
Factors Affecting the Baseline and Post-Treatment Scores on the Hopkins Verbal Learning Test-Revised Japanese Version before and after Whole-Brain Radiation Therapy

 and
and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Factors Affecting the Baseline HVLT-R Scores
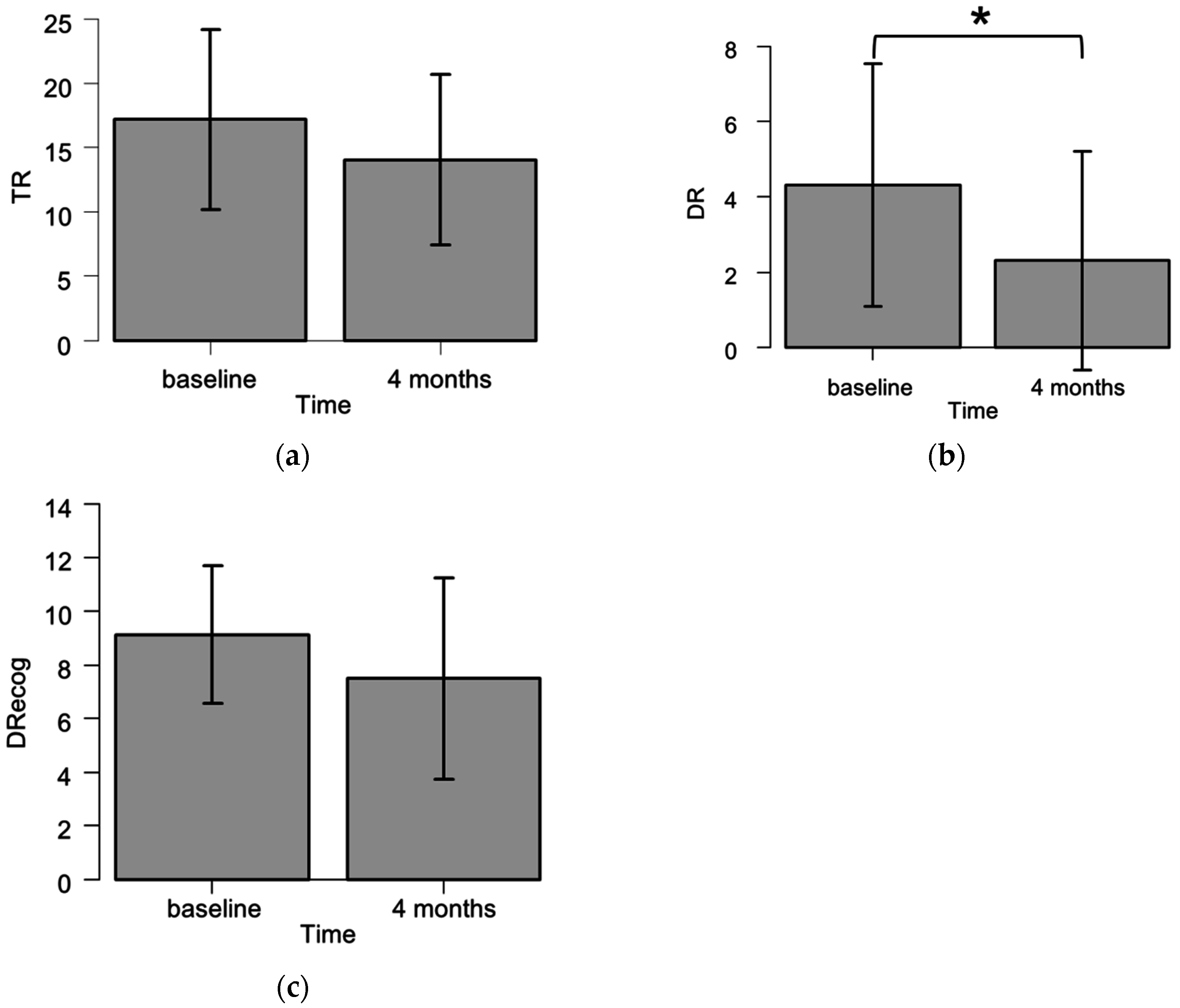
2.3. HVLT-R Raw Scores of the Patients Who Underwent Two Examinations (Baseline and Four Months) (Worse-Prognosis Group, n = 16)
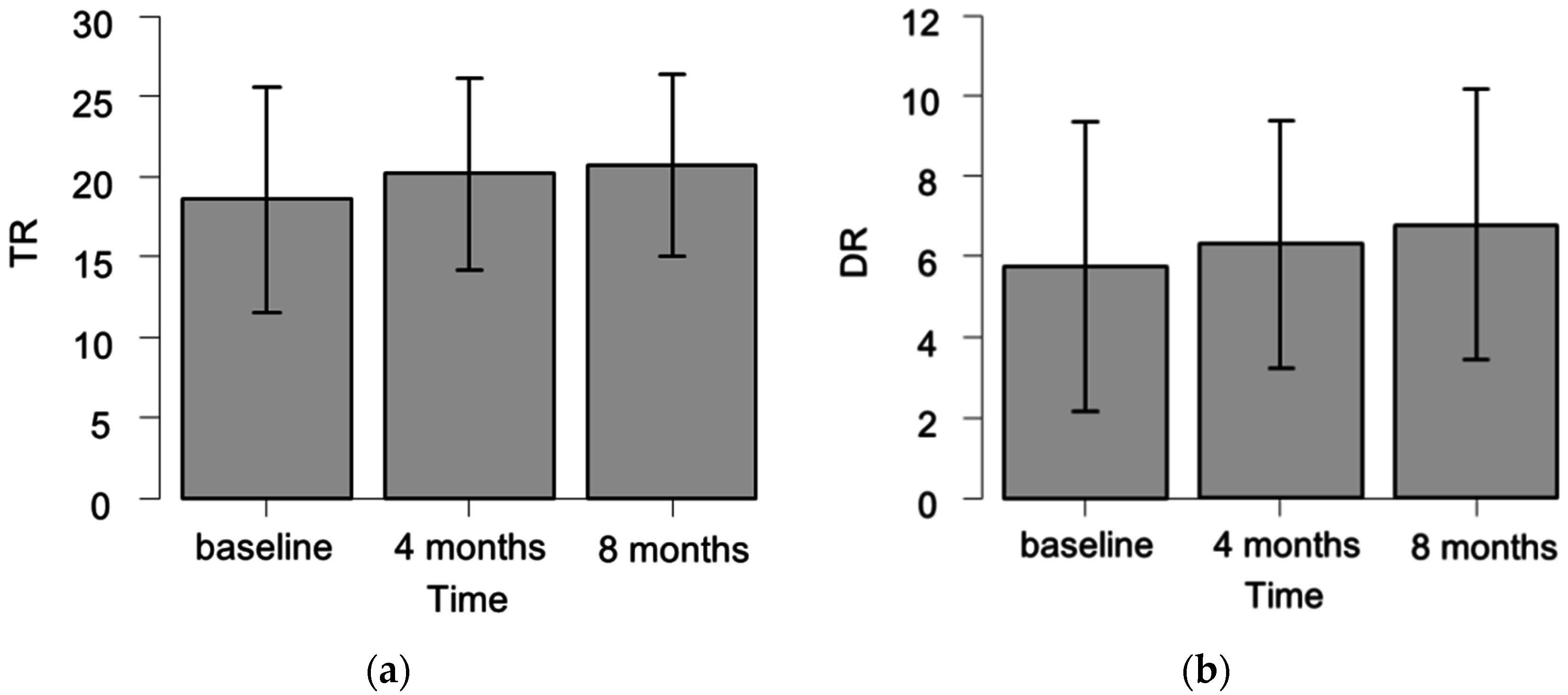
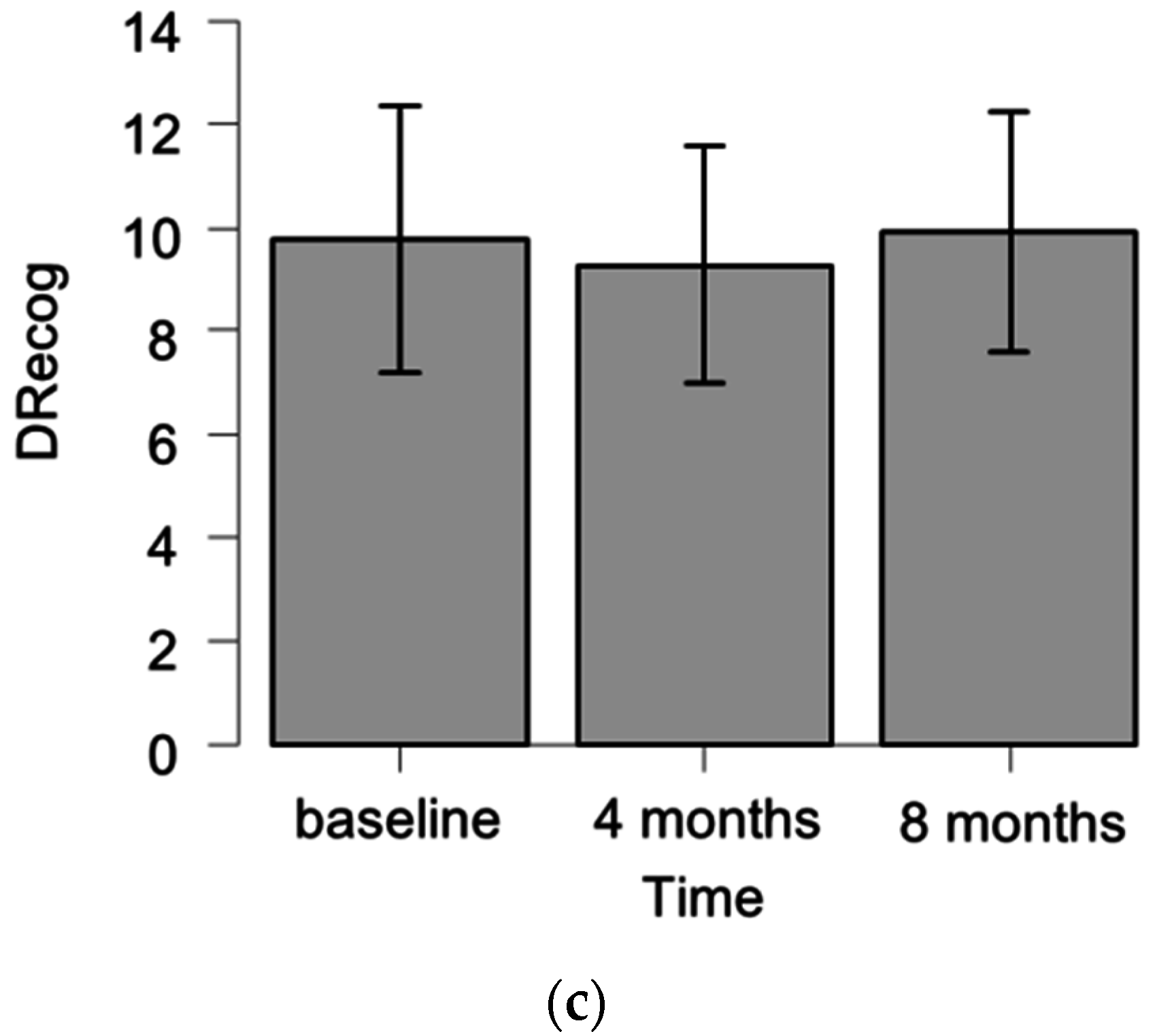
2.4. HVLT-R Raw Scores of the Patients Who Underwent Three Examinations (Baseline, Four, and Eight Months) (Better-Prognosis Group, n = 29)
2.5. Factors Associated with a Significant Decline in Individual HVLT-R Scores at Four Months
2.6. Factors Associated with a Significant Decline in Individual HVLT-R Scores at Eight Months
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Neurocognitive Function Assessment
4.3. Statistical Analyses
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BM | brain metastasis |
| CNS | central nervous system |
| COWAT | Controlled Oral Word Association Test |
| DR | delayed recall |
| DRecog | delayed recognition |
| HVLT | Hopkins Verbal Learning Test |
| HVLT-R | Hopkins Verbal Learning Test-Revised |
| KPS | Karnofsky Performance Status |
| LD-SCLC | limited-disease small cell lung cancer |
| MMSE | Mini-Mental State Examination |
| NCF | neurocognitive function |
| NHL | non-Hodgkin lymphoma |
| NSCLC | non-small cell lung cancer |
| RTOG | Radiation Therapy Oncology Group |
| SCLC | small-cell lung cancer |
| SRS | stereotactic radiosurgery |
| TMT | Trail Making Test |
| TR | total recall |
| WBRT | whole-brain radiation therapy |
References
