Comparative Analysis of Bone Structural Parameters Reveals Subchondral Cortical Plate Resorption and Increased Trabecular Bone Remodeling in Human Facet Joint Osteoarthritis


Abstract
:
1. Introduction
2. Results
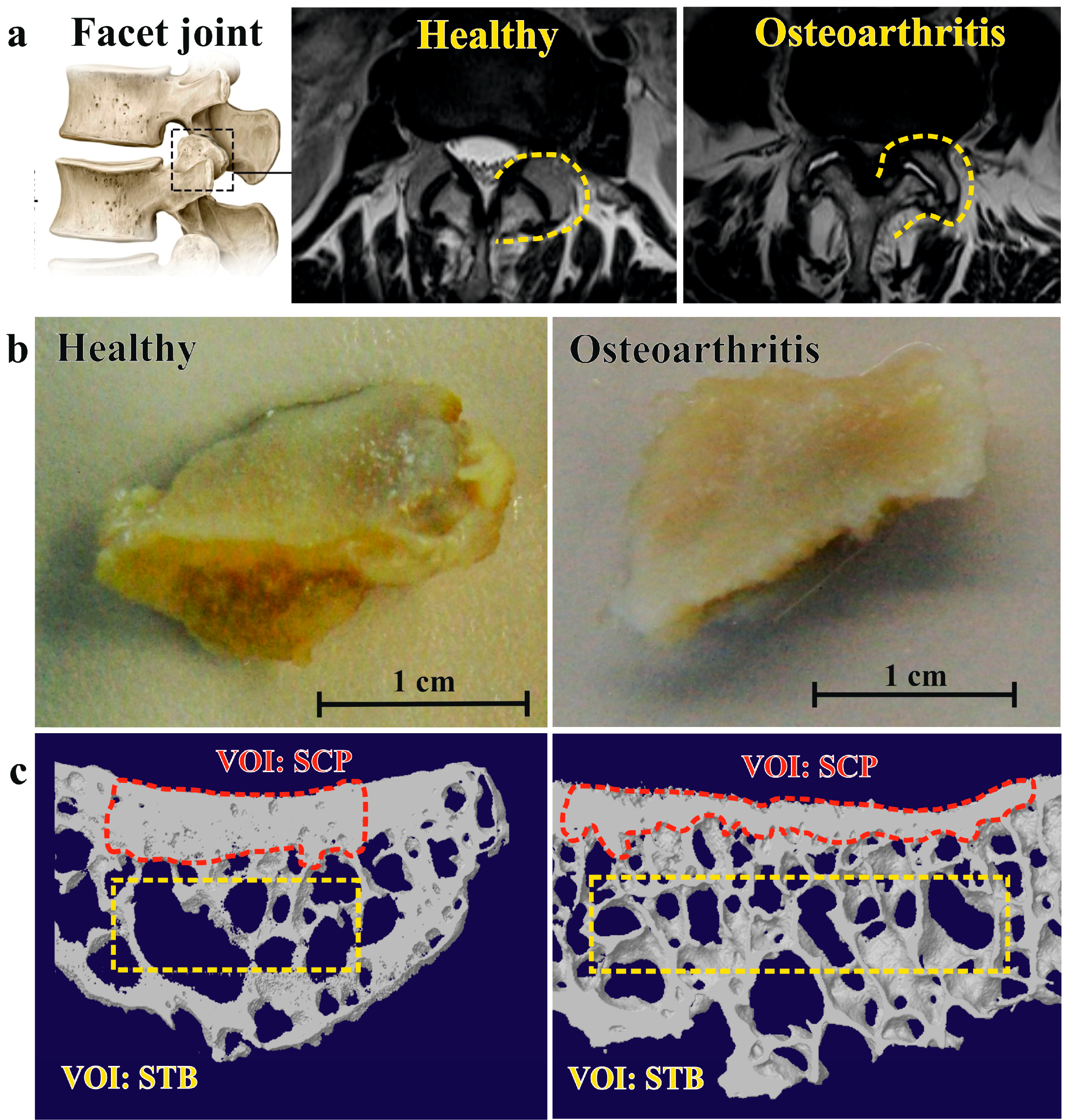
2.1. Facet Joint Osteoarthritis Is Characterized by Higher Trabecular Bone Volume and Less Subchondral Cortical Plate Thickness
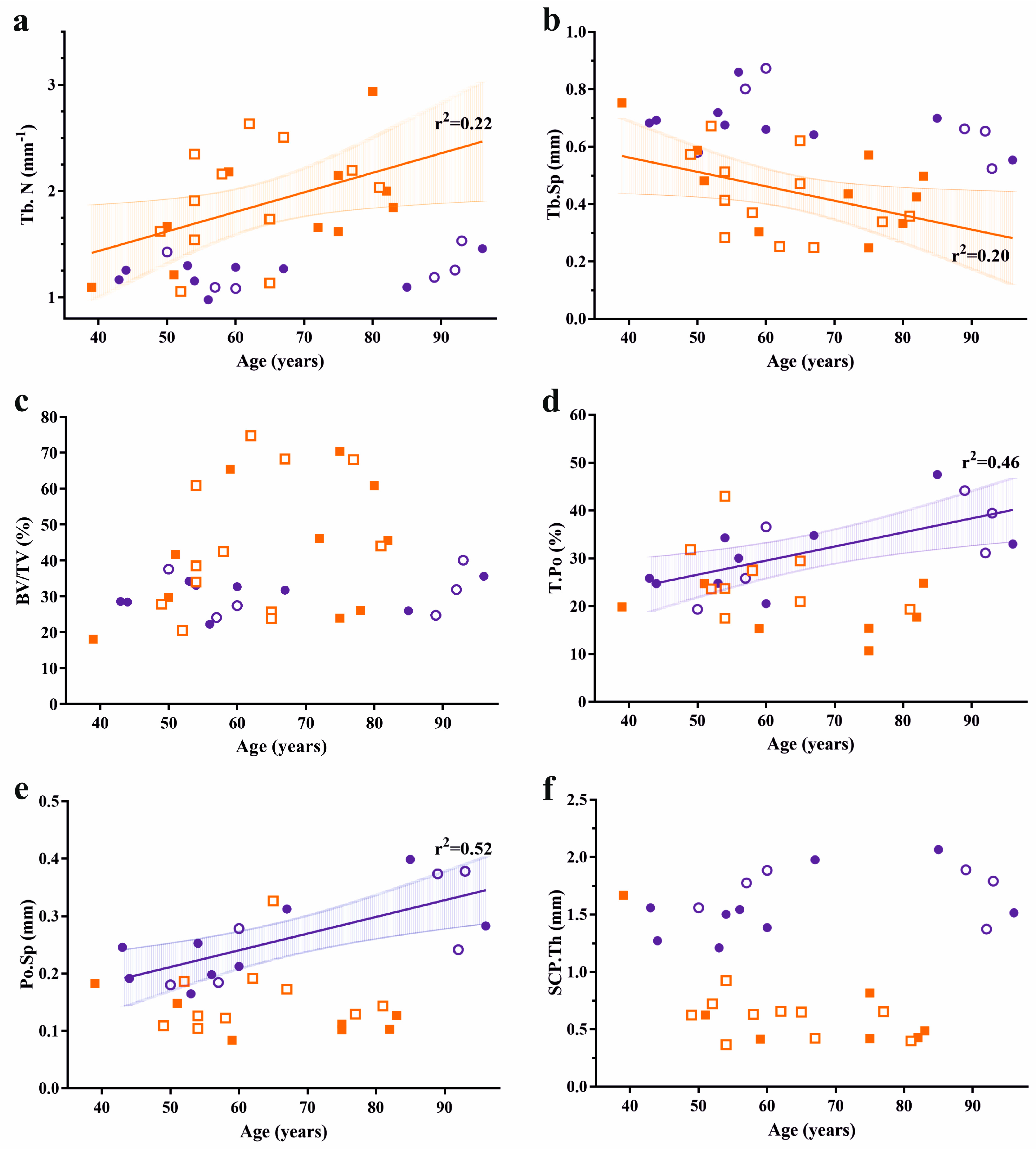
2.2. Bone Structural Parameters Associate with Osteoarthritis Severity and Age, but Are Not Gender-Dependent
2.3. Lack of Association between Trabecular and Cortical Structural Parameters in Facet Joints
3. Discussion
4. Materials and Methods
4.1. Collection of Clinical Specimens and Grading of Facet Joint Osteoarthritis
4.2. Micro Computed Tomography Scanning
4.3. Micro Computed Tomography Analysis
4.4. Comparative Analysis of Bone Structural Parameters of FJOA and Cadaveric Controls
4.5. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FJOA | Facet joint osteoarthritis |
| μCT | Micro computed tomography |
| SCP | Subchondral cortical plate |
| STB | Subchondral trabecular bone |
References
- Li, J.; Muehleman, C.; Abe, Y.; Masuda, K. Prevalence of facet joint degeneration in association with intervertebral joint degeneration in a sample of organ donors. J. Orthop. Res. 2011, 29, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Abbas, J.; Hamoud, K.; Peleg, S.; May, H.; Masharawi, Y.; Cohen, H.; Peled, N.; Hershkovitz, I. Facet joints arthrosis in normal and stenotic lumbar spines. Spine (Phila Pa 1976) 2011, 36, E1541–E1546. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, S.; Sonne-Holm, S.; Rovsing, H.; Monrad, H.; Gebuhr, P. Degenerative lumbar spondylolisthesis: An epidemiological perspective: The Copenhagen Osteoarthritis Study. Spine (Phila Pa 1976) 2007, 32, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Tamai, K.; Yamato, M.; An, H.S.; Yoshida, H.; Saotome, K.; Kurihashi, A. The relationship between facet joint osteoarthritis and disc degeneration of the lumbar spine: An MRI study. Eur. Spine J. 1999, 8, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.; Vaccaro, A.R.; Lee, S.; Lee, J.; Chang, H. The prevalence of lumbar spine facet joint osteoarthritis and its association with low back pain in selected Korean