
Exploring the Potential of Natural Product-Based Nanomedicine for Maintaining Oral Health

 , , , and
, , , and
Abstract
:1. Introduction
2. Herbal Remedies for Dental Diseases
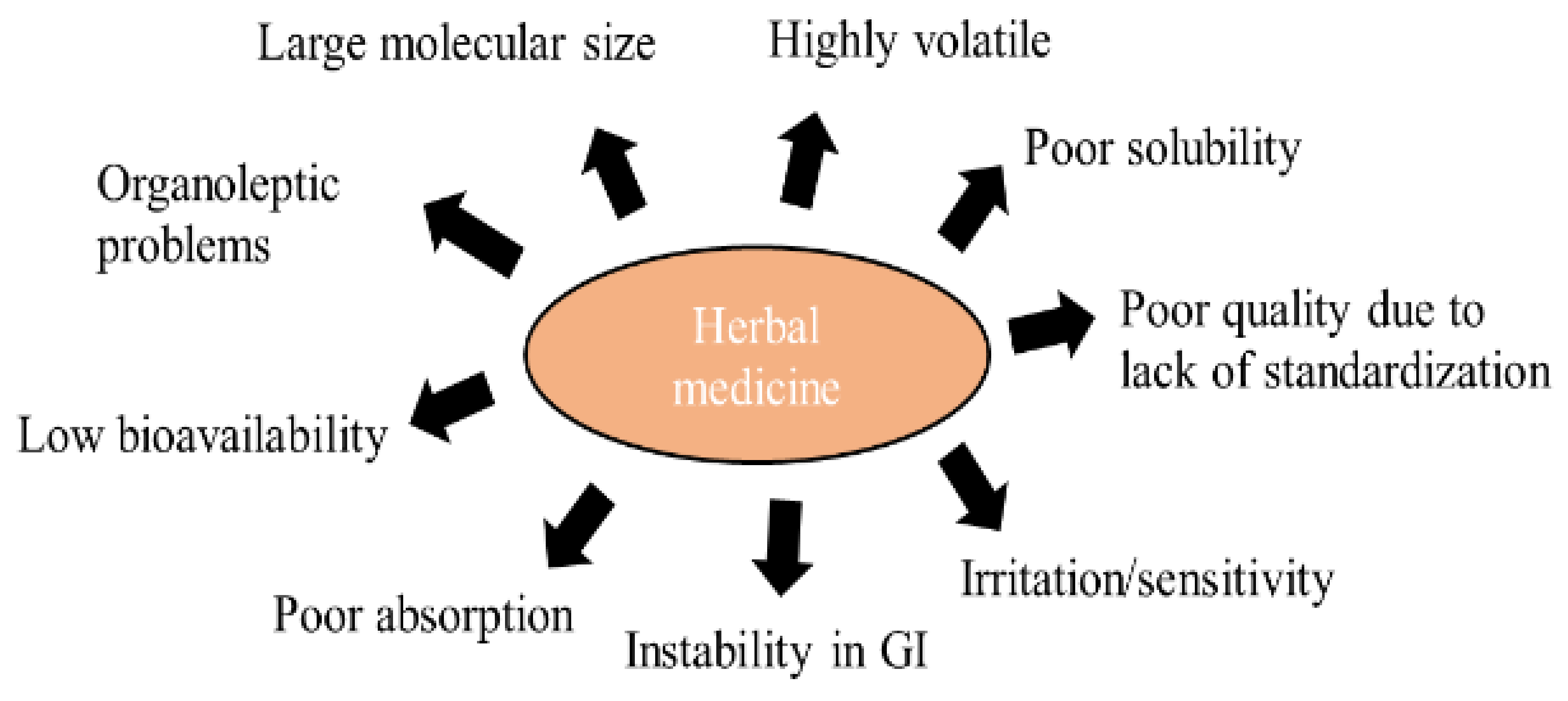
3. Challenges of Herbal Therapies
3.1. Safety Issues with Herbal Products
3.2. Patient Acceptance
3.3. Poor Bioavailability
3.4. Long Duration of Treatment
3.5. Lack of Harmonized Regulations
4. Nanotechnology in Herbal Dentistry
4.1. Nanotechnology to Enhance Solubility of Natural Bioactives
4.2. Nanotechnology to Enhance Permeability of Natural Bioactives
4.3. Nanotechnology to Enhance the Therapeutic Performance of Natural Products
5. Role of Nano-Herbal Technology in Biofilm Resistance
6. Synergistic Combinations of Phytoconstituents and Drugs in Nanotechnology
7. Regulatory and Commercial Manufacturing Challenges
- Availability of consistent quality raw material—Raw materials grown in different geographical conditions show different quality characteristics;
- Contamination with toxic or unwanted medicinal plants and/or plant parts is always present as, generally, the irrigation, collection, and supply chain are not well controlled;
- QC methods employed for herbal products are different from other conventional products, so specific expertise is required.
| IS 6356 (2001) | Toothpaste specification |
| AS 2827:1982 | Toothpaste specification |
| SABS 1302:1980 | Toothpaste specification |
| 1S0 11609:1995 (E) | Dentistry—Toothpaste requirements, test methods, and marking |
| BS 5136:1981 S | Toothpaste specification |
| SLS 275:1980 | Toothpaste specification |
| BDS 1216:1989 | Toothpaste specification |
- Fineness;
- pH of aqueous suspension;
- Heavy metal quantification (lead and arsenic);
- Foaming power;
- Fluoride quantification;
- Microbial counts (total viable counts and Gram-negative pathogens).
