β4 and β6 Integrin Expression Is Associated with the Subclassification and Clinicopathological Features of Intrahepatic Cholangiocarcinoma

Abstract
:1. Introduction
2. Results
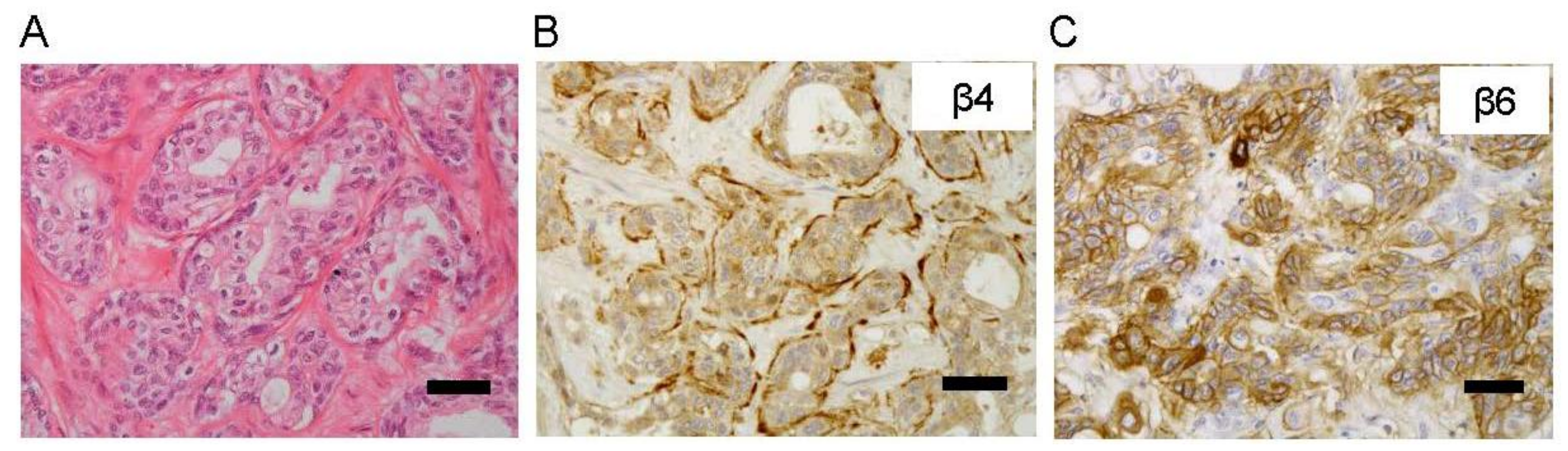
2.1. Relationships between β4 and β6 Integrin Expressions and Clinicopathological Features in Patients with Intrahepatic Cholangiocarcinoma (ICC)
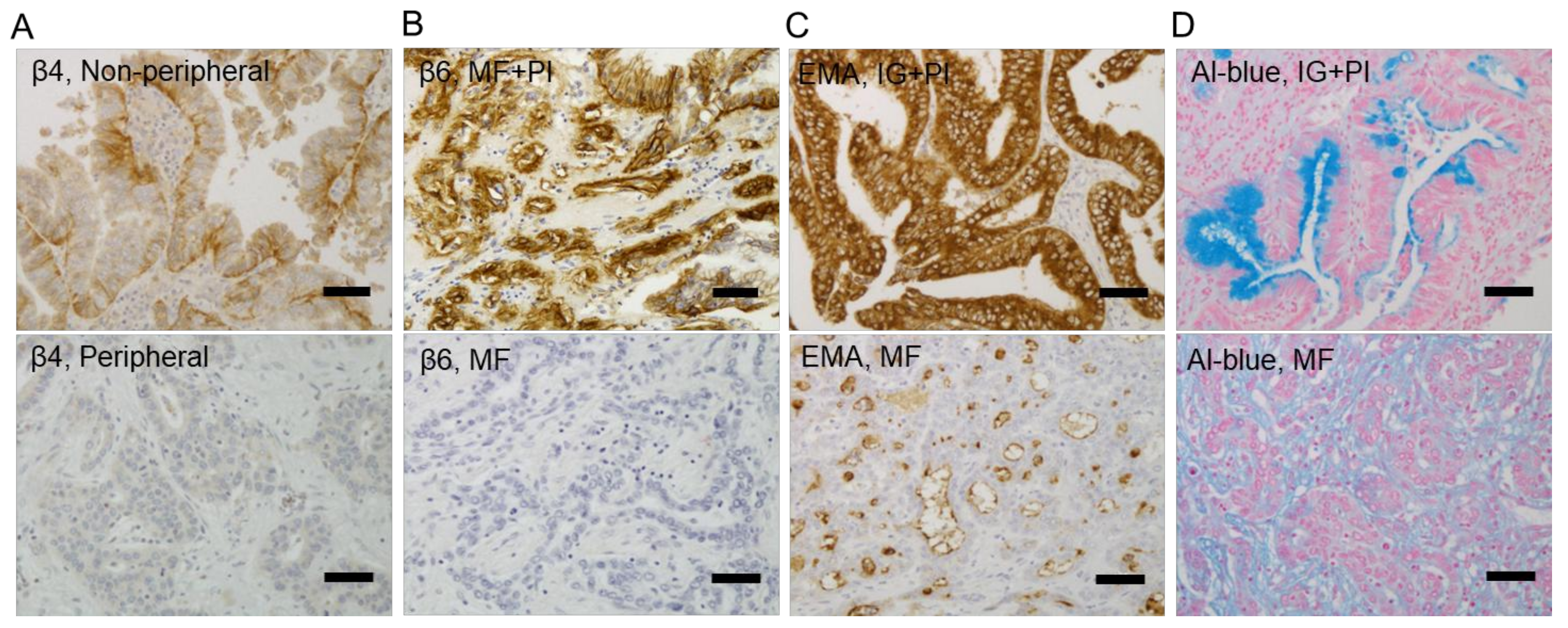
2.2. Correlations between β4 and β6 Integrin Expressions and EMA-Positive Patterns or Mucus Production in ICC
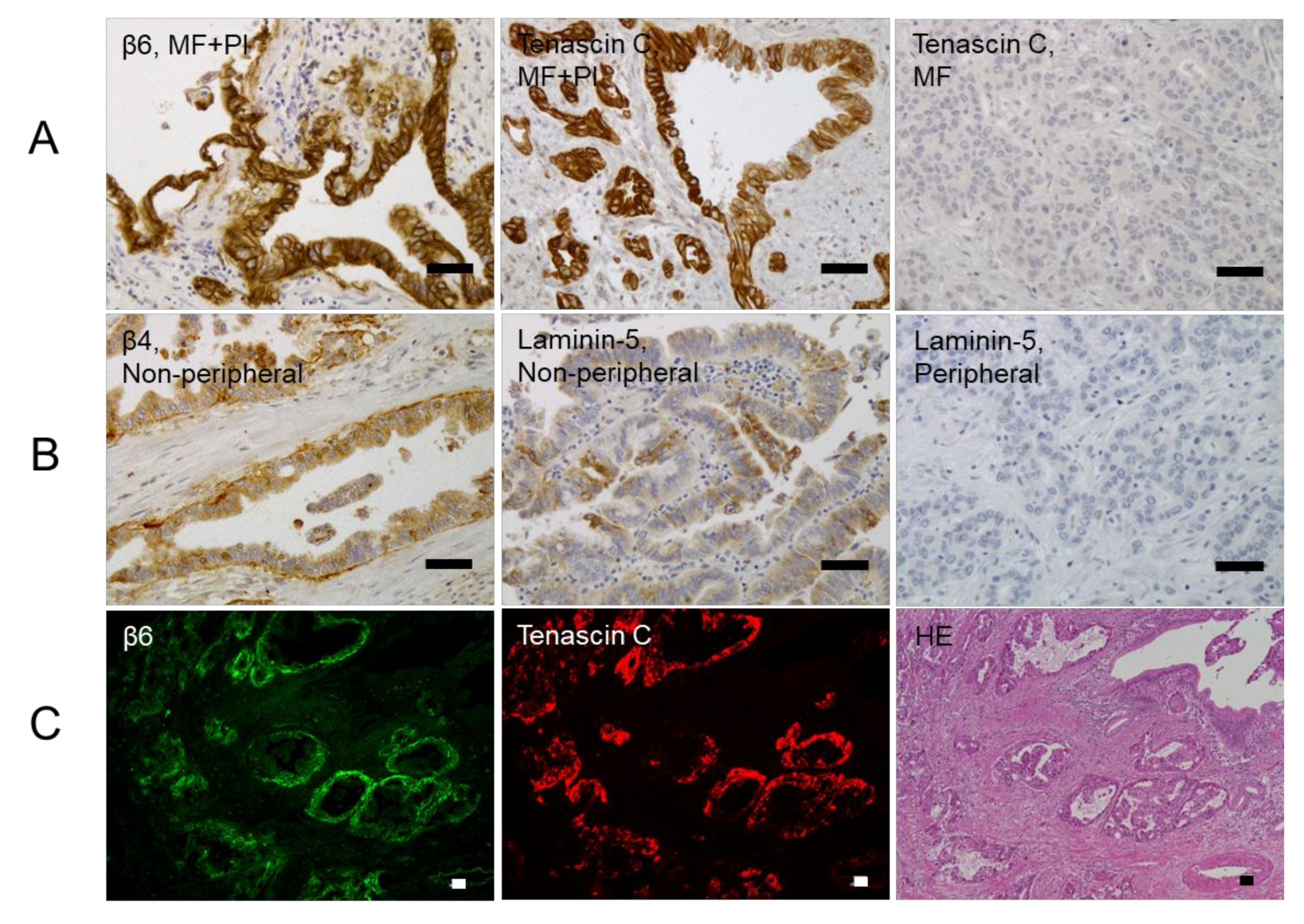
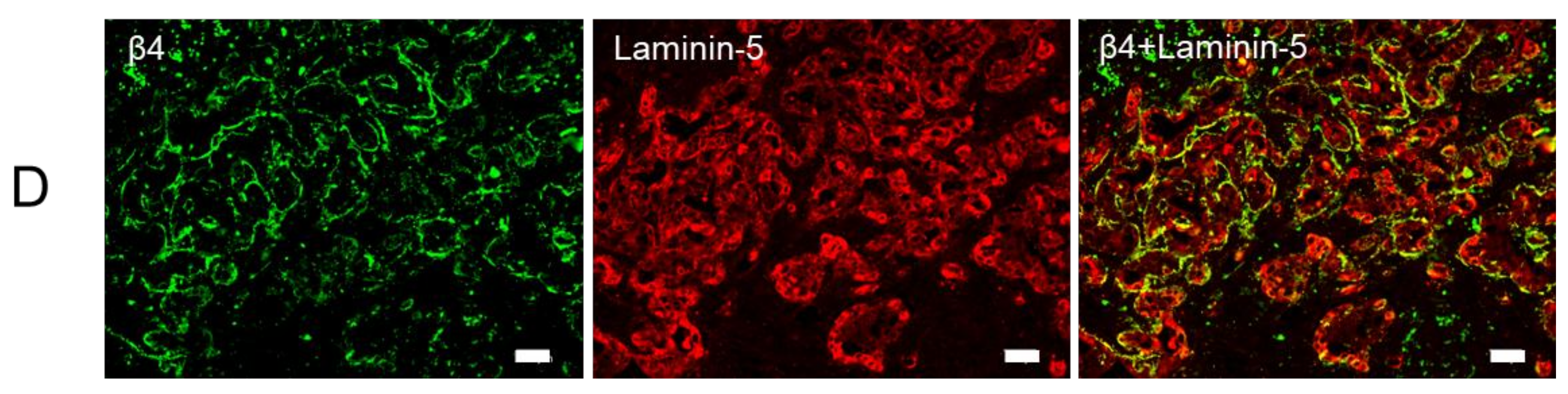
2.3. Relationships between β4 and β6 Integrin Expressions and Laminin-5 or Tenascin-C Expressions in ICC
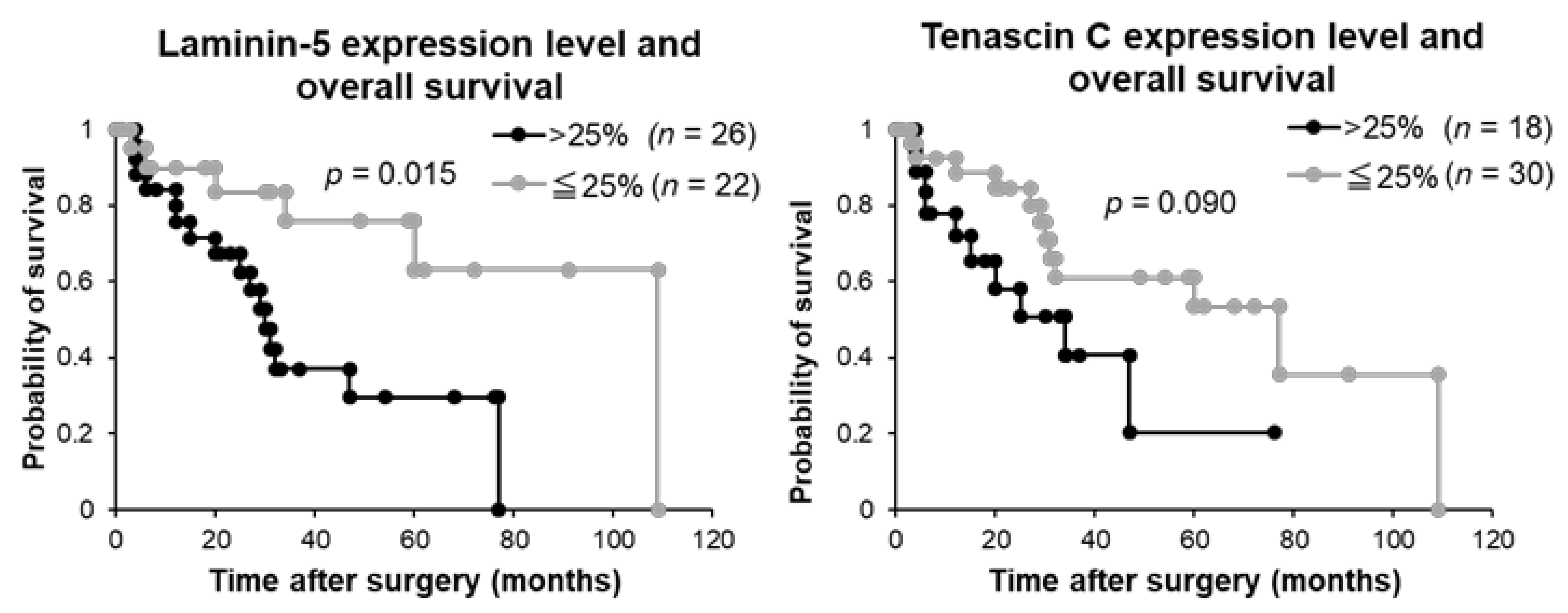
2.4. Relationships between Laminin-5 and Tenascin-C Expressions and Clinicopathological Features in Patients with ICC
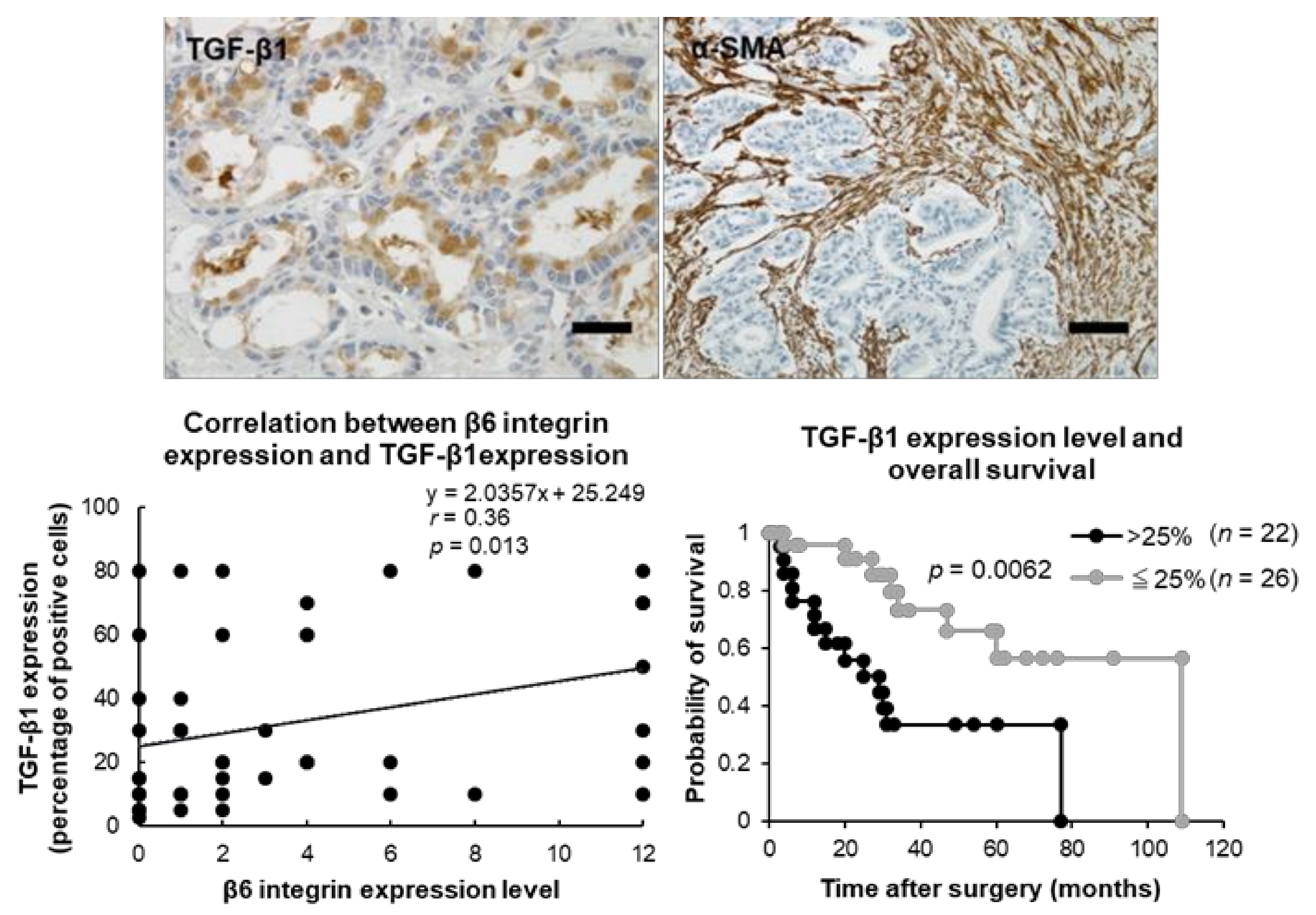
2.5. Relationships between β6 Integrin Expression and TGF-β1 and α-SMA Expressions in ICC
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. Immunohistochemistry
4.3. Immunofluorescence Analysis
4.4. Evaluation of Immunohistochemical Staining
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed]
- Buettner, S.; van Vugt, J.L.; IJzermans, J.N.; Groot Koerkamp, B. Intrahepatic cholangiocarcinoma: Current perspectives. Onco Targets Ther. 2017, 10, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Esnaola, N.F.; Meyer, J.E.; Karachristos, A.; Maranki, J.L.; Camp, E.R.; Denlinger, C.S. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016, 122, 1349–1369. [Google Scholar] [CrossRef] [PubMed]