populations. Clin. Orthop. Surg. 2014, 6, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Li, L.; Kim, D.H.; Guermazi, A.; Berkin, V.; O’Donnell, C.J.; Hoffmann, U.; Cole, R.; Hunter, D.J. Facet joint osteoarthritis and low back pain in the community-based population. Spine (Phila Pa 1976) 2008, 33, 2560–2565. [Google Scholar] [CrossRef] [PubMed]
- Suri, P.; Hunter, D.J.; Rainville, J.; Guermazi, A.; Katz, J.N. Presence and extent of severe facet joint osteoarthritis are associated with back pain in older adults. Osteoarthr. Cartil. 2013, 21, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Vekaria, R.; Bhatt, R.; Ellard, D.R.; Henschke, N.; Underwood, M.; Sandhu, H. Intra-articular facet joint injections for low back pain: A systematic review. Eur. Spine J. 2016, 25, 1266–1281. [Google Scholar] [CrossRef] [PubMed]
- Varlotta, G.P.; Lefkowitz, T.R.; Schweitzer, M.; Errico, T.J.; Spivak, J.; Bendo, J.A.; Rybak, L. The lumbar facet joint: A review of current knowledge: Part II: Diagnosis and management. Skelet. Radiol. 2011, 40, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Ali, M.H.; Wydra, F.; Li, X.; Hamilton, J.L.; An, H.S.; Cs-Szabo, G.; Andrews, S.; Moric, M.; Xiao, G.; et al. Characterization of degenerative human facet joints and facet joint capsular tissues. Osteoarthr. Cartil. 2015, 23, 2242–2251. [Google Scholar] [CrossRef] [PubMed]
- Kras, J.V.; Tanaka, K.; Gilliland, T.M.; Winkelstein, B.A. An anatomical and immunohistochemical characterization of afferents innervating the C6-C7 facet joint after painful joint loading in the rat. Spine (Phila Pa 1976) 2013, 38, E325–E331. [Google Scholar] [CrossRef] [PubMed]
- Surace, M.F.; Prestamburgo, D.; Campagnolo, M.; Fagetti, A.; Murena, L. Presence of NGF and its receptor TrkA in degenerative lumbar facet joint specimens. Eur. Spine J. 2009, 18 (Suppl S1), 122–125. [Google Scholar] [CrossRef] [PubMed]
- Ashton, I.K.; Ashton, B.A.; Gibson, S.J.; Polak, J.M.; Jaffray, D.C.; Eisenstein, S.M. Morphological basis for back pain: The demonstration of nerve fibers and neuropeptides in the lumbar facet joint capsule but not in ligamentum flavum. J. Orthop. Res. 1992, 10, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Netzer, C.; Urech, K.; Hugle, T.; Benz, R.M.; Geurts, J.; Scharen, S. Characterization of subchondral bone histopathology of facet joint osteoarthritis in lumbar spinal stenosis. J. Orthop. Res. 2016, 34, 1475–1480. [Google Scholar] [CrossRef] [PubMed]