8. Patent Analysis
9. Future Prospects of Herbal and Essential Oil-Based Formulations in the Treatment of Dental Diseases
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mosaddad, S.A.; Tahmasebi, E.; Yazdanian, A.; Rezvani, M.B.; Seifalian, A.; Yazdanian, M.; Tebyanian, H. Oral Microbial Biofilms: An Update. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2005–2019. [Google Scholar] [CrossRef]
- Kidd, E.A.; Fejerskov, O. Essentials of Dental Caries, 4th ed.; Oxford University Press: Oxford, UK, 2016; pp. 373–378. [Google Scholar]
- Komal, Z.; Rajan, J.S.; Khan, S.Q.; Siddiqui, T. Effect of Dietary and Oral Hygiene Pattern on Incidence of Dental Caries among a Population from Riyadh, Saudi Arabia. Ann. Jinnah Sindh Med. Univ. 2018, 4, 30–40. [Google Scholar]
- Schroth, R.J.; Levi, J.A.; Sellers, E.A.; Friel, J.; Kliewer, E.; Moffatt, M.E. Vitamin D Status of Children with Severe Early Childhood Caries: A Case-Control Study. BMC Paediatr. 2013, 13, 174. [Google Scholar] [CrossRef] [Green Version]
- Turner, B. Putting Ireland’s Health Spending into Perspective. Lancet 2018, 391, 833–834. [Google Scholar] [CrossRef] [Green Version]
- Tungare, S.; Paranjpe, A.G. Diet and Nutrition to Prevent Dental Problems. [Updated 11 August 2021]; In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hujoel, P.P.; Lingström, P. Nutrition, Dental Caries and Periodontal Disease: A Narrative Review. J. Clin. Periodontol. 2017, 44, S79–S84. [Google Scholar] [CrossRef] [Green Version]
- Ferreira de Oliveira, M.A.F.; Celeste, R.K.; Rodrigues, C.C.R.; Marinho, V.C.C.; Walsh, T. Topical Fluoride for Treating Dental Caries. Cochrane Database Syst. Rev. 2018, 2, CD003454. [Google Scholar] [CrossRef] [Green Version]
- Bodiba, D.; Szuman, K.M.; Lall, N. Medicinal Plants for Holististic Health and Well-Being; Elsevier Inc.: New York, NY, USA, 2018; pp. 183–212. [Google Scholar] [CrossRef]
- Porter, S.R.; Scully, C. Oral malodour (halitosis). BMJ 2006, 333, 632–635. [Google Scholar] [CrossRef] [Green Version]
- Thakar, V.J. Historical Development of Basic Concepts of Ayurveda from Veda up to Samhita. Ayurveda 2010, 31, 400–402. [Google Scholar] [CrossRef]
- Shanbhag, V.K. Oil Pulling for Maintaining Oral Hygiene—A review. J. Tradit. Complement. Med. 2016, 7, 106–109. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, V.F.; Angelo, C.P.A. Fitoterapia No Mundo Atual [Phytotherapy in the World Today]. Quím. Nova 2010, 33, 1829. [Google Scholar] [CrossRef]
- Ekor, M. The Growing Use of Herbal Medicines: Issues Relating to Adverse Reactions and Challenges in Monitoring Safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borges, R.S.; Keita, H.; Ortiz, B.; Dos Santos Sampaio, T.I.; Ferreira, I.M.; Lima, E.S.; de Jesus Amazonas da Silva, M.; Fernandes, C.P.; de Faria Mota Oliveira, A.; Cardoso da Ceiceiçäo, E.; et al. Anti-Inflammatory Activity of Nanoemulsions of Essential Oil from Rosmarinus Officinalis L.: In Vitro and in Zebra fish Studies. Inflammopharmacology 2018, 26, 1057–1080. [Google Scholar] [CrossRef] [PubMed]
- Benatti, F.B.; Pedersen, B.K. Exerciseas an Anti-Inflammatory Therapy for Rheumatic Diseases-Myokine Regulation. Nat. Rev. Rheumatol. 2015, 11, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Ogunwande, I.A.; Avoseh, O.N.; Olasunkanmi, K.N.; Lawal, O.A.; Ascrizzi, R.; Flamini, G. Chemical Composition, Anti-Nociceptive and Anti-Inflammatory Activities of Essential Oil of Bougainvillea Glabra. J. Ethnopharmacol. 2018, 232, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, R. Effect of Antioxidant Gel on Oxidative Stress and Salivary Flow Rate in Xerostomic Patients. Master’s Thesis, Texas A & M University, College Station, TX, USA, May 2017. [Google Scholar]
- Carbone, C.; Martins-Gomes, C.; Caddeo, C.; Silva, A.M.; Musumeci, T.; Pignatello, R.; Puglisi, G.; Souto, E.B. Mediterranean Essential Oils as Precious Matrix Components and Active Ingredients of Lipid Nanoparticles. Int. J. Pharm. 2018, 548, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Nimbulkar, G.; Garacha, V.; Shetty, V.; Bhor, K.; Srivastava, K.C.; Shrivastava, D.; Sghaireen, M.G. Microbiological and Clinical Evaluation of Neem Gel and Chlorhexidine Gel on Dental Plaque and Gingivitis in 20–30 Years Old Adults: A Randomized Parallel-Armed, Double-Blinded Controlled Trial. J. Pharm. Bioallied Sci. 2020, 12, S345–S351. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, J.; Balagopal, S.; Priya, M.S.; Selvi, S.; Senthil kumar, M. Evaluation of Antimicrobial Efficacy of Triphala (an Indian Ayurvedic Herbal Formulation) and 0.2% Chlorhexidine against Streptococcus Mutans Biofilm Formed on Tooth Substrate: An in Vitro Study. Indian J. Dent. Res. 2014, 25, 475–479. [Google Scholar] [CrossRef]
- Thomas, A.; Sneha, T.; Sanjana, M. Comparison of the Antimicrobial Efficacy of Chlorhexidine, Sodium Fluoride, Fluoride with Essential Oils, Alum, Green Tea, and Garlic with Lime Mouth Rinses on Cariogenic Microbes. J. Int. Soc. Prev. Commun. Dent. 2015, 5, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Mohankumar, K.P.; Priya, N.K.; Madhushankari, G.S. Anticariogenic Efficacy of Herbal and Conventional Toothpastes—A Comparative In-Vitro Study. J. Int. Oral Health 2013, 5, 8–13. [Google Scholar]
- Harput, U.S. Herbal products for oral hygiene: An overview of their biological activities. In Natural Oral Care in Dental Therapy; Chauhan, D.N., Singh, P.R., Shah, K., Chauhan, N.S., Eds.; Wiley: Hoboken, NJ, USA, 2020; pp. 31–44. [Google Scholar] [CrossRef]
- Cimino, C.; Maurel, O.M.; Musumeci, T.; Bonaccorso, A.; Drago, F.; Souto, E.; Pignatello, R.; Carbone, C. Essential Oils: Pharmaceutical Applications and Encapsulation Strategies into Lipid-Based Delivery Systems. Pharmaceutics 2021, 13, 327. [Google Scholar] [CrossRef]
- Dobler, D.; Runkel, F.; Schmidts, T. Effect of Essential Oils on Oral Halitosis Treatment: A Review. Eur. J. Oral Sci. 2020, 128, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Janakiram, C.; Venkitachalam, R.; Fontelo, P.; Iafolla, T.J.; Dye, B.A. Effectiveness of Herbal Oral Care Products in Reducing Dental Plaque & Gingivitis—A systematic review and meta-analysis. BMC Complement. Med. Ther. 2020, 20, 43. [Google Scholar] [CrossRef]
