
FKBP51 Immunohistochemical Expression: A New Prognostic Biomarker for OSCC?

 ,
,  , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Study Population
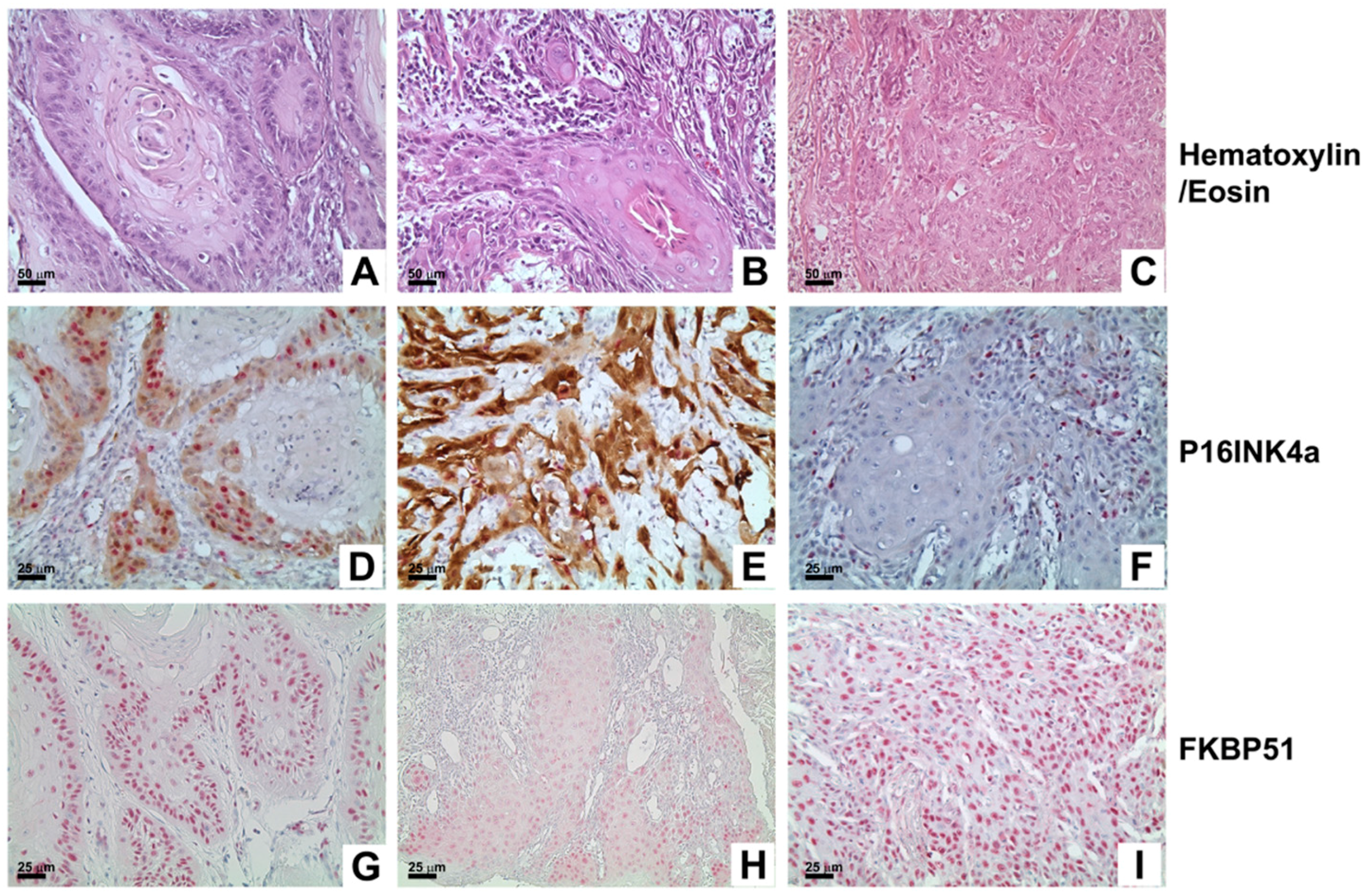
2.2. Immunohistochemical Staining and Statistical Analysis
2.3. Bayesian Statistic
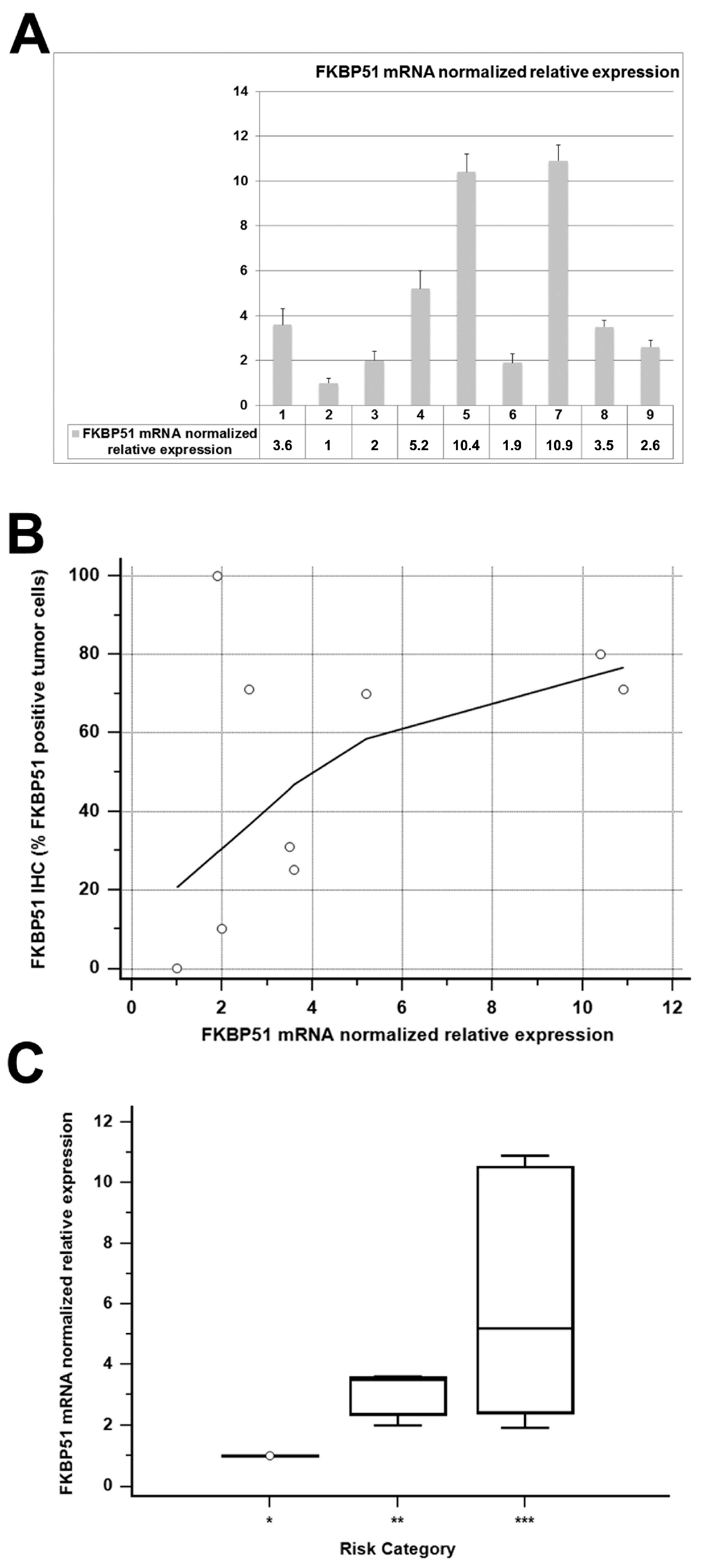
2.4. FKBP51 mRNA Expression
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. Immunohistochemistry
4.3. HPV Testing and Genotyping
4.4. Real-Time PCR
4.5. Statistical Analysis
4.6. Bayesian Statistic
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FKBP51 | FK binding protein 51 |
| SCC | Squamous cell carcinoma |
| HNC | Head and neck cancer |
| OSCC | Oral squamous cell carcinoma |
| HPV | Human papilloma virus |
| IHC | Immunohistochemistry |
References
- Argiris, A.; Karamouzis, M.V.; Raben, D.; Ferris, R.L. Head and neck cancer. Lancet 2008, 371, 1695–1709. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-tieulent, J.; Jemal, A. Global cancer statistics, 2012. Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Simard, E.P.; Torre, L.A.; Jemal, A. International trends in head and neck cancer incidence rates: Differences by country, sex and anatomic site. Oral Oncol. 2014, 50, 387–403. [Google Scholar] [CrossRef] [PubMed]
- AIOM-AIRTUM work group (AA.VV). I Numeri del Cancro in Italia; Il pensiero scientifico editore: Rome, Italy, 2016. [Google Scholar]
