


Developed and Validated Capillary Isotachophoresis Method for the Rapid Determining Organic Acids in Children’s Saliva
 , ,
, ,
Abstract
:1. Introduction
2. Results and Discussion
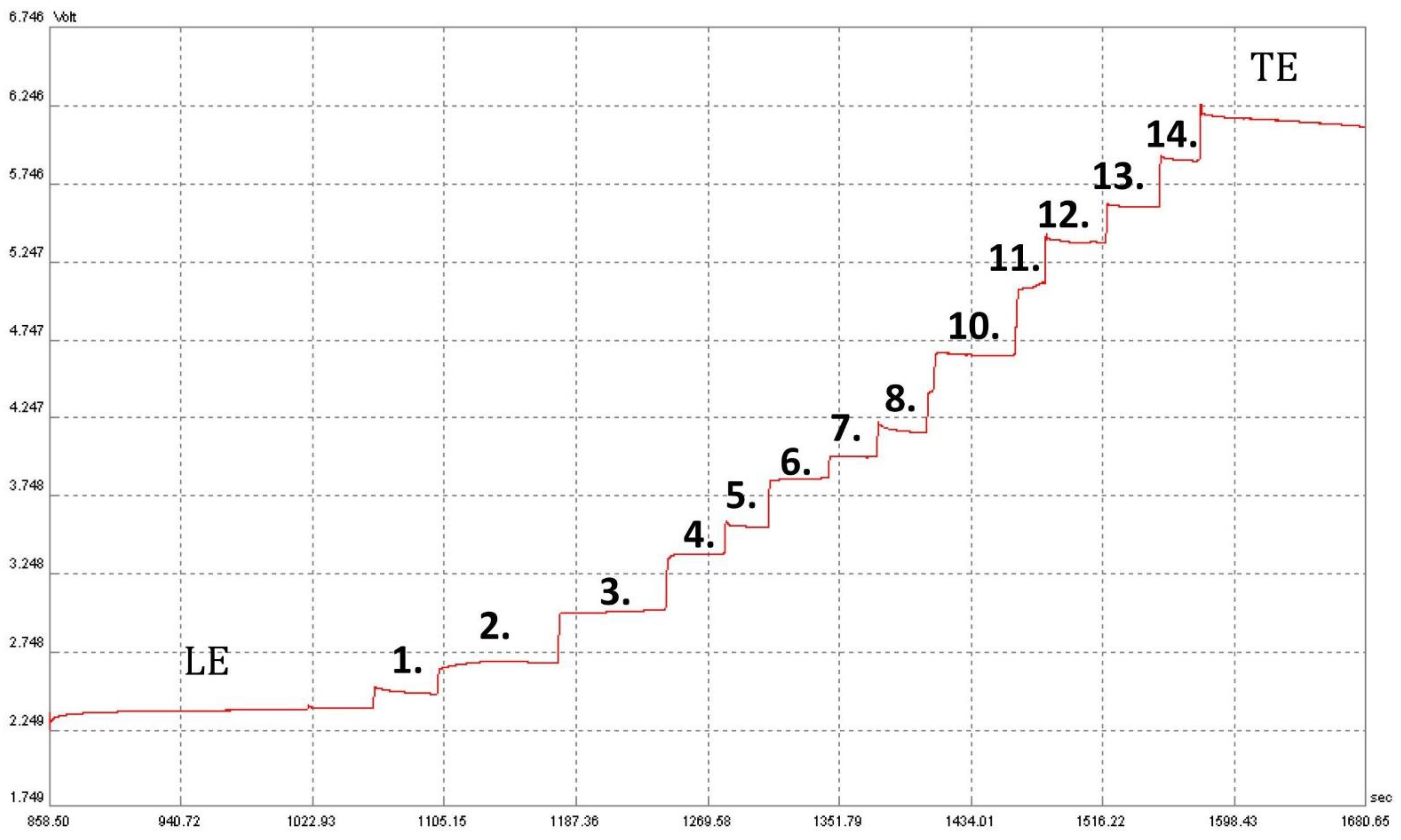
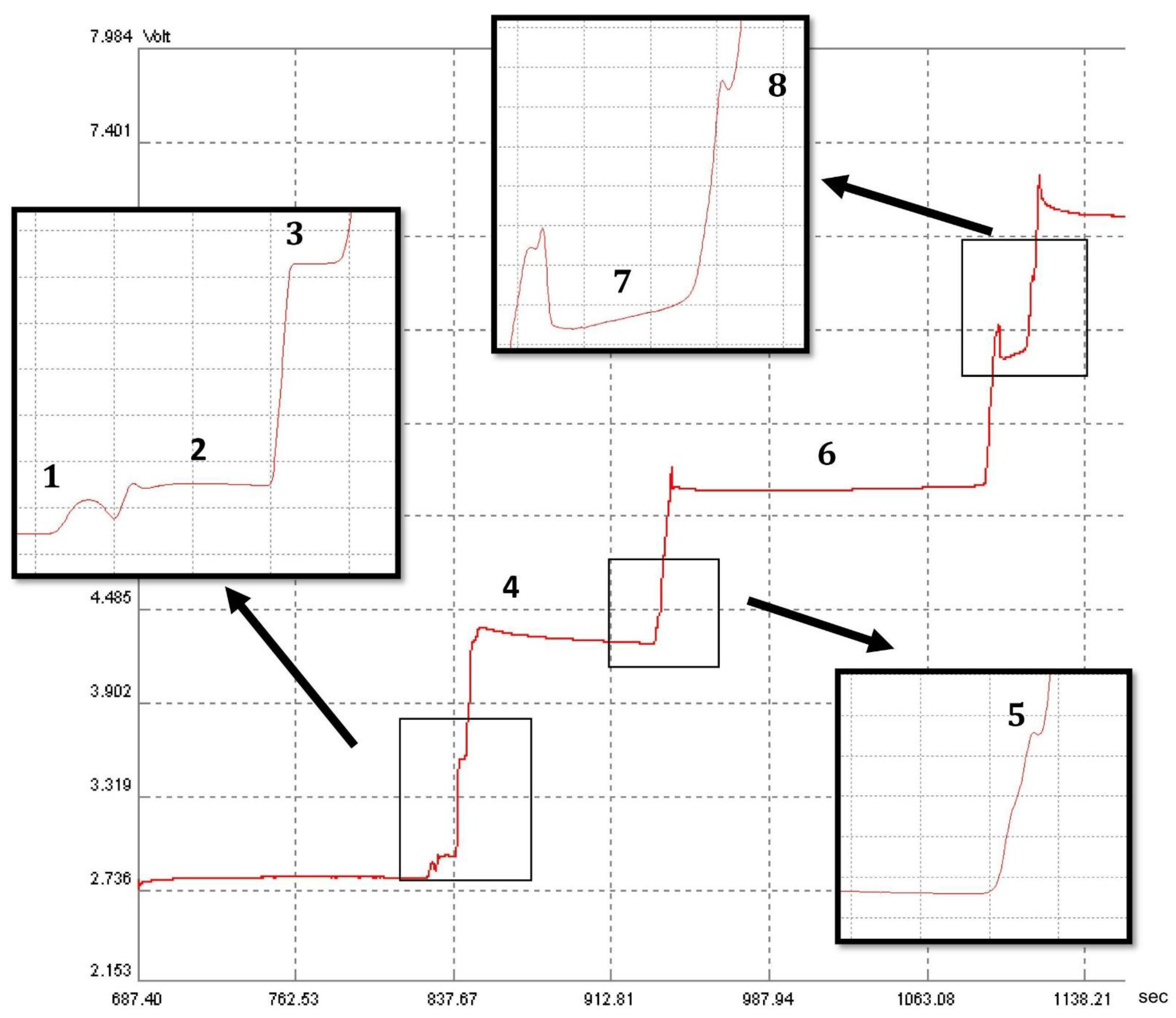
2.1. Separation of Organic and Inorganic Acid Ions
2.2. Identification of Organic and Inorganic Acid Ions
2.3. Validation of the Method
2.3.1. Limit of Detection and Quantification, Calibration Curves
2.3.2. Precision and Recovery
2.4. Organic Acid in Children’s Saliva Determined by Means of Other Analytical Methods
2.5. Application of the RGB Model for Method Evaluation
3. Materials and Methods
3.1. Sample Collection and Sample Preparation
3.2. Reagents
3.3. Instrumentation
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Limitations
References
- Javaid, M.A.; Ahmed, A.S.; Durand, R.; Tran, S.D. Saliva as a diagnostic tool for oral and systemic diseases. J. Oral Biol. Craniofac. Res. 2016, 6, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dąbek-Drobny, A.; Kaczmarczyk, O.; Woźniakiewicz, M.; Paśko, P.; Dobrowolska-Iwanek, J.; Woźniakiewicz, A.; Piątek-Guz iewicz, A.; Zagrodzki, P.; Zwolińska-Wcisło, M. Association between Fecal Short-Chain Fatty Acid Levels, Diet, and Body Mass Index in Patients with Inflammatory Bowel Disease. Biology 2022, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Richards, V.P.; Alvarez, A.J.; Luce, A.R.; Bedenbaugh, M.; Mitchell, M.L.; Burne, R.A.; Nascimento, M.M. Microbiomes of Site-Specific Dental Plaques from Children with Different Caries Status. Infect. Immun. 2017, 85, e00106-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qudeimat, M.A.; Alyahya, A.; Karched, M.; Behbehani, J.; Salako, N.O. Dental plaque microbiota profiles of children with caries-free and caries-active dentition. J. Dent. 2021, 104, 103539. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal disease, tooth loss, and cancer risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bel’skaya, L.V.; Sarf, E.A.; Solomatin, D.V.; Kosenok, V.K. Metabolic Features of Saliva in Breast Cancer Patients. Metabolites 2022, 12, 166. [Google Scholar] [CrossRef] [PubMed]
