
Fatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty Acids

 ,
,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Fatty Acids Composition of Vegetable Oils

{kind=link}
{kind=link}
{kind=link}
| FAs [%] | SAF | GRP | SIL | HMP | SFL | WHG | PMS | SES | RB | ALM | RPS | PNT | OL | COC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C6:0 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | 0.52 |
| C8:0 | nd | 0.01 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | 7.6 |
| C10:0 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | 0.01 | nd | nd | 5.5 |
| C12:0 | nd | 0.01 | 0.01 | nd | 0.02 | 0.07 | nd | nd | nd | 0.09 | nd | nd | nd | 47.7 |
| C14:0 | 0.10 | 0.05 | 0.09 | 0.07 | 0.09 | nd | 0.17 | nd | 0.39 | 0.07 | nd | 0.04 | nd | 19.9 |
| C15:0 | nd | 0.01 | 0.02 | nd | nd | 0.04 | nd | nd | nd | nd | 0.02 | nd | nd | nd |
| C16:0 | 6.7 | 6.6 | 7.9 | 6.4 | 6.2 | 17.4 | 13.1 | 9.7 | 20.0 | 6.8 | 4.6 | 7.5 | 16.5 | nd |
| C17:0 | 0.04 | 0.06 | 0.06 | 0.05 | 0.02 | 0.03 | 0.13 | nd | nd | 0.05 | 0.04 | 0.07 | nd | nd |
| C18:0 | 2.4 | 3.5 | 4.5 | 2.6 | 2.8 | 0.7 | 5.7 | 6.5 | 2.1 | 2.3 | 1.7 | 2.1 | 2.3 | 2.7 |
| C20:0 | nd | 0.16 | 2.6 | nd | 0.21 | nd | 0.47 | 0.63 | nd | 0.09 | nd | 1.01 | 0.43 | nd |
| C22:0 | nd | nd | nd | nd | nd | nd | nd | 0.14 | nd | nd | nd | nd | 0.15 | nd |
| C16:1 (n-7) | 0.08 | 0.08 | 0.05 | 0.11 | 0.12 | 0.21 | 0.12 | 0.11 | 0.19 | 0.53 | 0.21 | 0.07 | 1.8 | nd |
| C17:1 (n-7) | nd | nd | 0.03 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| C18:1cis (n-9) | 11.5 | 14.3 | 20.4 | 11.5 | 28.0 | 12.7 | 24.9 | 41.5 | 42.7 | 67.2 | 63.3 | 71.1 | 66.4 | 6.2 |
| C18:1trans (n-9) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | 0.14 | nd | nd | nd |
| C20:1(n-9) | nd | 0.40 | 0.15 | 16.5 | 0.18 | 7.91 | 1.08 | 0.32 | 1.11 | 0.16 | 9.1 | nd | 0.30 | nd |
| C18:2cis (n-6) | 79.0 | 74.7 | 63.3 | 59.4 | 62.2 | 59.7 | 54.2 | 40.9 | 33.1 | 22.8 | 19.6 | 18.2 | 16.4 | 1.6 |
| C18:3 (n-3) | 0.15 | 0.15 | 0.88 | 0.36 | 0.16 | 1.2 | 0.12 | 0.21 | 0.45 | nd | 1.2 | nd | 1.6 | nd |
| C18:3 (n-6) | nd | nd | nd | 3.0 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| SFAs | 9.3 | 10.4 | 15.1 | 9.2 | 9.4 | 18.2 | 19.6 | 16.9 | 22.5 | 9.3 | 6.3 | 10.7 | 19.4 | 92.1 |
| MUFAs | 11.6 | 14.8 | 20.7 | 28.1 | 28.3 | 20.9 | 26.1 | 42.0 | 44.0 | 67.9 | 72.8 | 71.1 | 68.2 | 6.2 |
| PUFAs | 79.1 | 74.9 | 64.2 | 62.8 | 62.4 | 61.0 | 54.3 | 41.2 | 33.6 | 22.8 | 20.9 | 18.2 | 18.0 | 1.6 |
| n-3 PUFAs | 0.2 | 0.2 | 0.9 | 0.4 | 0.2 | 1.2 | 0.1 | 0.2 | 0.5 | 0.0 | 1.2 | 0.0 | 1.6 | 0.0 |
| n-6 PUFAs | 79.0 | 74.7 | 63.3 | 62.4 | 62.2 | 59.7 | 54.2 | 40.9 | 33.1 | 22.8 | 19.6 | 18.2 | 16.4 | 1.6 |
2.1.1. Saturated Fatty Acids (SFAs)
