Synergies of Targeting Tumor Angiogenesis and Immune Checkpoints in Non-Small Cell Lung Cancer and Renal Cell Cancer: From Basic Concepts to Clinical Reality


Abstract
:
1. Introduction
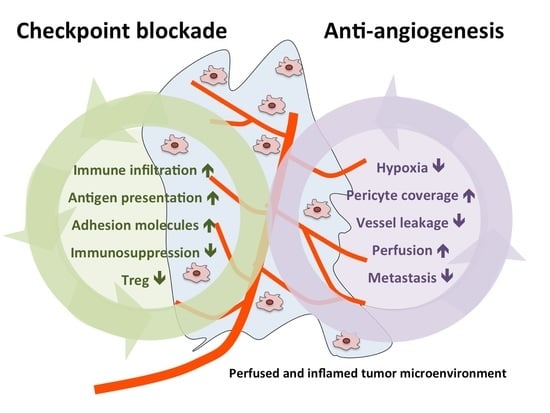
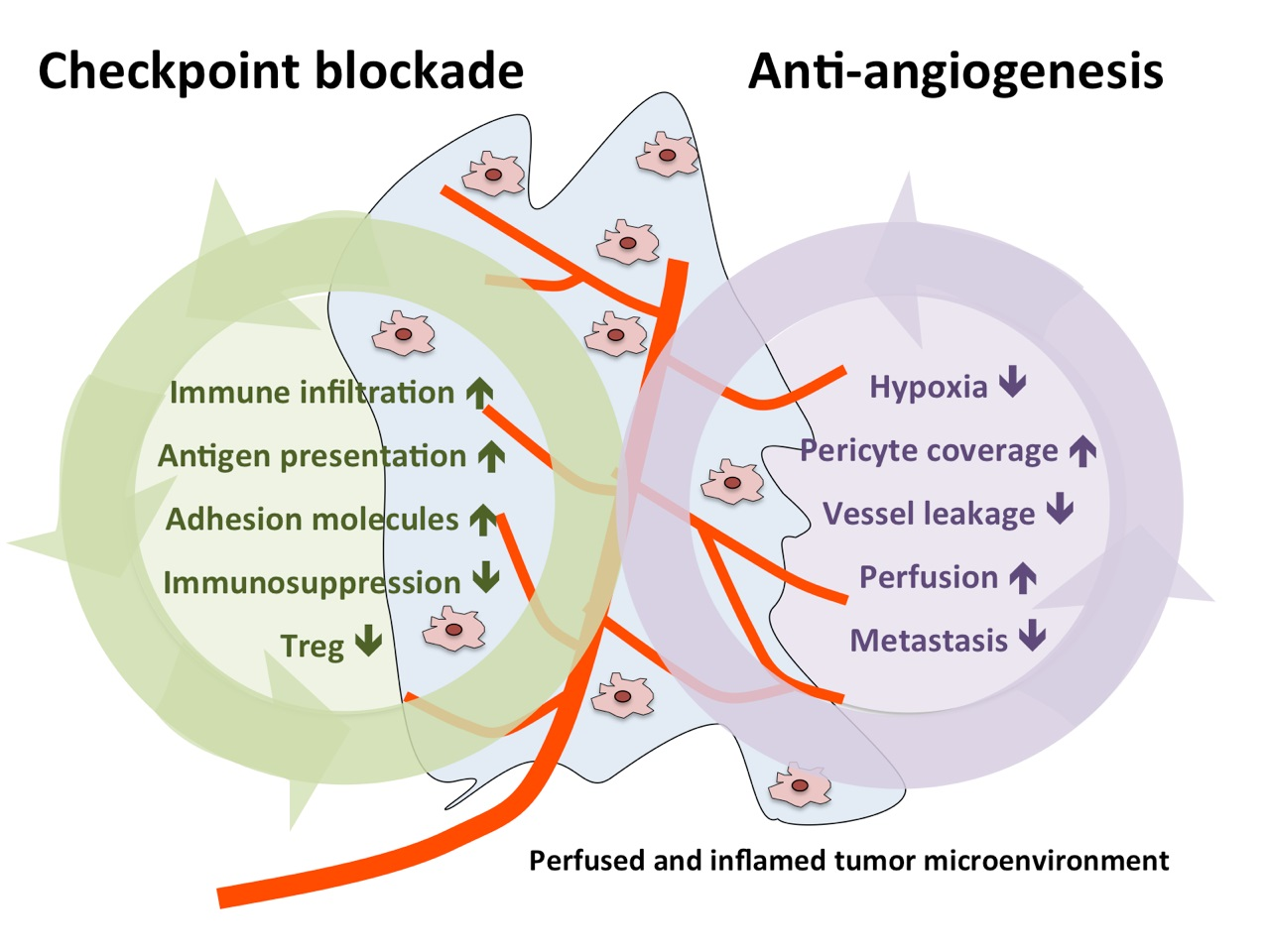
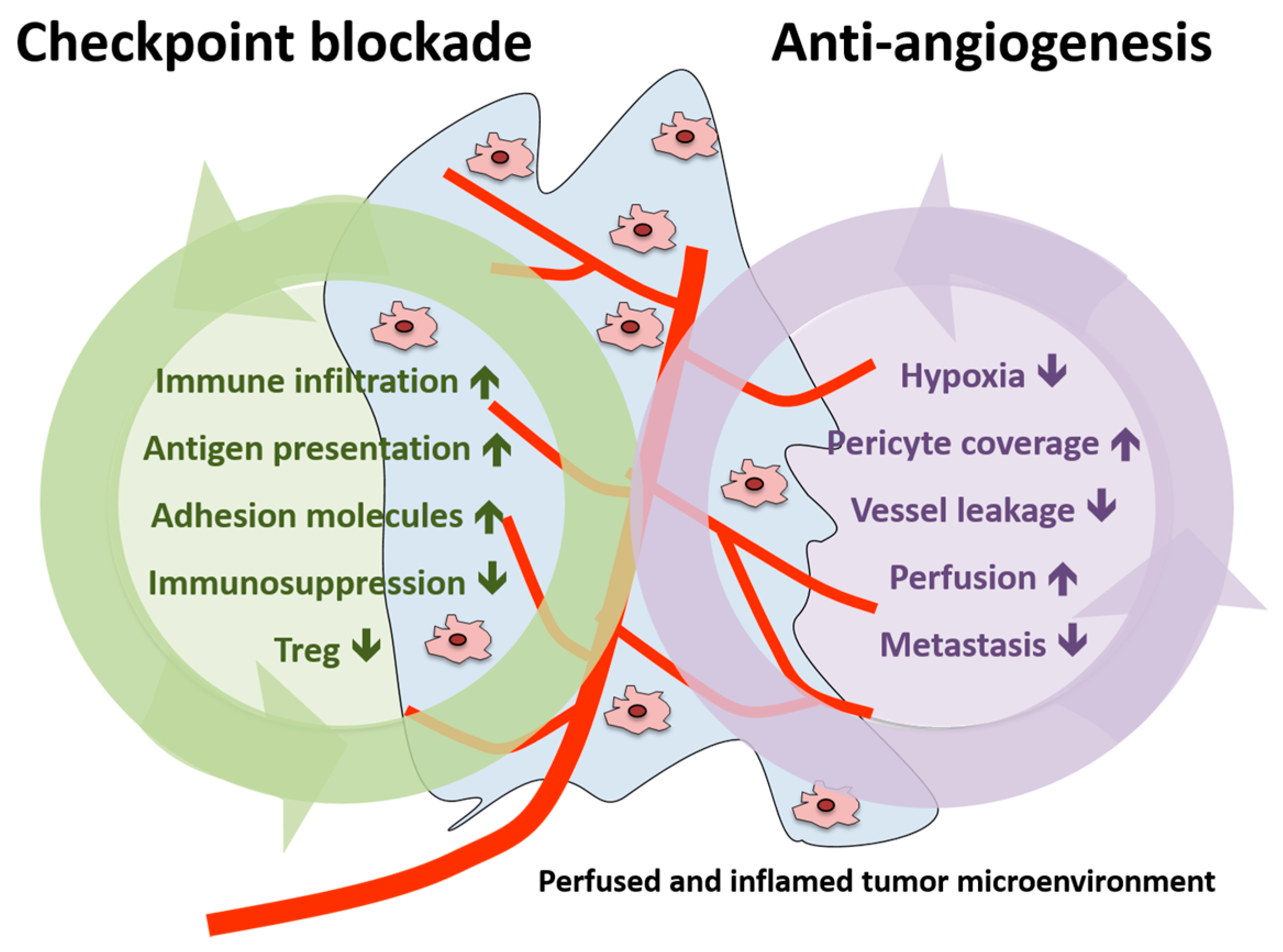
2. Preclinical Rationale for Combined AA and Immune-Activating Therapy
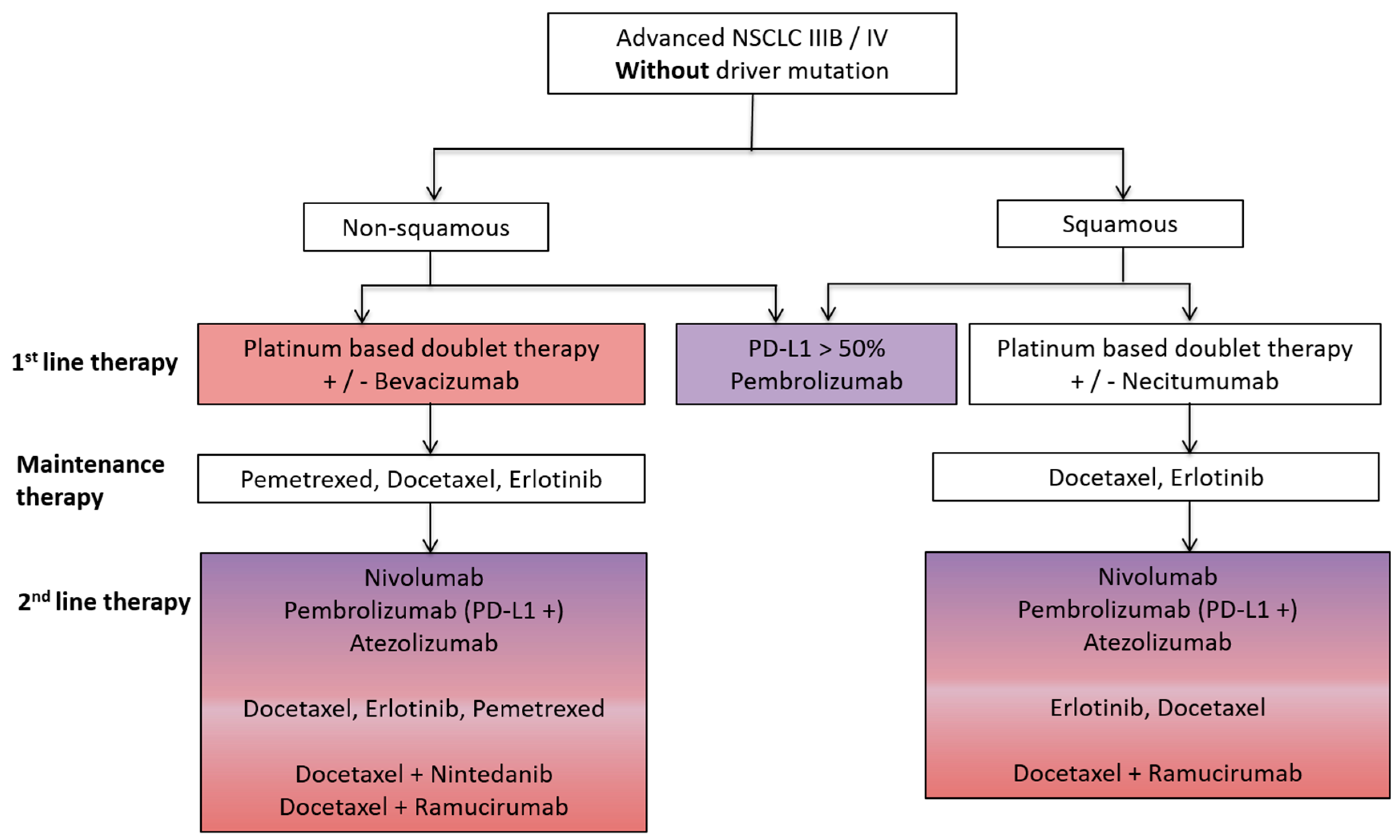
3. Non-Small Cell Lung Cancer (NSCLC)
4. Preclinical Concepts Combining AA and Immunotherapies in NSCLC
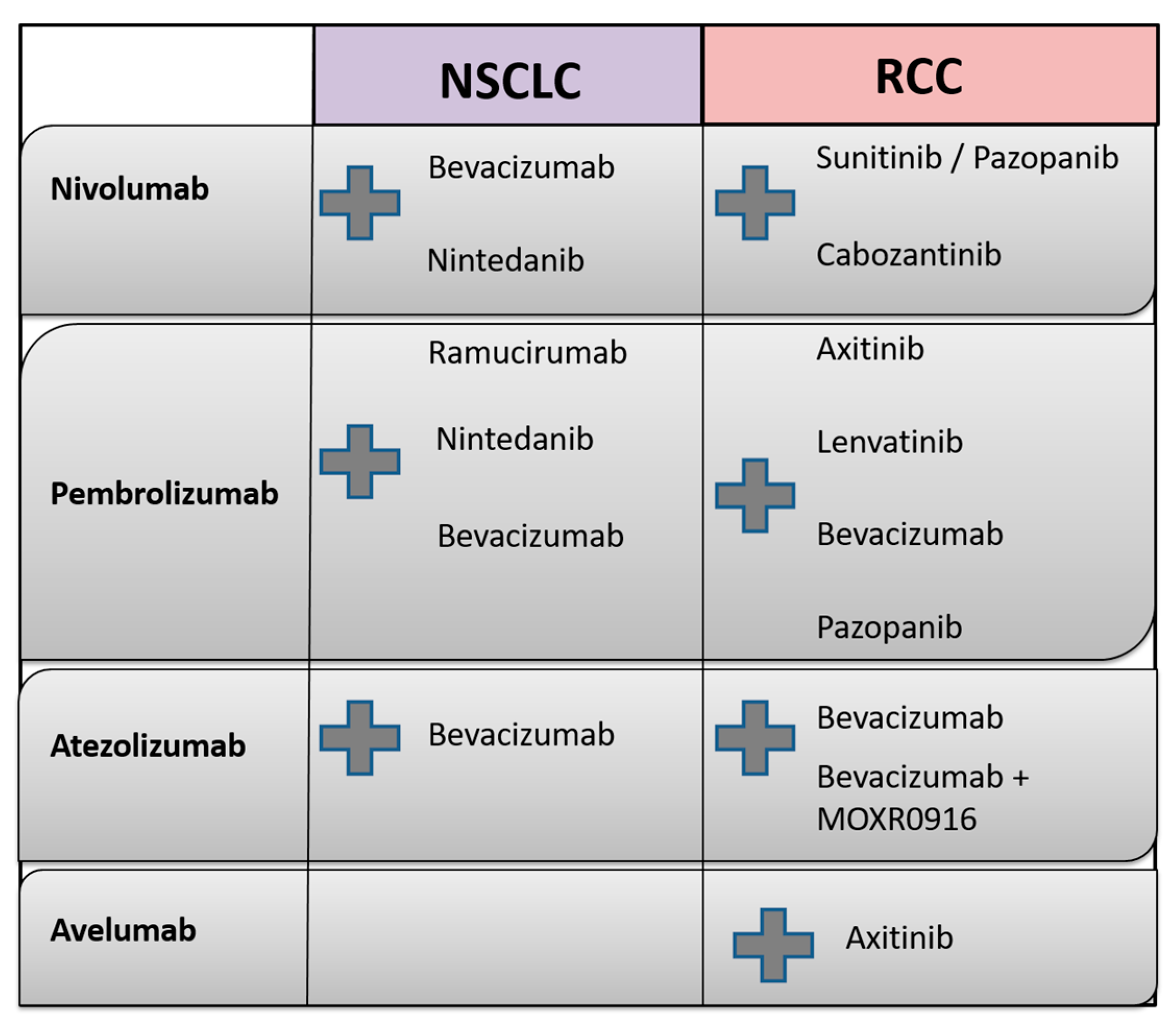
5. Clinical Studies Combining AA and Immunotherapies in NSCLC
5.1. Clinical Studies Combining Bevacizumab with Nivolumab
5.2. Clinical Studies Combining VEGF/VEGFR Targeting with Pembrolizumab
5.3. Clinical Studies Combining Bevacizumab with Atezolizumab
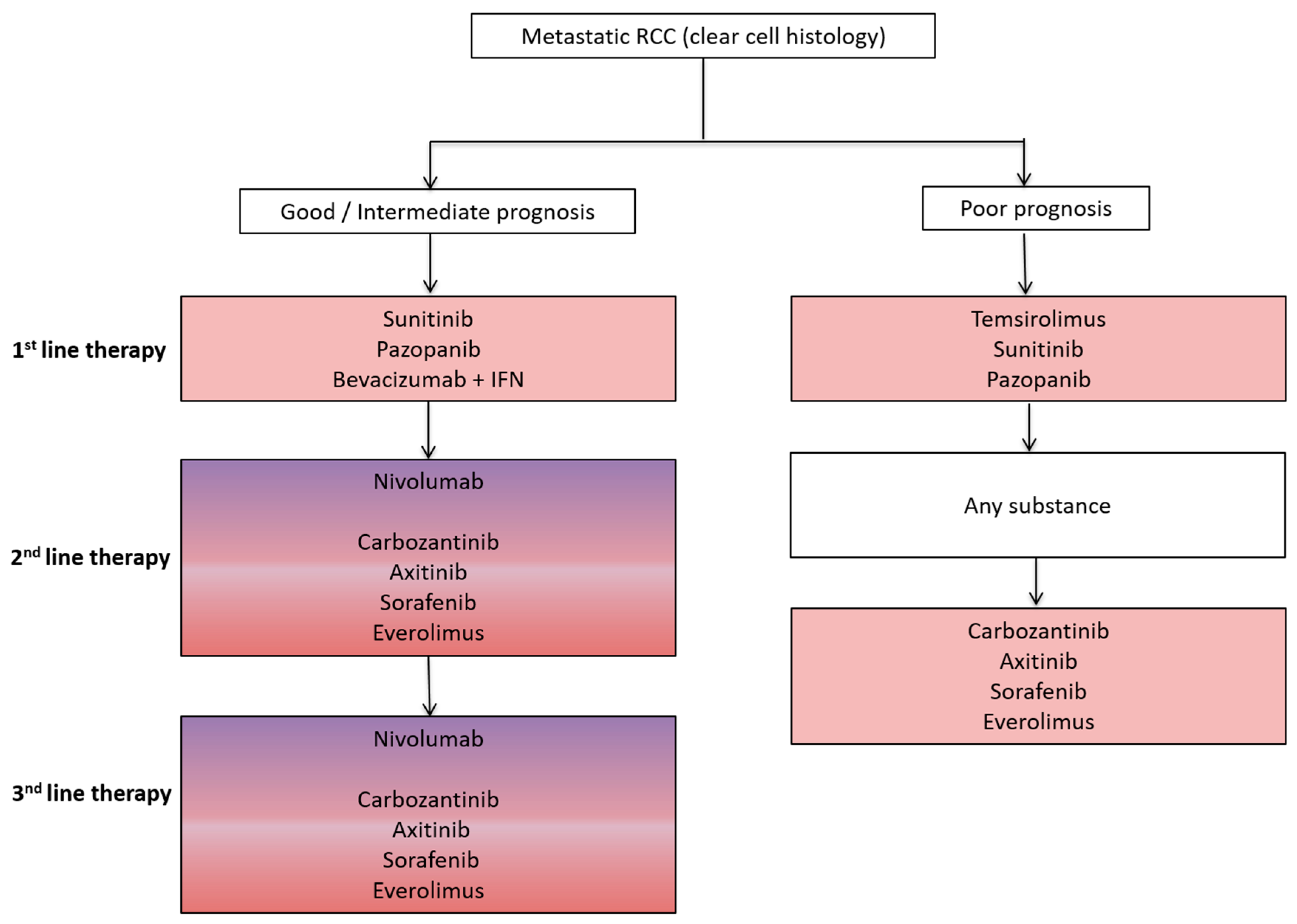
6. Renal Cell Cancer (RCC)
7. Preclinical Concepts Combining AA and Immunotherapies in RCC
8. Clinical Studies Combining AA and Immunotherapies in RCC
8.1. Clinical Studies Combining AA with Nivolumab
8.2. Clinical Studies Combining AA with Pembrolizumab
8.3. Clinical Studies Combining AA with Atezolizumab
9. Further Ongoing Studies Combining Immunotherapy and AA Therapy in RCC
10. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Novello, S.; Barlesi, F.; Califano, R.; Cufer, T.; Ekman, S.; Levra, M.G.; Kerr, K.; Popat, S.; Reck, M.; Senan, S.; et al. Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v1–v27. [Google Scholar] [CrossRef] [PubMed]
- Manegold, C.; Dingemans, A.C.; Gray, J.E.; Nakagawa, K.; Nicolson, M.; Peters, S.; Reck, M.; Wu, Y.L.; Brustugun, O.T.; Crino, L.; et al. The potential of combined immunotherapy and antiangiogenesis for the synergistic treatment of advanced NSCLC. J. Thorac. Oncol. 2017, 12, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.A.; Farnsworth, R.H.; Solomon, B.; Achen, M.G.; Stacker, S.A.; Fox, S.B. The role of the tumor vasculature in the host immune response: Implications for therapeutic strategies targeting the tumor microenvironment. Front. Immunol. 2016, 7, 621. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- De Palma, M.; Biziato, D.; Petrova, T.V. Microenvironmental regulation of tumour angiogenesis. Nat. Rev. Cancer 2017, 17, 457–474. [Google Scholar] [CrossRef] [PubMed]
