Molecular Epidemiology of Helicobacter pylori Infection in a Minor Ethnic Group of Vietnam: A Multiethnic, Population-Based Study

 ,
, 
Abstract
:1. Introduction
2. Results
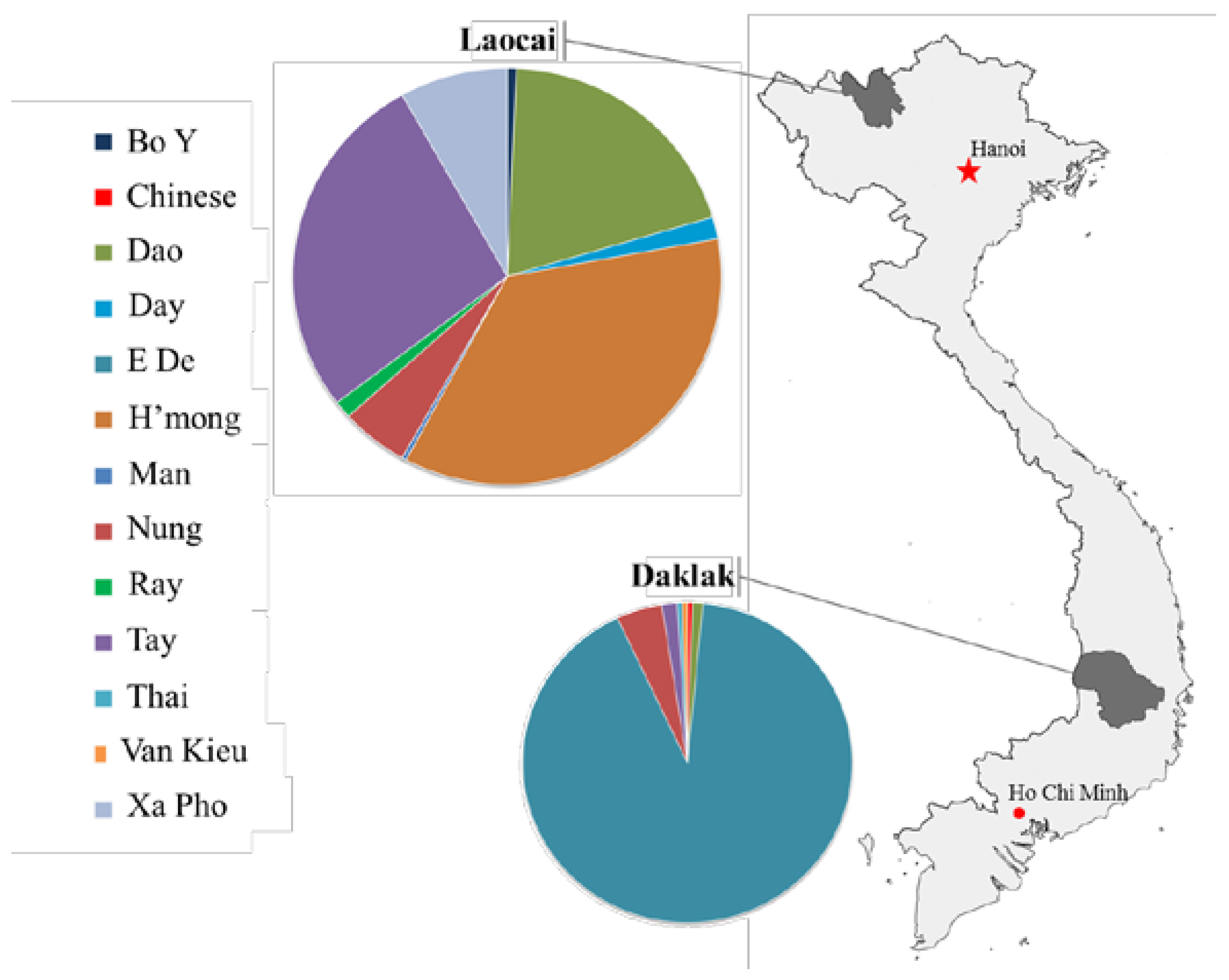
2.1. Characteristics of the Study Population
2.2. The Prevalence of H. pylori Infection in General as Well as Its Differences between Geographical Regions and Ethnicities
2.3. Risk of H. pylori Infection
2.4. H. pylori and the Gastroduodenal Diseases
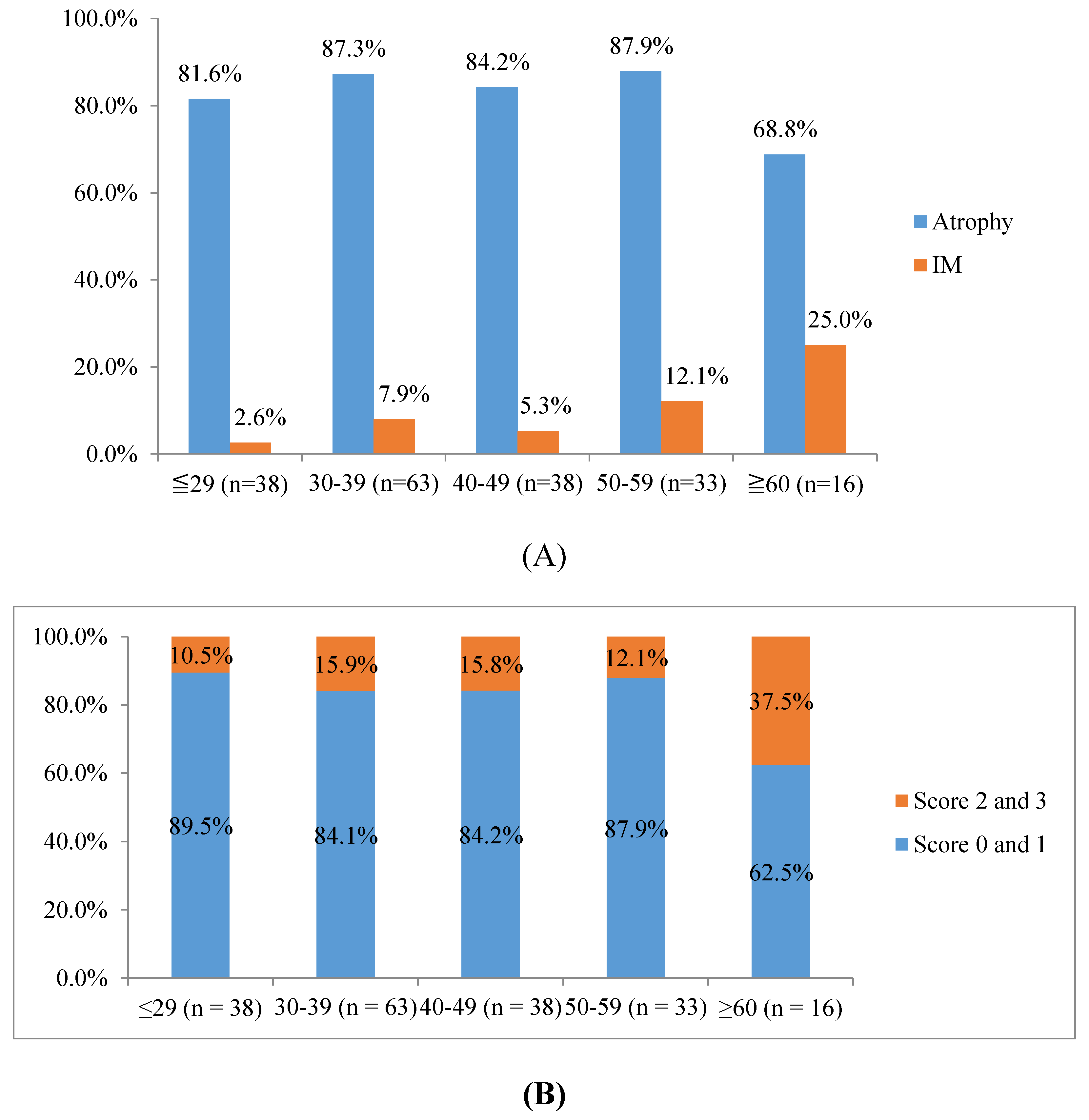
2.5. H. pylori and Histological Evaluation
2.6. The Distribution of cagA and vacA Genotypes
3. Discussion
4. Material and Methods
4.1. Study Design and Study Population
4.2. Sampling
4.3. The Determination of H. pylori Status
4.4. Histological Status of Chronic Gastritis
4.5. Cytotoxin Associated Gene A (cagA) and Vacuolating Cytoxotin (vacA) Genotype Analysis
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| GC | Gastric cancer |
| Helicobacter pylori | H. Pylori |
| PU | Peptic ulcer |
| ASR | Age-standardized incidence rate |
| DU | Duodenal ulcer |
| GU | Gastric ulcer |
| RUT | Rapid urease test |
| IHC | Immunohistochemistry |
| OLGA | Operative link for gastritis assessment |
| OLGIM | Operative link on gastric intestinal metaplasia |
| cagA | Cytotoxin-associated gene A |
| vacA | Vacuolating cytotoxin |
| OR | Odds ratio |
| CI | Confidence interval |
| IM | Intestinal metaplasia |
References
- Malaty, H.M. Epidemiology of Helicobacter pylori infection. Best Pract. Res. Clin. Gastroenterol. 2007, 21, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, Y. Mechanisms of disease: Helicobacter pylori virulence factors. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Marshall, B.; Warren, J.R. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. The Lancet 1984, 323, 1311–1315. [Google Scholar] [CrossRef]
- Peek, R.M., Jr.; Blaser, M.J. Helicobacter pylori and gastrointestinal tract adenocarcinomas. Nat. Rev. Cancer 2002, 2, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Suerbaum, S.; Michetti, P. Helicobacter pylori infection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Lu, H.; Yamaoka, Y. African, Asian or Indian enigma, the East Asian Helicobacter pylori: Facts or medical myths. J. Dig. Dis. 2009, 10, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the development of gastric cancer. N. Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.L.; Uchida, T.; Tsukamoto, Y.; Trinh, D.T.; Ta, L.; Mai, B.H.; Le, S.H.; Thai, K.D.; Ho, D.D.; Hoang, H.H.; et al. Helicobacter pylori infection and gastroduodenal diseases in Vietnam: A cross-sectional, hospital-based study. BMC Gastroenterol. 2010, 10, 114. [Google Scholar] [CrossRef] [PubMed]
- Binh, T.T.; Tuan, V.P.; Dung, H.D.Q.; Tung, P.H.; Tri, T.D.; Thuan, N.P.M.; Khien, V.V.; Hoan, P.Q.; Suzuki, R.; Uchida, T.; et al. Advanced non-cardia gastric cancer and Helicobacter pylori infection in Vietnam. Gut. Pathogens 2017, 9, 46. [Google Scholar] [CrossRef] [PubMed]
- Vietnam Image of The Community of 54 Ethnic Groups. Available online: http://cema.gov.vn (accessed on 1 March 2018).
- Hoang, T.T.; Bengtsson, C.; Phung, D.C.; Sorberg, M.; Granstrom, M. Seroprevalence of Helicobacter pylori infection in urban and rural Vietnam. Clin. Diagn. Lab. Immunol. 2005, 12, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.T.; Uchida, T.; Tsukamoto, Y.; Trinh, T.D.; Ta, L.; Ho, D.Q.; Matsuhisa, T.; Uchida, M.; Takayama, A.; Hijiya, N.; et al. Evaluation of rapid urine test for the detection of Helicobacter pylori infection in the Vietnamese population. Dig. Dis. Sci. 2010, 55, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Piriyapong, K.; Tangaroonsanti, A.; Mahachai, V.; Vilaichone, R.K. Helicobacter pylori infection impacts on functional dyspepsia in Thailand. Asian Pac. J. Cancer Prev. 2014, 15, 10887–10891. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Miftahussurur, M.; Pittayanon, R.; Vilaichone, R.K.; Wisedopas, N.; Ratanachu-Ek, T.; Kishida, T.; Moriyama, M.; Yamaoka, Y.; Mahachai, V. Helicobacter pylori Infection in Thailand: A Nationwide Study of the CagA Phenotype. PLoS ONE 2015, 10, e0136775. [Google Scholar] [CrossRef] [PubMed]
- Vannarath, S.; Vilaichone, R.K.; Rasachak, B.; Mairiang, P.; Yamaoka, Y.; Shiota, S.; Binh, T.T.; Mahachai, V. Virulence genes of Helicobacter pylori in gastritis, peptic ulcer and gastric cancer in Laos. Asian Pac. J. Cancer Prev. 2014, 15, 9027–9031. [Google Scholar] [CrossRef] [PubMed]
