The Optimal PEG for Kidney Preservation: A Preclinical Porcine Study

 and
and
Abstract
:1. Introduction
2. Results
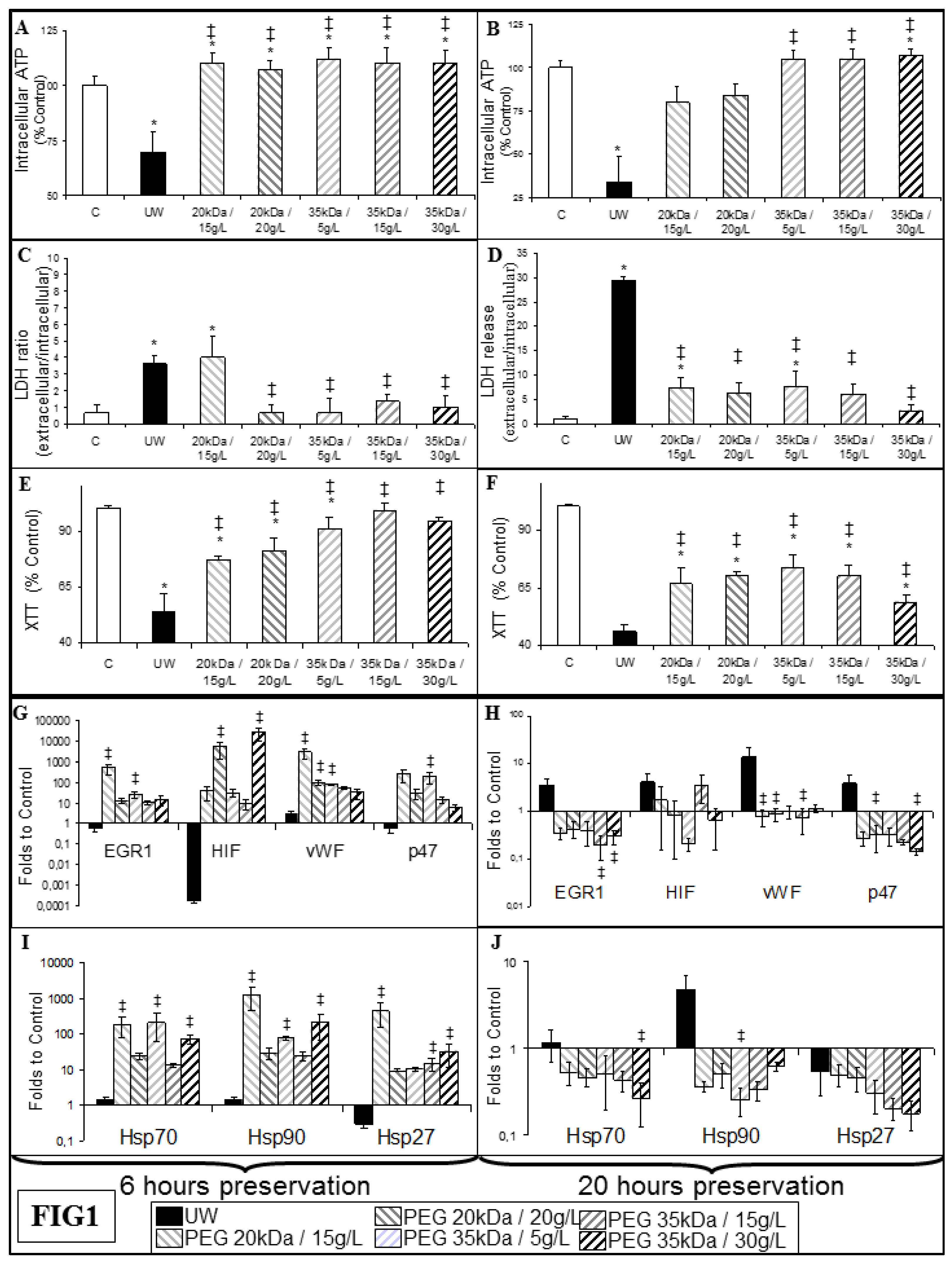
2.1. Protection from Hypoxia in Endothelial Cells
2.2. Protection from Ischemia Ex Vivo
2.3. Graft Function Recovery
2.4. Chronic Outcome
2.5. PEG 20 kDa Reduced Chronic Tubular Atrophy and Interstitial Fibrosis
2.6. PEG 20 kDa Grafts Show Decreased Activation of Lesional Pathways
3. Discussion
4. Materials and Methods
4.1. In Vitro Experiments
4.2. In Vivo Surgical Procedures and Experimental Groups
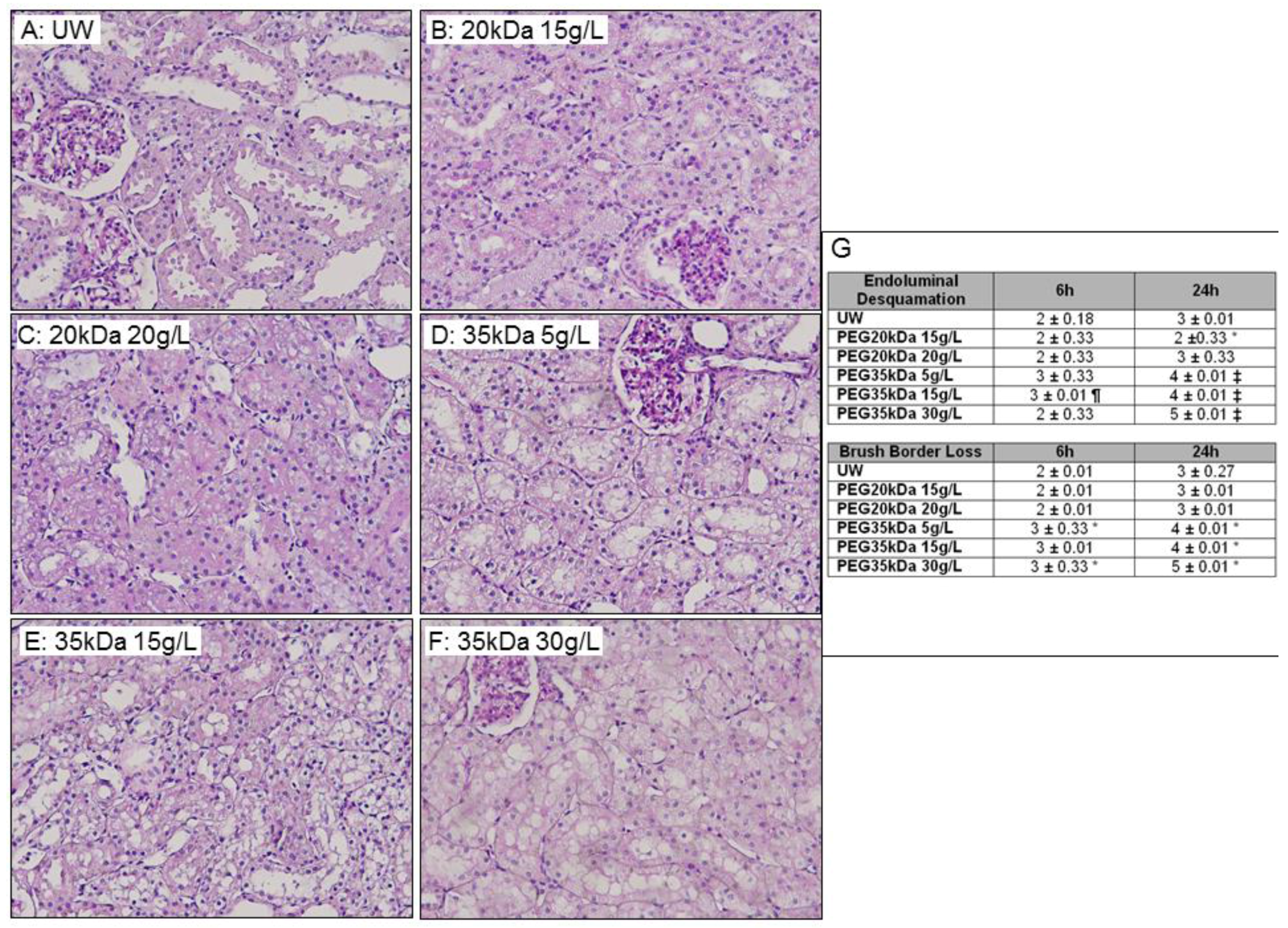
4.3. Function and Histopathology
4.4. Real Time PCR
4.5. Statistical Methods
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| EGR1 | Early growth response factor 1 |
| Flk | VEGF receptor |
| HES | Hydroxyethyl starch |
| HIF1α | Hypoxia inducible factor 1 alpha |
| IGL1 | Institut George Lopez |
| LDH | Lactate DesHydrogenase |
| MHC | major histocompatibility complex |
| p47 | NADPH oxidase subunit Phoxp47 |
| PEG | Polyethylene glycol |
| SCOT | Solution de Conservation des Organes et des Tissus |
| TGFβ | Transforming growth factor β 1 |
| UW | University of Wisconsin |
| VEGF | Vascular endothelium growth factor |
| vWF | Von Willebrand factor |
| XTT | 2,3-Bis-(2-Methoxy-4-Nitro-5-Sulfophenyl)-2H-Tetrazolium-5-Carboxanilide |
References
- Salahudeen, A.K. Cold ischemic injury of transplanted organs: Some new strategies against an old problem. Am. J. Transplant. 2004, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Faure, J.P.; Baumert, H.; Han, Z.; Goujon, J.M.; Favreau, F.; Dutheil, D.; Petit, I.; Barriere, M.; Tallineau, C.; Tillement, J.P.; et al. Evidence for a protective role of trimetazidine during cold ischemia: Targeting inflammation and nephron mass. Biochem. Pharmacol. 2003, 66, 2241–2250. [Google Scholar] [CrossRef] [PubMed]
- Jayle, C.; Favreau, F.; Zhang, K.; Doucet, C.; Goujon, J.M.; Hebrard, W.; Carretier, M.; Eugene, M.; Mauco, G.; Tillement, J.P.; et al. Comparison of protective effects of trimetazidine against experimental warm ischemia of different durations: Early and long-term effects in a pig kidney model. Am. J. Physiol. 2007, 292, F1082–F1093. [Google Scholar] [CrossRef] [PubMed]