- Karygianni, L.; Al-Ahmad, A.; Argyropoulou, A.; Hellwig, E.; Anderson, A.C.; Skaltsounis, A.L. Natural Antimicrobials and Oral Microorganisms: A Systematic Review on Herbal Interventions for the Eradication of Multispecies Oral Biofilms. Front. Microbiol. 2015, 6, 1529. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, K.; Amaechi, B.T. Antimicrobial Effect of Herbal Extract of Acacia Arabica with Triphala on the Biofilm Forming Cariogenic Microorganisms. J. Ayurvedic Integr. Med. 2020, 11, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Juache, A.; Aranda-Romo, S.; Bermeo-Escalona, J.R.; Gómez-Hernández, A.; Pozos-Guillén, A.; Sánchez-Vargas, L.O. The Essential Oil of Allium sativum as an Alternative Agent against Candida isolated from Dental Prostheses. Rev. Iberoam. Micol. 2017, 34, 158–164. [Google Scholar] [CrossRef]
- Oliveira, M.; Borges, A.C.; Brighenti, F.L.; Salvador, M.J.; Gontijo, A.; Koga-Ito, C.Y. Cymbopogon citratus essential oil: Effectonpoly microbialcaries-related biofilm with low cytotoxicity. Braz. Oral Res. 2017, 31, 89. [Google Scholar] [CrossRef] [Green Version]
- Chaveli-López, B. Oral Toxicity Produced by Chemotherapy: A systematic review. J. Clin. Exp. Dent. 2014, 6, e81–e90. [Google Scholar] [CrossRef] [Green Version]
- Elaguel, A.; Kallel, I.; Gargouri, B.; Amor, I.B.; Hadrich, B.; Messaoud, E.B.; Gdoura, R.G.; Lassoued, S.; Gargouri, A. Lawsonia Inermis Essential Oil: Extraction Optimization by RSM, Antioxidant Activity, Lipid Peroxydation and Antiproliferative Effects. Lipids Health Dis. 2019, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.H.; Chou, Y.R.; Deng, Y.H.; Huang, M.S.; Chien, S.T.; Quynh, B.; Wu, C.Y.; Achtmann, E.A.P.; Cheng, H.C.; Dubey, N.K.; et al. The Novel Herbal Cocktail AGA Alleviates Oral Cancer through Inducing Apoptosis, Inhibited Migration and Promotion of Cell Cycle Arrest at Sub G1 Phase. Cancers 2020, 12, 3214. [Google Scholar] [CrossRef]
- Willenbacher, E.; Khan, S.Z.; Mujica, S.; Trapani, D.; Hussain, S.; Wolf, D.; Willenbacher, W.; Spizzo, G.; Seeber, A. Curcumin: New Insights into an Ancient Ingredient against Cancer. Int. J. Mol. Sci. 2019, 20, 1808. [Google Scholar] [CrossRef] [Green Version]
- Anuchapreeda, S.; Thanarattanakorn, P.; Sittipreechacharn, S.; Chanarat, P.; Limtrakul, P. Curcumin inhibits WT1 gene expression in human leukemic K562 cells. Acta Pharmacol. Sin. 2006, 27, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.D.; Kim, J.Y. Essential Oil from Cryptomeria japonica induces Apoptosis in Humanoral Epidermoid Carcinoma Cells via Mitochondrial Stress and Activation of Caspases. Molecules 2012, 17, 3890–3901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fekrazad, R.; Afzali, M.; Aliabadi-Pasban, H.; Esmaeili-Mahani, S.; Aminizadeh, M.; Mostafavi, A. Cytotoxic Effect of Thymus caramanicus Jalas on Human Oral Epidermoid Carcinoma KB Cells. Braz. Dent. J. 2017, 28, 72–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, T.Q.; Felisberto, J.; Guimarães, E.F.; Queiroz, G.A.; Fonseca, A.; Ramos, Y.J.; Marques, A.M.; Moreira, D.L.; Robbs, B.K. Apoptotic Effect of β-pinene on Oral Squamous Cell Carcinomaas one of the Major Compounds from Essential Oil of Medicinal Plant Piper rivinoides Kunth. Nat. Prod. Res. 2021, 1–5. [Google Scholar] [CrossRef]
- Ohnishi, S.; Takeda, H. Herbal Medicines for the Treatment of Cancer Chemotherapy-induced Side Effects. Front. Pharmacol. 2015, 6, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd El-Kalek, H.H.; Mohamed, E.A. Synergistic Effect of Certain Medicinal Plants and Amoxicillin against Some Clinical Isolates of Methicillin—Resistant Staphylococcus Aureus (MRSA). Int. J. Pharm. Appl. 2012, 3, 976–2639. Available online: http://www.bipublication.com (accessed on 28 August 2021).
- Shekar, B.R.C.; Nagarajappa, R.; Suma, S.; Thakur, R. Herbal Extracts in Oral Healthcare—A Review of the Current Scenario and its Future Needs. Pharmacogn. Rev. 2015, 9, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Joshi, S.G.; Shettar, L.G.; Agnihotri, P.S.; Acharya, A.; Thakur, S.L. Solanum Xanthocarpum and Acacia Catechu Willd-An Ayurvedic Soothe: A Randomized Clinical Trial. J. Ayurvedic Herb. Med. 2021, 7, 1–4. Available online: www.ayurvedjournal.com (accessed on 28 August 2021). [CrossRef]
- Baena-Santillán, E.S.; Piloni-Martini, J.; Santos-López, E.M.; Gómez-Aldapa, C.A.; Rangel-Vargas, E.; Castro-Rosas, J. Comparison of the Antimicrobial Activity of Hibiscus Sabdariffa Calyx Extracts, Six Commercial Types of Mouthwashes, and Chlorhexidine on Oral Pathogenic Bacteria, and the Effect of Hibiscus Sabdariffa Extracts and Chlorhexidine on Permeability of the Bacterial Membrane. J. Med. Food 2021, 24, 67–76. [Google Scholar] [CrossRef]
- Arunachalam, L.T.; Sudhakar, U.; Vasanth, J.; Khumukchum, S.; Selvam, V.V. Comparison of Anti-Plaque and Anti-Gingivitis Effect of Curcumin and Chlorhexidine Mouth Rinse in the Treatment of Gingivitis: A Clinical and Biochemical Study. J. Indian Soc. Periodontol. 2017, 21, 478–483. [Google Scholar] [CrossRef]
- Jeong, Y.-J.; Choi, J.-S. Antimicrobial Effect of Cinnamon Oil Against Oral Microorganisms. Med. Leg. Update 2020, 20, 1591–1594. [Google Scholar] [CrossRef]
- Cunha, B.G.; Duque, C.; Sampaio Caiaffa, K.; Massunari, L.; Araguê Catanoze, I.; Dos Santos, D.M.; de Oliveira, S.; Guiotti, A.M. Cytotoxicity and Antimicrobial Effects of Citronella Oil (Cymbopogon Nardus) and Commercial Mouthwashes on S. Aureus and C. Albicans Biofilms in Prosthetic Materials. Arch. Oral Biol. 2020, 109, 104577. [Google Scholar] [CrossRef] [PubMed]
- Ragul, P.; Dhanraj, M.; Jain, A.R. Efficacy of Eucalyptus Oil over Chlorhexidine Mouthwash in Dental Practice. Drug Invent. Today 2018, 10, 638–641. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01920139/full (accessed on 28 August 2021).
- Khirtika, S.G.; Ramesh, S.; Muralidharan, N.P. Comparative Evaluation of Antimicrobial Efficacy of 0.2% Chlorhexidine, 2% Iodine and Homemade Mouthrinse as an Anti-Caries Agent-A Clinical Study. J. Pharm. Sci. Res. 2017, 9, 2114–2116. Available online: https://www.researchgate.net/publication/321889363 (accessed on 28 August 2021).
- Rasaie, N.; Esfandiari, E.; Rasouli, S.; Abdolahian, F. Antimicrobial Effect of Myrtus Communis L. Essential Oils Against Oral Microorganism. Jentashapir J. Health Res. 2018, 9, e12032. Available online: https://sites.kowsarpub.com/jjcmb/articles/12032.html (accessed on 28 August 2021).