- Myint, T.; Shiota, S.; Vilaichone, R.K.; Ni, N.; Aye, T.T.; Matsuda, M.; Tran, T.T.; Uchida, T.; Mahachai, V.; Yamaoka, Y. Prevalence of Helicobacter pylori infection and atrophic gastritis in patients with dyspeptic symptoms in Myanmar. World J. Gastroenterol. 2015, 21, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Correa, P.; Haenszel, W.; Cuello, C.; Tannenbaum, S.; Archer, M. A model for gastric cancer epidemiology. Lancet 1975, 2, 58–60. [Google Scholar] [CrossRef]
- Vilaichone, R.K.; Mahachai, V.; Tumwasorn, S.; Wu, J.Y.; Graham, D.Y.; Yamaoka, Y. Molecular epidemiology and outcome of Helicobacter pylori infection in Thailand: a cultural cross roads. Helicobacter 2004, 9, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.R.; Joo, Y.M.; Jang, S.; Yoo, Y.J.; Lee, H.S.; Chung, I.S.; Olsen, C.H.; Whitmire, J.M.; Merrell, D.S.; Cha, J.H. Polymorphism in the CagA EPIYA motif impacts development of gastric cancer. J. Clin. Microbiol. 2009, 47, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Azuma, T.; Yamakawa, A.; Yamazaki, S.; Ohtani, M.; Ito, Y.; Muramatsu, A.; Suto, H.; Yamazaki, Y.; Keida, Y.; Higashi, H.; et al. Distinct diversity of the cag pathogenicity island among Helicobacter pylori strains in Japan. J. Clin. Microbiol. 2004, 42, 2508–2517. [Google Scholar] [CrossRef] [PubMed]
- Hatakeyama, M. Oncogenic mechanisms of the Helicobacter pylori CagA protein. Nat. Rev. Cancer 2004, 4, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Matsunari, O.; Shiota, S.; Suzuki, R.; Watada, M.; Kinjo, N.; Murakami, K.; Fujioka, T.; Kinjo, F.; Yamaoka, Y. Association between Helicobacter pylori virulence factors and gastroduodenal diseases in Okinawa, Japan. J. Clin. Microbiol. 2012, 50, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Atherton, J.C.; Cao, P.; Peek, R.M.; Tummuru, M.K.; Blaser, M.J.; Cover, T.L. Mosaicism in vacuolating cytotoxin alleles of Helicobacter pylori. Association of specific vacA types with cytotoxin production and peptic ulceration. J. Biol. Chem. 1995, 270, 17771–17777. [Google Scholar] [CrossRef] [PubMed]