- Bleil, J.; Maier, R.; Hempfing, A.; Sieper, J.; Appel, H.; Syrbe, U. Granulation Tissue Eroding the Subchondral Bone Also Promotes New Bone Formation in Ankylosing Spondylitis. Arthritis Rheumatol. 2016, 68, 2456–2465. [Google Scholar] [CrossRef] [PubMed]
- Appel, H.; Maier, R.; Loddenkemper, C.; Kayser, R.; Meier, O.; Hempfing, A.; Sieper, J. Immunohistochemical analysis of osteoblasts in zygapophyseal joints of patients with ankylosing spondylitis reveal repair mechanisms similar to osteoarthritis. J. Rheumatol. 2010, 37, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Wilke, H.J.; Zanker, D.; Wolfram, U. Internal morphology of human facet joints: Comparing cervical and lumbar spine with regard to age, gender and the vertebral core. J. Anat. 2012, 220, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Zhang, Y.; Yin, X.; Lu, H.; Hu, J.; Duan, C. 3D visualization of the lumbar facet joint after degeneration using propagation phase contrast micro-tomography. Sci. Rep. 2016, 6, 21838. [Google Scholar] [CrossRef] [PubMed]
- Duan, C.Y.; Espinoza Orias, A.A.; Shott, S.; An, H.S.; Andersson, G.B.; Hu, J.Z.; Lu, H.B.; Inoue, N. In vivo measurement of the subchondral bone thickness of lumbar facet joint using magnetic resonance imaging. Osteoarth. Cartil. 2011, 19, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Zhen, G.; Wen, C.; Jia, X.; Li, Y.; Crane, J.L.; Mears, S.C.; Askin, F.B.; Frassica, F.J.; Chang, W.; Yao, J.; et al. Inhibition of TGF-beta signaling in mesenchymal stem cells of subchondral bone attenuates osteoarthritis. Nat. Med. 2013, 19, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Botter, S.M.; van Osch, G.J.; Clockaerts, S.; Waarsing, J.H.; Weinans, H.; van Leeuwen, J.P. Osteoarthritis induction leads to early and temporal subchondral plate porosity in the tibial plateau of mice: An in vivo microfocal computed tomography study. Arthritis Rheumatol. 2011, 63, 2690–2699. [Google Scholar] [CrossRef] [PubMed]