- Belzer, F.O.; Southard, J.H. Principles of solid-organ preservation by cold storage. Transplantation 1988, 45, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Rauen, U.; de Groot, H. New insights into the cellular and molecular mechanisms of cold storage injury. J. Investig. Med. 2004, 52, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Salahudeen, A.K. Cold ischemic injury of transplanted kidneys: New insights from experimental studies. Am. J. Physiol. 2004, 287, F181–F187. [Google Scholar] [CrossRef] [PubMed]
- Huter, L.; Simon, T.P.; Weinmann, L.; Schuerholz, T.; Reinhart, K.; Wolf, G.; Amann, K.U.; Marx, G. Hydroxyethylstarch impairs renal function and induces interstitial proliferation, macrophage infiltration and tubular damage in an isolated renal perfusion model. Crit. Care 2009, 13, R23. [Google Scholar] [CrossRef] [PubMed]
- Codas, R.; Petruzzo, P.; Morelon, E.; Lefrancois, N.; Danjou, F.; Berthillot, C.; Contu, P.; Espa, M.; Martin, X.; Badet, L. IGL-1 solution in kidney transplantation: First multi-center study. Clin. Transplant. 2009, 23, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Stewart, Z.A.; Lonze, B.E.; Warren, D.S.; Dagher, N.N.; Singer, A.L.; Montgomery, R.A.; Segev, D.L. Histidine-tryptophan-ketoglutarate (HTK) is associated with reduced graft survival of deceased donor kidney transplants. Am. J. Transplant. 2009, 9, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Faure, J.P.; Hauet, T.; Han, Z.; Goujon, J.M.; Petit, I.; Mauco, G.; Eugene, M.; Carretier, M.; Papadopoulos, V. Polyethylene glycol reduces early and long-term cold ischemia-reperfusion and renal medulla injury. J. Pharmacol. Exp. Ther. 2002, 302, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Badet, L.; Ben Abdennebi, H.; Petruzzo, P.; McGregor, B.; Espa, M.; Hadj-Aissa, A.; Ramella-Virieux, S.; Steghens, J.P.; Portoghese, F.; Martin, X. Effect of IGL-1, a new preservation solution, on kidney grafts (a pre-clinical study). Transpl. Int. 2005, 17, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Schreinemachers, M.C.; Doorschodt, B.M.; Florquin, S.; van den Bergh Weerman, M.A.; Reitsma, J.B.; Lai, W.; Sitzia, M.; Minor, T.M.; Tolba, R.H.; van Gulik, T.M. Improved preservation and microcirculation with POLYSOL after transplantation in a porcine kidney autotransplantation model. Nephrol. Dial. Transplant. 2009, 24, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Bradley, A.J.; Scott, M.D. Immune complex binding by immunocamouflaged [poly(ethylene glycol)-grafted] erythrocytes. Am. J. Hematol. 2007, 82, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Murad, K.L.; Gosselin, E.J.; Eaton, J.W.; Scott, M.D. Stealth cells: Prevention of major histocompatibility complex class II-mediated T-cell activation by cell surface modification. Blood 1999, 94, 2135–2141. [Google Scholar] [PubMed]
