Molecular and Clinicopathological Differences by Age at the Diagnosis of Colorectal Cancer

Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Clinical Data
4.2. Collection of Tumor Tissues
4.3. DNA Isolation and Quantification
4.4. MassArray-based Mutation Characterization
4.5. MSI Analysis
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| APC | Adenomatous Polyposis Coli |
| BRAF | B-Raf proto-oncogene |
| CSS | Cancer Specific Survival |
| CRC | Colorectal cancer |
| CI | Confidence interval |
| CIMP | CpG island methylator phenotype |
| FBXW7 | F-box and WD repeat domain containing 7 |
| KRAS | KRAS proto-oncogene |
| LVI | Lymphovascular invasion |
| MSI | Microsatellite instability |
| OS | Overall survival |
| PCR | Polymerase chain reaction |
| PI3K | Phosphoinositol-3-kinase |
| PTEN | phosphatase and tensin homolog |
| TGF-β | Transforming growth factor beta |
| TNM | Tumor-Node-Metastasis |
References
- The Department of Health. Healthy Statistics: Cancer Registry Annual Report in Taiwan Area; The Department of Health, the Executive Yuan: Chiayi City, Taiwan, 2007.
- Abdelsattar, Z.M.; Wong, S.L.; Regenbogen, S.E.; Jomaa, D.M.; Hardiman, K.M.; Hendren, S. Colorectal cancer outcomes and treatment patterns in patients too young for average-risk screening. Cancer 2016, 122, 929–934. [Google Scholar] [CrossRef] [PubMed]
- De Magalhaes, J.P. How ageing processes influence cancer. Nat. Rev. Cancer 2013, 13, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Laurie, C.C.; Laurie, C.A.; Rice, K.; Doheny, K.F.; Zelnick, L.R.; McHugh, C.P.; Ling, H.; Hetrick, K.N.; Pugh, E.W.; Amos, C.; et al. Detectable clonal mosaicism from birth to old age and its relationship to cancer. Nat. Genet. 2012, 44, 642–650. [Google Scholar] [CrossRef] [PubMed]
- McCleary, N.J.; Sato, K.; Nishihara, R.; Inamura, K.; Morikawa, T.; Zhang, X.; Wu, K.; Yamauchi, M.; Kim, S.A.; Sukawa, Y.; et al. Prognostic Utility of Molecular Factors by Age at Diagnosis of Colorectal Cancer. Clin. Cancer Res. 2016, 22, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.M.; Marcet, J.E.; Frattini, J.C.; Prather, A.D.; Mateka, J.J.; Nfonsam, V.N. Is it time to lower the recommended screening age for colorectal cancer? J. Am. Coll. Surg. 2011, 213, 352–361. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Liu, J.H.; Etzioni, D.A.; Livingston, E.H.; Ko, C.Y. Rates of colon and rectal cancers are increasing in young adults. Am. Surg. 2003, 69, 866–872. [Google Scholar] [PubMed]