- Njei, B. Changing pattern of epidemiology in intrahepatic cholangiocarcinoma. Hepatology 2014, 60, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Lu, L.; Lin, P.; Chen, Z.; Quan, Z.; Tang, Z. Multiple cellular origins and molecular evolution of intrahepatic cholangiocarcinoma. Cancer Lett. 2016, 379, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Nakanuma, Y.; Sato, Y.; Harada, K.; Sasaki, M.; Xu, J.; Ikeda, H. Pathological classification of intrahepatic cholangiocarcinoma based on a new concept. World J. Hepatol. 2010, 2, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, Y.; Kokudo, N.; Matsuyama, Y.; Sakamoto, M.; Izumi, N.; Kadoya, M.; Kaneko, S.; Ku, Y.; Kudo, M.; Takayama, T.; et al. Liver Cancer Study Group of J. Proposal of a new staging system for intrahepatic cholangiocarcinoma: Analysis of surgical patients from a nationwide survey of the Liver Cancer Study Group of Japan. Cancer 2016, 122, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Vijgen, S.; Terris, B.; Rubbia-Brandt, L. Pathology of intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2017, 6, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Komuta, M.; Govaere, O.; Vandecaveye, V.; Akiba, J.; Van Steenbergen, W.; Verslype, C.; Laleman, W.; Pirenne, J.; Aerts, R.; Yano, H.; et al. Histological diversity in cholangiocellular carcinoma reflects the different cholangiocyte phenotypes. Hepatology 2012, 55, 1876–1888. [Google Scholar] [CrossRef] [PubMed]