- Le, Y.; Scott, M.D. Immunocamouflage: The biophysical basis of immunoprotection by grafted methoxypoly(ethylene glycol) (mPEG). Acta Biomater. 2010, 6, 2631–2641. [Google Scholar] [CrossRef] [PubMed]
- Maathuis, M.H.; Leuvenink, H.G.; Ploeg, R.J. Perspectives in organ preservation. Transplantation 2007, 83, 1289–1298. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Theruvath, A.J.; Ge, X.; Floerchinger, B.; Jurisch, A.; Garcia-Cardena, G.; Tullius, S.G. Machine perfusion or cold storage in organ transplantation: Indication, mechanisms, and future perspectives. Transpl. Int. 2010, 23, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Ben Abdennebi, H.; Elrassi, Z.; Scoazec, J.Y.; Steghens, J.P.; Ramella-Virieux, S.; Boillot, O. Evaluation of IGL-1 preservation solution using an orthotopic liver transplantation model. World J. Gastroenterol. 2006, 12, 5326–5330. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.A. Effect of polyethylene glycol-based preservation solutions on graft injury in experimental kidney transplantation (Br. J. Surg. 2010; 98: 368–378). Br. J. Surg. 2010, 98, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, R.; Giraud, S.; Favreau, F.; Goujon, J.M.; Desurmont, T.; Eugene, M.; Barrou, B.; Hauet, T. Improving Long-Term Outcome in Allograft Transplantation: Role of Ionic Composition and Polyethylene Glycol. Transplantation 2011, 91, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, R.; Renard, C.; Rogel-Gaillard, C.; Demars, J.; Milan, D.; Forestier, L.; Ouldmoulene, A.; Goujon, J.M.; Badet, L.; Hauet, T. Effect of polyethylene glycol-based preservation solutions on graft injury in experimental kidney transplantation. Br. J. Surg. 2010, 98, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Giraud, S.; Claire, B.; Eugene, M.; Debre, P.; Richard, F.; Barrou, B. A new preservation solution increases islet yield and reduces graft immunogenicity in pancreatic islet transplantation. Transplantation 2007, 83, 1397–1400. [Google Scholar] [PubMed]