- Welti, J.; Loges, S.; Dimmeler, S.; Carmeliet, P. Recent molecular discoveries in angiogenesis and antiangiogenic therapies in cancer. J. Clin. Investig. 2013, 123, 3190–3200. [Google Scholar] [CrossRef] [PubMed]
- Jayson, G.C.; Kerbel, R.; Ellis, L.M.; Harris, A.L. Antiangiogenic therapy in oncology: Current status and future directions. Lancet 2016, 388, 518–529. [Google Scholar] [CrossRef]
- Wolf, D.; Sopper, S.; Pircher, A.; Gastl, G.; Wolf, A.M. Treg(s) in cancer: Friends or foe? J. Cell. Physiol. 2015, 230, 2598–2605. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Allison, J.P. Immune checkpoint targeting in cancer therapy: Toward combination strategies with curative potential. Cell 2015, 161, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Cantelmo, A.R.; Pircher, A.; Kalucka, J.; Carmeliet, P. Vessel pruning or healing: Endothelial metabolism as a novel target? Expert Opin. Ther. Targets 2017, 21, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Carmeliet, P.; Jain, R.K. Principles and mechanisms of vessel normalization for cancer and other angiogenic diseases. Nat. Rev. Drug Discov. 2011, 10, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Tolaney, S.M.; Boucher, Y.; Duda, D.G.; Martin, J.D.; Seano, G.; Ancukiewicz, M.; Barry, W.T.; Goel, S.; Lahdenrata, J.; Isakoff, S.J.; et al. Role of vascular density and normalization in response to neoadjuvant bevacizumab and chemotherapy in breast cancer patients. Proc. Natl. Acad. Sci. USA 2015, 112, 14325–14330. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yuan, J.; Righi, E.; Kamoun, W.S.; Ancukiewicz, M.; Nezivar, J.; Santosuosso, M.; Martin, J.D.; Martin, M.R.; Vianello, F.; et al. Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. Proc. Natl. Acad. Sci. USA 2012, 109, 17561–17566. [Google Scholar] [CrossRef] [PubMed]
- Shrimali, R.K.; Yu, Z.; Theoret, M.R.; Chinnasamy, D.; Restifo, N.P.; Rosenberg, S.A. Antiangiogenic agents can increase lymphocyte infiltration into tumor and enhance the effectiveness of adoptive immunotherapy of cancer. Cancer Res. 2010, 70, 6171–6180. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.; Jabouille, A.; Rivera, L.B.; Lodewijckx, I.; Missiaen, R.; Steri, V.; Feyen, K.; Tawney, J.; Hanahan, D.; Michael, I.P.; et al. Combined antiangiogenic and anti-PD-L1 therapy stimulates tumor immunity through HEV formation. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; Goldstein, A.; Wang, H.; Ching Lo, H.; Sun Kim, I.; Welte, T.; Sheng, K.; Dobrolecki, L.E.; Zhang, X.; Putluri, N.; et al. Mutual regulation of tumour vessel normalization and immunostimulatory reprogramming. Nature 2017, 544, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Thienpont, B.; Lambrechts, D. It’s t time for normal blood vessels. Dev. Cell 2017, 41, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Luft, T.; Dietrich, S.; Falk, C.; Conzelmann, M.; Hess, M.; Benner, A.; Neumann, F.; Isermann, B.; Hegenbart, U.; Ho, A.D.; et al. Steroid-refractory GVHD: T-cell attack within a vulnerable endothelial system. Blood 2011, 118, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Carman, C.V.; Martinelli, R. T lymphocyte-endothelial interactions: Emerging understanding of trafficking and antigen-specific immunity. Front. Immunol. 2015, 6, 603. [Google Scholar] [CrossRef] [PubMed]
- Henze, A.T.; Mazzone, M. The impact of hypoxia on tumor-associated macrophages. J. Clin. Investig. 2016, 126, 3672–3679. [Google Scholar] [CrossRef] [PubMed]
- Sica, A.; Massarotti, M. Myeloid suppressor cells in cancer and autoimmunity. J. Autoimmun. 2017. [Google Scholar] [CrossRef] [PubMed]
- Dirkx, A.E.; oude Egbrink, M.G.; Castermans, K.; van der Schaft, D.W.; Thijssen, V.L.; Dings, R.P.; Kwee, L.; Mayo, K.H.; Wagstaff, J.; Bouma-ter Steege, J.C.; et al. Anti-angiogenesis therapy can overcome endothelial cell anergy and promote leukocyte-endothelium interactions and infiltration in tumors. FASEB J. 2006, 20, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Pircher, A.; Johrer, K.; Kocher, F.; Steiner, N.; Graziadei, I.; Heidegger, I.; Pichler, R.; Leonhartsberger, N.; Kremser, C.; Kern, J.; et al. Biomarkers of evasive resistance predict disease progression in cancer patients treated with antiangiogenic therapies. Oncotarget 2016, 7, 20109–20123. [Google Scholar] [CrossRef] [PubMed]
- De Palma, M.; Jain, R.K. CD4+ T cell activation and vascular normalization: Two sides of the same coin? Immunity 2017, 46, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Hilbe, W.; Manegold, C.; Pircher, A. Targeting angiogenesis in lung cancer—Pitfalls in drug development. Transl. Lung Cancer Res. 2012, 1, 122–128. [Google Scholar] [PubMed]