- Liau, J.Y.; Tsai, J.H.; Yuan, R.H.; Chang, C.N.; Lee, H.J.; Jeng, Y.M. Morphological subclassification of intrahepatic cholangiocarcinoma: Etiological, clinicopathological, and molecular features. Mod. Pathol. 2014, 27, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, A.; Misumi, K.; Shibahara, J.; Arita, J.; Sakamoto, Y.; Hasegawa, K.; Kokudo, N.; Fukayama, M. Distinct Clinicopathologic and Genetic Features of 2 Histologic Subtypes of Intrahepatic Cholangiocarcinoma. Am. J. Surg. Pathol. 2016, 40, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Zhao, Y.; Yuan, Z.; Qin, G. Research advances on structure and biological functions of integrins. Springerplus 2016, 5, 1094. [Google Scholar] [CrossRef] [PubMed]
- Volpes, R.; van den Oord, J.J.; Desmet, V.J. Integrins as differential cell lineage markers of primary liver tumors. Am. J. Pathol. 1993, 142, 1483–1492. [Google Scholar] [PubMed]
- Ding, Y.B.; Deng, B.; Huang, Y.S.; Xiao, W.M.; Wu, J.; Zhang, Y.Q.; Wang, Y.Z.; Wu, D.C.; Lu, G.T.; Wu, K.Y. A high level of integrin α6 expression in human intrahepatic cholangiocarcinoma cells is associated with a migratory and invasive phenotype. Dig. Dis. Sci. 2013, 58, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Breuss, J.M.; Gallo, J.; DeLisser, H.M.; Klimanskaya, I.V.; Folkesson, H.G.; Pittet, J.F.; Nishimura, S.L.; Aldape, K.; Landers, D.V.; Carpenter, W.; et al. Expression of the β 6 integrin subunit in development, neoplasia and tissue repair suggests a role in epithelial remodeling. J. Cell Sci. 1995, 108 Pt 6, 2241–2251. [Google Scholar] [PubMed]