- Simmons, M.N.; Schreiber, M.J.; Gill, I.S. Surgical renal ischemia: A contemporary overview. J. Urol. 2008, 180, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Giraud, S.; Favreau, F.; Chatauret, N.; Thuillier, R.; Maiga, S.; Hauet, T. Contribution of Large Pig for Renal Ischemia-Reperfusion and Transplantation Studies: The Preclinical Model. J. Biomed. Biotechnol. 2011, in press. [Google Scholar] [CrossRef] [PubMed]
- Copeland, J.W.; Beaumont, B.W.; Merrilees, M.J.; Pilmore, H.L. Epithelial-to-mesenchymal transition of human proximal tubular epithelial cells: Effects of rapamycin, mycophenolate, cyclosporin, azathioprine, and methylprednisolone. Transplantation 2007, 83, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Favreau, F.; Thuillier, R.; Cau, J.; Milin, S.; Manguy, E.; Mauco, G.; Zhu, X.; Lerman, L.O.; Hauet, T. Anti-thrombin Therapy During Warm Ischemia and Cold Preservation Prevents Chronic Kidney Graft Fibrosis in a DCD Model. Am. J. Transplant. 2009, 10, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, R.; Favreau, F.; Celhay, O.; Macchi, L.; Milin, S.; Hauet, T. Thrombin inhibition during kidney ischemia-reperfusion reduces chronic graft inflammation and tubular atrophy. Transplantation 2010, 90, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Khachigian, L.M. Early growth response-1 in cardiovascular pathobiology. Circ. Res. 2006, 98, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Bonventre, J.V.; Sukhatme, V.P.; Bamberger, M.; Ouellette, A.J.; Brown, D. Localization of the protein product of the immediate early growth response gene, Egr-1, in the kidney after ischemia and reperfusion. Cell Regul. 1991, 2, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Autieri, M.V.; Kelemen, S.E.; Gaughan, J.P.; Eisen, H.J. Early growth responsive gene (Egr)-1 expression correlates with cardiac allograft rejection. Transplantation 2004, 78, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Eddy, A.A. Molecular basis of renal fibrosis. Pediatr. Nephrol. 2000, 15, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Haase, V.H. Oxygen regulates epithelial-to-mesenchymal transition: Insights into molecular mechanisms and relevance to disease. Kidney Int. 2009, 76, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Giraud, S.; Thuillier, R.; Belliard, A.; Hebrard, W.; Nadeau, C.; Milin, S.; Goujon, J.M.; Manguy, E.; Mauco, G.; Hauet, T.; et al. Direct thrombin inhibitor prevents delayed graft function in a porcine model of renal transplantation. Transplantation 2009, 87, 1636–1644. [Google Scholar] [CrossRef] [PubMed]