- Dadpe, M.V.; Dhore, S.V.; Dahake, P.T.; Kale, Y.J.; Kendre, S.B.; Siddiqui, A.G. Evaluation of Antimicrobial Efficacy of Trachyspermum Ammi (Ajwain) Oil and Chlorhexidine against Oral Bacteria: An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 357–363. [Google Scholar] [CrossRef]
- Qiu, Y.; Li, C.; Wang, Q.; Zeng, X.; Ji, P. Tanshinone IIA induces cell death via Beclin-1-dependent autophagy in oral squamous cell carcinoma SCC-9 cell line. Cancer Med. 2018, 7, 397–407. [Google Scholar] [CrossRef]
- Zheng, L.W.; Hua, H.; Cheung, L.K. Traditional Chinese medicine and oral diseases: Today and tomorrow. Oral Dis. 2011, 17, 7–12. [Google Scholar] [CrossRef]
- Luo, D.; Tu, Z.; Yin, W.; Fan, C.; Chen, N.; Wu, Z.; Ding, W.; Li, Y.; Wang, G.; Zhang, Y. Uncommon Bis-Amide Matrine-type Alkaloids from Sophoraal opecuroides with Anti-inflammatory Effects. Front. Chem. 2021, 9, 740421. [Google Scholar] [CrossRef]
- Hulan, U.; Bazarragchaa, T.; Nishimura, M.; Shimono, T. Invitro antibacterial effects of the crude extracts of Sophoraal opecuroides against oral microorganisms. Pediatric Dent. J. 2004, 14, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Helmy, H.; Darwish, Z.; El-Sheikh, S.; Afifi, M. The Therapeutic Effect of Camptothecin in Induced Oral Squamous Cell Carcinoma (experimental study). Alex. Dent. J. 2018, 43, 76–80. [Google Scholar] [CrossRef]
- Kang, M.H.; Lee, S.J.; Lee, M.H. Bone Remodeling Effects of Korean Red Ginseng extracts for Dental Implant Applications. J. Ginseng Res. 2020, 44, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Gupta, L.M.; Raina, R. Side Effects of Some Medicinal Plants. Curr. Sci. 1998, 75, 897–900. Available online: https://www.jstor.org/stable/24101663 (accessed on 28 August 2021).
- Santamaria, M., Jr.; Petermann, K.D.; Vedovello, S.A.; Degan, V.; Lucato, A.; Franzini, C.M. Antimicrobial Effect of Melaleuca Alternifolia Dental Gel in Orthodontic Patients. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Groppo, F.C.; Ramacciato, J.C.; Simões, R.P.; Flório, F.M.; Sartoratto, A. Antimicrobial Activity of Garlic, Tea Tree Oil, and Chlorhexidine against Oral Microorganisms. Int. Dent. J. 2002, 52, 433–437. [Google Scholar] [CrossRef]
- Squier, C.A. The Permeability of Oral Mucosa. Crit. Rev. Oral Biol. Med. 1991, 2, 13–32. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, I.; Zhang, M.; Pang, Y.; Li, Z.; Zhao, A.; Feng, J. Self-emulsifying drug delivery system and the applications in herbal drugs. Drug Deliv. 2015, 22, 475–486. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.L.; Wang, H.; Zhang, J.; Weimin, W.; Wang, H.; Wang, Y.C.; Zhang, Q. Microencapsulation of Radix Salvia Miltiorrhiza Nanoparticles by Spray-Drying. Powder Technol. 2008, 184, 114–121. [Google Scholar] [CrossRef]
- Kohlert, C.; Schindler, G.; März, R.W.; Abel, G.; Brinkhaus, B.; Derendorf, H.; Gräfe, E.U.; Veit, M. Systemic Availability and Pharmacokinetics of Thymol in Humans. J. Clin. Pharmacol. 2002, 42, 731–737. [Google Scholar] [CrossRef]
- Mukherjee, K.P.; Harwansh, R.K.; Bhattacharyya, S. Evidence Based Validation of Herbal Medicine; Elsevier Inc.: New York, NY, USA, 2015; pp. 217–245. [Google Scholar] [CrossRef]
- Calixto, J.B. Efficacy, Safety, Quality Control, Marketing and Regulatory Guidelines for Herbal Medicines (Phytotherapeutic Agents). Braz. J. Med. Biol. Res. 2000, 33, 179–189. [Google Scholar] [CrossRef]
- Schweiggert, U.; Carle, R.; Schieber, A. Conventional and alternative processes for spice production—A review. Trends Food Sci. Technol. 2007, 18, 260–268. [Google Scholar] [CrossRef]
- Khogta, S.; Patel, J.; Barve, K.; Londhe, V. Herbal Nano-Formulations for Topical Delivery. J. Herb. Med. 2020, 20, 100300. [Google Scholar] [CrossRef]
- Löbenberg, R.; Amidon, G.L. Modern Bioavailability, Bioequivalence and Biopharmaceutics Classification System. New Scientific Approaches to International Regulatory Standards. Eur. J. Pharm. Biopharm. 2000, 50, 3–12. [Google Scholar] [CrossRef]
- Malekzadeh, M.; Kia, S.J.; Mashaei, L.; Moosavi, M.-S. Oral nano-curcumin on gingival inflammation in patients with gingivitis and mild periodontitis. Clin. Exp. Dent. Res. 2021, 7, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Md, S.; Kit, B.C.M.; Jagdish, S.; David, D.J.; Pandey, M.; Chatterjee, L.A. Development and In Vitro Evaluation of a Zerumbone Loaded Nanosuspension Drug Delivery System. Crystals 2018, 8, 286. [Google Scholar] [CrossRef] [Green Version]
- Eid, E.E.M.; Abdul, A.B.; Suliman, F.O.; Sukari, M.A.; Abdulla, S.; Fatah, S.S. Characterization of the inclusion complex of zerumbone with hydroxypropyl-β-cyclodextrin. Carbohydr. Polym. 2013, 83, 1707–1714. [Google Scholar] [CrossRef]
- Onoue, S.; Takahashi, H.; Kawabata, Y.; Seto, Y.; Hatanaka, J.; Timmermann, B.; Yamada, S. Formulation Design and Photochemical Studies on Nanocrystal Solid Dispersion of Curcumin with Improved Oral Bioavailability. J. Pharm. Sci. 2010, 99, 1871–1881. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Wu, C.L.; Liu, C.W.; Chuo, W.H.; Li, P.C.; Tsai, T.R. Preparation, Characterization and Cytotoxicity Evaluation of Tanshinone IIA Nanoemulsions. J. Biomed. Nanotechnol. 2011, 7, 558–567. [Google Scholar] [CrossRef]
- Sahibzada, M.U.K.; Sadiq, A.; Faidah, H.S.; Khurram, M.; Amin, M.U.; Haseeb, A.; Kakar, M. Berberine Nanoparticles with Enhanced invitro Bioavailability: Characterization and antimicrobialactivity. Drug Des. Devel. Ther. 2018, 12, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, S. Phytosomes: The New Technology for Enhancement of Bioavailability of Botanicals and Nutraceuticals. Int. J. Health Res. 2009, 2, 225–232. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, Y.; Wei, Y.; Liu, H.; Zhang, G.; Wu, X. Preparation and in Vitro Evaluation of Ethosomal Total Alkaloids of Sophora Alopecuroides Loaded by a Transmembrane PH-Gradient Method. AAPS Pharm. Sci. Tech. 2010, 11, 1350–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.G. Preparation of Curcumin Ethosomes. Afr. J. Pharm. Pharmacol. 2013, 7, 2246–2251. [Google Scholar] [CrossRef]
- Tong, W.; Wang, L.; D’Souza, M.J. Evaluation of PLGA microspheres as delivery system for antitumor agent-camptothecin. Drug Dev. Ind. Pharm. 2003, 29, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Thangavelu, M.; Adithan, A.; Peter, J.S.J.; Hossain, M.A.; Kim, N.S.; Hwang, K.C.; Khang, G.; Kim, J.H. Ginseng compound K incorporated porous Chitosan/biphasic calcium phosphate composite microsphere for bone regeneration. Int. J. Biol. Macromol. 2020, 146, 1024–1029. [Google Scholar] [CrossRef]
- Zeng, Z.; Zhou, G.; Wang, X.; Huang, E.Z.; Zhan, X.; Liu, J.; Wang, S.; Wang, A.; Li, H.; Pei, X.; et al. Preparation, Characterization and Relative Bioavailability of Oral Elemene o/w Microemulsion. Int. J. Nanomed. 2010, 5, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Chang, X.; Weng, T.; Zhao, X.; Gao, Z.; Yang, Y.; Xu, C.; Yang, X. A Study of Microemulsion Systems for Transdermal Delivery of Triptolide. J. Control. Release 2004, 98, 427–436. [Google Scholar] [CrossRef]