- Patsenker, E.; Wilkens, L.; Banz, V.; Osterreicher, C.H.; Weimann, R.; Eisele, S.; Keogh, A.; Stroka, D.; Zimmermann, A.; Stickel, F. The αvβ6 integrin is a highly specific immunohistochemical marker for cholangiocarcinoma. J. Hepatol. 2010, 52, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Biswas, S.; Liang, B.; Zou, X.; Shan, L.; Li, Y.; Fang, R.; Niu, J. Integrin β6 serves as an immunohistochemical marker for lymph node metastasis and promotes cell invasiveness in cholangiocarcinoma. Sci. Rep. 2016, 6, 30081. [Google Scholar] [CrossRef] [PubMed]
- Soejima, Y.; Inoue, M.; Takahashi, Y.; Uozaki, H.; Sawabe, M.; Fukusato, T. Integrins αvβ6, α6β4 and α3β1 are down-regulated in cholangiolocellular carcinoma but not cholangiocarcinoma. Hepatol. Res. 2014, 44, E320–E334. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Marshall, J.F. The role of integrins in TGFβ activation in the tumour stroma. Cell Tissue Res. 2016, 365, 657–673. [Google Scholar] [CrossRef] [PubMed]
- Otranto, M.; Sarrazy, V.; Bonte, F.; Hinz, B.; Gabbiani, G.; Desmouliere, A. The role of the myofibroblast in tumor stroma remodeling. Cell Adhes. Migr. 2012, 6, 203–219. [Google Scholar] [CrossRef] [PubMed]
- Maeno, S.; Kondo, F.; Sano, K.; Takada, T.; Asano, T. Morphometric and immunohistochemical study of cholangiolocellular carcinoma: Comparison with non-neoplastic cholangiole, interlobular duct and septal duct. J. Hepatobiliary Pancreat Sci. 2012, 19, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Aishima, S.; Oda, Y. Pathogenesis and classification of intrahepatic cholangiocarcinoma: Different characters of perihilar large duct type versus