- You, Y.N.; Xing, Y.; Feig, B.W.; Chang, G.J.; Cormier, J.N. Young-onset colorectal cancer: Is it time to pay attention? Arch. Intern. Med. 2012, 172, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Sijmons, R.H.; Hofstra, R.M. Review: Clinical aspects of hereditary DNA Mismatch repair gene mutations. DNA Repair 2016, 38, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Maccaroni, E.; Bracci, R.; Giampieri, R.; Bianchi, F.; Belvederesi, L.; Brugiati, C.; Pagliaretta, S.; Del Prete, M.; Scartozzi, M.; Cascinu, S. Prognostic impact of mismatch repair genes germline defects in colorectal cancer patients: Are all mutations equal? Oncotarget 2015, 6, 38737–38748. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.T.; Pai, R.K.; Rybicki, L.A.; Dimaio, M.A.; Limaye, M.; Jayachandran, P.; Koong, A.C.; Kunz, P.A.; Fisher, G.A.; Ford, J.M.; et al. Clinicopathologic and molecular features of sporadic early-onset colorectal adenocarcinoma: An adenocarcinoma with frequent signet ring cell differentiation, rectal and sigmoid involvement, and adverse morphologic features. Mod. Pathol. 2012, 25, 1128–1139. [Google Scholar] [CrossRef] [PubMed]
- Goel, G. Evolving role of gene expression signatures as biomarkers in early-stage colon cancer. J. Gastrointest. Cancer 2014, 45, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Limburg, P.J.; Harmsen, W.S.; Chen, H.H.; Gallinger, S.; Haile, R.W.; Baron, J.A.; Casey, G.; Woods, M.O.; Thibodeau, S.N.; Lindor, N.M. Prevalence of alterations in DNA mismatch repair genes in patients with young-onset colorectal cancer. Clin. Gastroenterol. Hepatol. 2011, 9, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Kothari, N.; Teer, J.K.; Abbott, A.M.; Srikumar, T.; Zhang, Y.; Yoder, S.J.; Brohl, A.S.; Kim, R.D.; Reed, D.R.; Shibata, D. Increased incidence of FBXW7 and POLE proofreading domain mutations in young adult colorectal cancers. Cancer 2016, 122, 2828–2835. [Google Scholar] [CrossRef] [PubMed]