- Jourghanian, P.; Ghaffari, S.; Ardjmand, M.; Haghighat, S.; Mohammadnejad, M. Sustained release Curcumin loaded Solid Lipid Nanoparticles. Adv. Pharm. Bull. 2006, 6, 17–21. [Google Scholar] [CrossRef] [Green Version]
- Mei, Z.; Li, X.; Wu, Q.; Hu, S.; Yang, X. The Research on the Anti-inflammatory activity and Hepatotoxicity of triptolide-loaded Solid Lipid Nanoparticle. Pharmacol. Res. 2005, 51, 345–351. [Google Scholar] [CrossRef]
- El-Samaligy, M.S.; Nagia, N.A.; Enas, A.M. Evaluation of Hybrid Liposomes-Encapsulated Silymarin Regarding Physical Stability and in Vivo Performance. Int. J. Pharm. 2006, 319, 121–129. [Google Scholar] [CrossRef]
- Wencui, Z.; Qi, Z.; Ying, W.; Di, W. Preparation of solid lipid nanoparticles loaded with garlic oil and evaluation of their in vitro and in vivo characteristics. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3742–3750. [Google Scholar]
- Sinjari, B.; Pizzicannella, J.; D’Aurora, M.; Zappacosta, R.; Gatta, V.; Fontana, A.; Trubiani, O.; Diomede, F. Curcumin/Liposome Nanotechnology as Delivery Platform for Anti-Inflammatory Activities via NFkB/ERK/pERK Pathway in Human Dental Pulp Treated with 2-Hydroxy Ethyl MethAcrylate (HEMA). Front. Physiol. 2019, 10, 633. [Google Scholar] [CrossRef] [PubMed]
- Ruan, J.; Liu, J.; Zhu, D.; Gong, T.; Yang, F.; Hao, X.; Zhang, Z. Preparation and Evaluation of Self-Nanoemulsified Drug Delivery Systems (SNEDDSs) of Matrine Based on Drug-Phospholipid Complex Technique. Int. J. Pharm. 2010, 386, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Gunasekaran, T.; Haile, T.; Nigusse, T.; Dhanaraju, M.D. Nanotechnology: An Effective Tool for Enhancing Bioavailability and Bioactivity of Phytomedicine. Asian Pac. J. Trop. Biomed. 2014, 4, S1–S7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Zhang, T.; Ye, Y.; Zhang, X.; Wu, B. Enhanced Bioavailability of Tripterine through Lipid Nanoparticles using Broccoli-Derived Lipid S as a Carrier Material. Int. J. Pharm. 2015, 495, 948–955. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, T.; Zhou, X.; Liu, H.; Sun, H.; Ma, Z.; Wu, B. Enhancement of Oral Bioavailability of Tripterine through Lipid Nanospheres: Preparation, Characterization, and Absorption Evaluation. J. Pharm. Sci. 2014, 103, 1711–1719. [Google Scholar] [CrossRef]
- Freag, M.S.; Saleh, W.M.; Abdallah, O.Y. Laminated Chitosan-based Composite Sponges for Transmucosal Delivery of Novel Protamine-Decorated Tripterine Phytosomes: Ex-vivo Mucopenetration and in-vivo Pharmacokinetic Assessments. Carbohydr. Polym. 2018, 188, 108–120. [Google Scholar] [CrossRef]
- Tonglairoum, P.; Ngawhirunpat, T.; Rojanarata, T.; Kaomongkolgit, R.; Opanasopit, P. Fabrication and Evaluation of Nanostructured Herbal Oil/Hydroxypropyl-β-Cyclodextrin/Polyvinylpyrrolidone Mats for Denture Stomatitis Prevention and Treatment. AAPS Pharm. Sci. Tech. 2016, 17, 1441–1449. [Google Scholar] [CrossRef] [Green Version]
- You, J.; Cui, F.D.; Han, X.; Wang, Y.S.; Yang, L.; Yu, Y.W.; Li, Q.P. Study of the Preparation of Sustained-Release Microspheres Containing Zedoary Turmeric Oil by the Emulsion-Solvent-Diffusion Method and Evaluation of the Self-Emulsification and Bioavailability of the Oil. Colloids Surf. B Biointerfaces 2006, 48, 35–41. [Google Scholar] [CrossRef]
- Zhang, J.; Lv, H.; Jiang, K.; Gao, Y. Enhanced Bioavailability after Oral and Pulmonary Administration of Baicalein Nanocrystal. Int. J. Pharm. 2011, 420, 180–188. [Google Scholar] [CrossRef]
- Bilia, A.R.; Guccione, C.; Isacchi, B.; Righeschi, C.; Firenzuoli, F.; Bergonzi, M.C. Essential Oils Loaded in Nanosystems: A Developing Strategy for a Successful Therapeutic Approach. Evid. Based Complement. Altern. Med. 2014, 2014, 651593. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Chevvuri, R.; Sharma, H. Nanotechnology in Dentistry: Unleashing the Hidden Gems. J. Indian Soc. Periodontol. 2018, 22, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Tubtimsri, S.; Limmatvapirat, C.; Limsirichaikul, S.; Akkaramongkolporn, P.; Inoue, Y.; Limmatvapirat, S. Fabrication and Characterization of Spearmint Oil Loaded Nanoemulsions as Cytotoxic Agents against Oral Cancer Cell. Asian J. Pharm. Sci. 2018, 13, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, A.C.L.; Pereira, S.A.C.; Pereira, J.V.; Pereira, L.F.; Furtado, D.; Macedo-Costa, M.R.; Higino, J.S. Antiadherent Effect of the Extract of the Matricaria Recutita Linn. on Microrganisms of Dental Biofilm. Rev. Odontol. UNESP 2010 2013, 39, 21–25. [Google Scholar]
- Ahmad, N.; Ahmad, F.J.; Bedi, S.; Sharma, S.; Umar, S.; Ansari, M.A. A Novel Nanoformulation Development of Eugenol and Their Treatment in Inflammation and Periodontitis. Saudi Pharm. J. 2019, 27, 778–790. [Google Scholar] [CrossRef]
- Lemes, R.S.; Alves, C.; Estevam, E.; Santiago, M.B.; Martins, C.; Santos, T.; Crotti, A.; Miranda, M. Chemical Composition and Antibacterial Activity of Essential Oils from Citrus Aurantifolia Leaves and Fruit Peel against Oral Pathogenic Bacteria. Acad. Bras. Cienc. 2018, 90, 1285–1292. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Ottolenghi, L.; Gaillard, C.; Bourgeois, D. Nanoparticlesas Anti-Microbial, Anti-Inflammatory, and Remineralizing Agents in Oral Care Cosmetics: A Review of the Current Situation. Nanomaterials 2020, 10, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moulari, B.; Lboutounne, H.; Chaumont, J.P.; Guillaume, Y.; Millet, J.; Pellequer, Y. Potentiation of the bactericidal activity of Harungana madagascariensis Lam. ex Poir. (Hypericaceae) leaf extract against oral bacteria using poly (D, L-lactide-co-glycolide) nanoparticles: In vitro study. Acta Odontol. Scand. 2006, 64, 153–158. [Google Scholar] [CrossRef]
- Horváth, B.; Balázs, V.L.; Varga, A.; Böszörményi, A.; Kocsis, B.; Horváth, G.; Széchenyi, A. Preparation, characterisation and microbiological examination of Pickering nano-emulsions containing essential oils, and their effect on Streptococcus mutans biofilm treatment. Sci. Rep. 2019, 9, 16611. [Google Scholar] [CrossRef]
- Donsì, F.; Ferrari, G. Essential Oil Nanoemulsions as Antimicrobial Agents in Food. J. Biotechnol. 2016, 233, 106–120. [Google Scholar] [CrossRef]
- Soltanzadeh, M.; Peighambardoust, S.H.; Ghanbarzadeh, B.; Mohammadi, M.; Lorenzo, J.M. Chitosan Nanoparticles as a Promising Nanomaterial for Encapsulation of Pomegranate (Punicagranatum L.) Peel Extract as a Natural Source of Antioxidants. Nanomaterials 2021, 11, 1439. [Google Scholar] [CrossRef]
- Cinthura, C.; Rajasekar, A. Antibacterial Activity of Cinnamon—Clove Mediated Silver Nanoparticles against Streptococcus Mutans. Plant Cell Biotechnol. Mol. Biol. 2020, 21, 11–17. Available online: https://www.ikppress.org/index.php/PCBMB/article/view/5348 (accessed on 28 August 2021).