- Djamali, A. Oxidative stress as a common pathway to chronic tubulointerstitial injury in kidney allografts. Am. J. Physiol. 2007, 293, F445–F455. [Google Scholar] [CrossRef] [PubMed]
- Lanneau, D.; Brunet, M.; Frisan, E.; Solary, E.; Fontenay, M.; Garrido, C. Heat shock proteins: Essential proteins for apoptosis regulation. J. Cell. Mol. Med. 2008, 12, 743–761. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Sharpe, E.; Bellamy, C.O.; McNally, S.J.; Devey, L.; Garden, O.J.; Ross, J.A.; Wigmore, S.J. Heat shock protein 90-binding agents protect renal cells from oxidative stress and reduce kidney ischemia-reperfusion injury. Am. J. Physiol. 2008, 295, F397–F405. [Google Scholar] [CrossRef] [PubMed]
- Yamano, T.; Murata, S.; Shimbara, N.; Tanaka, N.; Chiba, T.; Tanaka, K.; Yui, K.; Udono, H. Two distinct pathways mediated by PA28 and hsp90 in major histocompatibility complex class I antigen processing. J. Exp. Med. 2002, 196, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Guo, J.; Han, C.; Yang, M.; Cao, X. Heat shock protein 70, released from heat-stressed tumor cells, initiates antitumor immunity by inducing tumor cell chemokine production and activating dendritic cells via TLR4 pathway. J. Immunol. 2009, 182, 1449–1459. [Google Scholar] [CrossRef] [PubMed]
- Eugene, M. Polyethyleneglycols and immunocamouflage of the cells tissues and organs for transplantation. Cell. Mol. Biol. 2004, 50, 209–215. [Google Scholar] [PubMed]
- Hansen, P.L.; Cohen, J.A.; Podgornik, R.; Parsegian, V.A. Osmotic properties of poly(ethylene glycols): Quantitative features of brush and bulk scaling laws. Biophys. J. 2003, 84, 350–355. [Google Scholar] [CrossRef]
- Dutheil, D.; Rioja-Pastor, I.; Tallineau, C.; Goujon, J.M.; Hauet, T.; Mauco, G.; Petit-Paris, I. Protective effect of PEG 35,000 Da on renal cells: Paradoxical activation of JNK signaling pathway during cold storage. Am. J. Transplant. 2006, 6, 1529–1540. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, R.M.R. The immunology of chronic allograft injury. In Chronic Allograft Failure: Natural History, Pathogenesis, Diagnosis and Management; Ahsan, N., Ed.; Landes Bioscience: Austin, TX, USA, 2007. [Google Scholar]
- Scott, M.D.; Murad, K.L. Cellular camouflage: Fooling the immune system with polymers. Curr. Pharm. Des. 1998, 4, 423–438. [Google Scholar] [PubMed]
