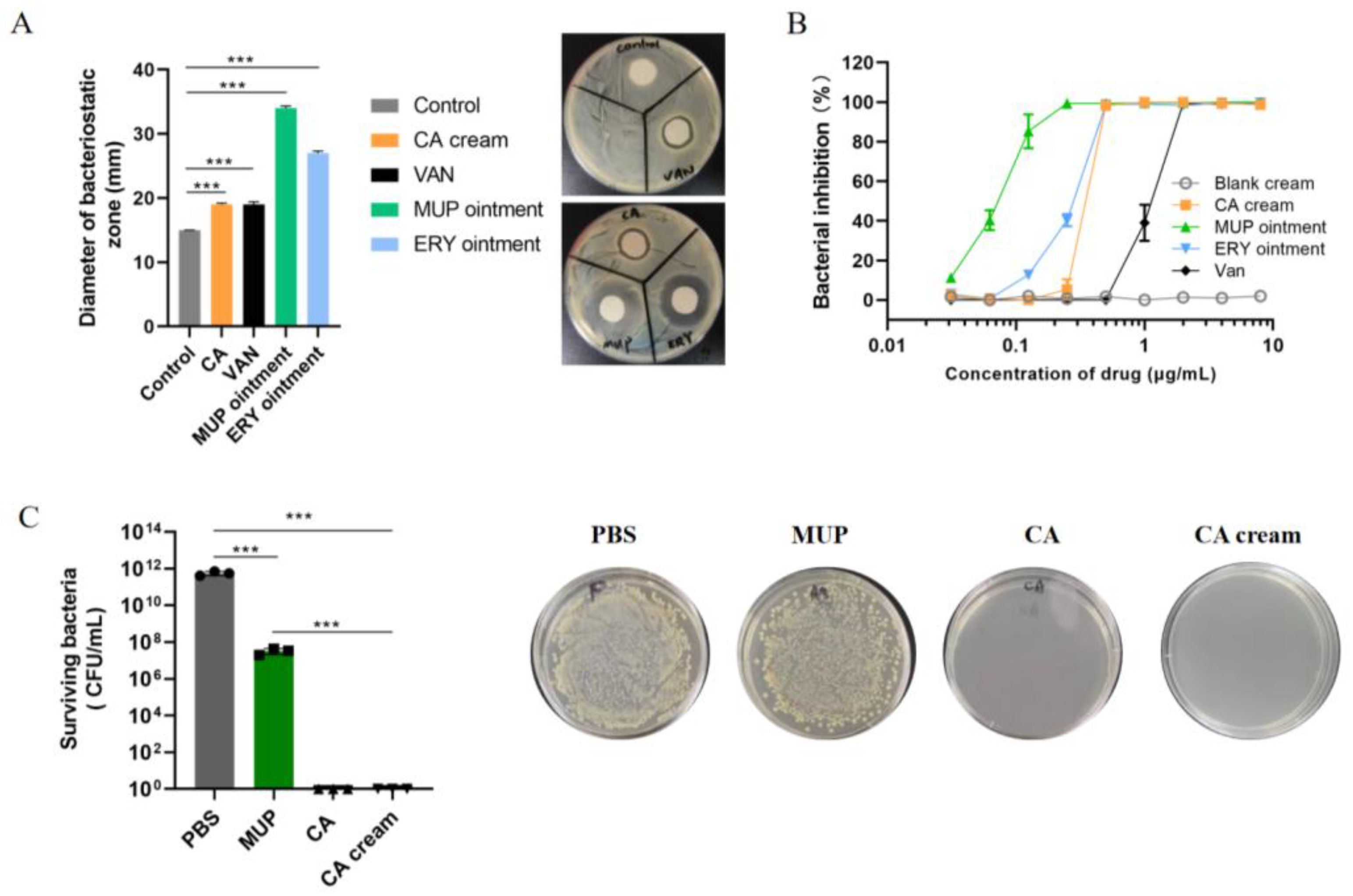
3.4. In Vitro Minimum Inhibitory Concentration of Chrysomycin A
3.5. In Vitro Antibacterial Activity of Chrysomycin A Cream
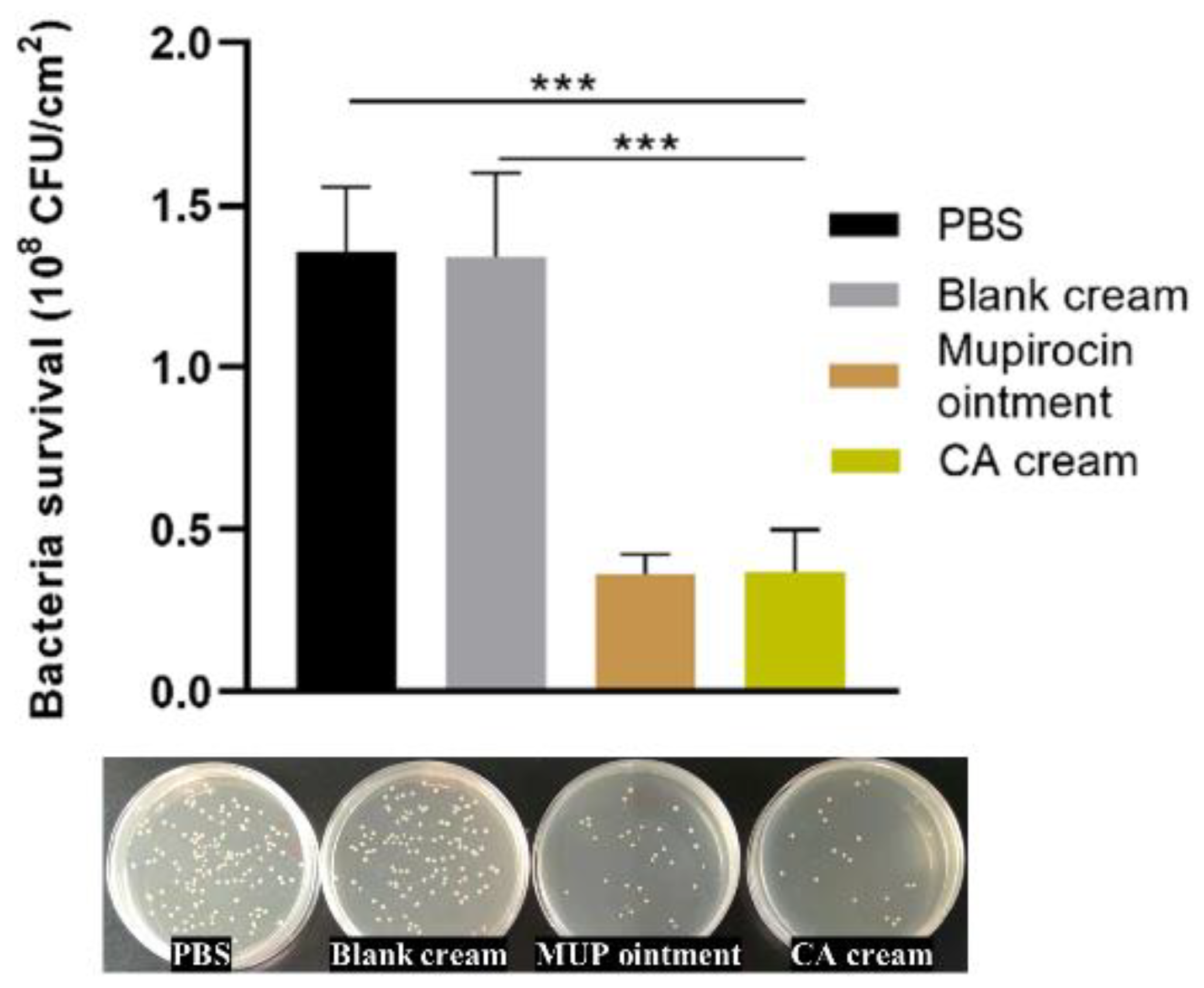
3.6. In Vivo Antibacterial Activity Evaluation of Chrysomycin A Cream
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lake, J.G.; Weiner, L.M.; Milstone, A.M. Pathogen Distribution and Antimicrobial Resistance Among Pediatric Healthcare-Associated Infections Reported to the National Healthcare Safety Network, 2011. Infect. Control Hosp. Epidemiol. 2018, 39(1), 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jevons, M.P. “Celbenin”-Resistant Staphylococcus. Br. Med. J. 1961, 1, 124–125. [Google Scholar] [CrossRef]
- Boswihi, S.S.; Udo, E.E. Methicillin-resistant Staphylococcus aureus: An update on the epidemiology, treatment options and infection control. Curr. Med. Res. Pract. 2018, 8, 18–24. [Google Scholar] [CrossRef]
- Talon, D.; Woronoff-Lemsi, M.C.; Limat, S. The impact of resistance to methicillin in Staphylococcus aureus bacteremia on mortality. Eur. J. Intern. Med. 2002, 13, 31–36. [Google Scholar] [CrossRef]
- Chang, L.; Liu, J. Antimicrobial treatment of Staphylococcus aureus infection in skin and soft tissue. Health Prot. Promot. 2016, 16, 60. [Google Scholar]
- Munckhof, W.J.; Schooneveldt, J.; Coombs, G.W. Emergence of community-acquired methicillin-resistant Staphylococcus aureus (MRSA) infection in Queensland, Australia. Int. J. Infect. Dis. 2003, 7, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Whitby, M. Fusidic acid in the treatment of methicillin-resistant Staphylococcus aureus. Int. J. Antimicrob. Agents 1999, 12 (Suppl. 2), S67–S71. [Google Scholar] [CrossRef]
- Rodvold, K.A.; McConeghy, K.W. Methicillin-resistant Staphylococcus aureus therapy: Past, present, and future. Clin. Infect. Dis. 2014, 58 (Suppl. 1), S20–S27. [Google Scholar] [CrossRef]
- Ullah, K.; Khan, S.A.; Mannan, A. Enhancing the Antibacterial Activity of Erythromycin with Titanium Dioxide Nanoparticles against MRSA. Curr. Pharm. Biotechnol. 2020, 21, 948–954. [Google Scholar] [CrossRef]