- Subsomwong, P.; Miftahussurur, M.; Uchida, T.; Vilaichone, R.K.; Ratanachu-Ek, T.; Mahachai, V.; Yamaoka, Y. Prevalence, risk factors, and virulence genes of Helicobacter pylori among dyspeptic patients in two different gastric cancer risk regions of Thailand. PLoS ONE 2017, 12, e0187113. [Google Scholar] [CrossRef] [PubMed]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Correa, P.; Di Mario, F.; El-Omar, E.; Fiocca, R.; Geboes, K.; Genta, R.M.; Graham, D.Y.; Hattori, T.; Malfertheiner, P.; et al. OLGA staging for gastritis: a tutorial. Dig. Liver Dis. 2008, 40, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Capelle, L.G.; de Vries, A.C.; Haringsma, J.; Ter Borg, F.; de Vries, R.A.; Bruno, M.J.; van Dekken, H.; Meijer, J.; van Grieken, N.C.; Kuipers, E.J. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest. Endosc. 2010, 71, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, Y.; Kodama, T.; Kita, M.; Imanishi, J.; Kashima, K.; Graham, D.Y. Relationship of vacA genotypes of Helicobacter pylori to cagA status, cytotoxin production, and clinical outcome. Helicobacter 1998, 3, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, Y.; El–Zimaity, H.M.T.; Gutierrez, O.; Figura, N.; Kim, J.K.; Kodama, T.; Kashima, K.; Graham, D.Y. Relationship between the cagA 3′ repeat region of Helicobacter pylori, gastric histology, and susceptibility to low pH. Gastroenterology 1999, 117, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Stecher, G.; Peterson, D.; Filipski, A.; Kumar, S. MEGA6: Molecular Evolutionary Genetics Analysis version 6.0. Mol. Biol. Evol. 2013, 30, 2725–2729. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Ethnic | H. pylori Infection | Total | |
|---|---|---|---|
| No. of participant (%) | 188 (38.1%) | 494 | |
| Daklak province | |||
| E De | 94 (51.4%) | 183 | |
| Nung | 6 (66.7%) | 9 | |
| Tay | 0 (0%) | 3 | |
| Dao | 0 (0%) | 2 | |
| Van Kieu | 1 (100%) | 1 | |
| Thai | 1 (100%) | 1 | |
| Chinese | 0 (0%) | 1 | |
| Lao Cai province | |||
| H′mong | 40 (38.1%) a | 105 | |
| Nung | 2 (13.3%) a,b | 15 | |
| Tay | 15 (18.8%) a,b | 80 | |
| Dao | 12 (20.7%) a,b | 58 | |
| Xa Pho | 13 (54.2%) | 24 | |
| Day | 1 (20%) | 5 | |
| Ray | 2 (50%) | 4 | |
| Bo Y | 0 (0%) | 2 | |
| Man | 1 (100%) | 1 |
| Risk Factor | H. pylori Positive/Total Number (%) | Crude OR | 95% CI | p-Value |
|---|---|---|---|---|
| Age group | ||||
| ≤ 29 | 38/118 (32.2%) | 0.72 | 0.45–1.13 | 0.16 |
| 30–39 | 63/156 (40.4%) | 1.15 | 0.77–1.73 | 0.49 |
| 40–49 | 38/107 (35.5%) | 0.87 | 0.54–1.39 | 0.58 |
| 50–59 | 33/67 (49.3%) | 1.70 | 0.98–2.95 | 0.06 |
| ≥ 60 | 16/46 (34.8%) | 0.86 | 0.42–1.68 | 0.75 |