2.1.2. Monounsaturated Fatty Acids (MUFAs)
2.1.3. Polyunsaturated Fatty Acids (PUFAs)
2.2. Contribution of Fatty Acid Groups of Vegetable Oils to Energy Daily Intake
| E (kJ/g) | SAF | GRP | SIL | HMP | SFL | WHG | PMS | SES | RB | ALM | RPS | PNT | OL | COC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SFAs | 2.9 | 2.6 | 5.0 | 3.0 | 4.7 | 4.1 | 4.6 | 3.5 | 6.2 | 2.1 | 4.4 | 3.2 | 0.7 | 26.2 |
| MUFAs | 3.7 | 3.8 | 6.0 | 9.5 | 14.6 | 4.8 | 8.9 | 8.1 | 12.3 | 16.4 | 47.4 | 22.0 | 2.6 | 1.7 |
| PUFAs | 26.0 | 19.7 | 19.0 | 21.1 | 32.6 | 14.2 | 12.5 | 9.4 | 9.4 | 5.5 | 13.6 | 5.7 | 0.7 | 0.4 |
| n-3 PUFAs | 0.1 | 0.0 | 0.4 | 0.1 | 0.1 | 0.3 | 0.0 | 0.0 | 0.1 | 0.0 | 0.9 | 0.0 | 0.0 | 0.0 |
| n-6 PUFAs | 25.9 | 19.6 | 18.6 | 20.9 | 32.5 | 13.9 | 12.4 | 9.4 | 9.3 | 5.5 | 12.8 | 5.7 | 0.1 | 0.4 |
| E [% ERDI] | SAF | GRP | SIL | HMP | SFL | WHG | PMS | SES | RB | ALM | RPS | PNT | OL | COC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SFAs | 77.2 | 69.9 | 132.2 | 78.5 | 124.9 | 107.5 | 121.3 | 93.9 | 163.4 | 56.7 | 116.2 | 84.2 | 19.4 | 695.7 |
| PUFAs | 626.3 | 474.5 | 457.1 | 507.9 | 786.8 | 342.3 | 300.9 | 226.9 | 227.2 | 132.7 | 329.1 | 137.4 | 16.4 | 10.6 |
| n-3 PUFAs | 6.7 | 5.5 | 47.8 | 17.0 | 11.2 | 41.1 | 5.0 | 4.4 | 17.6 | 0.0 | 117.1 | 0.0 | 0.0 | 0.0 |
| n-6 PUFAs | 764.0 | 578.7 | 547.6 | 617.0 | 959.2 | 409.3 | 366.6 | 276.4 | 273.8 | 162.2 | 376.2 | 167.9 | 1.8 | 13.0 |
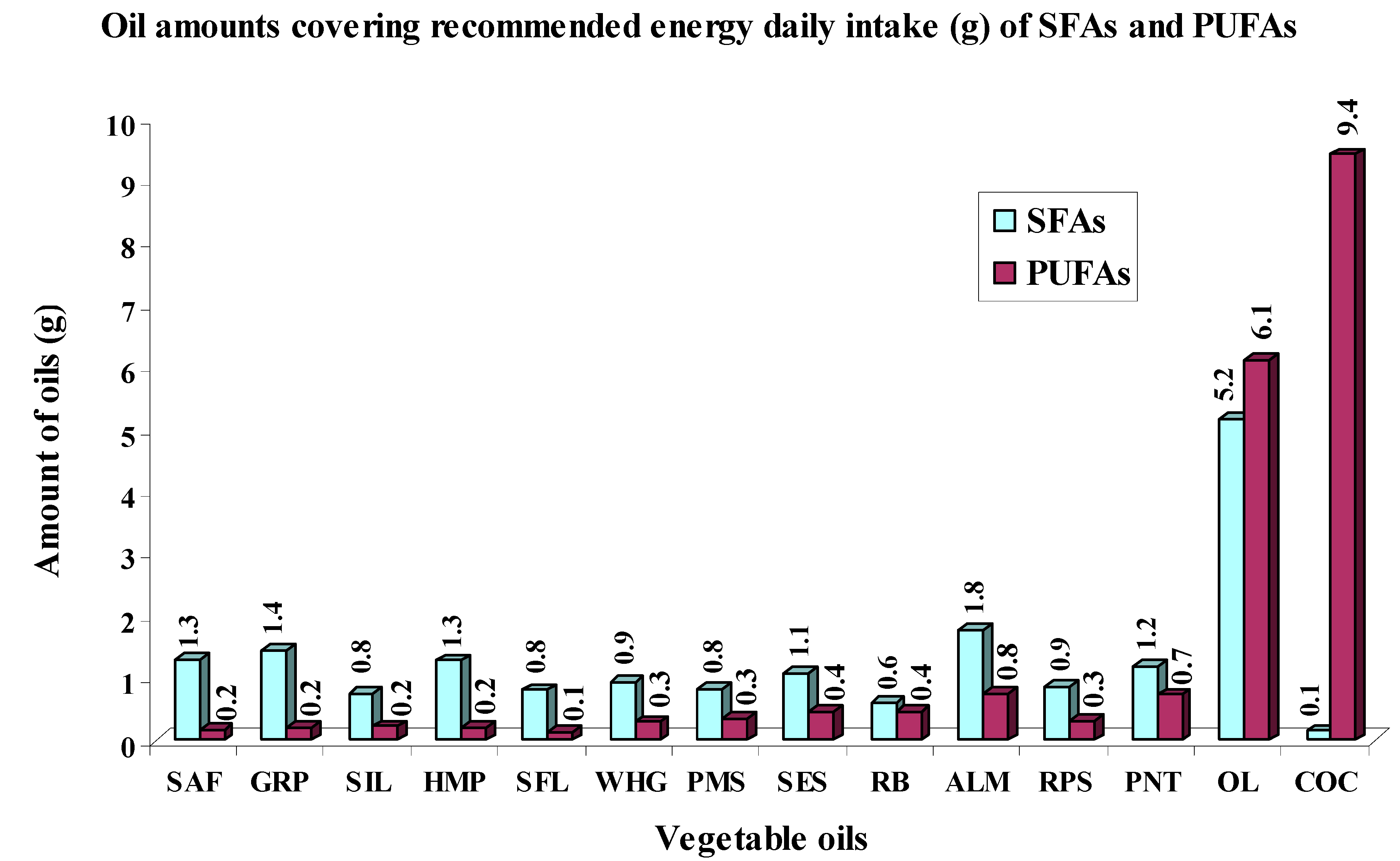
2.3. Oil Amounts Covering Recommended Daily Intakes of SFAs, PUFAs, n-3 and n-6 PUFAs


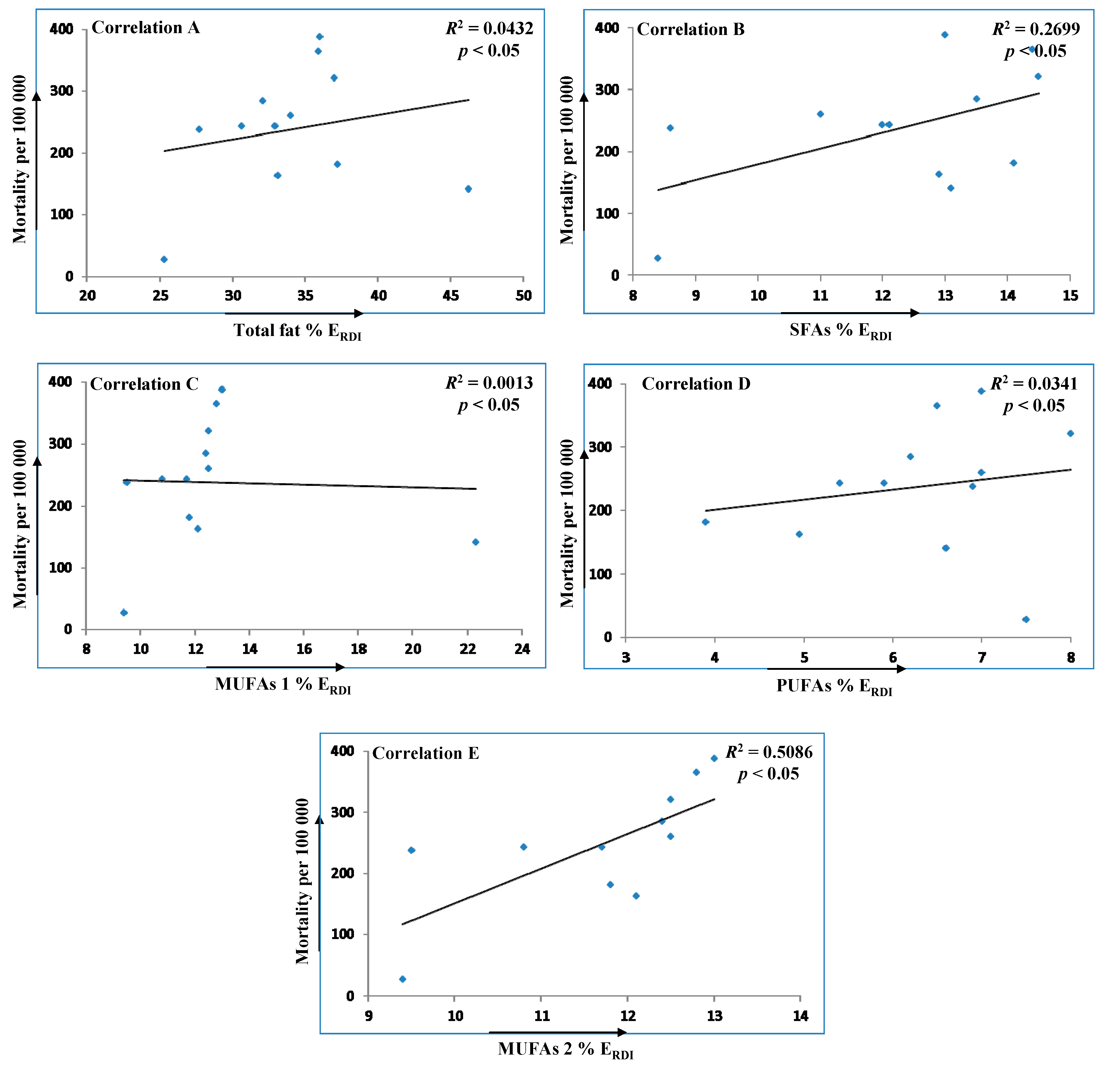
2.4. Statistical Evaluation of Impact of Fat Dietary Intake on the Number of CHD and CVD Mortality in Various Countries
| Country | CHD + Other CVD Mortality Per 100,000 1 | Total Fats | SFAs | MUFAs | PUFAs |
|---|---|---|---|---|---|
| (% ERDI) 2 | |||||
| Czech Republic | 388.27 | 36.0 | 13.0 | 13.0 | 7.0 |
| Germany | 364.75 | 35.9 | 14.4 | 12.8 | 6.5 |
| Austria | 320.92 | 37.0 | 14.5 | 12.5 | 8.0 |
| Finland | 284.69 | 32.1 | 13.5 | 12.4 | 6.2 |
| USA | 260.58 | 34.0 | 11.0 | 12.5 | 7.0 |
| United Kingdom | 243.45 | 32.9 | 12.0 | 11.7 | 5.9 |
| Norway | 242.72 | 30.6 | 12.1 | 10.8 | 5.4 |
| Republic of South Africa | 237.45 | 27.7 | 8.6 | 9.5 | 6.9 |
| France | 181.40 | 37.2 | 14.1 | 11.8 | 3.9 |
| Australia, New Zealand | 162.44 | 33.1 | 12.9 | 12.1 | 5.0 |
| Greece | 141.04 | 46.2 | 13.1 | 22.3 | 6.6 |
| Japan | 28.00 | 25.3 | 8.4 | 9.4 | 7.5 |

3. Experimental Section
3.1. Samples
| Oils | Samples | Plant Sources | Technological Process |
|---|---|---|---|
| Grape | GRP | Vitis vinifera | - |
| Peanut | PNT | Arachis hypogaea | - |
| Rapeseed | RPS | Brassica napus | Cold drawn |
| Sunflower | SFL | Helianthus annuus | Cold drawn |