peripheral small duct type. J. Hepatobiliary Pancreat Sci. 2015, 22, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Sia, D.; Hoshida, Y.; Villanueva, A.; Roayaie, S.; Ferrer, J.; Tabak, B.; Peix, J.; Sole, M.; Tovar, V.; Alsinet, C.; et al. Integrative molecular analysis of intrahepatic cholangiocarcinoma reveals 2 classes that have different outcomes. Gastroenterology 2013, 144, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Ren, Z.; Fan, J.; Gao, Q. Genetic profiling of intrahepatic cholangiocarcinoma and its clinical implication in targeted therapy. Am. J. Cancer Res. 2016, 6, 577–586. [Google Scholar] [PubMed]
- Walter, D.; Doring, C.; Feldhahn, M.; Battke, F.; Hartmann, S.; Winkelmann, R.; Schneider, M.; Bankov, K.; Schnitzbauer, A.; Zeuzem, S.; et al. Intratumoral heterogeneity of intrahepatic cholangiocarcinoma. Oncotarget 2017, 8, 14957–14968. [Google Scholar] [CrossRef] [PubMed]
- Kusaka, Y.; Tokiwa, T.; Sato, J. Establishment and characterization of a cell line from a human cholangiocellular carcinoma. Res. Exp. Med. 1988, 188, 367–375. [Google Scholar] [CrossRef]
- Lu, S.; Simin, K.; Khan, A.; Mercurio, A.M. Analysis of integrin β4 expression in human breast cancer: Association with basal-like tumors and prognostic significance. Clin. Cancer Res. 2008, 14, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.L.; West, D.; Wang, C.; Weiss, H.L.; Gal, T.; Durbin, E.B.; O’Connor, W.; Chen, M.; O’Connor, K.L. Elevated integrin α6 β4 expression is associated with venous invasion and decreased overall survival in non-small cell lung cancer. Hum. Pathol. 