- Tao, L.; Huang, G.; Shi, S.; Chen, L. Bevacizumab improves the antitumor efficacy of adoptive cytokine-induced killer cells therapy in non-small cell lung cancer models. Med. Oncol. 2014, 31, 777. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Wang, R.; Chen, Y.; Song, H.; Chen, L.; Huang, G. Combining antiangiogenic therapy with adoptive cell immunotherapy exerts better antitumor effects in non-small cell lung cancer models. PLoS ONE 2013, 8, e65757. [Google Scholar] [CrossRef] [PubMed]
- Tsukita, Y.; Okazaki, T.; Komatsu, R.; Nihei, M.; Kobayashi, M.; Sato, Y.; Yagita, H.; Ichinose, M. Effects of a combination of antiangiogenic and antilymphangiogenic therapies on a death receptor-5 mediated antitumor immunotherapy in mice. J. Clin. Oncol. 2017, 35, e23001. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Antonia, S.J.; Shepherd, F.A.; Chow, L.Q.; Goldman, J.; Shen, Y.; Chen, A.C.; Gettinger, S. Nivolumab (anti-PD-1; BMS-936558, ONO-4538) maintenance as monotherapy or in combination with bevacizumab (BEV) for non-small cell lung cancer (NSCLC) previously treated with chemotherapy. Int. J. Radiat. Oncol Biol. Phys. 2014, 90, S32. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Rizvi, N.A.; Goldman, J.W.; Gettinger, S.N.; Borghaei, H.; Brahmer, J.R.; Ready, N.E.; Gerber, D.E.; Chow, L.Q.; Juergens, R.A.; et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (CheckMate 012): Results of an open-label, phase 1, multicohort study. Lancet Oncol. 2017, 18, 31–41. [Google Scholar] [CrossRef]
- Wei, S.C.; Levine, J.H.; Cogdill, A.P.; Zhao, Y.; Anang, N.A.S.; Andrews, M.C.; Sharma, P.; Wang, J.; Wargo, J.A.; Pe’er, D.; et al. Distinct cellular mechanisms underlie anti-CTLA-4 and anti-PD-1 checkpoint blockade. Cell 2017, 170, 1120–1133. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Martin-Liberal, J.; Calvo, E.; Isambert, N.; Bendell, J.C.; Cassier, P.; Perez-Gracia, J.L.; Yang, J.; Rege, J.; Mi, G.; et al. Interim safety and clinical activity in patients with advanced NSCLC from a multi-cohort phase 1 study of ramucirumab (R) plus pembrolizumab (P). Ann. Oncol. 2016, 27. [Google Scholar] [CrossRef]