- Fairley, T.L.; Cardinez, C.J.; Martin, J.; Alley, L.; Friedman, C.; Edwards, B.; Jamison, P. Colorectal cancer in U.S. adults younger than 50 years of age, 1998–2001. Cancer 2006, 107, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Mendoza Silveiras, J.; Greenamyer, J.; Guiffre, S.; Axilbund, J.; Spiegel, A.; You, Y.N. The increasing incidence of young-onset colorectal cancer: A call to action. Mayo Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; De, P. Trends in colorectal cancer incidence and related lifestyle risk factors in 15-49-year-olds in Canada, 1969–2010. Cancer Epidemiol. 2016, 42, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Society. Risk Factors for Colorectal Cancer. Available online: http://www.cancer.ca/en/cancer-information/cancer-type/colorectal/risks/?region=on (accessed on 28 June 2017).
- World Cancer Research Fund (WCRF) Panel. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; World Cancer Research Fund: Washington, DC, USA, 2007. [Google Scholar]
- Ferrari, P.; Jenab, M.; Norat, T.; Moskal, A.; Slimani, N.; Olsen, A.; Tjonneland, A.; Overvad, K.; Jensen, M.K.; Boutron-Ruault, M.C.; et al. Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation into cancer and nutrition (EPIC). Int. J. Cancer 2007, 121, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Paskett, E.D.; Reeves, K.W.; Rohan, T.E.; Allison, M.A.; Williams, C.D.; Messina, C.R.; Whitlock, E.; Sato, A.; Hunt, J.R. Association between cigarette smoking and colorectal cancer in the Women’s Health Initiative. J. Natl. Cancer Inst. 2007, 99, 1729–1735. [Google Scholar] [CrossRef] [PubMed]
- Botteri, E.; Iodice, S.; Bagnardi, V.; Raimondi, S.; Lowenfels, A.B.; Maisonneuve, P. Smoking and colorectal cancer: A meta-analysis. JAMA 2008, 300, 2765–2778. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Morley, T.S.; Kim, M.; Clegg, D.J.; Scherer, P.E. Obesity and cancer-mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E. Insulin, insulin-like growth factors and colon cancer: A review of the evidence. J. Nutr. 2001, 131, 3109s–3120s. [Google Scholar] [PubMed]
- Inamura, K.; Song, M.; Jung, S.; Nishihara, R.; Yamauchi, M.; Lochhead, P.; Qian, Z.R.; Kim, S.A.; Mima, K.; Sukawa, Y.; et al. Prediagnosis Plasma Adiponectin in Relation to Colorectal Cancer Risk According to KRAS Mutation Status. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [PubMed]
