Microcephaly Prevalence in Infants Born to Zika Virus-Infected Women: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Results
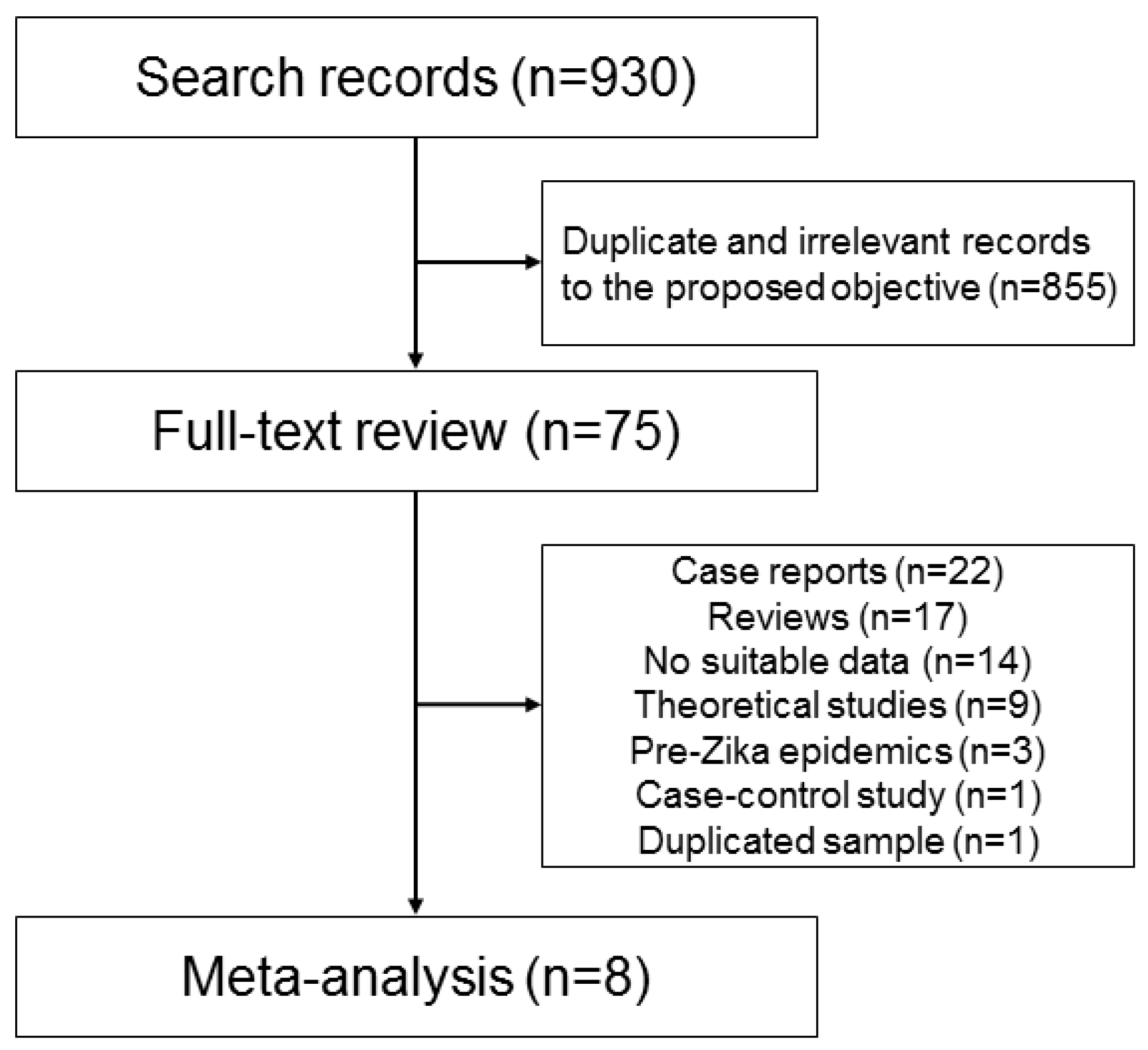
2.1. Selected Studies and Their Characteristics
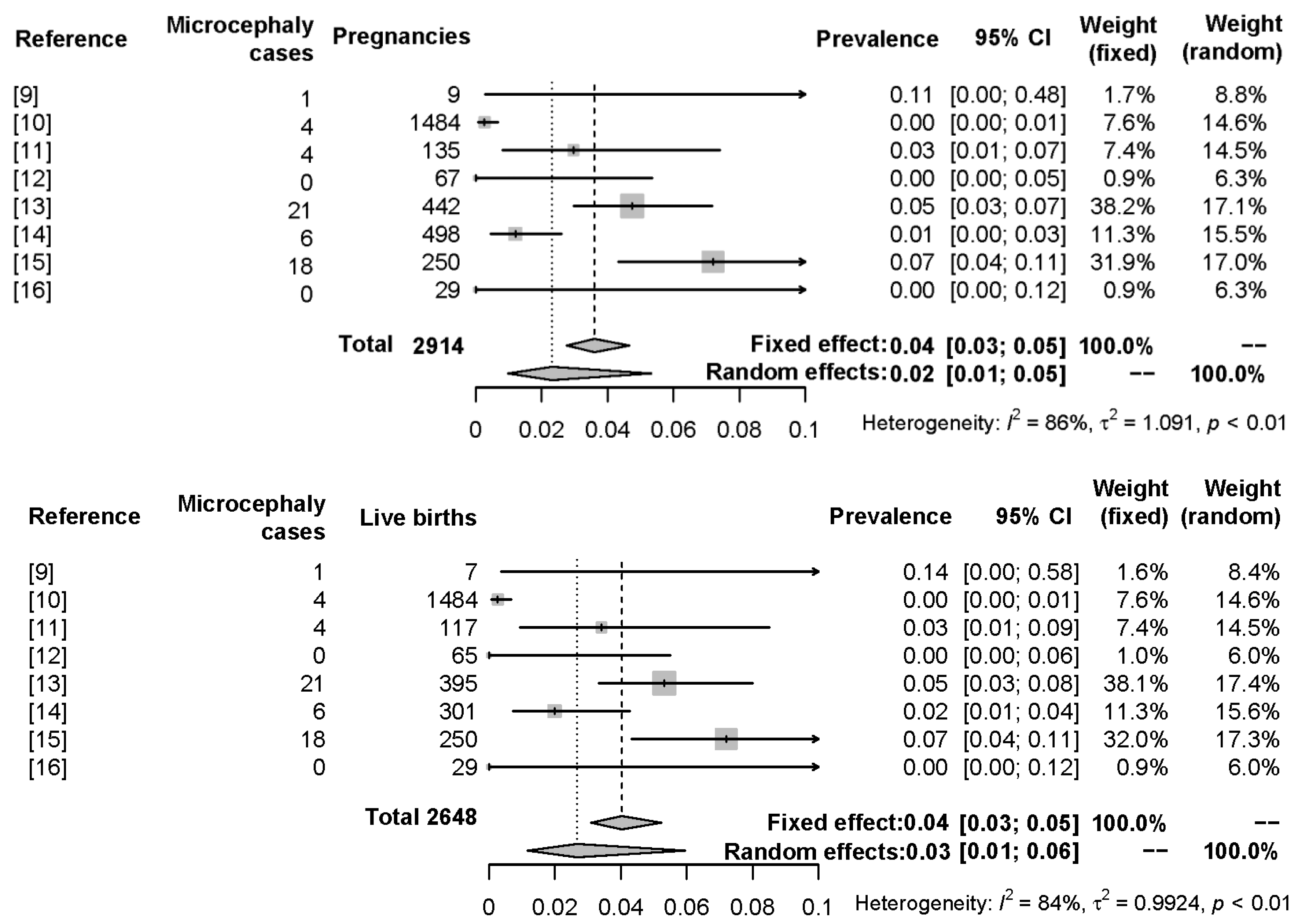
2.2. Meta-Analyses Results
3. Discussion
4. Materials and Methods
4.1. Systematic Review: Literature Search Strategy and Study Selection Criteria
4.2. Meta-Analysis Strategy
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Plourde, A.R.; Bloch, E.M. A literature review of Zika virus. Emerg. Infect. Dis. 2016, 22, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Sun, K.; Chinazzi, M.; Pastore y Piontti, A.; Dean, N.E.; Rojas, D.P.; Merler, S.; Mistry, D.; Poletti, P.; Rossi, L.; et al. Spread of Zika virus in the Americas. Proc. Natl. Acad. Sci. USA 2017, 114, E4334–E4343. [Google Scholar] [CrossRef] [PubMed]
- Paploski, I.A.D.; Prates, A.P.P.B.; Cardoso, C.W.; Kikuti, M.; Silva, M.M.O.; Waller, L.A.; Reis, M.G.; Kitron, U.; Ribeiro, G.S. Time lags between exanthematous illness attributed to Zika virus, Guillain-Barré syndrome, and microcephaly, Salvador, Brazil. Emerg. Infect. Dis. 2016, 22, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Fauci, A.S.; Morens, D.M. Zika virus in the Americas—Yet another arbovirus threat. N. Engl. J. Med. 2016, 374, 601–604. [Google Scholar] [CrossRef] [PubMed]
- De Brito, C.A.A.; de Brito, C.C.M.; Oliveira, A.C.; Rocha, M.; Atanásio, C.; Asfora, C.; Matos, J.D.; Lima, A.S.; Albuquerque, M.F.M. Zika in Pernambuco: Rewriting the first outbreak. Rev. Soc. Bras. Med. Trop. 2016, 49, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Faria, N.R.; da Silva