| Safflower | SAF | Carthamus tinctorius | Cold drawn |
| Almond | ALM | Amygdalus communis | Cold drawn |
| Wheat germ | WHG | Triticum aestivum | Cold drawn |
| Sesame | SES | Sesamum indicum | Cold drawn |
| Pumpkin seed | PMS | Cucurbita pepo | Cold drawn |
| Rice brain | RB | Oryza sativa | - |
| Silybum marianum | SIL | Silybum marianum | Cold drawn |
| Coconut | COC | Cocos nucifera | - |
| Hemp | HMP | Cannabis sativa | Cold drawn |
| Olive | OL | Olea europaea | Cold drawn |
3.2. Standards and Reagents
3.3. Preparation of FAMEs
3.4. GC Analysis of FAMEs
3.5. Determination of Energy Contribution of Fatty Acid Groups of Vegetable Oils
3.6. Statistical Evaluation of Impact of Fat Dietary Intake on the Number of CHD and CVD Mortality in Various Countries
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mišurcová, L.; Vávra Ambrožová, J.; Samek, D. Seaweed lipids as nutraceuticals. Adv. Food Nutr. Res. 2011, 64, 339–355. [Google Scholar] [PubMed]
- Brenna, J.T. Efficiency of conversion of α-linolenic acid to long chain n-3 fatty acids in man. Curr. Opin. Clin. Nutr. 2002, 5, 127–132. [Google Scholar] [CrossRef]
- Burdge, G.C.; Calder, P.C. Conversion of α-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod. Nutr. Dev. 2005, 45, 581–597. [Google Scholar] [CrossRef] [PubMed]
- Burdge, G.C.; Wootton, S.A. Conversion of eicoapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. Br. J. Nutr. 2002, 88, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Brenna, J.T.; Salem, J.N.; Sinclair, A.J.; Cunnane, S.C. α-Linolenic acid supplementation and conversion to n-3 long-chain polyunsaturated fatty acids in humans. Prostaglandins Leukot. Essent. Fat. Acids 2009, 80, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Huang, Ch.; Freter, C. Lipid metabolism, apoptosis and cancer therapy. Int. J. Mol. Sci. 2015, 16, 924–949. [Google Scholar] [CrossRef] [PubMed]
- Gatek, J.; Vrana, D.; Melichar, B.; Vazan, P.; Kotocova, K.; Kotoc, J.; Dudesek, B.; Hnatek, L.; Duben, J. Significance of the resection margin and risk factors for close or positive resection margin in patients undergoing breast-conserving surgery. J. BUON 2012, 17, 452–456. [Google Scholar] [PubMed]
- Simmons, G.E.; Pruitt, W.M.; Pruitt, K. Diverse roles of SIRT1 in cancer biology and lipid metabolism. Int. J. Mol. Sci. 2015, 16, 950–965. [Google Scholar] [CrossRef] [PubMed]
- Gatek, J.; Vrana, D.; Hnatek, L.; Bakala, J.; Dudesek, B.; Duben, J.; Musil, T. Sentinel node biopsy and neoadjuvant chemotherapy in the treatment of breast cancer. J. BUON 2012, 17, 265–270. [Google Scholar] [PubMed]