- Cindolo, L.; Patard, J.J.; Chiodini, P.; Schips, L.; Ficarra, V.; Tostain, J.; de La Taille, A.; Altieri, V.; Lobel, B.; Zigeuner, R.E.; et al. Comparison of predictive accuracy of four prognostic models for nonmetastatic renal cell carcinoma after nephrectomy: A multicenter european study. Cancer 2005, 104, 1362–1371. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Miller, J.D.; Li, J.Z.; Russell, M.W.; Charbonneau, C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): A literature review. Cancer Treat. Rev. 2008, 34, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Beltran, A.; Scarpelli, M.; Montironi, R.; Kirkali, Z. 2004 WHO classification of the renal tumors of the adults. Eur. Urol. 2006, 49, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Manola, J.; Royston, P.; Elson, P.; McCormack, J.B.; Mazumdar, M.; Negrier, S.; Escudier, B.; Eisen, T.; Dutcher, J.; Atkins, M.; et al. Prognostic model for survival in patients with metastatic renal cell carcinoma: Results from the international kidney cancer working group. Clin. Cancer Res. 2011, 17, 5443–5450. [Google Scholar] [CrossRef] [PubMed]
- Escudier, B.; Eisen, T.; Stadler, W.M.; Szczylik, C.; Oudard, S.; Siebels, M.; Negrier, S.; Chevreau, C.; Solska, E.; Desai, A.A.; et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Finke, J.H.; Rini, B.; Ireland, J.; Rayman, P.; Richmond, A.; Golshayan, A.; Wood, L.; Elson, P.; Garcia, J.; Dreicer, R.; et al. Sunitinib reverses type-1 immune suppression and decreases T-regulatory cells in renal cell carcinoma patients. Clin. Cancer Res. 2008, 14, 6674–6682. [Google Scholar] [CrossRef] [PubMed]
- Ozao-Choy, J.; Ma, G.; Kao, J.; Wang, G.X.; Meseck, M.; Sung, M.; Schwartz, M.; Divino, C.M.; Pan, P.Y.; Chen, S.H. The novel role of tyrosine kinase inhibitor in the reversal of immune suppression and modulation of tumor microenvironment for immune-based cancer therapies. Cancer Res. 2009, 69, 2514–2522. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.S.; Zea, A.H.; Rini, B.I.; Ireland, J.L.; Elson, P.; Cohen, P.; Golshayan, A.; Rayman, P.A.; Wood, L.; Garcia, J.; et al. Sunitinib mediates reversal of myeloid-derived suppressor cell accumulation in renal cell carcinoma patients. Clin. Cancer Res. 2009, 15, 2148–2157. [Google Scholar] [CrossRef] [PubMed]