- de Carvalho Bernardo, W.L.; Boriollo, M.; Tonon, C.C.; da Silva, J.J.; Cruz, F.M.; Martins, A.L.; Höfling, J.F.; Spolidorio, D. Antimicrobial Effects of Silver Nanoparticles and Extracts of Syzygium Cumini Flowers and Seeds: Periodontal, Cariogenic and Opportunistic Pathogens. Arch. Oral Biol. 2021, 125, 105101. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, D.A.; Bayoumi, F.S.; Taher, H.M.; Abdelmonem, B.H.; Eissa, T.F. Antimicrobial Potential of Mentha Spp. Essential Oils as Raw and Loaded Solid Lipid Nanoparticles against Dental Caries. Res. J. Pharm. Technol. 2020, 13, 4415–4422. [Google Scholar] [CrossRef]
- Comin, V.M.; Lopes, L.Q.; Quatrin, P.M.; de Souza, M.E.; Bonez, P.C.; Pintos, F.G.; Raffin, R.P.; Vaucher, R.; Martinez, D.S.; Santos, R.C. Influence of Melaleuca alternifolia oil nanoparticles on aspects of Pseudomonas aeruginosa biofilm. Microb. Pathog. 2016, 93, 120–125. [Google Scholar] [CrossRef]
- Souza, M.E.; Lopes, L.Q.; Bonez, P.C.; Gündel, A.; Martinez, D.S.; Sagrillo, M.R.; Giongo, J.L.; Vaucher, R.A.; Raffin, R.P.; Boligon, A.A.; et al. Melaleuca alternifolia nanoparticles against Candida species biofilms. Microb. Pathog. 2017, 104, 125–132. [Google Scholar] [CrossRef]
- Soltanzadeh, M.; Peighambardoust, S.H.; Ghanbarzadeh, B.; Mohammadi, M.; Lorenzo, J.M. Chitosan Nanoparticles Encapsulating lemongrass (Cymbopogon commutatus) essential oil: Physicochemical, Structural, Antimicrobial and in-vitro release properties. Int. J. Biol. Macromol. 2021, 192, 1084–1097. [Google Scholar] [CrossRef]
- Liakos, I.L.; Grumezescu, A.M.; Holban, A.M.; Florin, I.; D’Autilia, F.; Carzino, R.; Bianchini, P.; Athanassiou, A. Polylactic Acid-Lemongrass Essential Oil Nanocapsules with Antimicrobial Properties. Pharmaceuticals 2016, 9, 42. [Google Scholar] [CrossRef] [Green Version]
- Saquib, S.A.; AlQahtani, N.A.; Ahmad, I.; Kader, M.A.; AlShahrani, S.S.; Asiri, E.A. Evaluation and Comparison of Antibacterial Efficacy of Herbal Extracts in Combination with Antibiotics on Periodontal pathobionts: An in vitro Microbiological Study. Antibiotics 2019, 8, 89. [Google Scholar] [CrossRef] [Green Version]
- Dera, A.A.; Ahmad, I.; Rajagopalan, P.; Shahrani, M.A.; Saif, A.; Alshahrani, M.Y.; Alraey, Y.; Alamri, A.M.; Alasmari, S.; Makkawi, M. Synergistic Efficacies of Thymoquinone and Standard Antibiotics against Multi-Drug Resistant Isolates. Saudi Med. J. 2021, 42, 196–204. [Google Scholar] [CrossRef]
- Rafiq, Z.; Narasimhan, S.; Haridoss, M.; Vennila, R.; Vaidyanathan, R. Punica granatum rind extract: Antibiotic Potentiator and Efflux Pump Inhibitor of Multi drug-resistant Klebsiella pneumonia Clinical Isolates. Asian J. Pharm. Clin. Res. 2017, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.B.; Gao, S.S.; Yu, H.Y. Effect of Nano-hydroxyapatite Concentration on Remineralization of Initial Enamel Lesion in vitro. Biomed. Mater. 2009, 4, 034104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.; Gao, S.; Cheng, L.; Yu, H. Combined Eeffects of Nano-hydroxyapatite and Galla chinensis on Remineralisation of Initial Enamel Lesion in vitro. J. Dent. 2010, 38, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.C.F.; Seneviratne, C.J.; Li, X.; Leung, P.C.; Lau, C.B.; Wong, C.H.; Pang, K.Y.; Wong, C.W.; Wat, E.; Jin, L. Synergistic Antibacterial Effects of Nanoparticles Encapsulated with Scutellaria Baicalensis and Pure Chlorhexidine on Oral Bacterial Biofilms. Nanomaterials 2016, 6, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madan, S.; Nehate, C.; Barman, T.K.; Rathore, A.S.; Koul, V. Design, Preparation, and Evaluation of Liposomal Gel Formulations for Treatment of Acne: In vitro and in vivo studies. Drug Dev. Ind. Pharm. 2019, 45, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, S.; Alihosseini, F.; Sorkhabadi, S.M.R.; Bidgoli, S.A.; Mousavi, S.E.; Haghighat, S.; Nasab, A.A.; Kianvash, N. Nanotechnology in wound healing; Semisolid dosage forms containing Curcumin-Ampicillin solid lipid nanoparticles, in-vitro, ex-vivo and in-vivo characteristics. Adv. Pharm. Bull. 2018, 8, 395–400. [Google Scholar] [CrossRef]
- Harwansh, R.K.; Deshmukh, R.; Rahman, M.A. Nanoemulsion: Promising Nanocarrier System for Delivery of Herbal Bioactives. J. Drug Deliv. Sci. Technol. 2019, 51, 224–233. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| S. No | Plant | Biological Name | Active Phyto-Constitutent | Part of Plant Used | Activity | Reference |
|---|---|---|---|---|---|---|
| 1 | Neem | Azadirachtain indica | Azadirachtin | Leaves | Antimicrobial, anti-inflammatory,antibacterial, and antiplaque activity | [20] |
| 2 | Triphala | Emblica officinalis | Gallic acid, tannic acid, syringic acid, andepicatechinalong with ascorbic acid | Fruits | Antibacterial, antimicrobial, antioxidant, anti-inflammatory, and radical scavenging activity | [21] |
| 3 | Garlic | Alliumsativum | Allicin | Rhizomes | Antimicrobial, antibacterial, antifungal, antiviral, anti-inflammatory, and antioxidant activities | [22] |
| 4 | Gum acacia | Acacia catechu | Catechin, epicatechin, epigallocatechin, alkaloids, and tannins | Bark | Antibacterial, anti-inflammatory, astringent, antifungal, antimicrobial, and anticancer properties | [43] |
| 5 | Roselle | Hibiscus sabdariffa | Hibiscus acid andprotocatechuic acid | Seeds, leaves, fruits, and roots | Antimicrobial, antibacterial effect | [44] |
| 6 | Ginger | Zingiber officinale | Gingerols | Rhizome | Antimicrobial effect | [44] |
| 7 | Green tea | Camellia sinensis | Catechins | Dried leaves | Antibacterial activity | [44] |
| 8 | Liquorice | Glycyrrhiza glabra | Glycyrrhizin | Root extracts | Antiadherence, antimicrobial, and anti-inflammatory properties | [24] |