- Sperduto, P.W.; Shanley, R.; Luo, X.; Andrews, D.; Werner-Wasik, M.; Valicenti, R.; Bahary, J.P.; Souhami, L.; Won, M.; Mehta, M. Secondary analysis of RTOG 9508, a phase 3 randomized trial of whole-brain radiation therapy versus WBRT plus stereotactic radiosurgery in patients with 1–3 brain metastases; poststratified by the graded prognostic assessment (GPA). Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, H.; Tago, M.; Shirato, H. Stereotactic Radiosurgery with or without Whole-Brain Radiotherapy for Brain Metastases: Secondary Analysis of the JROSG 99–1 Randomized Clinical Trial. JAMA Oncol. 2015, 1, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G., 2nd; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients with 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Wefel, J.S.; Lee, E.Q.; Schiff, D.; van den Bent, M.J.; Soffietti, R.; Suh, J.H.; Vogelbaum, M.A.; Mehta, M.P.; Dancey, J.; et al. Challenges relating to solid tumour brain metastases in clinical trials, part 2: Neurocognitive, neurological, and quality-of-life outcomes. A report from the RANO group. Lancet Oncol. 2013, 14, e407–e416. [Google Scholar] [CrossRef]
- Aoyama, H.; Tago, M.; Kato, N.; Toyoda, T.; Kenjyo, M.; Hirota, S.; Shioura, H.; Inomata, T.; Kunieda, E.; Hayakawa, K.; et al. Neurocognitive function of patients with brain metastasis who received either whole brain radiotherapy plus stereotactic radiosurgery or radiosurgery alone. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1388–1395. [Google Scholar] [CrossRef] [PubMed]
