Indian Hedgehog in Synovial Fluid Is a Novel Marker for Early Cartilage Lesions in Human Knee Joint


Abstract
:1. Introduction
2. Results
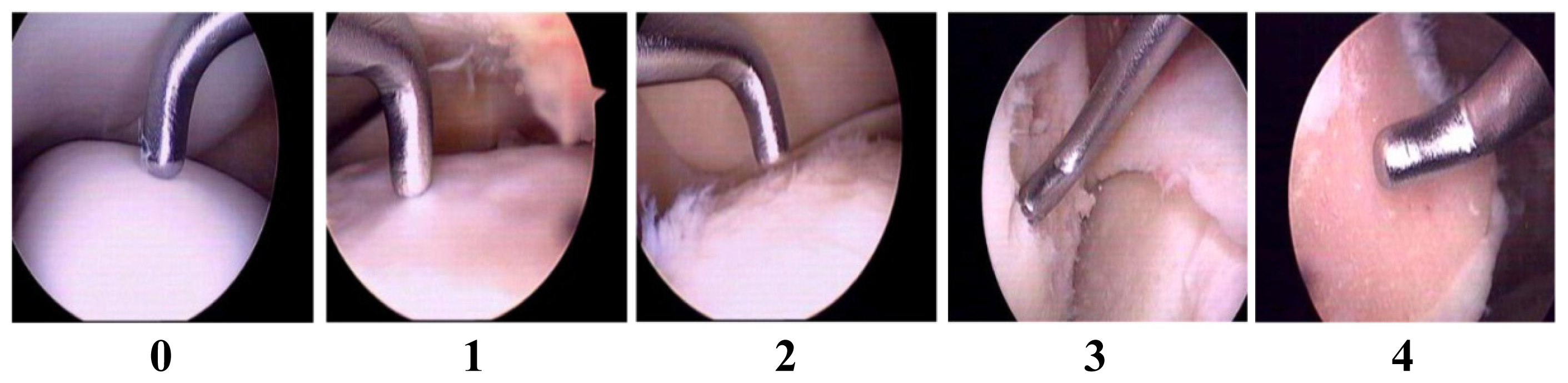
2.1. Validation of Articular Cartilage Lesions in Human Knee Joints Using the Outer-Bridge Scoring System
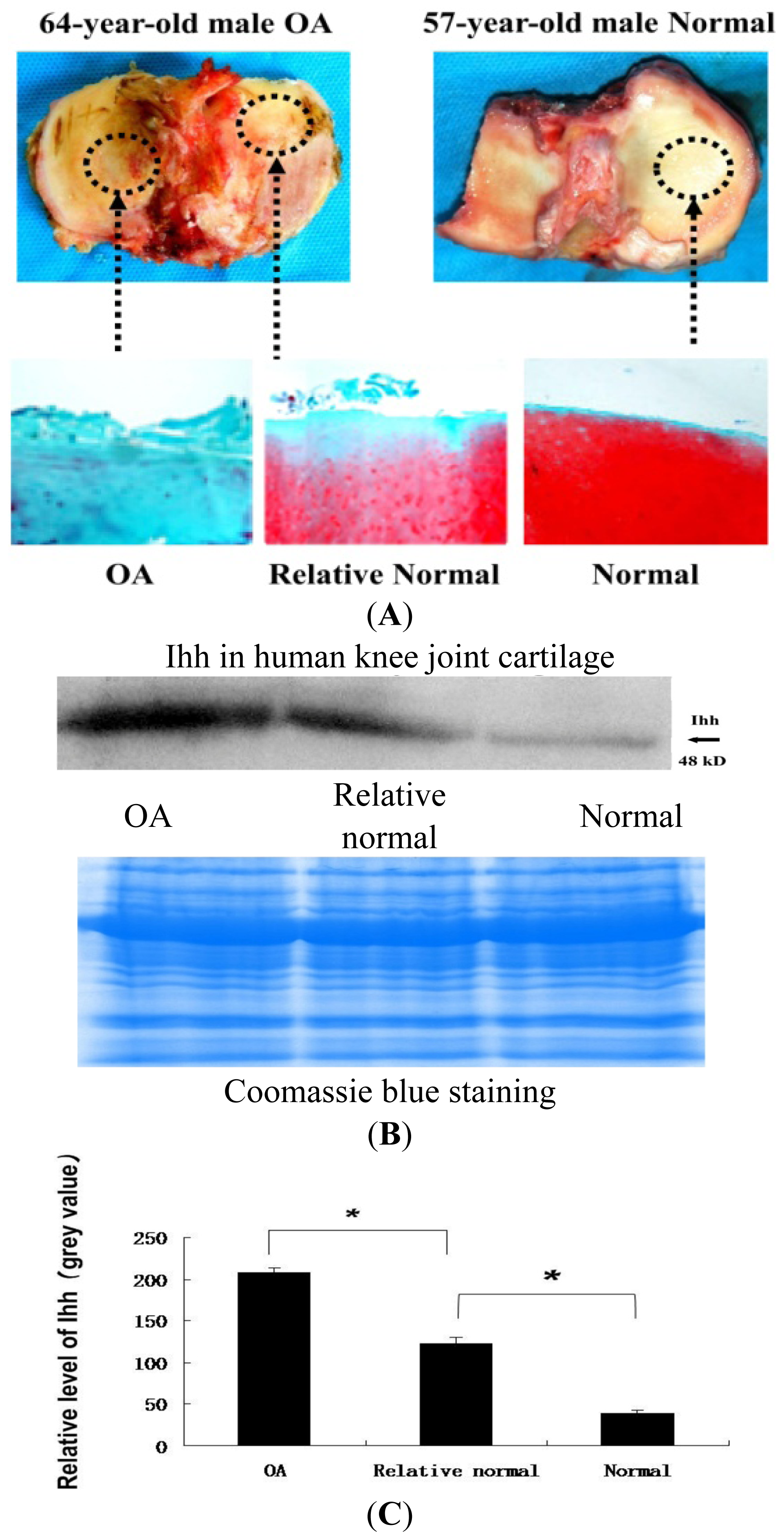
2.2. Increased Indian Hedgehog (Ihh) Expression in Human Osteoarthritis (OA) Cartilage Determined by Immunohistochemistry (IHC) and Western Blot Analysis
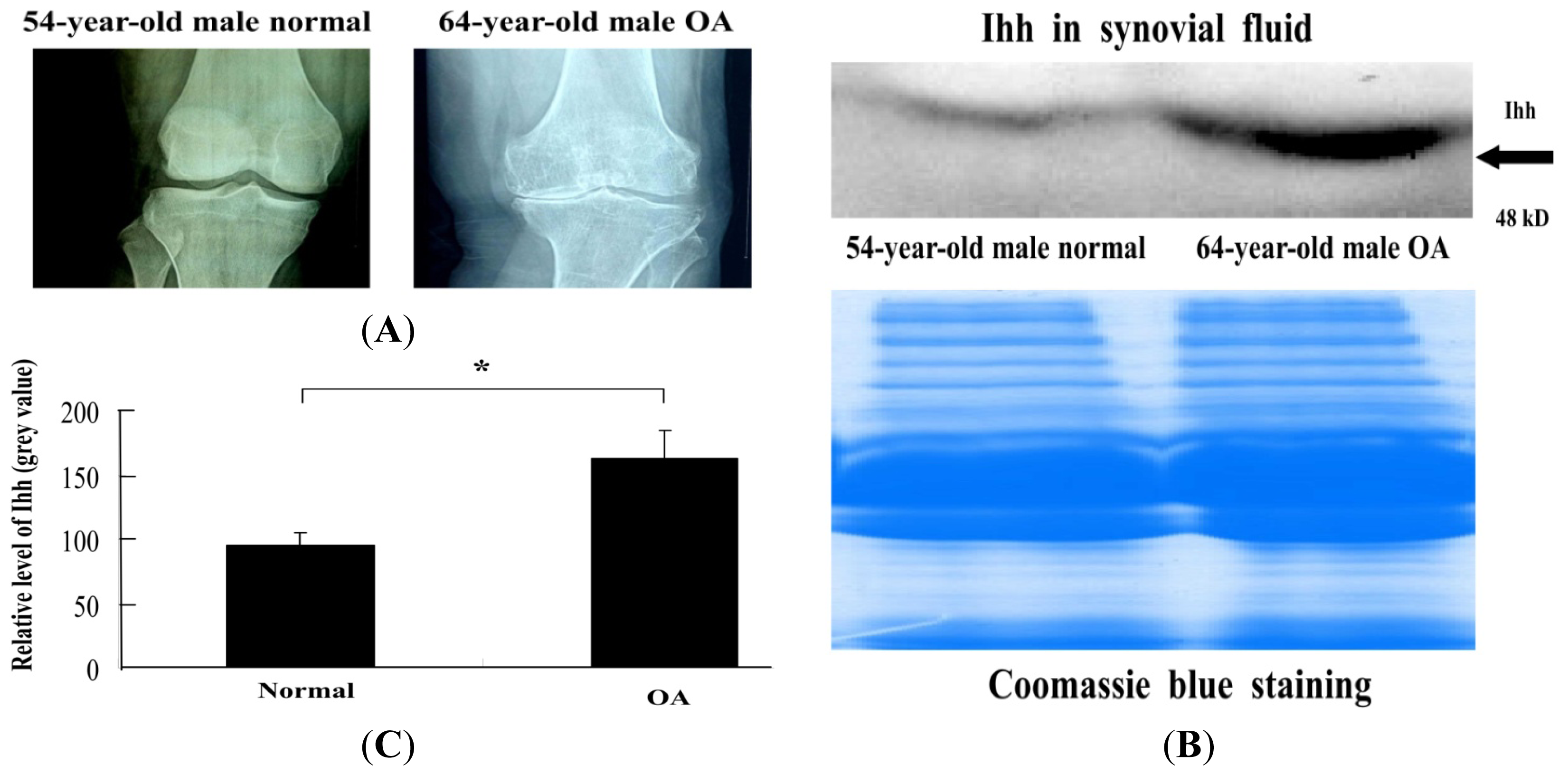
2.3. Increased Ihh Concentration in OA Synovial Fluid (SF) Determined by Western Blot
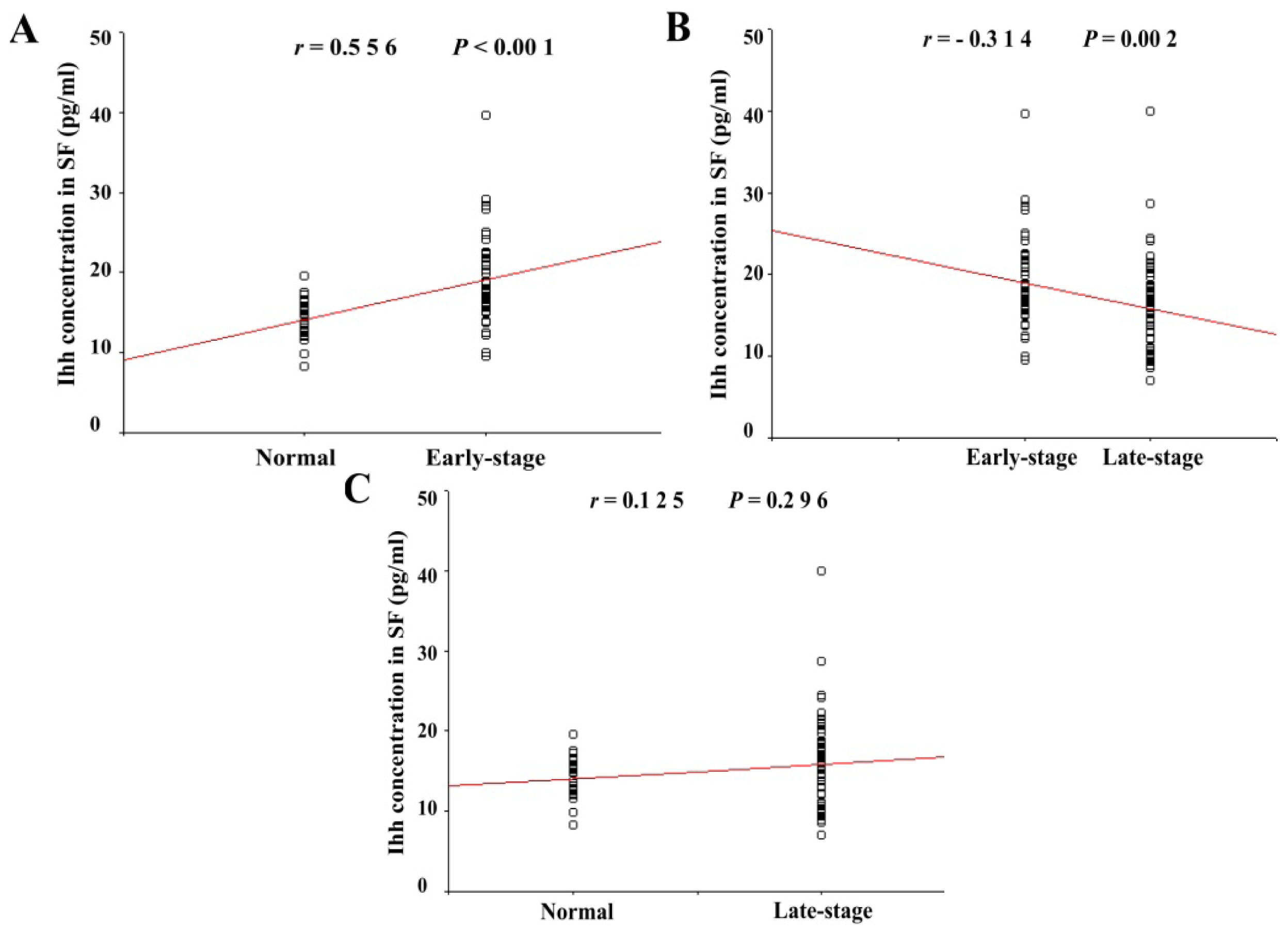
2.4. Ihh Concentration in SF Was Dependent on Cartilage Damage as Determined by the Maximal Outer-Bridge Score
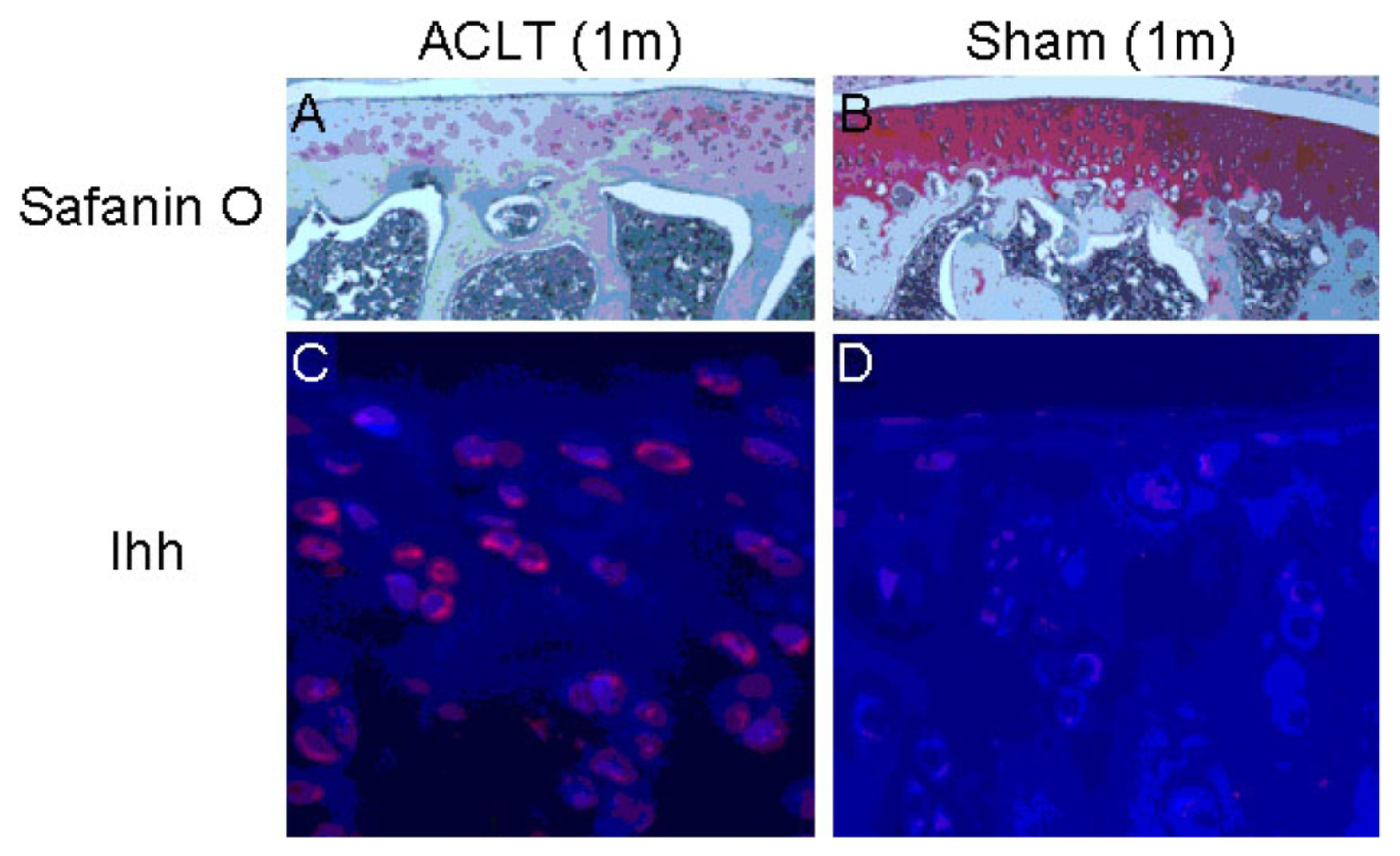