- Shibata, A.; Minami, J.; Nakamura, S.; Terano, M.; Koike, M.; Suenaga, H.; Fujii, H. Salivary organic acids in metal allergy suspected patients and non-metal allergy patients. Int. Chin. J. Dent. 2004, 4, 107–113. [Google Scholar]
- Park, Y.D.; Jang, J.H.; Oh, Y.J.; Kwon, H.J. Analyses of organic acids and inorganic anions and their relationship in human saliva before and after glucose intake. Arch. Oral Biol. 2014, 59, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Navazesh, M.; Kumar, S.K. Measuring salivary flow: Challenges and opportunities. J. Am. Dent. Assoc. 2008, 139, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Yamuna, P.K.; Muthu, P.K. Methods of collection of saliva—A Review. Int. J. Oral Health Dent. 2017, 3, 149–153. [Google Scholar]
- Bellagambi, F.G.; Lomonaco, T.; Salvo, P.; Vivaldi, F.; Hangouët, M.; Ghimenti, S.; Biagini, D.; Di Francesco, F.; Fuoco, R.; Errachid, A. Saliva sampling: Methods and devices: An overview. TrAC Trends Analytical Chem. 2019, 124, 115781. [Google Scholar] [CrossRef]
- See, H.H.; Ali, N.A. Electrophoresis. Capillary Electrophoresis: Principles of Capillary, Encyclopedia of Analytical Science, 3rd ed.; Worsfold, P., Poole, C., Townshend, A., Miró, M., Eds.; Academic Press: Oxford, UK, 2019; pp. 328–333. [Google Scholar]
- Malá, Z.; Gebauer, P. Analytical isotachophoresis 1967–2022: From standard analytical technique to universal on-line concentration tool. Trends Analyt. Chem. 2022, 158, 116837. [Google Scholar] [CrossRef]