- Proust, F.; Lucas, M.; Deawailly, É. Fatty acid profiles among the Inuit of Nunavi: Current status and temporal change. Prostaglandins Leukot. Essent. Fat. Acids 2014, 90, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Bozza, P.T.; Viola, J.P.B. Lipid droplets in inflammation and cancer. Prostaglandins Leukot. Essent. Fat. Acids 2014, 90, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Gard, M.L.; Thomson, A.B.R.; Clandinin, M.T. Effect of dietary cholesterol and/or ω3 fatty acids on lipid composition and ∆5-desaturase activity of rat liver microsomes. J. Nutr. 1988, 118, 661–668. [Google Scholar]
- Brenner, R.R.; Bernasconi, A.M.; González, M.S.; Rimoldi, O.J. Dietary cholesterol modulates ∆6 and ∆9 desaturase mRNAs and enzymatic activity in rats fed a low-EFA diet. Lipids 2002, 37, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Landau, J.M.; Sekowski, A.; Hamm, M.W. Dietary cholesterol and the activity of stearoyl CoA desaturase in rats: Evidence for an indirect regulatory effect. Biochim. Biophys. Acta 1997, 3, 349–357. [Google Scholar] [CrossRef]
- FAO/WHO. Fats and Fatty Acids in Human Nutrition. Report of an Expert Consultation; FAO/WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Tvrzická, E.; Staňková, B.; Vecka, M.; Žák, A. Fatty acids 1. Occurrence and biological significance. (In Czech)Cas. Lek. Cesk. 2009, 148, 16–24. [Google Scholar] [PubMed]
- Flachs, P.; Horakova, O.; Brauner, P.; Rossmeisl, M.; Pecina, P.; Franssen-van Hal, N.; Ruzickova, J.; Sponarova, J.; Drahota, Z.; Vlcek, C.; et al. Polyunsaturated fatty acids of marine origin upregulate mitochondrial biogenesis and induce β-oxidation in white fat. Diabetologia 2005, 48, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, J.E.; Lokesh, B.; Stone, R.A. Dietary n-3 polyunsaturated fatty acids and amelioration of cardiovascular disease: Possible mechanisms. Am. J. Clin. Nutr. 1990, 52, 1–28. [Google Scholar] [PubMed]
- Weiss, L.A.; Barrett-Connor, E.; von Mühlen, D. Ratio of n-6 to n-3 fatty acids and bone mineral density in older adults: The Rancho Bernardo Study. Am. J. Clin. Nutr. 2005, 81, 934–938. [Google Scholar] [PubMed]
- Hu, F.B.; Manson, J.A.E.; Willett, W.C. Types of dietary fat and risk of coronary heart disease: A critical review. J. Am. Coll. Nutr. 2001, 20, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Mobraten, K.; Haug, T.M.; Kleiveland, C.R.; Lea, T. Omega-3 and omega-6 PUFAs induce the same GPR120-mediated signaling events, but with different kinetics and intensity in Caco-2 cells. Lipids Health Dis. 2013, 12, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Salem, J.; Vandal, M.N.; Calon, F. The benefit of docosahexaenoic acid for the adult brain in aging and dementia. Prostaglandins Leukot. Essent. Fat. Acids 2015, 92, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, C.; Mann, J.D.; Faurot, K.R.; Lynch, C.; Imam, S.T.; MacIntosh, B.A.; Hibbeln, J.R.; Loewke, J.; Smith, S.; Coble, R.; et al. Low omega-6 vs. low omega-6 plus high omega-3 dietary intervention for Chronic Daily headache: Protocol for a randomized clinical trial. Trials 2011, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Puri, B.K.; Martins, J.G. Which polyunsaturated fatty acids are active in children with attention-deficit hyperactivity disorder receiving PUFA supplementation? A fatty acid validated meta-regression analysis of randomized controlled trials. Prostaglandins Leukot. Essent. Fat. Acids 2014, 90, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. Omega-3 fatty acids in inflammation and autoimmune diseases. J. Am. Coll. Nutr. 2002, 21, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Grieger, J.A.; Etherton, T.D. Dietary reference intakes for DHA and EPA. Prostaglandins Leukot. Essent. Fat. Acids 2009, 81, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Maehre, H.K.; Malde, M.K.; Eilertsen, K.E.; Elvevoll, E.O. Characterization of protein, lipid and mineral contents in common Norwegian seaweeds and evaluation of their potential as food and feed. J. Sci. Food Agric. 2014, 94, 3281–3290. [Google Scholar] [CrossRef] [PubMed]
- Hertting, G.; Seregi, A. Formation and function of eicosanoids in the central nervous system. Ann. N. Y. Acad. Sci. 1989, 559, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Pokorný, J.; Dubská, L. Technology of Lipids; (In Czech). Publisher of Technical Literature: Praque, Czech Republic, 1986; pp. 1–452. [Google Scholar]
- Zambiazi, R.C.; Przybylski, R.; Zambiazi, M.W.; Mendonca, C.B. Fatty acid composition of vegetable oils and fats. B. CEPPA Curitiba 2007, 25, 111–120. [Google Scholar]
- Kostik, V.; Memeti, S.; Bauer, B. Fatty acid composition of edible oils and fats. J. Hyg. Eng. Des. 2013, 4, 112–116. [Google Scholar]
- Rajah, K.K. Fats in Food Technology; Sheffield Academic Press: Sheffield, UK, 2002; pp. 1–379. [Google Scholar]
- Alfawaz, M.A. Chemical composition and oil characteristics of pumpkin (Cucurbita maxima) seed kernels. Food Sci. Agric. Res. Center 2004, 129, 5–18. [Google Scholar]
- Fathi-Achachlouei, B.; Azadmard-Damirchi, S. Milk thistle seed oil constituents from different varieties grown in Iran. J. Am. Oil Chem. Soc. 2009, 86, 643–649. [Google Scholar] [CrossRef]
- El-Mallah, M.H.; El-Shami, S.M.; Hassanein, M.M. Detailed studies on some lipids of Silybum marianum(L.) seed oil. Grasas Aceites 2003, 54, 397–402. [Google Scholar]
- Kamal-Eldin, A.; Anderson, R. A multivariate study of the correlation between tocopherol content and fatty acid composition in vegetable oils. J. Am. Oil Chem. Soc. 1997, 74, 375–380. [Google Scholar] [CrossRef]