- Kurita, G.P.; Sjogren, P.; Ekholm, O.; Kaasa, S.; Loge, J.H.; Poviloniene, I.; Klepstad, P. Prevalence and predictors of cognitive dysfunction in opioid-treated patients with cancer: A multinational study. J. Clin. Oncol. 2011, 29, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Hoops, S.; Nazem, S.; Siderowf, A.D.; Duda, J.E.; Xie, S.X.; Stern, M.B.; Weintraub, D. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology 2009, 73, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Bae, K.; Gore, E.M.; Movsas, B.; Wong, S.J.; Meyers, C.A.; Bonner, J.A.; Schild, S.E.; Gaspar, L.E.; Bogart, J.A.; et al. Phase III trial of prophylactic cranial irradiation compared with observation in patients with locally advanced non-small-cell lung cancer: Neurocognitive and quality-of-life analysis. J. Clin. Oncol. 2011, 29, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Pugh, S.L.; Tome, W.A.; Caine, C.; Corn, B.; Kanner, A.; Rowley, H.; Kundapur, V.; DeNittis, A.; Greenspoon, J.N.; et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): A phase II multi-institutional trial. J. Clin. Oncol. 2014, 32, 3810–3816. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.H.; Bae, K.; Komaki, R.; Meyers, C.; Movsas, B.; Le Pechoux, C.; Werner-Wasik, M.; Videtic, G.M.; Garces, Y.I.; Choy, H. Primary analysis of a phase II randomized trial Radiation Therapy Oncology Group (RTOG) 0212: Impact of different total doses and schedules of prophylactic cranial irradiation on chronic neurotoxicity and quality of life for patients with limited-disease small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 77–84. [Google Scholar] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | WBRT Dose Group | p | ||
|---|---|---|---|---|
| 25 Gy (n = 11) | 30 Gy (n = 18) | 35 Gy (n = 16) | ||
| Age: median (range) | 65 (52–77) | 65 (45–86) | 66 (39–81) | 0.95 |
| Cranial lesion (n): | ||||
| BM | 0 | 7 | 16 | <0.001 |