- Heald, B.; Mester, J.; Rybicki, L.; Orloff, M.S.; Burke, C.A.; Eng, C. Frequent gastrointestinal polyps and colorectal adenocarcinomas in a prospective series of PTEN mutation carriers. Gastroenterology 2010, 139, 1927–1933. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, G.A.; Der, C.J.; Rossman, K.L. RAS isoforms and mutations in cancer at a glance. J. Cell Sci. 2016, 129, 1287–1292. [Google Scholar] [CrossRef] [PubMed]
- Fetics, S.K.; Guterres, H.; Kearney, B.M.; Buhrman, G.; Ma, B.; Nussinov, R.; Mattos, C. Allosteric effects of the oncogenic RasQ61L mutant on Raf-RBD. Structure 2015, 23, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Witkiewicz, A.K.; McMillan, E.A.; Balaji, U.; Baek, G.; Lin, W.C.; Mansour, J.; Mollaee, M.; Wagner, K.U.; Koduru, P.; Yopp, A.; et al. Whole-exome sequencing of pancreatic cancer defines genetic diversity and therapeutic targets. Nat. Commun. 2015, 6, 6744. [Google Scholar] [CrossRef] [PubMed]
- Magnani, G.; Furlan, D.; Sahnane, N.; Reggiani Bonetti, L.; Domati, F.; Pedroni, M. Molecular features and methylation status in early onset (</=40 Years) colorectal cancer: A population based, case-control study. Gastroenterol. Res. Pract. 2015, 2015, 132190. [Google Scholar] [CrossRef] [PubMed]
- Sheaffer, K.L.; Elliott, E.N.; Kaestner, K.H. DNA hypomethylation contributes to genomic instability and intestinal cancer initiation. Cancer Prev. Res. 2016, 9, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Wolff, E.M.; Byun, H.M.; Han, H.F.; Sharma, S.; Nichols, P.W.; Siegmund, K.D.; Yang, A.S.; Jones, P.A.; Liang, G. Hypomethylation of a LINE-1 promoter activates an alternate transcript of the MET oncogene in bladders with cancer. PLoS Genet. 2010, 6, e1000917. [Google Scholar] [CrossRef] [PubMed]
- Goelz, S.E.; Vogelstein, B.; Hamilton, S.R.; Feinberg, A.P. Hypomethylation of DNA from benign and malignant human colon neoplasms. Science 1985, 228, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.A.; Baylin, S.B. The epigenomics of cancer. Cell 2007, 128, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Antelo, M.; Balaguer, F.; Shia, J.; Shen, Y.; Hur, K.; Moreira, L.; Cuatrecasas, M.; Bujanda, L.; Giraldez, M.D.; Takahashi, M.; et al. A high degree of LINE-1 hypomethylation is a unique feature of early-onset colorectal cancer. PLoS ONE 2012, 7, e45357. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Yamauchi, M.; Nishihara, R.; Lochhead, P.; Qian, Z.R.; Kuchiba, A.; Kim, S.A.; Mima, K.; Sukawa, Y.; Jung, S.; et al. Tumor LINE-1 methylation level and microsatellite instability in relation to colorectal cancer prognosis. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.W.; Sundaram, V.; Chew, T.A.; Ladabaum, U. Advanced-stage colorectal cancer in persons younger than 50 years not associated with longer duration of symptoms or time to diagnosis. Clin. Gastroenterol. Hepatol. 2017, 15, 728–737. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Livingston, E.H.; Yo, C.K. Colorectal cancer in the young. Am. J. Surg. 2004, 187, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Taggarshe, D.; Rehil, N.; Sharma, S.; Flynn, J.C.; Damadi, A. Colorectal cancer: Are the “young” being overlooked? Am. J. Surg. 2013, 205, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Lin, P.C.; Yang, S.H.; Wang, H.S.; Liang, W.Y.; Lin, J.K. Taiwan hospital-based detection of Lynch syndrome distinguishes 2 types of microsatellite instabilities in colorectal cancers. Surgery 2010, 147, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.T.; Yang, S.H.; Lin, J.K.; Lin, C.C.; Wang, H.S.; Chen, W.S.; Lin, T.C.; Jiang, J.K.; Chang, S.C. Genetic variations are associated with lymph node metastasis in colorectal cancer patients. J. Surg. Oncol. 2014, 110, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Lin, P.C.; Lin, J.K.; Lin, C.H.; Yang, S.H.; Liang, W.Y.; Chen, W.S.; Jiang, J.K. Mutation spectra of common cancer-associated genes in different phenotypes of colorectal carcinoma without distant metastasis. Ann. Surg. Oncol. 2016, 23, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [CrossRef]
- Lin, J.K.; Lin, P.C.; Lin, C.H.; Jiang, J.K.; Yang, S.H.; Liang, W.Y.; Chen, W.S.; Chang, S.C. Clinical relevance of alterations in quantity and quality of plasma DNA in colorectal cancer patients: Based on the mutation spectra detected in primary tumors. Ann. Surg. Oncol. 2014, 21 (Suppl. S4), S680–S686. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.K.; Chang, S.C.; Yang, Y.C.; Li, A.F. Loss of heterozygosity and DNA aneuploidy in colorectal adenocarcinoma. Ann. Surg. Oncol. 2003, 10, 1086–1094. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