Azevedo, R.D.S.; Kraemer, M.U.G.; Souza, R.; Cunha, M.S.; Hill, S.C.; Thézé, J.; Bonsall, M.B.; Bowden, T.A.; Rissanen, I.; et al. Zika virus in the Americas: Early epidemiological and genetic findings. Science 2016, 352, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Ministério da Saúde. Microcefalia: 1.638 Casos Confirmados Pelo Ministério da Saúde. Available online: http://portalsaude.saude.gov.br/index.php/cidadao/principal/agencia-saude/24350-microcefa-lia-1–638-casos-confirmados-pelo-ministerio-da-saude (accessed on 1 June 2017).
- Eickmann, S.H.; Carvalho, M.D.C.G.; Ramos, R.C.F.; Rocha, M.Â.W.; van der Linden, V.; da Silva, P.F.S. Síndrome da infecção congênita pelo vírus Zika. Cad. Saúde Pública 2016, 32, e00047716. [Google Scholar] [CrossRef] [PubMed]
- Meaney-Delman, D.; Hills, S.L.; Williams, C.; Galang, R.R.; Iyengar, P.; Hennenfent, A.K.; Rabe, I.B.; Panella, A.; Oduyebo, T.; Honein, M.A.; et al. Zika virus infection among U.S. pregnant travelers—August 2015–February 2016. Morb. Mortal. Wkly. Rep. 2016, 65, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, O.; Beltrán, M.; Nelson, C.A.; Valencia, D.; Tolosa, N.; Farr, S.L.; Padilla, A.V.; Tong, V.T.; Cuevas, E.L.; Espinosa-Bode, A.; et al. Zika virus disease in Colombia—Preliminary report. N. Engl. J. Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Brasil, P.; Pereira, J.; Jose, P.; Raja Gabaglia, C.; Damasceno, L.; Wakimoto, M.; Ribeiro Nogueira, R.M.; Carvalho de Sequeira, P.; Machado Siqueira, A.; Abreu de Carvalho, L.M.; et al. Zika virus infection in pregnant women in Rio de Janeiro—Preliminary report. N. Engl. J. Med. 2016, 375, 2321–2334. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.; Bello-Pagan, M.; Lozier, M.; Ryff, K.R.; Espinet, C.; Torres, J.; Perez-Padilla, J.; Febo, M.F.; Dirlikov, E.; Martinez, A.; et al. Update: ongoing Zika virus transmission—Puerto Rico, 1 November 2015–7 July 2016. Morb. Mortal. Wkly. Rep. 2016, 65, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Honein, M.A.; Dawson, A.L.; Petersen, E.E.; Jones, A.M.; Lee, E.H.; Yazdy, M.M.; Ahmad, N.; Macdonald, J.; Evert, N.; Bingham, A.; et al. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA 2016, 317, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Pomar, L.; Malinger, G.; Benoist, G.; Carles, G. Association between Zika virus and foetopathy: A prospective cohort study in French Guiana. Ultrasound Obstet. Gynecol. 2017, 49, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.R.; Jones, A.M.; Petersen, E.E.; Lee, E.H.; Rice, M.E.; Bingham, A.; Ellington, S.R.; Evert, N.; Reagan-Steiner, S.; Oduyebo, T.; et al. Vital signs: Update on Zika virus—Associated birth defects and evaluation of all U.S. infants with congenital Zika virus exposure—U.S. Zika pregnancy registry, 2016. Morb. Mortal. Wkly. Rep. 2017, 66, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, E.H.; Nelson, D.B.; Johnson, K.A.; Jacobs, S.; Rogers, V.L.; Roberts, S.; Sexton, T.; McIntire, D.D.; Casey, B. Infant outcomes among women with Zika virus infection during pregnancy: Results of a large prenatal Zika screening program. Am. J. Obstet. Gynecol. 2017, 216, 292.e1–292.e8. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic Tests for Zika Virus. Available online: https://www.cdc.gov/zika/hc-providers/types-of-tests.html (accessed on 30 May 2017).