| 9 | Meswak | Salvadora persica | Volatile oils, flavonoids, alkaloids, steroids, terpenoids, saponins, and carbohydrates | Roots | Antibacterial, anti-inflammatory, anticariogenic | [24] |
| 10 | Turmeric | Curcuma longa | Curcumin | Rhizome | Analgesic, anti-inflammatory, antioxidant, antiseptic, and antimicrobial activity | [45] |
| 11 | Cinnamon oil | Cinnamomum zeylanicum | Cinnamaldehyde, cinnamic acid, and trans-cinnamaldehyde | Leaves, bark, root, and fruit | Antimicrobial activity | [46] |
| 12 | Citronella oil | Cymbopogon nardus | Citronellal, citronellol, nerol, geraniol, limonene | Leaves and fruit peel | Antibiofilm, antibacterial, antiseptic, antifungal, and anticariogenic activity | [47] |
| 13 | Tea tree oil | Melaleuca alternifolia | Terpinen-4-ol, γ-terpinene, α-terpinene | Leaves | Antimicrobial properties | [24] |
| 14 | Eucalyptus oil | Eucalyptus globulus | Eucalyptol, α-pinene, δ-limonene | Leaves | Antibacterial, antimicrobial, anti-inflammatory effect, andfreshening properties | [48] |
| 15 | Lemongrass oil | Cymbopogon citratus | Citral | Leaves | Antibacterial, antifungal, antioxidant, antiseptic, astringent, anti-inflammatory properties | [49] |
| 16 | Myrtle oil | Myrtus communis | α-pinene, limonene, 1.8-cineole, 4-terpineol, α-terpineol, linalool | Leaves | Anti-inflammatory, antimicrobial, antibacterial activity | [50] |
| 17 | Ajwain oil | Trachyspermumammi | Thymol, camphene, myrcene, and α-3-carene | Leavesand the seed-like fruit | Antimicrobial, antibacterial, germicidal, antifungal activity | [51] |
| 18 | Red sage | Salvia miltiorrhiza | Tanshinone IIA | Stem, leaves, fruit | Anticancer activity against oral squamous cancer cell line | [52] |
| 19 | Thunder duke vine | Tripterygium wilfordii | Triptolide | Peeled roots | Anti-inflammatory in oral lichen planus, mouth ulcers | [53] |
| 20 | Bitter bean | Sophora alopecuroides | Sophora alkaloids | Seeds and aerial parts | Antibacterial, anti-inflammatory | [54,55] |
| 21 | Happy tree | Camptotheca acuminata | Camptothecin | Bark, wood | Anticancer activity against oral squamous cancer cell line | [56] |
| 22 | Korean red ginseng | Panax ginseng | Ginsenosides | Root | Bone regeneration in dental implant | [57] |
| Formulation | Phytoconstituent | Source | Outcome | Reference |
|---|---|---|---|---|
| Nanosuspension | Zerumbone | Zinigiber zerumbet rhizome | Formulations with 200 nm particle size were prepared, which significantly (p < 0.05) enhanced the saturation solubility and dissolution 2-fold | [71] |
| Inclusion complex with hydroxylpropyl-β-cyclodextrin | Zerumbone | Zinigiber zerumbet rhizome | Enhanced the solubility >30-fold | [72] |
| Nanoemulsion | Curcumin | Curcuma longa rhizomes | The droplet size of the formulation was 196 nm, which enhanced the dissolution by upto 95% and bioavailability 8-folds | [73] |
| Tanshinone IIA | Root of Salvia miltiorrhiza | Smaller particle size (95.6 nm) enabled faster dissolution, 100% in 20 min, and better cytotoxic properties can be expected | [74] | |
| Nanoparticles | Tanshinone IIA | Radix salvia miltiorrhiza | Small size of the nanoparticles improved the dissolution of tanshinone and better bioavailability can be expected | [63] |
| Berberine | Berberis aristata | Encapsulation into nanoparticles reduced the crystallinity of berberine coupled with small size, which significantly (p < 0.0001) enhanced the aqueous solubility and dissolution. The antimicrobial activity also increased 3–4-fold against Gram-positive bacteria, Gram-negative bacteria, and yeasts | [75] | |
| Phytosomes | Epigallocatechin-3-gallate | Thea sinensis | Complexation with phospholipids helped in increasing oral absorption and plasma drug concentration 2-fold, which suggests its potential in enhancing bioavailability | [76] |
| Silybin | Silymarin | The phospholipid complex augmented the lipophilicity of silymarin and improved the oral bioavailability 4-fold | [76] | |
| Ethosomes | Lemannine, matrine, sophoridine, sophocarpine | Sophora alopecuerides | Loading sophora alkaloids in ethosomes provided penetration to deeper skin layers (up to 180 µ) and facilitated transdermal delivery, which is a viable alternative to avoid bitter taste of drug | [77] |
| Curcumin | Curcuma longa | Ethosomes were prepared with 93% entrapment efficiency. The formulation enhanced skin permeation, which suggests that it can be used for transdermal delivery. High rate of metabolism in intestine and rapid clearance can be overcome by transdermal delivery of curcumin | [78] | |
| Microspheres | Camptothecin | Camptotheca acuminata | Camptothecin is sensitive to pH changes in the body. Encapsulation in PLGA microspheres provided stability through acidic microenvironment. The size of the microspehers (1.3 µm) improved antitumor activity by enhancing uptake by cancer cells | [79] |
| Ginsenosides | Ginseng | Chitosan microspheres provided adhesion to bone cells and the active compound ginsenosides promoted bone regeneration | [80] | |
| Microemulsion | Elemene oil | Curcuma wenyujin | Microemulsion improved the aqueous solubility, stability, and oral bioavailability (163%) of the volatile oil | [81] |
| Triptolide | Tripterygium wilfordii | The formulation provided sustained and prolonged delivery of herbal ingredient which is useful for limiting the toxicity associated with drug | [82] | |
| Solid lipid nanoparticles | Curcumin | Curcuma longa | SLN improved the solubility and bioavailability of curcumin and thus MIC and MBC wereconsiderably reduced | [83] |
| Triptolide | Tripterygium wilfordii | SLN loaded with triptolide was taken up by lymphatic system and exhibited negligle toxicity to liver and kidney. Improved anti-inflammatory activity due to increase in oral bioavailability and prolonged plasma drug levels was observed | [84] | |