- Schulz, A.; Lang, R.; Behr, J.; Hertel, S.; Reich, M.; Kummerer, K.; Hannig, M.; Hannig, C.; Hofmann, T. Targeted metabolomics of pellicle and saliva in children with different caries activity. Sci. Rep. 2020, 10, 697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahluwalia, M.; Brailsford, S.R.; Tarelli, E.; Gilbert, S.C.; Clark, D.T.; Barnard, K.; Beighton, D. Dental caries, oral hygiene, and oral clearance in children with craniofacial disorders. J. Dent. Res. 2004, 83, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A. Determination of the content of organic acids in the saliva of patients with breast cancer by capillary electrophoresis. Klin. Lab. Diagn. 2018, 63, 419–422. [Google Scholar] [PubMed]
- Fidalgo, T.; Freitas-Fernandes, L.B.; Angeli, R.; Muniz, A.M.S.; Gonsalves, E.; Santos, R.; Nadal, J.; Almeida, F.C.L.; Valente, A.P.; Souza, I.P.R. Salivary metabolite signatures of children with and without dental caries lesions. Metabolomics 2012, 9, 657–666. [Google Scholar] [CrossRef]
- Everaerts, F.M.; Beckers, J.L.; Verheggen, T.P.E.M. Choice of Electrolyte Systems. Journal of Chromatography Library, Volume 6; Elsevier: Amsterdam, The Netherlands; Oxford, UK; New York, NY, USA, 1976; pp. 83–113. [Google Scholar]
- Hirokawa, T.; Nishino, M.; Aoki, N.; Kiso, Y.; Sawamoto, Y.; Yagi, T.; Akiyama, J. Table of isotachophoretic indices: I. Simulated qualitative and quantitative indices of 287 anionic substances in the range pH 3–10. J. Chromatogr. 1983, 271, D1–D106. [Google Scholar] [CrossRef]
- Nowak, P.M.; Koscielniak, P. What color is your method? Adaptation of the RGB additive color model to analytical method evaluation. Anal. Chem. 2019, 91, 10343–10352. [Google Scholar] [CrossRef] [PubMed]
- Nowak, P.M.; Bis, A.; Rusin, M.; Woźniakiewicz, M. Carbon footprint of the analytical laboratory and the three-dimensional approach to its reduction. Green Anal. Chem. 2023, 4, 100051. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Acids | Conc. (mg/L) | LOD (mg/L /µM) | LOQ (mg/L /µM) | R2 | Recovery (%) Level I | Recovery (%) Level II | RSD (%) (n = 6) |