- Lewis, A.; Kang, R.; Levine, A.; Maghami, E. The new face of head and neck cancer: The HPV epidemic. Oncology 2015, 29, 616–626. [Google Scholar] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case-control study of human papillomavirus and oropharyngeal cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Castellsagué, X.; de González, A.B.; Gissmann, L. Chapter 1: HPV in the etiology of human cancer. Vaccine 2006, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Combes, J.-D.; Franceschi, S. Role of human papillomavirus in non-oropharyngeal head and neck cancers. Oral Oncol. 2014, 50, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Isayeva, T.; Li, Y.; Maswahu, D.; Brandwein-Gensler, M. Human papillomavirus in non-oropharyngeal head and neck cancers: A systematic literature review. Head Neck Pathol. 2012, 6, 104–120. [Google Scholar] [CrossRef] [PubMed]
- Walter, V.; Yin, X.; Wilkerson, M.D.; Cabanski, C.R.; Zhao, N.; Du, Y.; Ang, M.K.; Hayward, M.C.; Salazar, A.H.; Hoadley, K.A.; et al. Molecular subtypes in head and neck cancer exhibit distinct patterns of chromosomal gain and loss of canonical cancer genes. PLoS ONE 2013, 8, e56823. [Google Scholar] [CrossRef]
- Kang, H.; Kiess, A.; Chung, C.H. Emerging biomarkers in head and neck cancer in the era of genomics. Nat. Rev. Clin. Oncol. 2015, 12, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Avellino, R.; Romano, S.; Parasole, R.; Bisogni, R.; Lamberti, A.; Poggi, V.; Venuta, S.; Romano, M.F. Rapamycin stimulates apoptosis of childhood acute lymphoblastic leukemia cells. Blood 2005, 106, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; D’Angelillo, A.; Pacelli, R.; Staibano, S.; De Luna, E.; Bisogni, R.; Eskelinen, E.-L.; Mascolo, M.; Calì, G.; Arra, C.; et al. Role of FK506-binding protein 51 in the control of apoptosis of irradiated melanoma cells. Cell Death Differ. 2010, 17, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Dornan, J.; Taylor, P.; Walkinshaw, M.D. Structures of immunophilins and their ligand complexes. Curr. Top. Med. Chem. 2003, 3, 1392–1409. [Google Scholar] [CrossRef] [PubMed]
- Somarelli, J.A.; Lee, S.Y.; Skolnick, J.; Herrera, R.J. Structure-based classification of 45 FK506-binding proteins. Proteins 2008, 72, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; D’Angelillo, A.; Romano, M.F. Pleiotropic roles in cancer biology for multifaceted proteins FKBPs. Biochim. Biophys. Acta 2015, 1850, 2061–2068. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Zhang, B.; Miller, M.; Butko, E.; Wu, X.; Laver, T.; Kernag, C.; Kim, J.; Luo, Y.; Lamparski, H.; et al. Fully automated RNAscope in situ hybridization assays for formalin-fixed paraffin-embedded cells and tissues. J. Cell. Biochem. 2016, 117, 2201–2208. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA.