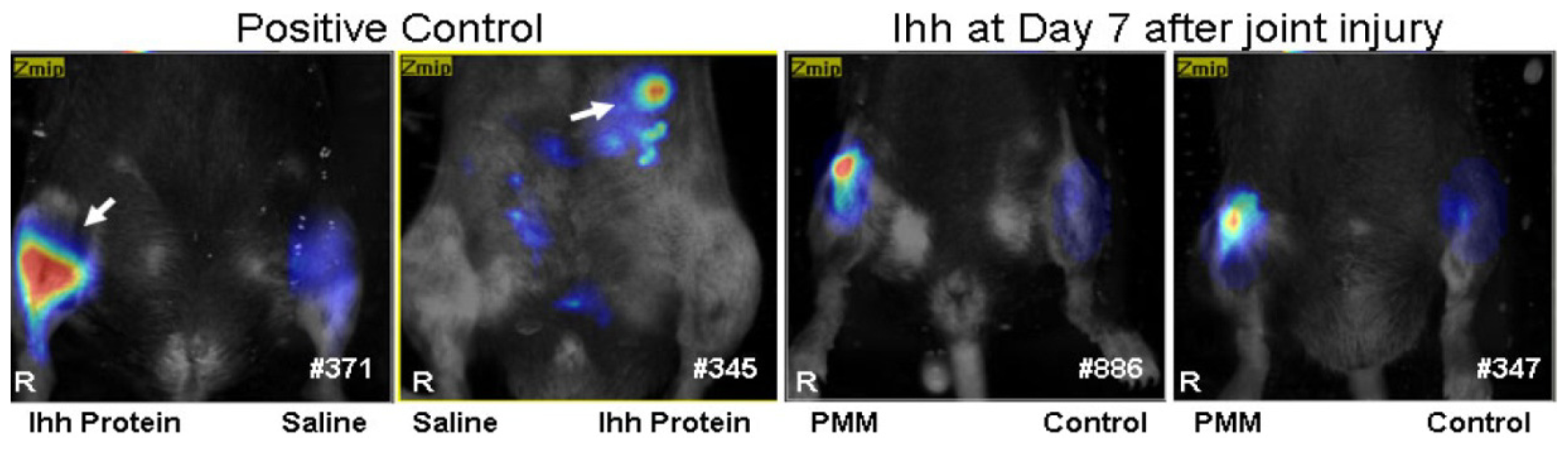
2.5. The Elevated Ihh Signal Was also Detected in Surgery-Induced OA Models
3. Discussion
4. Experimental Section
4.1. Enrollment of Patients
4.2. Cartilage Tissue Samples
4.3. Synovial Fluid Analysis
4.4. Animals
4.5. Histology
4.6. Immunohistochemistry (IHC)
4.7. Western Blot
4.8. Evaluation of Cartilage Damage
4.9. Measurement of Synovial Ihh
4.10. Fluorescence Molecular Tomography (FMT)
4.11. Statistical Analysis
5. Conclusions
Acknowledgments
Conflicts of Interest
- Author ContributionsCongming Zhang participated in the study design, wrote the manuscript, performed most of the experiments and analyzed data. Chongwei Chen, Kun Cao, Yongping Li, Qiang Jiao, Juan Ding, Jingming Zhou, performed some of the experiments and analyzed data. Xiaochun Wei, Chongwei Chen, Kun Cao, Yongping Li, Qiang Jiao, Juan Ding, Jingming Zhou, Braden C. Fleming, Qian Chen, Xianwen Shang participated in the interpretation of the data and/or revised the manuscript critically. Lei Wei conceived of the study, participated in its design, data analysis and revised the manuscript carefully and critically. All authors have read and approved the final manuscript.