- Denke, M.A.; Grundy, S.M. Comparison of effects of lauric acid and palmitic acid on plasma lipids and lipoproteins. Am. J. Clin. Nutr. 1992, 56, 895–898. [Google Scholar] [PubMed]
- Zock, P.L.; de Vries, J.H.M.; Katan, M.B. Impact of myristic acid versus palmitic acid on serum lipid and lipoprotein levels in healthy women and men. Arterioscler. Thromb. Vasc. 1994, 14, 567–575. [Google Scholar] [CrossRef]
- Mensink, R.P.; Zock, P.L.; Kester, A.D.M.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: A meta-analysis of 60 controlled trials1−3. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar] [PubMed]
- Lawrence, G.D. Dietary fats and health: Dietary recommendations in the context of scientific evidence. Adv. Nutr. 2013, 4, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Pala, V.; Krogh, V.; Muti, P.; Chajés, V.; Riboli, E.; Micheli, A.; Saadatian, M.; Sieri, S.; Berrino, F. Erythrocyte membrane fatty acids and subsaquent breast cancer: A prospective Italian study. J. Natl. Cancer Inst. 2001, 93, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Youn, K.; Yun, E.Y.; Hwang, J.S.; Jeong, W.S.; Ho, Ch.T.; Jun, M. Oleic acid ameliorates Aβ-induced inflammation by downregulation of COX-2 and iNOS via NFκB signaling pathway. J. Funct. Foods 2015, 14, 1–11. [Google Scholar] [CrossRef]
- Yongmanitchai, W.; Ward, O.P. Positional distribution of fatty acids, and molecular species of polar lipids, in the diatom Phaeodactylum tricornutum. J. Gen. Microbiol. 1993, 139, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Vávra Ambrožová, J.; Mišurcová, L.; Vícha, R.; Machů, L.; Samek, D.; Baroň, M.; Mlček, J.; Sochor, J.; Juříková, T. Influence of extractive solvents on lipid and fatty acids content of edible freshwater algal and seaweed products and green microalga Chlorella kessleri and cyanobacteria Spirulina platensis. Molecules 2014, 19, 2344–2360. [Google Scholar] [CrossRef] [PubMed]
- Mišurcová, L. Chemical composition of seaweeds. In Handbook of Marine Macroalgae: Biotechnology and Applied Phycology; Kim, S.K., Ed.; John Wiley & Sons Ltd.: Chichester, UK, 2011; pp. 173–192. [Google Scholar]
- De Caterina, R.; Basta, G. n-3 Fatty acids and the inflammatory response—Biological background. Eur. Heart J. Suppl. 2001, 3, D42–D49. [Google Scholar] [CrossRef]
- AI, F.F.; Bin, J.; Zhang, Z.M.; Huang, J.H.; Wang, J.B.; Liang, Y.Z.; Yu, L.; Yang, Z.Y. Application of random forests to select quality vegetable oils by their fatty acid composition. Food Chem. 2014, 143, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Abedi, E.; Sahari, M.A. Long-chain polyunsaturated fatty acid sources and evaluation of their nutritional and functional properties. Food Sci. Nutr. 2014, 2, 443–463. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Liao, J.K.; Libby, P. Fatty acid modulation of endothelial activation. Am. J. Clin. Nutr. 2000, 71, 213S–223S. [Google Scholar] [PubMed]