- O’Malley, A.J.; Zou, K.H.; Fielding, J.R.; Tempany, C.M.C. Bayesian regression methodology for estimating a receiver operating characteristic curve with two radiologic applications: Prostate biopsy and spiral CT of ureteral stones 1. Acad. Radiol. 2001, 8, 713–725. [Google Scholar] [CrossRef]
- Wittekindt, C.; Wagner, S.; Mayer, C.S.; Klussmann, J.P. Basics of tumor development and importance of human papilloma virus (HPV) for head and neck cancer. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2012. [Google Scholar] [CrossRef]
- Ramqvist, T.; Dalianis, T. Oropharyngeal cancer epidemic and human papillomavirus. Emerg. Infect. Dis. 2010, 16, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Gualeni, A.V.; Volpi, C.C.; Carbone, A.; Gloghini, A. A novel semi-automated in situ hybridisation protocol for microRNA detection in paraffin embedded tissue sections. J. Clin. Pathol. 2015, 68, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Mallen-St Clair, J.; Alani, M.; Wang, M.B.; Srivastan, E.S. Human papillomavirus in oropharyngeal cancer: The changing face of a disease. Biochim. Biophys. Acta Rev. Cancer 2016, 1866, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Rischin, D.; Young, R.J.; Fisher, R.; Fox, S.B.; Le, Q.T.; Peters, L.J.; Solomon, B.; Choi, J.; O’Sullivan, B.; Kenny, L.M.; et al. Prognostic significance of P16INKa and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J. Clin. Oncol. 2010, 28, 4142–4148. [Google Scholar] [CrossRef] [PubMed]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV-associated P16INK4a expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.C.; Lingen, M.W.; Perez-Ordonez, B.; He, X.; Pickard, R.; Koluder, M.; Jiang, B.; Wakely, P.; Xiao, W.; Gillison, M.L. Validation of methods for oropharyngeal cancer HPV status determination in US cooperative group trials. Am. J. Surg. Pathol. 2012, 36, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Tomar, S.; Graves, C.A.; Altomare, D.; Kowli, S.; Kassler, S.; Sutkowski, N.; Gillespie, M.B.; Creek, K.E.; Pirisi, L. Human papillomavirus status and gene expression profiles of oropharyngeal and oral cancers from European American and African American patients. Head Neck 2016, 38, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Stephen, J.K.; Divine, G.; Chen, K.M.; Chitale, D.; Havard, S.; Worsham, M.J. Significance of p16 in site-specific HPV positive and HPV negative head and neck squamous cell carcinoma. Cancer Clin. Oncol. 2013, 2, 51–61. [Google Scholar] [PubMed]
- Larsen, C.G.; Gyldenløve, M.; Jensen, D.H.; Therkildsen, M.H.; Kiss, K.; Norrild, B.; Konge, L.; Von Buchwald, C. Correlation between human papillomavirus and p16 overexpression in oropharyngeal tumours: A systematic review. Br. J. Cancer 2014, 110, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, G.; Zambrano, N.; Merolla, F.; Siano, M.; Varricchio, S.; Vecchione, M.; De Rosa, G.; Mascolo, M.; Staibano, S. Histopathological determinants of tumor resistance: A special look to the immunohistochemical expression of carbonic anhydrase IX in human cancers. Curr. Med. Chem. 2014, 21, 1569–1582. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, M.; Ilardi, G.; Romano, M.F.; Celetti, A.; Siano, M.; Romano, S.; Luise, C.; Merolla, F.; Rocco, A.; Vecchione, M.L.; et al. Overexpression of chromatin assembly factor-1 p60, poly(ADP-ribose) polymerase 1 and nestin predicts metastasizing behaviour of oral cancer. Histopathology 2012, 61, 1089–1105. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; D’Angelillo, A.; Staibano, S.; Ilardi, G.; Romano, M.F. FK506-binding protein 51 is a possible novel tumoral marker. Cell Death Dis. 2010, 1, e55. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, M.; Vecchione, M.L.; Ilardi, G.; Scalvenzi, M.; Molea, G.; Di Benedetto, M.; Nugnes, L.; Siano, M.; de Rosa, G.; Staibano, S. Overexpression of chromatin assembly factor-1/p60 helps to predict the prognosis of melanoma patients. BMC Cancer 2010, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Staibano, S.; Mascolo, M.; Ilardi, G.; Siano, M.; De Rosa, G. Immunohistochemical analysis of FKBP51 in human cancers. Curr. Opin. Pharmacol. 2011, 11, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Sorrentino, A.; Di Pace, A.L.; Nappo, G.; Mercogliano, C.; Romano, M.F. The emerging role of large immunophilin FK506 binding protein 51 in cancer. Curr. Med. Chem. 2011, 18, 5424–5429. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Mallardo, M.; Romano, M.F. FKBP51 and the NF-κB regulatory pathway in cancer. Curr. Opin. Pharmacol. 2011, 11, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Gaali, S.; Kirschner, A.; Cuboni, S.; Hartmann, J.; Kozany, C.; Balsevich, G.; Namendorf, C.; Fernandez-Vizarra, P.; Sippel, C.; Zannas, A.S.; et al. Selective inhibitors of the FK506-binding protein 51 by induced fit. Nat. Chem. Biol. 2014, 11, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Xiao, Y.; Nakaya, M.; D’Angelillo, A.; Chang, M.; Jin, J.; Hausch, F.; Masullo, M.; Feng, X.; Romano, M.F.; et al. FKBP51 employs both scaffold and isomerase functions to promote NF-κB activation in melanoma. Nucleic Acids Res. 2015, 43, 6983–6993. [Google Scholar] [CrossRef] [PubMed]
- Gaali, S.; Feng, X.; Hähle, A.; Sippel, C.; Bracher, A.; Hausch, F. Rapid, Structure-Based Exploration of pipecolic acid amides as novel selective antagonists of the FK506-binding protein 51. J. Med. Chem. 2016, 59, 2410–2422. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HPV Status | ||||
|---|---|---|---|---|
| - | HPV Positive | HPV Negative | Sub-Total | |
| (% Sub-Total) | (% Sub-Total) | (% Total) | ||
| 6 (8.3%) | 66 (91.7%) | 72 (100%) | ||
| Gender | male | 4 (10%) | 36 (90%) | 40 (55.6%) |
| female | 2 (6.3%) | 30 (93.8%) | 32 (44.4%) | |
| Age | Mean | 59.5 | 64.1 | 63.8 |
| Range | 44–72 | 29–89 | 29–89 | |
| Tumor stage | T1 | 0 | 10 (100%) | 10 (13.9%) |
| T2 | 2 (8%) | 23 (92%) | 25 (34.7%) | |
| T3 | 0 | 2 (100%) | 2 (2.8%) | |
| T4 | 0 | 30 (100%) | 30 (41.7%) | |
| unknown | 4 (80%) | 1 (20%) | 5 (6.9%) | |