- Wallin, J.J.; Bendell, J.C.; Funke, R.; Sznol, M.; Korski, K.; Jones, S.; Hernandez, G.; Mier, J.; He, X.; Hodi, F.S.; et al. Atezolizumab in combination with bevacizumab enhances antigen-specific T-cell migration in metastatic renal cell carcinoma. Nat. Commun. 2016, 7, 12624. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Tannir, N.M.; Mainwaring, P.N.; Rini, B.I.; Hammers, H.J.; Donskov, F.; Roth, B.J.; Peltola, K.; et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 917–927. [Google Scholar] [CrossRef]
- Dudek, A.Z.; Sica, R.A.; Sidani, A.; Jha, G.G.; Xie, H.; Alva, A.S.; Stein, M.N.; Singer, E.A. Phase Ib study of pembrolizumab in combination with bevacizumab for the treatment of metastatic renal cell carcinoma: Big Ten Cancer Research Consortium BTCRC-GU14–003. J. Clin. Oncol. 2016, 34, 559. [Google Scholar] [CrossRef]
- Chowdhury, S.; McDermott, D.F.; Voss, M.H.; Hawkins, R.E.; Aimone, P.; Voi, M.; Isabelle, N.; Wu, Y.; Infante, J.R. A phase I/II study to assess the safety and efficacy of pazopanib (PAZ) and pembrolizumab (PEM) in patients (pts) with advanced renal cell carcinoma (aRCC). J. Clin. Oncol. 2017, 35, 4506. [Google Scholar] [CrossRef]
- McDermott, D.F.; Atkins, M.B.; Motzer, R.J.; Rini, B.I.; Escudier, B.J.; Fong, L.; Joseph, R.W.; Pal, S.K.; Sznol, M.; Hainsworth, J.D.; et al. A phase II study of atezolizumab (atezo) with or without bevacizumab (bev) versus sunitinib (sun) in untreated metastatic renal cell carcinoma (mRCC) patients (pts). J. Clin. Oncol. 2017, 35, 431. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Larkin, J.M.G.; Oya, M.; Thistlethwaite, F.C.; Martignoni, M.; Nathan, P.D.; Powles, T.; McDermott, D.F.; Robbins, P.B.; Chism, D.D.; et al. First-line avelumab + axitinib therapy in patients (pts) with advanced renal cell carcinoma (aRCC): Results from a phase Ib trial. J. Clin. Oncol. 2017, 35, 4504. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Substance Type | Molecular Target |
|---|---|---|
| Avelumab | mAB | PD-L1 |
| Atezolizumab | mAB | PD-L1 |
| Axitinib | TKI | VEGFR 1–3, PDGFR, c-KIT |
| Bevacizumab | mAB | VEGF-A |
| Cabozantinib | TKI | VEGFR 2, c-MET |
| Cetuximab | mAB | EGFR |
| Durvalumab | mAB | PD-L1, CD80 |
| Lenvatinib | TKI | VEGFR 1–3, FGFR, PDGFR, RET, c-KIT |