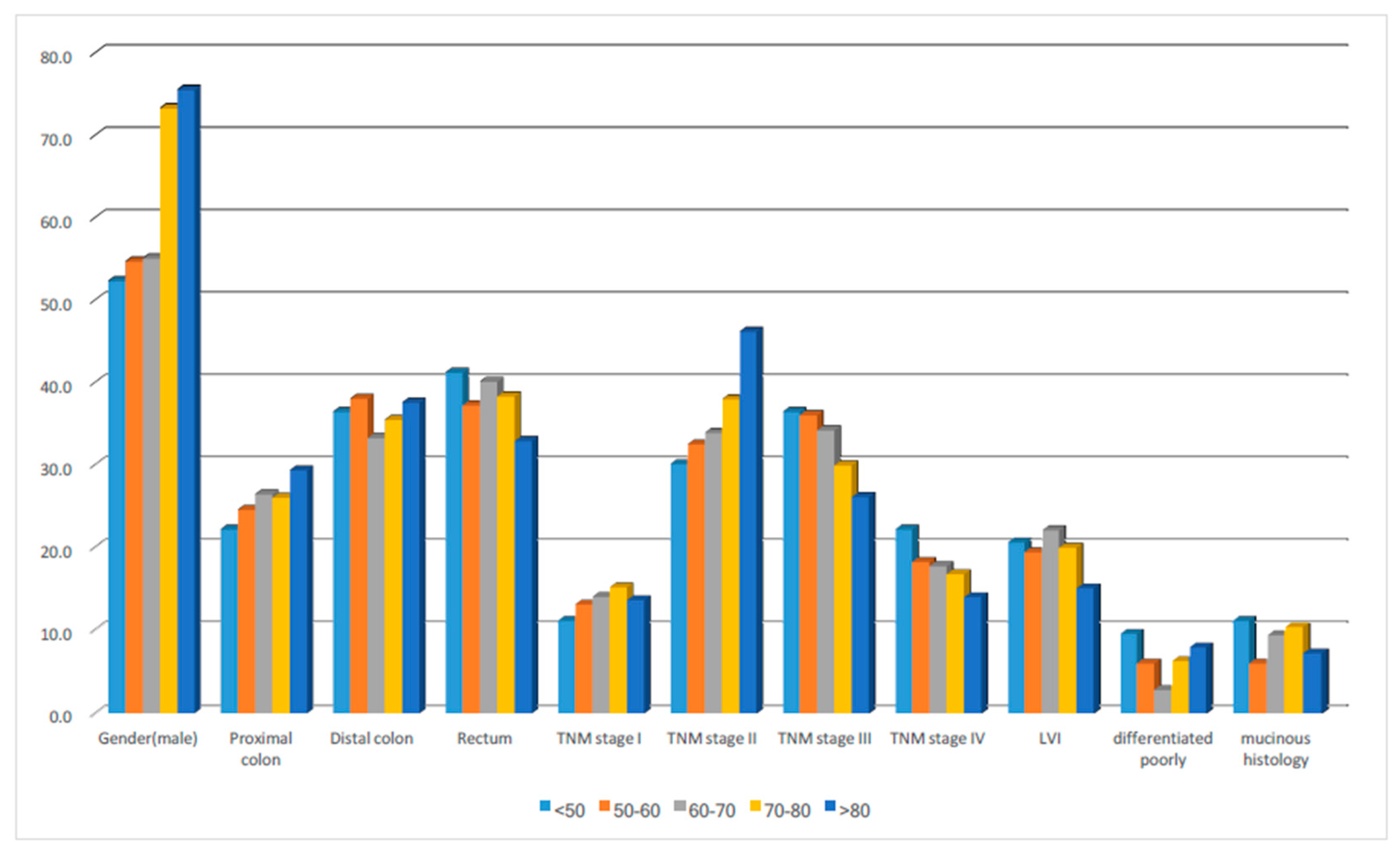
| Variable | <50 | % | 50–60 | % | 60–70 | % | 70–80 | % | >80 | % | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No./% | 63 | 4.3 | 252 | 17.1 | 321 | 21.8 | 560 | 38.0 | 279 | 18.9 | |
| Gender(male) | 33 | 52.4 | 138 | 54.8 | 177 | 55.1 | 411 | 73.4 | 211 | 75.6 | <0.001 |
| Location | |||||||||||
| Right | 14 | 22.2 | 62 | 24.6 | 85 | 26.5 | 146 | 26.1 | 82 | 29.4 | 0.719 |
| Left | 23 | 36.5 | 96 | 38.1 | 107 | 33.3 | 199 | 35.5 | 105 | 37.6 | |
| Rectum | 26 | 41.3 | 94 | 37.3 | 129 | 40.2 | 215 | 38.4 | 92 | 33.0 | |
| TNM stage | |||||||||||
| I | 7 | 11.1 | 33 | 13.1 | 45 | 14.0 | 85 | 15.2 | 38 | 13.6 | 0.083 |
| II | 19 | 30.2 | 82 | 32.5 | 109 | 34.0 | 213 | 38.0 | 129 | 46.2 | |
| III | 23 | 36.5 | 91 | 36.1 | 110 | 34.3 | 168 | 30.0 | 73 | 26.2 | |
| IV | 14 | 22.2 | 46 | 18.3 | 57 | 17.8 | 94 | 16.8 | 39 | 14.0 | |
| LVI | 13 | 20.6 | 49 | 19.4 | 71 | 22.1 | 112 | 20.0 | 42 | 15.1 | 0.281 |
| Poor differentiation | 6 | 9.5 | 15 | 6.0 | 9 | 2.8 | 35 | 6.3 | 22 | 7.9 | 0.058 |
| Mucinous histology | 7 | 11.1 | 15 | 6.0 | 30 | 9.3 | 58 | 10.4 | 20 | 7.2 | 0.223 |
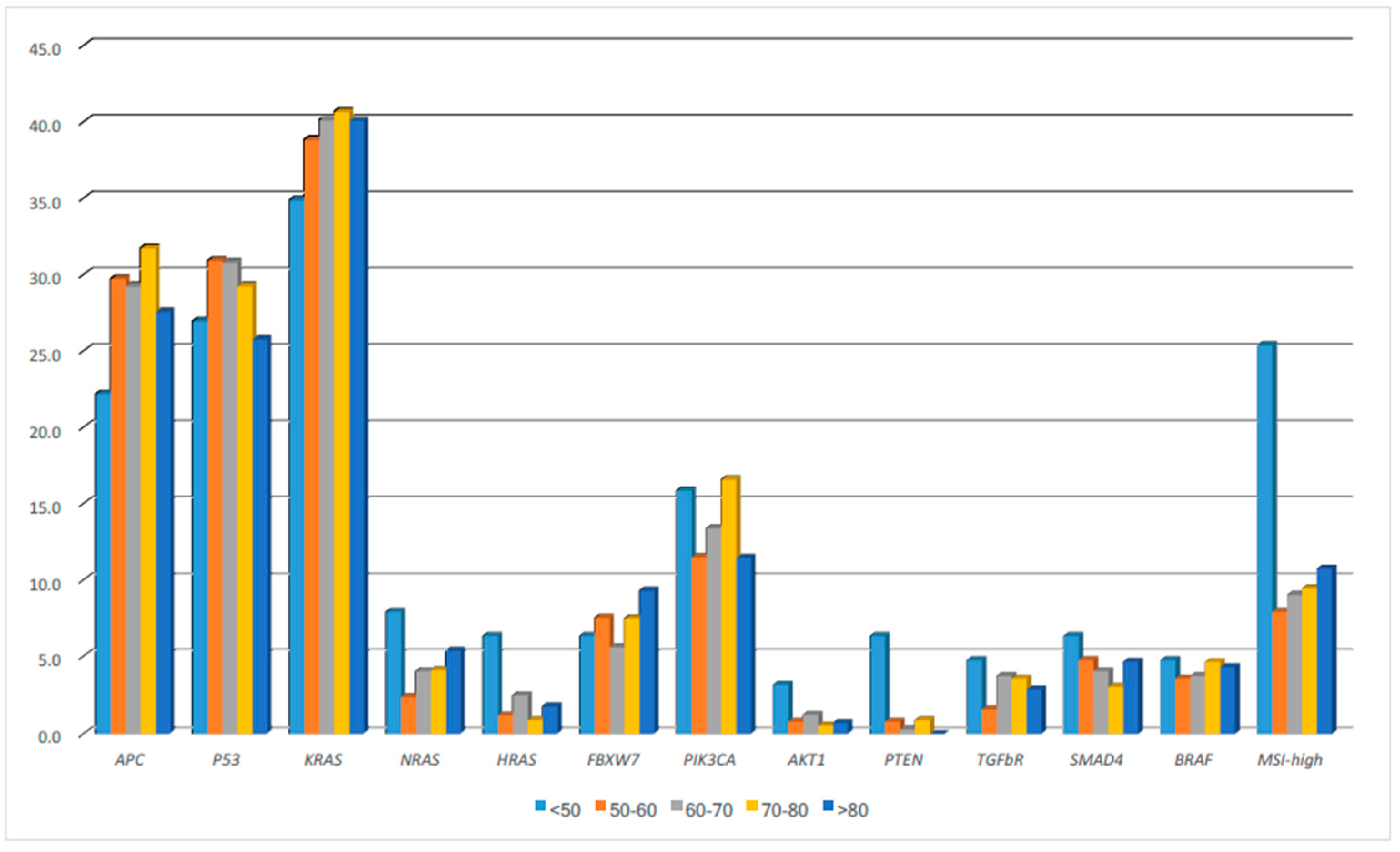
| Gene | <50 | % | 50–60 | % | 60–70 | % | 70–80 | % | >80 | % | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No/% | 63 | 4.3 | 252 | 17.1 | 321 | 21.8 | 560 | 38.0 | 279 | 18.9 | |
| APC | 14 | 22.2 | 75 | 29.8 | 94 | 29.3 | 178 | 31.8 | 77 | 27.6 | 0.482 |
| P53 | 17 | 27.0 | 78 | 31.0 | 99 | 30.8 | 164 | 29.3 | 72 | 25.8 | 0.645 |
| KRAS | 22 | 34.9 | 98 | 38.9 | 129 | 40.2 | 228 | 40.7 | 112 | 40.1 | 0.92 |
| NRAS | 5 | 7.9 | 6 | 2.4 | 13 | 4.0 | 23 | 4.1 | 15 | 5.4 | 0.263 |
| HRAS | 4 | 6.3 | 3 | 1.2 | 8 | 2.5 | 5 | 0.9 | 5 | 1.8 | 0.018 |
| FBXW7 | 4 | 6.3 | 19 | 7.5 | 18 | 5.6 | 42 | 7.5 | 26 | 9.3 | 0.537 |
| PIK3CA | 10 | 15.9 | 29 | 11.5 | 43 | 13.4 | 93 | 16.6 | 32 | 11.5 | 0.184 |
| AKT1 | 2 | 3.2 | 2 | 0.8 | 4 | 1.2 | 3 | 0.5 | 2 | 0.7 | 0.272 |
| PTEN | 4 | 6.3 | 2 | 0.8 | 1 | 0.3 | 5 | 0.9 | 0 | 0.0 | <0.001 |
| TGFbR | 3 | 4.8 | 4 | 1.6 | 12 | 3.7 | 20 | 3.6 | 8 | 2.9 | 0.513 |