- Narayan, B.; Miyashita, K.; Hosakawa, M. Physiological effects of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)—A review. Food Rev. Int. 2006, 22, 291–307. [Google Scholar] [CrossRef]
- Sugano, M.; Hirahara, F. Polyunsaturated fatty acids in the food chain in Japan. Am. J. Clin. Nutr. 2000, 71, 189S–196S. [Google Scholar] [PubMed]
- Cordain, L.; Eaton, S.B.; Miller, J.B.; Mann, N.; Hill, K. The paradoxical nature of hunter-gatherer diets: Meat-based, yet non-atherogenic. Eur. J. Clin. Nutr. 2002, 56, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Sundram, K.; Ismail, A.; Hayes, K.C.; Jeyamalar, R.; Pathmanathan, R. Trans (elaidic) fatty acids adversely affect the lipoprotein profile relative to specific saturated fatty acids in humans1,2. J. Nutr. 1997, 127, 514S–520S. [Google Scholar] [PubMed]
- Elmadfa, I.; Kornsteiner, M. Dietary fat intake—A global perspective. Ann. Nutr. Metab. 2009, 54, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Scarborough, P.; Peto, V.; Rayner, M.; Leal, J.; Luengo-Fernandez, R.; Gray, A. European Cardiovascular Disease Statistics; European Heart Network: Brussels, Belgium, 2008. [Google Scholar]
- Hay, D.R. Cardiovascular disease in New Zealand, 2004: A summary of recent statistical information. In Technical Report: To Medical and Allied Professions; Heart Foundation: Auckland, New Zealand, 2004. [Google Scholar]
- Norman, R.; Bradshaw, D.; Schneider, M.; Pieterse, D.; Groenewald, P. What are the top causes of death in South Africa? In Proceedings of the South African Medical Research Council, Cape Town, South Africa; 2006. [Google Scholar]
- Iso, H. Changes in coronary heart disease risk among Japanese. Circulation 2008, 118, 2725–2729. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2011, 125, 1–221. [Google Scholar]
- Harika, R.K.; Eilander, A.; Osendarp, S.J.M.; Zock, P.L. Intake of fatty acids in general Populations Worldwide Does Not Meet dietary recommendations to prevent Coronary Heart Disease: A systematic review of data from 40 countries. Ann. Nutr. Metab. 2013, 63, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Willett, W.C. Dietary fat intake and risk of coronary heart disease in women: 20 Years of follow-up of the nurses’health study. Am. J. Epidemiol. 2005, 161, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease1−5. Am. J. Clin. Nutr. 2010, 91, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk. Ann. Intern. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Czernichow, S.; Thomas, D.; Bruckert, E. n-6 Fatty acids and cardiovascular health: A review of the evidence for dietary intake recommendations. Br. J. Nutr. 2010, 104, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Fahimi, S.; Lim, S.; Andrews, K.G.; Engell, R.E.; Powles, J.; Ezzati, M.; Mozaffarian, D. Global, regional, and national consumption levels of dietary fats and oils in 1990 ad 2010: A systematic analysis including 266 country-specific nutrition surveys. Br. Med. J. 2014, 348, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakobsen, M.U.; O’Reilly, E.J.; Heitmann, B.L.; Pereira, M.A.; Balter, K.; Fraser, G.E.; Goldbourt, U.; Hallmans, G.; Knekt, P.; Liu, S.; et al. Major types of dietary fat and risk of coronary heart diseases: A pooled analysis of 11 cohort studies1−3. Am. J. Clin. Nutr. 2009, 89, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, F.; Brown, B.W.; Lamendola, C.; McLaughlin, T.; Reaven, G.M. Relationship between Obesity, Insulin Resistance, and Coronary Heart Disease Risk. J. Am. Coll. Cardiol. 2002, 40, 937–943. [Google Scholar] [CrossRef]
- ČSN CEN ISO/TS 17764–1; Animal Feeding Stuffs—Determination of the Content of Fatty Acids—Part 1: Preparation of Methyl Esters; Czech Standards Institute: Prague, Czech Republic, 2007; pp. 1–20.
- Macedo, L.F.A.; Lacerda, E.C.Q.; Silva, R.R.; Simionato, J.I.; Pedrao, M.R.; Coro, F.A.G.; de Souza, N.E. Implication of method chosen for analysis of fatty acids in meat: A review. Am. J. Agric. Biol. Sci. 2012, 7, 278–284. [Google Scholar] [CrossRef]
- ČSN CEN ISO/TS 17764–2; Animal Feeding Stuffs—Determination of the Content of Fatty Acids—Part 2: Gas Chromatographic Method; Czech Standards Institute: Prague, Czech Republic, 2007; pp. 1–24.
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsavova, J.; Misurcova, L.; Ambrozova, J.V.; Vicha, R.; Mlcek, J. Fatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty Acids. Int. J. Mol. Sci. 2015, 16, 12871-12890. https://doi.org/10.3390/ijms160612871
Orsavova J, Misurcova L, Ambrozova JV, Vicha R, Mlcek J. Fatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty Acids. International Journal of Molecular Sciences. 2015; 16(6):12871-12890. https://doi.org/10.3390/ijms160612871
Chicago/Turabian StyleOrsavova, Jana, Ladislava Misurcova, Jarmila Vavra Ambrozova, Robert Vicha, and Jiri Mlcek. 2015. "Fatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty Acids" International Journal of Molecular Sciences 16, no. 6: 12871-12890. https://doi.org/10.3390/ijms160612871
APA StyleOrsavova, J., Misurcova, L., Ambrozova, J. V., Vicha, R., & Mlcek, J. (2015). Fatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty Acids. International Journal of Molecular Sciences, 16(6), 12871-12890. https://doi.org/10.3390/ijms160612871