- Choo, E.J.; Chambers, H.F. Treatment of Methicillin-Resistant Staphylococcus aureus Bacteremia. Infect. Chemother. 2016, 48, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Roch, M.; Gagetti, P.; Davis, J. Daptomycin Resistance in Clinical MRSA Strains Is Associated with a High Biological Fitness Cost. Front. Microbiol. 2017, 8, 2303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strelitz, F.; Flon, H.; Asheshov, I.N. Chrysomysin: A new antibiotic substance for bacterial viruses. J. Bacteriol. 1955, 69, 280–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, U.; Yoshihira, K.; Highet, R.J. The Chemistry of the Antibiotics Chrysomycin A and B. Antitumor activity of chrysomycin A. J. Antibiot. 1982, 35, 1194–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.; Zheng, S.; Gao, X. Mechanochemical preparation of chrysomycin A self-micelle solid dispersion with improved solubility and enhanced oral bioavailability. J. Nanobiotechnol. 2021, 19, 164. [Google Scholar] [CrossRef]
- Balaji, M.; Dan, V.M.; Vinodh, J.S. Anti-microbial activity of chrysomycin A produced by Streptomyces sp. against Mycobacterium tuberculosis. RSC Adv. 2017, 7, 36335–36339. [Google Scholar] [CrossRef] [Green Version]
- Waghule, T.; Singhvi, G.; Dubey, S.K. Microneedles: A smart approach and increasing potential for transdermal drug delivery system. Biomed. Pharm. 2019, 109, 1249–1258. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef]
- Ni, H.; Lv, S.; Sheng, Y. Optimization of fermentation conditions and medium compositions for the production of chrysomycin a by a marine-derived strain Streptomyces sp. Prep. Biochem. Biotechnol. 2021, 51, 998–1003. [Google Scholar] [CrossRef]
- Tam, V.H.; Schilling, A.N.; Neshat, S. Optimization of meropenem minimum concentration/MIC ratio to suppress in vitro resistance of Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2005, 49, 4920–4927. [Google Scholar] [CrossRef] [Green Version]
- Long, S.S.; Prober, C.G.; Fischer, M. Principles and Practice of Pediatric Infectious Diseases, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1422–1434. [Google Scholar]