| SMAD4 | 4 | 6.3 | 12 | 4.8 | 13 | 4.0 | 17 | 3.0 | 13 | 4.7 | 0.564 |
| BRAF | 3 | 4.8 | 9 | 3.6 | 12 | 3.7 | 26 | 4.6 | 12 | 4.3 | 0.945 |
| MSI-high | 16 | 25.4 | 20 | 7.9 | 29 | 9.0 | 53 | 9.5 | 30 | 10.8 | <0.001 |
| Variable | Hazard Ratio | 95% Confidence Interval | p |
|---|---|---|---|
| TNM | 4.56 | 3.99–5.21 | <0.001 |
| Lymphovascular invasion | 1.57 | 1.27–1.88 | <0.001 |
| Poorly differentiated | 1.60 | 1.16–2.22 | 0.004 |
| Mucinous histology | 1.15 | 0.86–1.54 | 0.339 |
| Age classification | 1.08 | 0.99–1.18 | 0.075 |
| Variable | Hazard Ratio | 95% Confidence Interval | p |
|---|---|---|---|
| TNM | 2.04 | 1.85–2.26 | <0.001 |
| Lymphovascular invasion | 1.54 | 1.28–1.86 | <0.001 |
| Poorly differentiated | 1.29 | 0.95–1.75 | 0.106 |
| Mucinous histology | 1.19 | 0.93–1.53 | 0.166 |
| Age classification | 1.46 | 1.35–1.58 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-C.; Lin, P.-C.; Lin, C.-C.; Lan, Y.-T.; Lin, H.-H.; Lin, C.-H.; Yang, S.-H.; Liang, W.-Y.; Chen, W.-S.; Jiang, J.-K.; et al. Molecular and Clinicopathological Differences by Age at the Diagnosis of Colorectal Cancer. Int. J. Mol. Sci. 2017, 18, 1441. https://doi.org/10.3390/ijms18071441
Chang C-C, Lin P-C, Lin C-C, Lan Y-T, Lin H-H, Lin C-H, Yang S-H, Liang W-Y, Chen W-S, Jiang J-K, et al. Molecular and Clinicopathological Differences by Age at the Diagnosis of Colorectal Cancer. International Journal of Molecular Sciences. 2017; 18(7):1441. https://doi.org/10.3390/ijms18071441
Chicago/Turabian StyleChang, Chu-Cheng, Pei-Ching Lin, Chun-Chi Lin, Yuan-Tzu Lan, Hung-Hsin Lin, Chien-Hsing Lin, Shung-Haur Yang, Wen-Yi Liang, Wei-Shone Chen, Jeng-Kai Jiang, and et al. 2017. "Molecular and Clinicopathological Differences by Age at the Diagnosis of Colorectal Cancer" International Journal of Molecular Sciences 18, no. 7: 1441. https://doi.org/10.3390/ijms18071441
APA StyleChang, C. -C., Lin, P. -C., Lin, C. -C., Lan, Y. -T., Lin, H. -H., Lin, C. -H., Yang, S. -H., Liang, W. -Y., Chen, W. -S., Jiang, J. -K., Lin, J. -K., & Chang, S. -C. (2017). Molecular and Clinicopathological Differences by Age at the Diagnosis of Colorectal Cancer. International Journal of Molecular Sciences, 18(7), 1441. https://doi.org/10.3390/ijms18071441