| Gender | ||||
| Male | 90/210 (42.9%) | 1.42 | 0.98–2.05 | 0.06 |
| Female | 98/284 (34.5%) | 1.00 | ||
| Geographical location | ||||
| Daklak | 102/200 (51.0%) | 2.52 | 1.73–3.65 | <0.001 |
| Lao Cai | 86/294 (29.3%) | 1.00 | ||
| Ethnicities | ||||
| E De | 94/183 (51.4%) | 2.44 | 1.64–3.62 | <0.001 |
| H′mong | 40/105 (38.1%) | 1.00 | 0.62–1.59 | 1.00 |
| Nung | 8/24 (33.3%) | 0.81 | 0.29–2.04 | 0.67 |
| Tay | 15/83 (18.1%) | 0.30 | 0.16–0.56 | <0.001 |
| Dao | 12/60 (20%) | 0.37 | 0.17–0.73 | 0.002 |
| Xa Pho | 13/24 (54.2%) | 1.99 | 0.87–4.54 | 0.13 |
| Other* | 6/15 (40%) | 0.64 | 0.24–1.68 | 0.5 |
| Marital status | ||||
| Single | 1/3 (33.3%) | 1.00 | ||
| Married | 187/491 (38.1%) | 1.23 | 0.06–73.0 | 1.00 |
| Smoking | ||||
| Yes | 28/81 (34.6%) | 0.84 | 0.49–1.41 | 0.53 |
| No | 160/413 (38.7%) | 1.00 | ||
| Drinking | ||||
| Yes | 55/121 (45.5%) | 1.50 | 0.97–2.32 | 0.07 |
| No | 133/373 (35.7%) | 1.00 |
| E De (n = 90) | Nung (n = 6) | H’mong (n = 39) | Tay (n = 12) | Dao (n = 9) | Xa Pho (n = 11) | Kinh (n = 103) a | ||
|---|---|---|---|---|---|---|---|---|
| Antrum | ||||||||
| Neutrophil | 1.2 (1) | 2.0 (2) b | 1.7 (2) c | 1.7 (2) d | 1.7 (2) e | 2.0 (2) f | 1.2 (1) | |
| Monocyte | 1.6 (2) | 2.3 (2.5) b | 2.1 (2) c | 2.2 (2) d | 2.0 (2) | 2.2 (2) f | 1.7 (2) | |
| Atrophy | 0.9 (1) | 1.5 (1) | 1.0 (1) | 1.2 (1) | 0.9 (1) | 1.0 (1) | 0.9 (1) | |
| IM | 0.02 (0) | 0.0 (0) | 0.2 (0) c | 0.2 (0) d | 0.0 (0) | 0.4 (0) f | 0.1 (0) | |
| Corpus | ||||||||
| Neutrophil | 0.8 (1) | 0.8 (1) | 1.0 (1) c | 0.9 (1) | 1.1 (1) | 0.9 (1) | 1.0 (1) g | |
| Monocyte | 0.6 (1) | 0.5 (0.5) | 1.2 (1) c | 1.1 (1) d | 1.2 (1) e | 0.6 (1) | 1.5 (1) g | |
| Atrophy | 0.02 (0) | 0.0 (0) | 0.2 (0) c | 0.2 (0) d | 0.2 (0) e | 0.0 (0) | 0.6 (1) g | |
| IM | 0.01 (0) | 0.0 (0) | 0.0 (0) | 0.0 (0) | 0.0 (0) | 0.0 (0) | 0.1 (0) g | |
| OLGA | 0.9 (1) | 1.5 (1) | 1.1 (1) | 1.2 (1) | 0.9 (1) | 1.0 (1) | 1.0 (1) | |
| OLGIM | 0.03 (0) | 0.0 (0) | 0.2 (0) c | 0.2 (0) d | 0.0 (0) | 0.4 (0) f | 0.2 (0) g | |
| H. pylori Culture Positive Cases | cagA Positive | CagA Type | vacA s and m | ||
|---|---|---|---|---|---|
| Western | East Asian | s1m1 | s1m2 | ||
| Daklak (n = 96) | 95 (99%) | 73 (76.8%) | 22 (23.2%) | 78 (81.3%) | 18 (18.8%) |