- Hu, J.; Quan, Y.; Lai, Y. A smart aminoglycoside hydrogel with tunable gel degradation, on-demand drug release, and high antibacterial activity. J. Control Release 2017, 247, 145–152. [Google Scholar] [CrossRef]
- Ferrer International, S.A. Pharmaceutical Topical Compositions. U.S. Patent 9,180,200, B2, 10 November 2015. [Google Scholar]
- Bouguéon, G.; Lagarce, F.; Martin, L. Formulation and characterization of a 0.1% rapamycin cream for the treatment of Tuberous Sclerosis Complex-related angiofibromas. Int. J. Pharm. 2016, 509, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Shandong Xinhua Pharm. Co., Ltd. Elofesalamide Ointment and Its Preparation Process. CN Patent 102,793,660 B, 2 July 2014. [Google Scholar]
- Il Yang Pharm. Co., Ltd. Antifungal Composition for External Use Containing Fluconazole Having Improved Skin Permeability and Stability and Causing No Side-Effects. KOR Patent 2,006,066,780 A, 19 June 2006. [Google Scholar]
- Guan, Y.; Gao, Q.; Jiang, J. Assessment of transdermal absorption for etofesalamide self-emulsion-base cream. Chin. J. New Drugs 2006, 15, 1766–1768. [Google Scholar] [CrossRef]
- Józsa, L.; Ujhelyi, Z.; Vasvári, G. Formulation of Creams Containing Spirulina Platensis Powder with Different Nonionic Surfactants for the Treatment of Acne Vulgaris. Molecules 2020, 25, 4856. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Peng, Q.; Shi, S. Preparation, characterization, and in vivo evaluation of a self-nanoemulsifying drug delivery system (SNEDDS) loaded with morin-phospholipid complex. Int. J. Nanomed. 2011, 6, 3405–3414. [Google Scholar] [CrossRef] [Green Version]
- Lei, Y.; Lu, Y.; Qi, J. Solid self-nanoemulsifying cyclosporin A pellets prepared by fluid-bed coating: Preparation, characterization and in vitro redispersibility. Int. J. Pharm. 2011, 6, 795–805. [Google Scholar] [CrossRef] [Green Version]
- Balakrishnan, P.; Lee, B.J.; Oh, D.H. Enhanced oral bioavailability of dexibuprofen by a novel solid self-emulsifying drug delivery system (SEDDS). Eur. J. Pharm. Biopharm. 2009, 72, 539–545. [Google Scholar] [CrossRef]