| Dissemination | 0 | 6 | 0 | |
| NHL | 0 | 3 | 0 | |
| Skull metastasis | 0 | 2 | 0 | |
| None | 11 | 0 | 0 | |
| Gender (n): | ||||
| Female | 3 | 10 | 11 | 0.10 |
| Male | 8 | 8 | 5 | |
| KPS (n): | ||||
| ≤70 | 0 | 7 | 5 | 0.062 |
| 80–100 | 11 | 11 | 11 | |
| Primary site (n): | ||||
| Breast | 0 | 4 | 3 | <0.001 |
| NSCLC | 0 | 10 | 8 | |
| SCLC | 11 | 1 | 1 | |
| NHL | 0 | 3 | 0 | |
| others | 0 | 0 | 4 | |
| Total number of examinations (n): | ||||
| Two (baseline and 4 mos) | 1 | 8 | 7 | 0.11 |
| Three (baseline, 4, and 8 mos) | 10 | 10 | 9 | |
| Reason for discontinuation (n): | ||||
| Denial | 0 | 2 | 0 | 0.52 |
| Death from cancer | 1 | 3 | 4 | |
| Worsened general condition | 0 | 3 | 3 | |
| Variable | Total Number of Examinations | p | |
|---|---|---|---|
| 2 (baseline and 4 mos) (n = 16) | 3 (baseline, 4, and 8 mos) (n = 29) | ||
| Age: | |||
| ≤65 | 8 (32%) | 17 (68%) | 0.76 |
| ≥66 | 8 (40%) | 12 (60%) | |
| KPS: | |||
| ≤70 | 8 (67%) | 4 (33%) | 0.014 |
| 80–100 | 8 (24%) | 25 (76%) | |
| Dissemination | |||
| No | 15 (38%) | 24 (62%) | 0.40 |
| Yes | 1 (17%) | 5 (83%) | |
| Subdomain | Variable | n | Average (SD) | p |
|---|---|---|---|---|
| TR | KPS: | |||
| ≤70 | 12 | 13.1 (6.4) | 0.0053 | |
| 80–100 | 33 | 19.9 (6.3) | ||
| Age: | ||||
| ≤65 | 25 | 20.0 (6.2) | 0.030 | |
| ≥66 | 20 | 15.7 (7.3) | ||
| Dose (Gy): | ||||
| 25 | 11 | 17.0 (4.6) | 0.19 | |
| 30 | 18 | 16.2 (8.1) | ||
| 35 | 16 | 20.9 (6.4) | ||
| Cranial Lesion: | ||||
| BM | 23 | 18.1 (7.0) | 0.011 | |
| Dissemination | 6 | 23.5 (4.6) | ||
| NHL | 3 | 6.7 (5.9) | ||
| Skull metastasis | 2 | 24.5 (2.1) | ||
| None | 11 | 17.0 (4.6) | ||
| DR | KPS: | |||
| ≤70 | 12 | 3.0 (2.8) | 0.012 | |
| 80–100 | 33 | 6.1 (3.4) | ||
| Age: | ||||