| Nivolumab | mAB | PD-1 |
| Nintedanib | TKI | VEGFR 1–3, FGFR 1–3, PDGFR |
| Pazopanib | TKI | VEGFR 1–3, PDGFR, c-KIT |
| Pembrolizumab | mAB | PD-1 |
| Ramucirumab | mAB | VEGFR 2 |
| Sunitinib | TKI | PDGFR, VEGFR 1–3, c-KIT, FLT |
| Study Name | Targeting Agents | Comparison | Phase | Primary Endpoint | Therapy Setting | Status * | NCT Number |
|---|---|---|---|---|---|---|---|
| CheckMate 012 | bevacizumab + nivolumab | bevacizumab | I | PFS, OS | First line maintenance | Active Not recruiting | NCT01454102 |
| N.a. | ramucirumab + pembrolizumab | ramucirumab | I | PFS, OS | Inoperable patients | Recruiting | NCT02443324 |
| IMpower150 | Atezolizumab + bevazicumab carboplatin + paclitaxel | Atezolizumab + carboplatin + paclitaxel | III | PFS, OS | First line (Stage IV) | Recruiting | NCT02366143 |
| N.a. | atezolizumab + bevacizumab | / | Ib | Safety | First line | Active Not recruiting | NCT01633970 |
| N.a. | pembrolizumab + nintedanib | / | Ib | MTD of nintedanib, Safety | First line | Recruiting | NCT02856425 |
| N.a. | nivolumab + nintedanib | / | Ib | Safety | Second line | Not recruiting | TBA |
| N.a. | pembrolizumab + paclitacel + bevazicumab | Pembrolizumab + paclitacel | I/II | Clinical efficacy and safety | First line (Stage IIIB/IV) | Recruiting | NCT02039674 |
| Study Name | Targeting Agents | Comparison | Phase | Primary Endpoint | Therapy Setting | Status * | NCT Number |
|---|---|---|---|---|---|---|---|
| WO29637 | atezolizumab + bevacizumab | sunitinib | III | PFS, OS | First line | Active Not recruiting | NCT02420821 |
| JAVELIN Renal 101 | avelumab + axitinib | sunitinib | III | PFS | First line | Recruiting | NCT02684006 |
| JAVELIN Renal 100 | avelumab + axitinib | / | I | MTD | First line | Active Not recruiting | NCT02493751 |
| 200249 | pembrolizumab + pazopanib | monotherapy | II | Clinical efficacy and safety | First line | Active Not recruiting | NCT02014636 |
| KEYNOTE-426 | pembrolizumab + axitinib | sunitinib | III | PFS, OS | First line | Recruiting | NCT02853331 |
| E7080-G000-307 | lenvatinib + pembrolizumab or everolimus | sunitinib | III | PFS | First line | Recruiting | NCT02811861 |
| N.a. | pembrolizumab + axitinib | / | Ib | Safety, treatment efficacy | First line | Active | NCT02133742 |