| Liposomes | Silymarin | Silybum marianum | Silymarin hybrid liposomes were developed to improve its poor bioavailability. It showed improved hepatoprotective activity, enhanced permeation through buccal mucosa, and stability of silymarin | [85] |
| Garlic oil | Allium sativum | SLN were prepared with >90% entrapment efficiency. The formulation also improved the solubility of garlic oil, as evident by drug relase studies carried out in phosphate-buffered medium (11% in 17 h) | [86] | |
| Curcumin | Curcuma longa | Encapsulation in liposomes increased the solubility and anti-inflammatory activity in 2-hydroxyethyl methacrylate induced inflammation in dental pulp stem cells | [87] | |
| Self- nanoemulsified delivery system (SNEDDS) | Matrine | Sophora flavescens | Matrine was complexed with phospholipid and lipid solubility was increased by 600%. Further, the complex was loaded in SNEDDS, increasing the intestinal absorption and ultimately oral bioavailability by 60% | [88] |
| Phytoconstituent | Nanodelivery System | Bacterial Sp. | Outcome | Reference |
|---|---|---|---|---|
| Nano punica granatum and nano garlic herbal extract | Nanoemulsification | Enterococcus faecalis and Staphylococcus epidermidis | Significantly (p < 0.001) higher dead bacterial count was witnessed withnano-herbal extracts when compared to medicated calcium hydroxide gel. Insignificant differences were observed between pomegranate and garlic extract. | [106] |
| Eugenol | Nanoemulsion | S. aureus and E. coli | The eugenol nanoemulsion gel showed improved antibacterial activity (double) compared to eugenol solution. The small size helped in fusion with bacterial cells and the surfactants in the formulation disrupted the cell membrane. | [100] |
| Cinnamon, clove | Silver nanoparticles | Streptococcus mutans | Cinnamon and clove silver nanoparticles exhibited wider zones of inhibition (10 mm) compared to amoxycillin (8 mm), suggestive of good antibacterial efficiency. | [107] |
| Syzygium cumini | Silver nanoparticles | C. albicans and S. mutans | The extracts encapsulated in silver nanoparticles exhibited improved antimicrobial properties, as suggested by a ratio of MIC of 0.98 for silver nanoparticles to seed extracts. | [108] |
| Mentha spp. | Solid lipid nanostructure | Streptococcus mutans and Streptococcus pyogenes | The findings demonstrated that Mentha essential oil loaded in nanostructure increased theantibacterial activity (zone of inhibition 20 mm, compared to 10 mm shown by essential oil solution). | [109] |
| Tea tree oil | Nanoparticles | P. aeruginosa | Tea tree oil nanoparticles reduced the motility of bacteria (by 62%) and adhesion of biofilms, which was otherwise not detected on using bare oil. | [110] |
| Tea tree oil | Nanoparticles | P. gingivalis, A. actinomycetemcomitan, F. nucleatum | Nanoparticles were prepared with size of 198 nm. Small size allowed penetration within the biofilm matrix and the bacterial viability was 26%, compared to 51% shown by M. alternifolia oil. | [111] |
| Lemongrass oil (Citral) | Chitosan nanoparticles | Gram-positive and Gram-negative bacteria | Chitosan nanoparticles increased the thermal stability of oil. The antimicrobial properties increased sinificantly (p < 0.001) when compared to bare oil. | [112] |
| Lemongrass oil | Nanocapsule | P. aeruginosa, E. coli, C. albicans, S. aureus | The lemongrass oil reduced the MIC by almost half when loaded in nanocapsules. The biofilm formation was also reduced by 2 times for all the species except P. aeruginosa. | [113] |
| Eucalyptus oil (eucalyptol, α-pinene, and δ-limonene) | Nanoemulsion | P. aeruginosa, Candida spp. |
| Formulation | Drug | Phytoconstitutent | Outcome | Reference |
|---|---|---|---|---|
| Nanoparticles | Chlorhexidine | Scutellaria baicalensi | Study showed one-fold enhanced antibacterial effects of nanoparticles with chlorhexidine and Scutellaria baicalensi (MIC 50 µg/mL) on oral bacterial biofilms compared to either treatment used alone (MIC 100 µg/mL). | [119] |
| Liposome | Lauric acid | Curcumin | Liposome formulation containing lauric acid and curcumin in 1:1 ratio exhibited 1.5–2-fold greater antibacterial activity than their single forms. | [120] |
| Nanostructured lipid carriers | Ampicillin | Curcumin | The formulation showed synergistic antibacterial efficacy and enhanced the wound healing rate. | [121] |
| Patent No. | Published | Description |
|---|---|---|
| U.S. 10,342,840 B2 | 9 July 2019 | Titanium dioxide nanomaterials adsorbed with organic functional groups and citric acid herbal extracts for antimicrobial activity |
| WO 2021/116917 A1 | 17 June 2021 | Nanocellulose with active herbal ingredients formulated as gels/films |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, R.; Mirza, M.A.; Naseef, P.P.; Kuruniyan, M.S.; Zakir, F.; Aggarwal, G. Exploring the Potential of Natural Product-Based Nanomedicine for Maintaining Oral Health. Molecules 2022, 27, 1725. https://doi.org/10.3390/molecules27051725
Kumar R, Mirza MA, Naseef PP, Kuruniyan MS, Zakir F, Aggarwal G. Exploring the Potential of Natural Product-Based Nanomedicine for Maintaining Oral Health. Molecules. 2022; 27(5):1725. https://doi.org/10.3390/molecules27051725
Chicago/Turabian StyleKumar, Rajeev, Mohd A. Mirza, Punnoth Poonkuzhi Naseef, Mohamed Saheer Kuruniyan, Foziyah Zakir, and Geeta Aggarwal. 2022. "Exploring the Potential of Natural Product-Based Nanomedicine for Maintaining Oral Health" Molecules 27, no. 5: 1725. https://doi.org/10.3390/molecules27051725
APA StyleKumar, R., Mirza, M. A., Naseef, P. P., Kuruniyan, M. S., Zakir, F., & Aggarwal, G. (2022). Exploring the Potential of Natural Product-Based Nanomedicine for Maintaining Oral Health. Molecules, 27(5), 1725. https://doi.org/10.3390/molecules27051725