| ≤65 | 25 | 6.0 (3.3) | 0.080 | |
| ≥66 | 20 | 4.3 (3.6) | ||
| Dose (Gy): | ||||
| 25 | 11 | 5.4 (2.2) | 0.21 | |
| 30 | 18 | 4.2 (4.0) | ||
| 35 | 16 | 6.4 (3.5) | ||
| Cranial Lesion: | ||||
| BM | 23 | 4.9 (3.8) | 0.014 | |
| Dissemination | 6 | 8.5 (2.2) | ||
| NHL | 3 | 0.0 (0.0) | ||
| Skull metastasis | 2 | 6.5 (2.1) | ||
| None | 11 | 5.4 (2.2) | ||
| DRecog | KPS: | |||
| ≤70 | 12 | 7.5 (3.4) | 0.0078 | |
| 80–100 | 33 | 10.3 (1.7) | ||
| Age: | ||||
| ≤65 | 25 | 10.4 (1.6) | 0.031 | |
| ≥66 | 20 | 8.5 (3.1) | ||
| Dose (Gy): | ||||
| 25 | 11 | 9.8 (1.7) | 0.27 | |
| 30 | 18 | 8.6 (3.4) | ||
| 35 | 16 | 10.4 (1.6) | ||
| Cranial Lesion: | ||||
| BM | 23 | 9.7 (2.1) | 0.021 | |
| Dissemination | 6 | 11.2 (1.0) | ||
| NHL | 3 | 3.3 (2.9) | ||
| Skull metastasis | 2 | 11.0 (1.4) | ||
| None | 11 | 9.8 (1.7) |
| Dose (Gy) | n | Subdomain | Baseline Score Avg. (SD) | 4-Month Score Avg. (SD) | 8-Month Score Avg. (SD) | p (Friedman Test) |
|---|---|---|---|---|---|---|
| 25 | 10 | TR | 16.7 (4.8) | 19.9 (3.7) | 18.4 (4.7) | 0.078 |
| DR | 5.4 (2.3) | 6.1 (2.1) | 6.8 (2.7) | 0.19 | ||
| DRecog | 9.6 (1.7) | 9.0 (2.2) | 9.9 (1.6) | 0.30 | ||
| 30 | 10 | TR | 18.9 (9.1) | 21.1 (6.9) | 21.5 (4.2) | 0.71 |
| DR | 5.7 (4.4) | 6.9 (3.8) | 7.1 (3.7) | 0.44 | ||
| DRecog | 9.4 (3.9) | 9.4 (2.6) | 10.3 (2.4) | 0.23 | ||
| 35 | 9 | TR | 20.3 (6.8) | 19.6 (7.5) | 22.3 (7.6) | 0.52 |
| DR | 6.2 (4.2) | 5.9 (3.4) | 6.4 (4.0) | 0.88 | ||
| DRecog | 10.3 (1.5) | 9.4 (2.3) | 9.4 (3.1) | 0.96 |
| Subdomain | Variable | Declined, n (%) | Not Declined, n (%) | p |
|---|---|---|---|---|
| TR | Age: | |||
| ≤65 | 4 (16) | 21 (84) | 0.30 | |
| ≥66 | 6 (30) | 14 (70) | ||
| Dose (Gy): | ||||
| 25 | 1 (0.9) | 10 (90.9) | 0.22 | |