2016, 54, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.L.; Lai, I.R.; Peng, Y.J.; Ding, S.T.; Shen, T.L. Activation of focal adhesion kinase through an interaction with β4 integrin contributes to tumorigenicity of colon cancer. FEBS Lett. 2016, 590, 1826–1837. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, T.; Otero, J.; Chen, Y.; Kim, Y.M.; Koutcher, J.A.; Satagopan, J.; Reuter, V.; Carver, B.; de Stanchina, E.; Enomoto, K.; et al. β4 Integrin signaling induces expansion of prostate tumor progenitors. J. Clin. Investig. 2013, 123, 682–699. [Google Scholar] [CrossRef] [PubMed]
- Cantor, D.I.; Cheruku, H.R.; Nice, E.C.; Baker, M.S. Integrin αvβ6 sets the stage for colorectal cancer metastasis. Cancer Metastasis Rev. 2015, 34, 715–734. [Google Scholar] [CrossRef] [PubMed]
- Berghoff, A.S.; Kovanda, A.K.; Melchardt, T.; Bartsch, R.; Hainfellner, J.A.; Sipos, B.; Schittenhelm, J.; Zielinski, C.C.; Widhalm, G.; Dieckmann, K.; et al. αvβ3, αvβ5 and αvβ6 integrins in brain metastases of lung cancer. Clin. Exp. Metastasis 2014, 31, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Z.; Zhou, R.; Xu, X.; Tian, T.; Liu, Y.; Liu, Y.; Lian, P.; Wang, J.; Xu, K. Clinical significance of integrin αvβ6 expression effects on gastric carcinoma invasiveness and progression via cancer-associated fibroblasts. Med. Oncol. 2013, 30, 580. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, C.; Sgarra, C.; Trerotoli, P.; Lupo, L.; Azzariti, A.; Antonaci, S.; Giannelli, G. Laminin-5 stimulates hepatocellular carcinoma growth through a different function of α6β4 and α3β1 integrins. Hepatology 2007, 46, 1801–1809. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.P.; Chiquet-Ehrismann, R. Tenascin-C: Its functions as an integrin ligand. Int. J. Biochem. Cell Biol. 2015, 65, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Aishima, S.; Matsuura, S.; Terashi, T.; Taguchi, K.; Shimada, M.; Maehara, Y.; Tsuneyoshi, M. Aberrant expression of laminin gamma 2 chain and its prognostic significance in intrahepatic cholangiocarcinoma according to growth morphology. Mod. Pathol. 2004, 17, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Aishima, S.; Taguchi, K.; Terashi, T.; Matsuura, S.; Shimada, M.; Tsuneyoshi, M. Tenascin expression at the invasive front is associated with poor prognosis in intrahepatic cholangiocarcinoma. Mod. Pathol. 2003, 16, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, M.; Derynck, R.; Miyazono, K. TGF-β and the TGF-β Family: Context-Dependent Roles in Cell and Tissue Physiology. Cold Spring Harb. Perspect. Biol. 2016, 8, a021873. [Google Scholar] [CrossRef] [PubMed]
- Nakanuma, Y.; Curabo, M.P.; Franceschi, S. Intrahepatic cholangiocarcinoma. In WHO Classification of Tumours of the Digestive System, 4th ed.; Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D., Eds.; IARC: Lyon, France, 2010; pp. 217–224. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Cases (n = 48) | β4 integrin Expression | β6 integrin Expression | ||||||
|---|---|---|---|---|---|---|---|---|
| Negative-Low (n = 29) | High (n = 19) | p-Value | Negative-Low (n = 36) | High (n = 12) | p-Value | |||