References
- Eckstein, F.; Mosher, T.; Hunter, D. Imaging of knee osteoarthritis: Data beyond the beauty. Curr. Opin. Rheumatol 2007, 19, 435–443. [Google Scholar]
- Radin, E.L.; Rose, R.M. Role of subchondral bone in the initiation and progression of cartilage damage. Clin. Thop. Relat. Res 1986, 213, 34–40. [Google Scholar]
- Bauer, D.C.; Hunter, D.J.; Abramson, S.B.; Attur, M.; Corr, M.; Felson, D.; Heinegard, D.; Jordan, J.M.; Kepler, T.B.; Lane, N.E.; et al. Classification of osteoarthritis biomarkers: A proposed approach. Osteoarthr. Cartil 2006, 14, 723–727. [Google Scholar]
- Guermazi, A.; Hunter, D.J.; Roemer, F.W. Plain radiography and magnetic resonance imaging diagnostics in osteoarthritis: Validated staging and scoring. J. Bone Jt. Surg 2009, 91, 54–62. [Google Scholar]
- Kraus, V.B.; Burnett, B.; Coindreau, J.; Cottrell, S.; Eyre, D.; Gendreau, M.; Gardiner, J.; Garnero, P.; Hardin, J.; Henrotin, Y.; et al. Application of biomarkers in the development of drugs intended for the treatment of osteoarthritis. Osteoarthr. Cartil 2011, 19, 515–542. [Google Scholar]
- Aigner, T.; Reichenberger, E.; Bertling, W.; Kirsch, T.; Stoss, H.; von der Mark, K. Type X collagen expression in osteoarthritic and rheumatoid articular cartilage. Virchows Arch. B 1993, 63, 205–211. [Google Scholar]
- Aigner, T.; Soder, S.; Gebhard, P.M.; McAlinden, A.; Haag, J. Mechanisms of disease: Role of chondrocytes in the pathogenesis of osteoarthritis—Structure, chaos and senescence. Nat. Clin. Pract 2007, 3, 391–399. [Google Scholar]
- Hoyland, J.A.; Thomas, J.T.; Donn, R.; Marriott, A.; Ayad, S.; Boot-Handford, R.P.; Grant, M.E.; Freemont, A.J. Distribution of type X collagen mRNA in normal and osteoarthritic human cartilage. Bone Miner 1991, 15, 151–163. [Google Scholar]
- Slagboom, E.; Meulenbelt, I. Genetics of osteoarthritis: Early developmental clues to an old disease. Nat. Clin. Pract 2008, 4, 563. [Google Scholar]
- Von der Mark, K.; Kirsch, T.; Nerlich, A.; Kuss, A.; Weseloh, G.; Gluckert, K.; Stoss, H. Type X collagen synthesis in human osteoarthritic cartilage. Indication of chondrocyte hypertrophy. Arthritis Rheum 1992, 35, 806–811. [Google Scholar]
- Brew, C.J.; Clegg, P.D.; Boot-Handford, R.P.; Andrew, J.G.; Hardingham, T. Gene expression in human chondrocytes in late osteoarthritis is changed in both fibrillated and intact cartilage without evidence of generalised chondrocyte hypertrophy. Ann. Rheum. Dis 2010, 69, 234–240. [Google Scholar]
- Wang, X.; Manner, P.A.; Horner, A.; Shum, L.; Tuan, R.S.; Nuckolls, G.H. Regulation of MMP-13 expression by RUNX2 and FGF2 in osteoarthritic cartilage. Osteoarthr. Cartil 2004, 12, 963–973. [Google Scholar]
- Van der Kraan, P.M.; van den Berg, W.B. Chondrocyte hypertrophy and osteoarthritis: Role in initiation and progression of cartilage degeneration? Osteoarthr. Cartil 2012, 20, 223–232. [Google Scholar]
- Wei, F.; Zhou, J.; Wei, X.; Zhang, J.; Fleming, B.C.; Terek, R.; Pei, M.; Chen, Q.; Liu, T.; Wei, L. Activation of Indian hedgehog promotes chondrocyte hypertrophy and upregulation of MMP-13 in human osteoarthritic cartilage. Osteoarthr. Cartil 2012, 20, 755–763. [Google Scholar]
- Maeda, Y.; Nakamura, E.; Nguyen, M.T.; Suva, L.J.; Swain, F.L.; Razzaque, M.S.; Mackem, S.; Lanske, B. Indian hedgehog produced by postnatal chondrocytes is essential for maintaining a growth plate and trabecular bone. Proc. Natl. Acad. Sci. USA 2007, 104, 6382–6387. [Google Scholar]
- Wang, W.; Lian, N.; Li, L.; Moss, H.E.; Wang, W.; Perrien, D.S.; Elefteriou, F.; Yang, X. Atf4 regulates chondrocyte proliferation and differentiation during endochondral ossification by activating Ihh transcription. Development 2009, 136, 4143–4153. [Google Scholar]
- Beaupre, G.S.; Stevens, S.S.; Carter, D.R. Mechanobiology in the development, maintenance, and degeneration of articular cartilage. J. Rehabil. Res. Dev 2000, 37, 145–151. [Google Scholar]