| E De | 89 (98.9%) | 73 (82%) | 16 (18%) | 74 (82.2%) | 16 (17.8%) |
| Nunga | 4 (100%) | 0 (0%) | 4 (100%) | 2 (50%) | 2 (50%) |
| Van Kieu | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) |
| Thai | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) |
| Lao Cai (n = 75) | 75 (100%) | 0 (0%) | 75 (100%) | 34 (45.3%) | 39 (52%) |
| H’mong | 39 (100%) | 0 (0%) | 39 (100%) | 17 (43.6%) | 20 (51.3%) |
| Nung a | 2 (100%) | 0 (0%) | 2 (100%) | 2 (100%) | 0 (0%) |
| Tay a | 12 (100%) | 0 (0%) | 12 (100%) | 7 (41.7%) | 7 (58.3%) |
| Dao a | 9 (100%) | 0 (0%) | 9 (100%) | 4 (44.4%) | 5 (55.6%) |
| Xa Pho | 11 (100%) | 0 (0%) | 11 (100%) | 4 (36.4%) | 7 (63.6%) |
| Ray | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) |
| Man | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) |
| Total (n = 171) | 170 (99.4%) | 73 (42.9%) | 97 (57.1%) | 112 (65.5%) b | 57 (33.3%) b |
| Cell Infiltration | Western-Type CagA E De (n = 73) | East Asian-Type CagA E De (n = 16) | East Asian-Type CagA Non-E De (n = 81) | East Asian-Type CagA Kinh (n = 103) |
|---|---|---|---|---|
| Histological scoresMean (median) | ||||
| Antrum | ||||
| Neutrophil | 1.2 (1) | 1.2 (1) | 1.7 (2) a | 1.2 (1) |
| Monocyte | 1.5 (2) | 1.7 (2) | 2.1 (2) a | 1.7 (2) |
| Atrophy | 0.9 (1) | 1.1 (1) | 1.1 (1) | 0.9 (1) |
| IM | 0.03 (0) | 0.0 (0) | 0.2 (0) a | 0.1 (0) |
| Corpus | ||||
| Neutrophil | 0.8 (1) | 0.6 (1) | 0.9 (1) | 1.0 (1) |
| Monocyte | 0.6 (1) | 0.5 (1) | 1.0 (1) a | 1.5 (2) a |
| Atrophy | 0.02 (0) | 0.0 (0) | 0.2 (0) a | 0.6 (1) a |
| IM | 0.01 (0) | 0.0 (0) | 0.0 (0) | 0.1 (0) |
| OLGA | 0.9 (1) | 1.1 (1) | 1.1 (1) | 1.0 (1) |
| OLGIM | 0.04 (0) | 0.0 (0) | 0.2 (0) a | 0.2 (0) a |
| No. of Samples | |||||
|---|---|---|---|---|---|
| Type | GU | DU | PU | Gastritis | Total |
| No of culture positive cases | 10 | 6 | 16 | 155 | 171 |
| cagA positive | 10 (100%) | 6 (100%) | 16 (100%) | 154 (99.4%) | 170 (99.4%) |
| Western-type CagA | 4 (40%) | 2 (33.3%) | 6 (37.5%) | 67 (43.2%) | 73 (42.9%) |
| East-Asian-type CagA | 6 (60%) | 4 (66.7%) | 10 (62.5%) | 87 (56.1%) | 97 (57.1%) |
| vacA s1 | 10 (100%) | 6 (100%) | 16 (100%) | 155 (100%) | 171 (100%) |
| vacA m1 | 8 (80%) | 5 (83.3%) | 13 (81.3%) | 99 (63.9%) | 112 (65.5%) |
| vacA m2 | 2 (20%) | 1 (16.7%) | 3 (18.7%) | 54 (34.8%) | 57 (33.3%) |