- Tao, Y.; Bu, C.; Zou, L. A comprehensive review on microbial production of 1,2-propanediol: Micro-organisms, metabolic pathways, and metabolic engineering. Biotechnol. Biofuels 2021, 14, 216. [Google Scholar] [CrossRef]
- Zeng, X. Use of Chitosan-Amino Acid Gel Thickening Emollient Useful in Face Cream, Comprises E.G.Polyquaternium-10 Conditioner, Allantoin, Citric Acid, Chelating Agent, Emollient, Skin Conditioner, Humectant, Emulsion Stabilizer and Preservatives. CHN Patent 111,358,712 A, 3 July 2020. [Google Scholar]
- Joye, I.J. Encyclopedia of Food Chemistry, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–9. [Google Scholar]
- Brul, S.; Coote, P. Preservative agents in foods: Mode of action and microbial resistance mechanisms. Int. J. Food Microbiol. 1999, 50(1-2), 1–17. [Google Scholar] [CrossRef]
- Wei, T.T.; Byrne, K.M.; Warnick-Pickle, D. Studies on the mechanism of actin of gilvocarcin V and chrysomycin A. J. Antibiot. 1982, 35, 545–548. [Google Scholar] [CrossRef] [Green Version]
- Muralikrishnan, B.; Edison, L.K.; Dusthackeer, A. Chrysomycin A inhibits the topoisomerase I of Mycobacterium tuberculosis. J. Antibiot. 2022, 75, 226–235. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | A: Tefose® 63 (%) | B: Labrifil® M 1944 CS (%) | C: 2-(2-Ethoxyethoxy) Ethanol (%) | D: 1-Octadecanol (%) |
|---|---|---|---|---|
| 1 | 15 | 10 | 5 | 1 |
| 2 | 20 | 15 | 10 | 5 |
| 3 | 25 | 20 | 15 | 10 |
| Level | A: Tefose® 63 (%) | B: Labrifil® M 1944 CS (%) | C: 2-(2-Ethoxyethoxy) Ethanol (%) | D: 1-Octadecanol (%) |
|---|---|---|---|---|
| 1 | 13 | 6 | 5 | 5 |
| 2 | 14 | 7 | 7 | 7 |
| 3 | 15 | 8 | 9 | 9 |
| No. | Stability | Spreading | Appearance | A: Tefose® 63 (%) | B: Labrifil® M 1944 CS (%) | C: 2-(2-Ethoxyethoxy) Ethanol (%) | D: 1-Octadecanol (%) |
|---|---|---|---|---|---|---|---|
| 1 | 10 | 8 | 9 | 13 | 6 | 5 | 5 |
| 2 | 9 | 8 | 6 | 13 | 7 | 7 | 7 |
| 3 | 10 | 5 | 6 | 13 | 8 | 9 | 9 |
| 4 | 7 | 4 | 6 | 14 | 6 | 7 | 9 |
| 5 | 8 | 8 | 8 | 14 | 7 | 9 | 5 |
| 6 | 9 | 6 | 8 | 14 | 8 | 5 | 7 |
| 7 | 7 | 4 | 7 | 15 | 6 | 9 | 7 |
| 8 | 7 | 5 | 5 | 15 | 7 | 5 | 9 |
| 9 | 7 | 9 | 9 | 15 | 8 | 7 | 5 |