- Lin, A.C.; Seeto, B.L.; Bartoszko, J.M.; Khoury, M.A.; Whetstone, H.; Ho, L.; Hsu, C.; Ali, S.A.; Alman, B.A. Modulating hedgehog signaling can attenuate the severity of osteoarthritis. Nat. Med 2009, 15, 1421–1425. [Google Scholar]
- Mak, K.K.; Kronenberg, H.M.; Chuang, P.T.; Mackem, S.; Yang, Y. Indian hedgehog signals independently of PTHrP to promote chondrocyte hypertrophy. Development 2008, 135, 1947–1956. [Google Scholar]
- Zhang, E.; Yan, X.; Zhang, M.; Chang, X.; Bai, Z.; He, Y.; Yuan, Z. Aggrecanases in the human synovial fluid at different stages of osteoarthritis. Clin. Rheumatol 2013, 32, 797–803. [Google Scholar]
- Elsaid, K.A.; Machan, J.T.; Waller, K.; Fleming, B.C.; Jay, G.D. The impact of anterior cruciate ligament injury on lubricin metabolism and the effect of inhibiting tumor necrosis factor alpha on chondroprotection in an animal model. Arthritis Rheum 2009, 60, 2997–3006. [Google Scholar]
- Jay, G.D.; Fleming, B.C.; Watkins, B.A.; McHugh, K.A.; Anderson, S.C.; Zhang, L.X.; Teeple, E.; Waller, K.A.; Elsaid, K.A. Prevention of cartilage degeneration and restoration of chondroprotection by lubricin tribosupplementation in the rat following anterior cruciate ligament transection. Arthritis Rheum 2010, 62, 2382–2391. [Google Scholar]
- Bedson, J.; Croft, P.R. The discordance between clinical and radiographic knee osteoarthritis: A systematic search and summary of the literature. BMC Musculoskelet. Disord 2008, 9, 116. [Google Scholar]
- Thomas, E.; Peat, G.; Mallen, C.; Wood, L.; Lacey, R.; Duncan, R.; Croft, P. Predicting the course of functional limitation among older adults with knee pain: Do local signs, symptoms and radiographs add anything to general indicators? Ann. Rheum. Dis 2008, 67, 1390–1398. [Google Scholar]
- Wood, L.; Peat, G.; Thomas, E.; Hay, E.M.; Sim, J. Associations between physical examination and self-reported physical function in older community-dwelling adults with knee pain. Phys. Ther 2008, 88, 33–42. [Google Scholar]
- Blanke, M.; Carl, H.D.; Klinger, P.; Swoboda, B.; Hennig, F.; Gelse, K. Transplanted chondrocytes inhibit endochondral ossification within cartilage repair tissue. Calcif. Tissue Int 2009, 85, 421–433. [Google Scholar]
- Drissi, H.; Zuscik, M.; Rosier, R.; O’Keefe, R. Transcriptional regulation of chondrocyte maturation: Potential involvement of transcription factors in OA pathogenesis. Mol. Asp. Med 2005, 26, 169–179. [Google Scholar]
- Tchetina, E.V.; Squires, G.; Poole, A.R. Increased type II collagen degradation and very early focal cartilage degeneration is associated with upregulation of chondrocyte differentiation related genes in early human articular cartilage lesions. J. Rheumatol 2005, 32, 876–886. [Google Scholar]
- Zhou, J.; Chen, Q.; Lanske, B.; Fleming, B.C.; Terek, R.; Wei, X.; Zhang, G.; Wang, S.; Li, K.; Wei, L. Disrupting the Indian hedgehog signaling pathway in vivo attenuates surgically induced osteoarthritis progression in Col2a1-CreERT2; Ihhfl/fl mice. Arthritis Res. Ther 2014, 16, R11. [Google Scholar]
- Scharstuhl, A.; Glansbeek, H.L.; van Beuningen, H.M.; Vitters, E.L.; van der Kraan, P.M.; van den Berg, W.B. Inhibition of endogenous TGF-β during experimental osteoarthritis prevents osteophyte formation and impairs cartilage repair. J. Immunol 2002, 169, 507–514. [Google Scholar]
- Long, F.; Ornitz, D.M. Development of the endochondral skeleton. Cold Spring Harb. Perspect. Biol 2013, 5, a008334. [Google Scholar]
- Adams, C.S.; Horton, W.E., Jr. Chondrocyte apoptosis increases with age in the articular cartilage of adult animals. Anat. Rec 1998, 250, 418–425. [Google Scholar]
- Hashimoto, S.; Ochs, R.L.; Rosen, F.; Quach, J.; McCabe, G.; Solan, J.; Seegmiller, J.E.; Terkeltaub, R.; Lotz, M. Chondrocyte-derived apoptotic bodies and calcification of articular cartilage. Proc. Natl. Acad. Sci. USA 1998, 95, 3094–3099. [Google Scholar]
- Jimenez, P.A.; Glasson, S.S.; Trubetskoy, O.V.; Haimes, H.B. Spontaneous osteoarthritis in Dunkin Hartley guinea pigs: Histologic, radiologic, and biochemical changes. Lab. Anim. Sci 1997, 47, 598–601. [Google Scholar]