- Sniekers, Y.H.; Intema, F.; Lafeber, F.P.; van Osch, G.J.; van Leeuwen, J.P.; Weinans, H.; Mastbergen, S.C. A role for subchondral bone changes in the process of osteoarthritis; a micro-CT study of two canine models. BMC Musculoskelet. Disord. 2008, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhu, H.; Zhang, K.; Chen, K.; Yang, H. Estrogen deficiency accelerates lumbar facet joints arthritis. Sci. Rep. 2017, 7, 1379. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.E.; Kim, C.H. Mechanical consequence of trabecular bone loss and its treatment: A three-dimensional model simulation. Bone 2002, 30, 404–411. [Google Scholar] [CrossRef]
- Cavani, F.; Ferretti, M.; Smargiassi, A.; Palumbo, C. PTH(1-34) effects on repairing experimentally drilled holes in rat femur: Novel aspects—Qualitative vs. quantitative improvement of osteogenesis. J. Anat. 2017, 230, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, M.; Palumbo, C.; Contri, M.; Marotti, G. Static and dynamic osteogenesis: Two different types of bone formation. Anat. Embryol. 2002, 206, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.P.; Nelson, A.E.; Kraus, V.B.; Renner, J.B.; Jordan, J.M. Biomarkers reflect differences in osteoarthritis phenotypes of the lumbar spine: The Johnston County Osteoarthritis Project. Osteoarthr. Cartil. 2017, 25, 1672–1679. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Michaelis, M.; Ladel, C.; Siebuhr, A.S.; Bihlet, A.R.; Andersen, J.R.; Guehring, H.; Christiansen, C.; Bay-Jensen, A.C.; Kraus, V.B. Disease-modifying treatments for osteoarthritis (DMOADs) of the knee and hip: Lessons learned from failures and opportunities for the future. Osteoarthr. Cartil. 2016, 24, 2013–2021. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Bay-Jensen, A.C.; Lories, R.J.; Abramson, S.; Spector, T.; Pastoureau, P.; Christiansen, C.; Attur, M.; Henriksen, K.; Goldring, S.R.; et al. The coupling of bone and cartilage turnover in osteoarthritis: Opportunities for bone antiresorptives and anabolics as potential treatments? Ann. Rheum. Dis. 2014, 73, 336–348. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T.; Nevitt, M.C.; Ensrud, K.E.; Bauer, D.; Felson, D.T. The effect of alendronate on progression of spinal osteophytes and disc-space narrowing. Ann. Rheum. Dis. 2008, 67, 1427–1430. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, D.S.; Liu, R.W.; Xie, K.K.; Morris, W.Z.; Gebhart, J.J.; Gordon, Z.L. Increased and decreased pelvic incidence, sagittal facet joint orientations are associated with lumbar spine osteoarthritis in a large cadaveric collection. Int. Orthop. 2017, 41, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Suri, P.; Guermazi, A.; Li, L.; Hunter, D.J. Facet orientation and tropism: Associations with facet joint osteoarthritis and degeneratives. Spine (Phila Pa 1976) 2009, 34, E579–E585. [Google Scholar] [CrossRef] [PubMed]
- Weishaupt, D.; Zanetti, M.; Boos, N.; Hodler, J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skelet. Radiol. 1999, 28, 215–219. [Google Scholar] [CrossRef]
- Hemmatian, H.; Laurent, M.R.; Ghazanfari, S.; Vanderschueren, D.; Bakker, A.D.; Klein-Nulend, J.; van Lenthe, G.H. Accuracy and reproducibility of mouse cortical bone microporosity as quantified by desktop microcomputed tomography. PLoS ONE 2017, 12, e0182996. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Healthy | Osteoarthritis | p-Value |
|---|---|---|---|
| Age in years | 66.6 ± 18.9 | 63.6 ± 12.5 | 0.563 |
| Gender (f/m) | 9/6 | 12/10 | 0.398 |
| Subchondral Trabecular Bone | |||
| Trabecular number in mm−1 | 1.24 ± 0.15 | 1.87 ± 0.50 | <0.0001 |
| Trabecular separation in mm | 0.685 ± 0.099 | 0.443 ± 0.145 | <0.0001 |
| Trabecular thickness in mm | 0.240 ± 0.018 | 0.232 ± 0.064 | 0.637 |
| Bone volume fraction in % | 30.5 ± 5.2 | 43.5 ± 18.4 | 0.012 |
| Trabecular pattern factor in mm−1 | −0.080 ± 0.98 | −4.54 ± 7.04 | 0.021 |
| Degree of anisotropy | 9.6 ± 15.6 | 6.5 ± 8.5 | 0.453 |
| Subchondral Cortical Plate | |||
| Total porosity in % | 31.5 ± 8.2 | 22.9 ± 7.8 | 0.0054 |
| Pore space in mm | 0.26 ± 0.08 | 0.15 ± 0.06 | <0.0001 |
| Cortical thickness in mm | 1.62 ± 0.26 | 0.62 ± 0.31 | <0.0001 |
| Parameter | Spearman r [95% CI] | p-Value |
|---|---|---|
| Age | 0.47 [0.04, 0.75] | 0.028 |
| Subchondral Trabecular Bone | ||
| Trabecular number | 0.55 [0.15, 0.79] | 0.009 |
| Trabecular separation | −0.57 [−0.80, −0.18] | 0.006 |
| Trabecular thickness | 0.27 [−0.18, 063] | 0.219 |
| Bone volume fraction | 0.52 [0.11, 0.78] | 0.014 |
| Trabecular pattern factor | −0.42 [−0.72, 0.02] | 0.053 |
| Degree of anisotropy | 0.37 [−0.07, 0.69] | 0.260 |
| Subchondral Cortical Plate | ||
| Total porosity | −0.07 [−0.55, 0.45] | 0.798 |