| N.a. | pembrolizumab + lenvatinib | / | Ib/II | MTD, ORR | No standard therapies anymore available | Active | NCT02501096 |
| BTCRC-GU14-003 | pembrolizumab + bevacizumab | / | Ib/II | Safety, efficacy tolerability | At least second line | Active Not recruiting | NCT02348008 |
| N.a. | atezolizumab + MOXR0916 + bevacizumab | atezolizumab + MOXR0916 | I | Dose limiting toxicities Side effects | Any | Recruiting | NCT02410512 |
| CheckMate 016 | nivolumab + sunitinib or pazopanib or ipilimumab | nivolumab | I | Safety tolerability | First line Second line | Recruiting | NCT01472081 |
| N.a. | cabozantinib + nivolumab | cabozantinib + nivolumab + ipilimumab | I | Safety tolerability | No standard therapies anymore available | Recruiting | NCT02496208 |
| IMmotion150 | atezolizumab +/−bevacizumab | sunitinib | II | PFS | First line | Active Not recruiting | NCT01984242 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pircher, A.; Wolf, D.; Heidenreich, A.; Hilbe, W.; Pichler, R.; Heidegger, I. Synergies of Targeting Tumor Angiogenesis and Immune Checkpoints in Non-Small Cell Lung Cancer and Renal Cell Cancer: From Basic Concepts to Clinical Reality. Int. J. Mol. Sci. 2017, 18, 2291. https://doi.org/10.3390/ijms18112291
Pircher A, Wolf D, Heidenreich A, Hilbe W, Pichler R, Heidegger I. Synergies of Targeting Tumor Angiogenesis and Immune Checkpoints in Non-Small Cell Lung Cancer and Renal Cell Cancer: From Basic Concepts to Clinical Reality. International Journal of Molecular Sciences. 2017; 18(11):2291. https://doi.org/10.3390/ijms18112291
Chicago/Turabian StylePircher, Andreas, Dominik Wolf, Axel Heidenreich, Wolfgang Hilbe, Renate Pichler, and Isabel Heidegger. 2017. "Synergies of Targeting Tumor Angiogenesis and Immune Checkpoints in Non-Small Cell Lung Cancer and Renal Cell Cancer: From Basic Concepts to Clinical Reality" International Journal of Molecular Sciences 18, no. 11: 2291. https://doi.org/10.3390/ijms18112291
APA StylePircher, A., Wolf, D., Heidenreich, A., Hilbe, W., Pichler, R., & Heidegger, I. (2017). Synergies of Targeting Tumor Angiogenesis and Immune Checkpoints in Non-Small Cell Lung Cancer and Renal Cell Cancer: From Basic Concepts to Clinical Reality. International Journal of Molecular Sciences, 18(11), 2291. https://doi.org/10.3390/ijms18112291