| 30 | 3 (17) | 15 (83) | ||
| 35 | 6 (37) | 10 (63) | ||
| KPS: | ||||
| ≤70 | 6 (50) | 6 (50) | 0.013 | |
| 80–100 | 4 (12) | 29 (88) | ||
| Total number of examinations: | ||||
| Two (baseline and 4 mos) | 8 (50) | 8 (50) | 0.0017 | |
| Three (baseline, 4, and 8 mos) | 2 (7) | 27 (93) | ||
| DR | Age: | |||
| ≤65 | 6 (24) | 19 (76) | 1 | |
| ≥66 | 5 (25) | 15 (75) | ||
| Dose (Gy): | ||||
| 25 | 2 (18) | 9 (82) | 0.75 | |
| 30 | 4 (22) | 14 (78) | ||
| 35 | 5 (31) | 11 (69) | ||
| KPS: | ||||
| ≤70 | 4 (33) | 8 (67) | 0.45 | |
| 80–100 | 7 (21) | 26 (79) | ||
| Total number of examinations: | ||||
| Two (baseline and 4 mos) | 7 (44) | 9 (56) | 0.035 | |
| Three (baseline, 4, and 8 mos) | 4 (14) | 25 (86) | ||
| DRecog | Age: | |||
| ≤65 | 8 (32) | 17 (68) | 1 | |
| ≥66 | 7 (35) | 13 (65) | ||
| Dose (Gy): | ||||
| 25 | 4 (36) | 7 (64) | 0.41 | |
| 30 | 4 (22) | 14 (78) | ||
| 35 | 7 (44) | 9 (56) | ||
| KPS: | ||||
| ≤70 | 5 (42) | 7 (58) | 0.50 | |
| 80–100 | 10 (33) | 23 (67) | ||
| Total number of examinations: | ||||
| Two (baseline and 4 mos) | 7 (44) | 9 (56) | 0.33 | |
| Three (baseline, 4, and 8 mos) | 8 (28) | 21 (72) | ||
| Subdomain | Variable | Declined, n (%) | Not Declined, n (%) | p |
|---|---|---|---|---|
| TR | Age: | |||
| ≤65 | 2 (12) | 15 (88) | 1 | |
| ≥66 | 1 (8) | 11 (92) | ||
| Dose (Gy): | ||||
| 25 | 1 (10) | 9 (90) | 1 | |
| 30 | 1 (10) | 9 (90) | ||
| 35 | 1 (11) | 8 (89) | ||
| KPS: | ||||
| ≤70 | 0 (0) | 4 (100) | 1 | |
| 80–100 | 3 (12) | 22 (88) | ||
| DR | Age: | |||
| ≤65 | 0 (0) | 17 (100) | 0.060 | |
| ≥66 | 3 (25) | 9 (75) | ||
| Dose (Gy): | ||||
| 25 | 1 (10) | 9 (90) | 1 | |
| 30 | 1 (10) | 9 (90) | ||
| 35 | 1 (11) | 8 (89) | ||
| KPS: | ||||
| ≤70 | 1 (25) | 3 (75) | 0.37 | |