- Perrin, H.; Thaunat, O.; Malcus, C.; Badet, L.; Hennino, A.; Codas, R.; Touraine-Moulin, F.; Nicolas, J.F.; Morelon, E. Immunoprotection by polyethylene glycol in organ preservation solutions is not due to an immunomasking effect. Nephrol. Dial. Transplant. 2009, 24, 1682–1685. [Google Scholar] [CrossRef] [PubMed]
- Mannon, R.B.; Fairchild, R. Allograft fibrosis—Unmasking the players at the dance. Am. J. Transplant. 2010, 10, 201–202. [Google Scholar] [CrossRef] [PubMed]
- Nakorchevsky, A.; Hewel, J.A.; Kurian, S.M.; Mondala, T.S.; Campbell, D.; Head, S.R.; Marsh, C.L.; Yates, J.R., 3rd; Salomon, D.R. Molecular Mechanisms of Chronic Kidney Transplant Rejection via Large-Scale Proteogenomic Analysis of Tissue Biopsies. J. Am. Soc. Nephrol. 2010, 21, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Seron, D.; Moreso, F. Protocol biopsies in renal transplantation: Prognostic value of structural monitoring. Kidney Int. 2007, 72, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Chok, M.K.; Ferlicot, S.; Conti, M.; Almolki, A.; Durrbach, A.; Loric, S.; Benoit, G.; Droupy, S.; Eschwege, P. Renoprotective potency of heme oxygenase-1 induction in rat renal ischemia-reperfusion. Inflamm. Allergy Drug Targets 2009, 8, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yang, C.; He, X. Expression of HO-1 in chronic renal insufficiency. Rat kidney and implication. J. Huazhong Univ. Sci. Technol. Med. Sci. 2003, 23, 271–274. [Google Scholar] [PubMed]
- Giraud, S.; Bon, D.; Neuzillet, Y.; Thuillier, R.; Eugene, M.; Hauet, T.; Barrou, B. Concentration and chain length of polyethylene glycol in islet isolation solution: Evaluation in a pancreatic islet transplantation model. Cell Transplant. 2012, 21, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Hauet, T.; Eugene, M. A new approach in organ preservation: Potential role of new polymers. Kidney Int. 2008, 74, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Hauet, T.; Mothes, D.; Goujon, J.M.; Carretier, M.; Eugene, M. Protective effect of polyethylene glycol against prolonged cold ischemia and reperfusion injury: Study in the isolated perfused rat kidney. J. Pharmacol. Exp. Ther. 2001, 297, 946–952. [Google Scholar] [PubMed]