|---|---|---|---|---|---|---|---|
| formic acid | 7.5 ± 0.3 | 0.13/2.82 | 0.39/8.47 | 0.9997 | 107 | 97 | 5.0 |
| lactic acid | 6.0 ± 0.3 | 0.26/2.65 | 0.78/7.95 | 0.9997 | 90 | 75 | 4.9 |
| acetic acid | 502 ± 8 | 0.02/0.28 | 0.05/0.83 | 0.9988 | 97 | 106 | 1.5 |
| propionic acid | 64 ± 2 | 0.13/1.76 | 0.39/5.27 | 0.9961 | 110 | 105 | 3.2 |
| butyric acid | 5.7 ± 0.1 | 0.52/5.68 | 1.56/17.04 | 0.9956 | 100 | 101 | 1.9 |
| Method | Final Color | Redness | Greenness | Blueness | Brilliance (MB) |
|---|---|---|---|---|---|
| Isotachophoresis | White | 85.1% | 68.6% | 81.8% | 78.2% |
| UPLC-MS/MS | Gray (colorless) | 59.2% | 49.3% | 53.5% | 53.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrowolska-Iwanek, J.; Jamka-Kasprzyk, M.; Rusin, M.; Paśko, P.; Grekh, S.; Jurczak, A. Developed and Validated Capillary Isotachophoresis Method for the Rapid Determining Organic Acids in Children’s Saliva. Molecules 2023, 28, 1092. https://doi.org/10.3390/molecules28031092
Dobrowolska-Iwanek J, Jamka-Kasprzyk M, Rusin M, Paśko P, Grekh S, Jurczak A. Developed and Validated Capillary Isotachophoresis Method for the Rapid Determining Organic Acids in Children’s Saliva. Molecules. 2023; 28(3):1092. https://doi.org/10.3390/molecules28031092
Chicago/Turabian StyleDobrowolska-Iwanek, Justyna, Małgorzata Jamka-Kasprzyk, Marcelina Rusin, Paweł Paśko, Sviatoslav Grekh, and Anna Jurczak. 2023. "Developed and Validated Capillary Isotachophoresis Method for the Rapid Determining Organic Acids in Children’s Saliva" Molecules 28, no. 3: 1092. https://doi.org/10.3390/molecules28031092
APA StyleDobrowolska-Iwanek, J., Jamka-Kasprzyk, M., Rusin, M., Paśko, P., Grekh, S., & Jurczak, A. (2023). Developed and Validated Capillary Isotachophoresis Method for the Rapid Determining Organic Acids in Children’s Saliva. Molecules, 28(3), 1092. https://doi.org/10.3390/molecules28031092