| 80–100 | 2 (8) | 23 (92) | ||
| DRecog | Age: | |||
| ≤65 | 2 (12) | 15 (88) | 0.20 | |
| ≥66 | 4 (33) | 8 (67) | ||
| Dose (Gy): | ||||
| 25 | 1 (10) | 9 (90) | 0.46 | |
| 30 | 2 (20) | 8 (80) | ||
| 35 | 3 (33) | 6 (67) | ||
| KPS: | ||||
| ≤70 | 2 (50) | 2 (50) | 0.18 | |
| 80–100 | 4 (16) | 21 (84) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, H.; Tanaka, K.; Kanemoto, A.; Nakano, T.; Abe, E.; Aoyama, H. Factors Affecting the Baseline and Post-Treatment Scores on the Hopkins Verbal Learning Test-Revised Japanese Version before and after Whole-Brain Radiation Therapy. Int. J. Mol. Sci. 2016, 17, 1834. https://doi.org/10.3390/ijms17111834
Saito H, Tanaka K, Kanemoto A, Nakano T, Abe E, Aoyama H. Factors Affecting the Baseline and Post-Treatment Scores on the Hopkins Verbal Learning Test-Revised Japanese Version before and after Whole-Brain Radiation Therapy. International Journal of Molecular Sciences. 2016; 17(11):1834. https://doi.org/10.3390/ijms17111834
Chicago/Turabian StyleSaito, Hirotake, Kensuke Tanaka, Ayae Kanemoto, Toshimichi Nakano, Eisuke Abe, and Hidefumi Aoyama. 2016. "Factors Affecting the Baseline and Post-Treatment Scores on the Hopkins Verbal Learning Test-Revised Japanese Version before and after Whole-Brain Radiation Therapy" International Journal of Molecular Sciences 17, no. 11: 1834. https://doi.org/10.3390/ijms17111834
APA StyleSaito, H., Tanaka, K., Kanemoto, A., Nakano, T., Abe, E., & Aoyama, H. (2016). Factors Affecting the Baseline and Post-Treatment Scores on the Hopkins Verbal Learning Test-Revised Japanese Version before and after Whole-Brain Radiation Therapy. International Journal of Molecular Sciences, 17(11), 1834. https://doi.org/10.3390/ijms17111834