| Nodal stage | Nx | - | 6 (100%) | 6 (8.3%) |
| N0 | 1 (3.6%) | 27 (96.4%) | 28 (38.9%) | |
| N1 | 1 (6.7%) | 14 (93.3%) | 15 (20.8%) | |
| N2 | - | 18 (100%) | 18 (25.0%) | |
| N3 | - | 1 (100%) | 1 (1.4%) | |
| unknown | 4 (100%) | 0 | 4 (5.6%) | |
| Stage | I | - | 8 (100%) | 8 (11.1%) |
| II | 1 (6.7%) | 14 (93.3%) | 15 (20.8%) | |
| III | 1 (16.7%) | 5 (83.3%) | 6 (8.3%) | |
| IV | - | 38 (100%) | 38 (52.8%) | |
| Unknown | 4 (80%) | 1 (20%) | 5 (6.9%) | |
| Histological tumor differentiation | Poor | - | 40 (100%) | 40 (55.6%) |
| Moderate | - | 23 (100%) | 23 (31.9%) | |
| Well | - | 3 (100%) | 3 (4.2%) | |
| unknown | 6 (100%) | - | 6 (8.3%) | |
| Anatomical primary site of tumor | OP | 6 (23.1%) | 20 (76.9%) | 26 (36.1%) |
| NOP | 0 | 46 (100%) | 46 (63.9%) | |
| Follow-up | DOD | - | 32 (100%) | 32 (44.4%) |
| W&A | 6 (18.2%) | 27 (81.8%) | 33 (45.8%) | |
| Unknown | - | 7 (100%) | 7 (9.7%) | |
| Title | Value |
|---|---|
| Area under the ROC curve (AUC) | 0.907 |
| Standard error | 0.0394 |
| 95% Confidence interval | 0.806–0.966 |
| z Statistic | 10.332 |
| Significance level P (Area = 0.5) | <0.0001 |
| Youden index J | 0.8013 |
| Associated criterion | >51 |
| Sensitivity | 88.46 |
| Specificity | 91.67 |
| Source of Variation | Sum of Squares | Degree of Freedom (DF) | Mean Square |
|---|---|---|---|
| Between groups (influence factor) | 86,791,323 | 1 | 86,791,323 |
| Within groups (other fluctuations) | 469,380,677 | 68 | 6,902,657 |
| Total | 556,172,000 | 69 | - |
| F-ratio | - | - | 12,574 |
| Significance level | - | - | p = 0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, D.; Merolla, F.; Mascolo, M.; Ilardi, G.; Romano, S.; Varricchio, S.; Napolitano, V.; Celetti, A.; Postiglione, L.; Di Lorenzo, P.P.; et al. FKBP51 Immunohistochemical Expression: A New Prognostic Biomarker for OSCC? Int. J. Mol. Sci. 2017, 18, 443. https://doi.org/10.3390/ijms18020443
Russo D, Merolla F, Mascolo M, Ilardi G, Romano S, Varricchio S, Napolitano V, Celetti A, Postiglione L, Di Lorenzo PP, et al. FKBP51 Immunohistochemical Expression: A New Prognostic Biomarker for OSCC? International Journal of Molecular Sciences. 2017; 18(2):443. https://doi.org/10.3390/ijms18020443
Chicago/Turabian StyleRusso, Daniela, Francesco Merolla, Massimo Mascolo, Gennaro Ilardi, Simona Romano, Silvia Varricchio, Virginia Napolitano, Angela Celetti, Loredana Postiglione, Pier Paolo Di Lorenzo, and et al. 2017. "FKBP51 Immunohistochemical Expression: A New Prognostic Biomarker for OSCC?" International Journal of Molecular Sciences 18, no. 2: 443. https://doi.org/10.3390/ijms18020443
APA StyleRusso, D., Merolla, F., Mascolo, M., Ilardi, G., Romano, S., Varricchio, S., Napolitano, V., Celetti, A., Postiglione, L., Di Lorenzo, P. P., Califano, L., Dell’Aversana, G. O., Astarita, F., Romano, M. F., & Staibano, S. (2017). FKBP51 Immunohistochemical Expression: A New Prognostic Biomarker for OSCC? International Journal of Molecular Sciences, 18(2), 443. https://doi.org/10.3390/ijms18020443