| vacA m1m2 | 2 (20%) | 0 (0%) | 2 (12.5%) | 2 (1.3%) | 2 (1.2%) |
| vacA s1m1 | 8 (80%) | 5 (83.3%) | 13 (81.3%) | 99 (63.9%) | 112 (65.5%) |
| vacA s1m2 | 2 (20%) | 1 (16.7%) | 0 (0%) | 54 (34.8%) | 57 (33.3%) |
| vacA s1m1m2 | 2 (20%) | 0 (0%) | 0 (0%) | 2 (1.3%) | 2 (1.2%) |
| Western-type CagA/vacA s1m1 | 4 (40%) | 1 (16.7%) | 5 (31.3%) | 58 (37.4%) | 63 (36.8%) |
| Western-type CagA/vacA s1m2 | 0 (0%) | 1 (16.7%) | 1 (6.3%) | 9 (5.8%) | 10 (5.8%) |
| East-Asian-type CagA/vacA s1m1 | 4 (40%) | 4 (66.7%) a | 8 (50%) | 40 (25.8%) a | 48 (28.1%) |
| East-Asian-type CagA/vacA s1m2 | 2 (20%) | 0 (0%) | 0 (0%) | 45 (29%) | 47 (27.5%) |
| East-Asian-type CagA/vacA s1m1m2 | 0 (0%) | 0 (0%) | 0 (0%) | 2 (1.3%) | 2 (1.2%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binh, T.T.; Tuan, V.P.; Dung, H.D.Q.; Tung, P.H.; Tri, T.D.; Thuan, N.P.M.; Tam, L.Q.; Nam, B.C.; Giang, D.A.; Hoan, P.Q.; et al. Molecular Epidemiology of Helicobacter pylori Infection in a Minor Ethnic Group of Vietnam: A Multiethnic, Population-Based Study. Int. J. Mol. Sci. 2018, 19, 708. https://doi.org/10.3390/ijms19030708
Binh TT, Tuan VP, Dung HDQ, Tung PH, Tri TD, Thuan NPM, Tam LQ, Nam BC, Giang DA, Hoan PQ, et al. Molecular Epidemiology of Helicobacter pylori Infection in a Minor Ethnic Group of Vietnam: A Multiethnic, Population-Based Study. International Journal of Molecular Sciences. 2018; 19(3):708. https://doi.org/10.3390/ijms19030708
Chicago/Turabian StyleBinh, Tran Thanh, Vo Phuoc Tuan, Ho Dang Quy Dung, Pham Huu Tung, Tran Dinh Tri, Ngo Phuong Minh Thuan, Le Quang Tam, Bui Chi Nam, Do Anh Giang, Phan Quoc Hoan, and et al. 2018. "Molecular Epidemiology of Helicobacter pylori Infection in a Minor Ethnic Group of Vietnam: A Multiethnic, Population-Based Study" International Journal of Molecular Sciences 19, no. 3: 708. https://doi.org/10.3390/ijms19030708
APA StyleBinh, T. T., Tuan, V. P., Dung, H. D. Q., Tung, P. H., Tri, T. D., Thuan, N. P. M., Tam, L. Q., Nam, B. C., Giang, D. A., Hoan, P. Q., Uchida, T., Trang, T. T. H., Khien, V. V., & Yamaoka, Y. (2018). Molecular Epidemiology of Helicobacter pylori Infection in a Minor Ethnic Group of Vietnam: A Multiethnic, Population-Based Study. International Journal of Molecular Sciences, 19(3), 708. https://doi.org/10.3390/ijms19030708