| Stability | I j | 29 | 16 | 26 | 25 | ||
| II j | 24 | 25 | 23 | 25 | |||
| III j | 21 | 26 | 25 | 24 | |||
| Ī j | 9.667 | 5.333 | 8.667 | 8.333 | |||
| ĪĪ j | 8 | 8.333 | 7.667 | 8.333 | |||
| ĪĪĪ j | 7 | 8.667 | 8.333 | 8 | |||
| R j | 2.667 | 3.333 | 1 | 0.333 | |||
| Spreading | I j | 21 | 16 | 19 | 25 | ||
| II j | 18 | 21 | 21 | 18 | |||
| III j | 18 | 20 | 17 | 14 | |||
| Ī j | 7 | 5.333 | 6.333 | 8.333 | |||
| ĪĪ j | 6 | 7 | 7 | 6 | |||
| ĪĪĪ j | 6 | 6.667 | 5.667 | 4.667 | |||
| R j | 1 | 1.667 | 1.333 | 3.667 | |||
| Appearance | I j | 21 | 22 | 22 | 26 | ||
| II j | 22 | 19 | 21 | 21 | |||
| III j | 21 | 23 | 21 | 17 | |||
| Ī j | 7 | 7.333 | 7.333 | 8.667 | |||
| ĪĪ j | 7.333 | 6.333 | 7 | 7 | |||
| ĪĪĪ j | 7 | 7.667 | 7 | 5.667 | |||
| R j | 0.333 | 1.333 | 0.333 | 3 |
| Purposes | Components | Dosage |
|---|---|---|
| Effective drug | Chrysomycin A | 1% |
| Emulsifier | Tefose® 63 | 13% |
| Cosurfactant | Labrifil® M 1944 CS | 8% |
| Solvent | 2-(2-Ethoxyethoxy) ethanol | 5% |
| Thickener | 1-Octadecanol | 5% |
| Preservative | Benzoic acid | 0.1% |
| Humectant | 1,2-Propanediol | 10% |
| Water phase | Purified water | 57.9% (up to 100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.; Cai, Y.; Chu, Y.; Yu, X.; Song, F.; Wang, H.; Zhang, H.; Sun, X. Formulation of Chrysomycin A Cream for the Treatment of Skin Infections. Molecules 2022, 27, 4613. https://doi.org/10.3390/molecules27144613
Liu H, Cai Y, Chu Y, Yu X, Song F, Wang H, Zhang H, Sun X. Formulation of Chrysomycin A Cream for the Treatment of Skin Infections. Molecules. 2022; 27(14):4613. https://doi.org/10.3390/molecules27144613
Chicago/Turabian StyleLiu, Haohua, Yue Cai, Yuteng Chu, Xiaojie Yu, Fuhang Song, Hong Wang, Huawei Zhang, and Xuanrong Sun. 2022. "Formulation of Chrysomycin A Cream for the Treatment of Skin Infections" Molecules 27, no. 14: 4613. https://doi.org/10.3390/molecules27144613
APA StyleLiu, H., Cai, Y., Chu, Y., Yu, X., Song, F., Wang, H., Zhang, H., & Sun, X. (2022). Formulation of Chrysomycin A Cream for the Treatment of Skin Infections. Molecules, 27(14), 4613. https://doi.org/10.3390/molecules27144613