- Hauet, T.; Goujon, J.M.; Vandewalle, A.; Baumert, H.; Lacoste, L.; Tillement, J.P.; Eugene, M.; Carretier, M. Trimetazidine reduces renal dysfunction by limiting the cold ischemia/reperfusion injury in autotransplanted pig kidneys. J. Am. Soc. Nephrol. 2000, 11, 138–148. [Google Scholar] [PubMed]
- Hauet, T.; Goujon, J.M.; Baumert, H.; Petit, I.; Carretier, M.; Eugene, M.; Vandewalle, A. Polyethylene glycol reduces the inflammatory injury due to cold ischemia/reperfusion in autotransplanted pig kidneys. Kidney Int. 2002, 62, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Grimm, P.C.; Nickerson, P.; Gough, J.; McKenna, R.; Stern, E.; Jeffery, J.; Rush, D.N. Computerized image analysis of Sirius Red-stained renal allograft biopsies as a surrogate marker to predict long-term allograft function. J. Am. Soc. Nephrol. 2003, 14, 1662–1668. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Solution | PEG Concentration (mM) | Density (g/cm3) | Viscosity (Cst) |
|---|---|---|---|
| UW | 0 | 1.047 | 3.22 |
| PEG 20kDa/15 g | 0.75 | 1.010 | 1.41 |
| PEG 20 kDa/20 g | 1 | 1.011 | 1.55 |
| PEG 35kDa/5 g | 0.14 | 1.008 | 1.23 |
| PEG 35 kDa/15 g | 0.43 | 1.010 | 1.90 |
| PEG 35 kDa/30 g | 0.85 | 1.032 | 4.56 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraud, S.; Thuillier, R.; Codas, R.; Manguy, E.; Barrou, B.; Valagier, A.; Puichaud, A.; Badet, L.; Nicolas, E.; Eugene, M.; et al. The Optimal PEG for Kidney Preservation: A Preclinical Porcine Study. Int. J. Mol. Sci. 2018, 19, 454. https://doi.org/10.3390/ijms19020454
Giraud S, Thuillier R, Codas R, Manguy E, Barrou B, Valagier A, Puichaud A, Badet L, Nicolas E, Eugene M, et al. The Optimal PEG for Kidney Preservation: A Preclinical Porcine Study. International Journal of Molecular Sciences. 2018; 19(2):454. https://doi.org/10.3390/ijms19020454
Chicago/Turabian StyleGiraud, Sebastien, Raphael Thuillier, Ricardo Codas, Emily Manguy, Benoit Barrou, Alexandre Valagier, Alexis Puichaud, Lionel Badet, Emmanuelle Nicolas, Michel Eugene, and et al. 2018. "The Optimal PEG for Kidney Preservation: A Preclinical Porcine Study" International Journal of Molecular Sciences 19, no. 2: 454. https://doi.org/10.3390/ijms19020454
APA StyleGiraud, S., Thuillier, R., Codas, R., Manguy, E., Barrou, B., Valagier, A., Puichaud, A., Badet, L., Nicolas, E., Eugene, M., & Hauet, T. (2018). The Optimal PEG for Kidney Preservation: A Preclinical Porcine Study. International Journal of Molecular Sciences, 19(2), 454. https://doi.org/10.3390/ijms19020454