- Mobasheri, A. Role of chondrocyte death and hypocellularity in ageing human articular cartilage and the pathogenesis of osteoarthritis. Med. Hypotheses 2002, 58, 193–197. [Google Scholar]
- Todd Allen, R.; Robertson, C.M.; Harwood, F.L.; Sasho, T.; Williams, S.K.; Pomerleau, A.C.; Amiel, D. Characterization of mature vs. aged rabbit articular cartilage: Analysis of cell density, apoptosis-related gene expression and mechanisms controlling chondrocyte apoptosis. Osteoarthr. Cartil 2004, 12, 917–923. [Google Scholar]
- Yatsugi, N.; Tsukazaki, T.; Osaki, M.; Koji, T.; Yamashita, S.; Shindo, H. Apoptosis of articular chondrocytes in rheumatoid arthritis and osteoarthritis: Correlation of apoptosis with degree of cartilage destruction and expression of apoptosis-related proteins of p53 and c-myc. J. Orthop. Sci 2000, 5, 150–156. [Google Scholar]
- Wu, C.W.; Morrell, M.R.; Heinze, E.; Concoff, A.L.; Wollaston, S.J.; Arnold, E.L.; Singh, R.; Charles, C.; Skovrun, M.L.; FitzGerald, J.D.; et al. Validation of American College of Rheumatology classification criteria for knee osteoarthritis using arthroscopically defined cartilage damage scores. Semin. Arthritis Rheum 2005, 35, 197–201. [Google Scholar]
- Cameron, M.L.; Briggs, K.K.; Steadman, J.R. Reproducibility and reliability of the outer-bridge classification for grading chondral lesions of the knee arthroscopically. Am. J. Sports Med 2003, 31, 83–86. [Google Scholar]
- Ntziachristos, V.; Bremer, C.; Weissleder, R. Fluorescence imaging with near-infrared light: New technological advances that enable in vivo molecular imaging. Eur. Radiol 2003, 13, 195–208. [Google Scholar]
- Peterson, J.D.; Labranche, T.P.; Vasquez, K.O.; Kossodo, S.; Melton, M.; Rader, R.; Listello, J.T.; Abrams, M.A.; Misko, T.P. Optical tomographic imaging discriminates between disease-modifying anti-rheumatic drug (DMARD) and non-DMARD efficacy in collagen antibody-induced arthritis. Arthritis Res. Ther 2010, 12, R105. [Google Scholar]
- Vinegoni, C.; Razansky, D.; Pitsouli, C.; Perrimon, N.; Ntziachristos, V.; Weissleder, R. Mesoscopic fluorescence tomography for in vivo imaging of developing Drosophila. J. Vis. Exp 2009, 2009. [Google Scholar] [CrossRef]
- Weissleder, R.; Ntziachristos, V. Shedding light onto live molecular targets. Nat. Med 2003, 9, 123–128. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group (Based on Outer-Bridge Score) | Ihh Concentration (pg/mL) | n |
|---|---|---|
| Normal Group | 14.04 ± 2.55 | 25 |
| Early stage Group | 19.03 ± 5.2 | 50 |
| Late stage Group | 15.16 ± 6.28 | 47 |
| Total | 122 | |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhang, C.; Wei, X.; Chen, C.; Cao, K.; Li, Y.; Jiao, Q.; Ding, J.; Zhou, J.; Fleming, B.C.; Chen, Q.; et al. Indian Hedgehog in Synovial Fluid Is a Novel Marker for Early Cartilage Lesions in Human Knee Joint. Int. J. Mol. Sci. 2014, 15, 7250-7265. https://doi.org/10.3390/ijms15057250
Zhang C, Wei X, Chen C, Cao K, Li Y, Jiao Q, Ding J, Zhou J, Fleming BC, Chen Q, et al. Indian Hedgehog in Synovial Fluid Is a Novel Marker for Early Cartilage Lesions in Human Knee Joint. International Journal of Molecular Sciences. 2014; 15(5):7250-7265. https://doi.org/10.3390/ijms15057250
Chicago/Turabian StyleZhang, Congming, Xiaochun Wei, Chongwei Chen, Kun Cao, Yongping Li, Qiang Jiao, Juan Ding, Jingming Zhou, Braden C. Fleming, Qian Chen, and et al. 2014. "Indian Hedgehog in Synovial Fluid Is a Novel Marker for Early Cartilage Lesions in Human Knee Joint" International Journal of Molecular Sciences 15, no. 5: 7250-7265. https://doi.org/10.3390/ijms15057250
APA StyleZhang, C., Wei, X., Chen, C., Cao, K., Li, Y., Jiao, Q., Ding, J., Zhou, J., Fleming, B. C., Chen, Q., Shang, X., & Wei, L. (2014). Indian Hedgehog in Synovial Fluid Is a Novel Marker for Early Cartilage Lesions in Human Knee Joint. International Journal of Molecular Sciences, 15(5), 7250-7265. https://doi.org/10.3390/ijms15057250