- Chiodo, F.; Verucchi, G.; Mori, F.; Attard, L.; Ricchi, E. Infective diseases during pregnancy and their teratogenic effects. Ann. Ist. Super. Sanita 1993, 29, 57–67. [Google Scholar] [PubMed]
- Krauer, F.; Riesen, M.; Reveiz, L.; Oladapo, O.T.; Martínez-Vega, R.; Porgo, T.V.; Haefliger, A.; Broutet, N.J.; Low, N. Zika virus infection as a cause of congenital brain abnormalities and Guillain-Barré Syndrome: Systematic review. PLoS Med. 2017, 14, e1002203. [Google Scholar] [CrossRef] [PubMed]
- Cauchemez, S.; Besnard, M.; Bompard, P.; Dub, T.E.; Guillemette-Artur, P.; Eyrolle-Guignot, D.; Salje, H.; van Kerkhove, M.D.; Abadie, V.; Garel, C.; et al. Association between Zika virus and microcephaly in French Polynesia, 2013-15: A retrospective study. Lancet 2016, 387, 2125–2132. [Google Scholar] [CrossRef]
- Ellington, S.R.; Devine, O.; Bertolli, J.; Martinez Quiñones, A.; Shapiro-Mendoza, C.K.; Perez-Padilla, J.; Rivera-Garcia, B.; Simeone, R.M.; Jamieson, D.J.; Valencia-Prado, M.; et al. Estimating the number of Pregnant women infected with Zika virus and expected infants with microcephaly following the Zika Virus outbreak in Puerto Rico, 2016. JAMA Pediatr. 2016, 170, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, A.J.L.A.; de Magalhães-Barbosa, M.C.; Setta, F.L.; de Andrade Medronho, R.; Prata-Barbosa, A. Microcephaly case fatality rate associated with Zika virus infection in Brazil. Pediatr. Infect. Dis. J. 2016, 36, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.A.; Mier-Y-Teran-Romero, L.; Reefhuis, J.; Gilboa, S.M.; Hills, S.L. Zika and the risk of microcephaly. N. Engl. J. Med. 2016, 375, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Jaenisch, T.; Rosenberger, K.D.; Brito, C.; Brady, O.; Brasil, P.; Marques, E.T. Risk of microcephaly after Zika virus infection in Brazil, 2015 to 2016. Bull. World Health Organ. 2017, 95, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.R.; Chen, T.H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.; Dubray, C.; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Rankin, J.; Garne, E.; Loane, M.; Greenlees, R.; Addor, M.-C.; Arriola, L.; Barisic, I.; Bergman, J.E.H.; Csaky-Szunyogh, M.; et al. Prevalence of microcephaly in Europe: Population based study. BMJ 2016, 354, i4721. [Google Scholar] [CrossRef] [PubMed]
- Cragan, J.D.; Mai, C.T.; Petersen, E.E.; Liberman, R.F.; Forestieri, N.E.; Stevens, A.C.; Delaney, A.; Dawson, A.L.; Ellington, S.R.; Shapiro-mendoza, C.K.; et al. Baseline prevalence of birth defects associated with congenital Zika virus. Morb. Mortal. Wkly. Rep. 2017, 66, 219–220. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, T.V.B.; Rodrigues, L.C.; de Alencar Ximenes, R.A.; de Barros Miranda-Filho, D.; Montarroyos, U.R.; de Melo, A.P.L.; Valongueiro, S.; de Albuquerque, M.d.F.P.M.; Souza, W.V.; Braga, C.; et al. Association between Zika virus infection and microcephaly in Brazil, January to May, 2016: Preliminary report of a case-control study. Lancet Infect. Dis. 2016, 16, 1356–1363. [Google Scholar] [CrossRef]
- De Oliveira Melo, A.S.; Aguiar, R.S.; Amorim, M.M.R.; Arruda, M.B.; de Oliveira Melo, F.; Ribeiro, S.T.C.; Batista, A.G.M.; Ferreira, T.; Dos Santos, M.P.; Sampaio, V.V.; et al. Congenital Zika virus infection: Beyond neonatal microcephaly. JAMA Neurol. 2016, 73, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. Available online: http://www.casp-uk.net/checklists (accessed on 1 June 2017).