| Pore space | −0.48 [−0.79, 0.04] | 0.063 |
| Cortical thickness | −0.32 [−0.71, 0.22] | 0.221 |
| Healthy | Osteoarthritis | |||
|---|---|---|---|---|
| Parameter | Pearson r [95% CI] | p-Value | Pearson r [95% CI] | p-Value |
| Subchondral Cortical Plate | ||||
| Total porosity | 0.73 [0.34, 0.90] | 0.002 | −0.07 [−0.55, 0.44] | 0.797 |
| Pore space | 0.75 [0.39, 0.91] | 0.001 | 0.28 [−0.25, 0.68] | 0.291 |
| Subchondral Trabecular Bone | ||||
| Trabecular thickness | −0.17 [−0.63, 0.37] | 0.543 | −0.04 [−0.53, 0.46] | 0.875 |
| Trabecular number | −0.22 [−0.66, 0.33] | 0.427 | −0.48 [−0.79, 0.03] | 0.068 |
| Trabecular separation | 0.08 [−0.45, 0.57] | 0.772 | 0.48 [−0.02, 0.79] | 0.062 |
| Bone volume fraction | −0.29 [−0.69, 0.26] | 0.299 | −0.25 [−0.66, 0.28] | 0.347 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netzer, C.; Distel, P.; Wolfram, U.; Deyhle, H.; Jost, G.F.; Schären, S.; Geurts, J. Comparative Analysis of Bone Structural Parameters Reveals Subchondral Cortical Plate Resorption and Increased Trabecular Bone Remodeling in Human Facet Joint Osteoarthritis. Int. J. Mol. Sci. 2018, 19, 845. https://doi.org/10.3390/ijms19030845
Netzer C, Distel P, Wolfram U, Deyhle H, Jost GF, Schären S, Geurts J. Comparative Analysis of Bone Structural Parameters Reveals Subchondral Cortical Plate Resorption and Increased Trabecular Bone Remodeling in Human Facet Joint Osteoarthritis. International Journal of Molecular Sciences. 2018; 19(3):845. https://doi.org/10.3390/ijms19030845
Chicago/Turabian StyleNetzer, Cordula, Pascal Distel, Uwe Wolfram, Hans Deyhle, Gregory F. Jost, Stefan Schären, and Jeroen Geurts. 2018. "Comparative Analysis of Bone Structural Parameters Reveals Subchondral Cortical Plate Resorption and Increased Trabecular Bone Remodeling in Human Facet Joint Osteoarthritis" International Journal of Molecular Sciences 19, no. 3: 845. https://doi.org/10.3390/ijms19030845
APA StyleNetzer, C., Distel, P., Wolfram, U., Deyhle, H., Jost, G. F., Schären, S., & Geurts, J. (2018). Comparative Analysis of Bone Structural Parameters Reveals Subchondral Cortical Plate Resorption and Increased Trabecular Bone Remodeling in Human Facet Joint Osteoarthritis. International Journal of Molecular Sciences, 19(3), 845. https://doi.org/10.3390/ijms19030845