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [PubMed]
- Meta: General Package for Meta-Analysis. Available online: https://cran.r-project.org/web/packages/meta/index.html (accessed on 5 June 2017).
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria. Available online: https://www.R-project.org/ (accessed on 30 May 2017).



{kind=link}
{kind=link}
| Reference | Country | Enrolled Pregnant Women | Zika Virus-Infected Pregnant Women | Proportion of Symptomatic Women a | Live Births | Loss to Follow-up | Microcephaly Cases | Deaths b | Ocular Damage | Cardiovascular Damage | Other Organs Damage |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [9] | USA | 258 | 9 | 100.0% | 7 | 0 | 1 | 2 | NA | NA | NA |
| [10] | Colombia | 11,984 | 1484 | NR | 1484 | 0 | 4 | 0 | NA | NA | NA |
| [11] | Brazil | 345 | 135 | 27.0% | 117 | 9 | 4 | 9 | NA | NA | NA |
| [12] | Puerto Rico | 9343 | 67 | 100.0% | 65 | 0 | 0 | 2 | NA | NA | NA |
| [13] | USA | 442 | 442 | 38.0% | 395 | 0 | 21 | 47 | 0.9% | NA | NA |
| [14] | French Guiana | 1690 | 498 | 17.0% | 301 | 177 | 6 | 20 | 1.0% | 1.0% | 7.0% |
| [15] | USA | 1297 | 250 | 56.0% | 250 | 0 | 18 | 0 | NA | NA | 2.0% |
| [16] | USA | 14,161 | 29 | 17.0% | 29 | 0 | 0 | 0 | NA | NA | NA |
| Model | Outcome, Stratification | Pooled Estimate (Prevalence) | 95% Confidence Interval | Heterogeneity | ||
|---|---|---|---|---|---|---|
| τ2 | I2 | Q a, p-Value | ||||
| 1 | Microcephaly, all pregnancies (pooled n = 2914) | 2.3% | 1.0–5.3% | 1.09 | 85.6% | 48.6, <0.001 |
| 2 | Microcephaly, live births (pooled n = 2648) | 2.7% | 1.2–6.0% | 0.99 | 84.3% | 44.7, <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, A.V.C.; Crovella, S. Microcephaly Prevalence in Infants Born to Zika Virus-Infected Women: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2017, 18, 1714. https://doi.org/10.3390/ijms18081714
Coelho AVC, Crovella S. Microcephaly Prevalence in Infants Born to Zika Virus-Infected Women: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2017; 18(8):1714. https://doi.org/10.3390/ijms18081714
Chicago/Turabian StyleCoelho, Antonio Victor Campos, and Sergio Crovella. 2017. "Microcephaly Prevalence in Infants Born to Zika Virus-Infected Women: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 18, no. 8: 1714. https://doi.org/10.3390/ijms18081714
APA StyleCoelho, A. V. C., & Crovella, S. (2017). Microcephaly Prevalence in Infants Born to Zika Virus-Infected Women: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 18(8), 1714. https://doi.org/10.3390/ijms18081714