| Gender | Male | 36 | 23 | 13 | 0.39 | 26 | 10 | 0.36 |
| Female | 12 | 6 | 6 | 10 | 2 | |||
| Age (mean) (years) | 71.5 (51–84) | 69.1 (39–84) | 0.42 | 70.4 (39–84) | 71.1 (51–82) | 0.83 | ||
| Tumor size (mean) (mm) | 60.2 (20–220) | 56.7 (18–140) | 0.78 | 61.9 (18–220) | 49.4 (23–100) | 0.20 | ||
| Localization | Peripheral | 38 | 26 | 12 | 0.033 * | 32 | 6 | 0.0092 ** |
| Non-peripheral | 10 | 3 | 7 | 4 | 6 | |||
| Macroscopic type | MF | 42 | 29 | 13 | 0.0022 *** | 34 | 8 | 0.028 * |
| MF+PI, IG+PI, PI | 6 | 0 | 6 | 2 | 4 | |||
| Histological differentiation | Well | 6 | 3 | 3 | 0.023 * | 2 | 4 | 0.0068 ** |
| Moderate | 29 | 14 | 15 | 21 | 8 | |||
| Poor | 13 | 12 | 1 | 13 | 0 | |||
| Growth type | Expansive | 23 | 18 | 5 | 0.015 * | 20 | 3 | 0.065 |
| Infiltrative | 25 | 11 | 14 | 16 | 9 | |||
| HBV | + | 6 | 5 | 1 | 0.22 | 6 | 0 | 0.15 |
| − | 42 | 24 | 18 | 30 | 12 | |||
| HCV | + | 8 | 6 | 2 | 0.31 | 6 | 2 | 0.68 |
| − | 40 | 23 | 17 | 30 | 10 | |||
| Cirrhosis | + | 7 | 4 | 3 | 0.58 | 7 | 0 | 0.11 |
| − | 41 | 25 | 16 | 29 | 12 | |||
| Serosa invasion | + | 24 | 12 | 12 | 0.14 | 16 | 8 | 0.18 |
| − | 24 | 17 | 7 | 20 | 4 | |||
| Portal vein invasion | + | 39 | 23 | 16 | 0.49 | 27 | 12 | 0.056 |
| − | 9 | 6 | 3 | 9 | 0 | |||
| Hepatic vein invasion | + | 21 | 10 | 11 | 0.11 | 14 | 7 | 0.24 |
| − | 27 | 19 | 8 | 22 | 5 | |||
| Hepatic artery invasion | + | 4 | 2 | 2 | 0.52 | 3 | 1 | 0.74 |
| − | 44 | 27 | 17 | 33 | 11 | |||
| Bile duct invasion | + | 26 | 11 | 15 | 0.0053 ** | 15 | 11 | 0.0026 *** |
| − | 22 | 18 | 4 | 21 | 1 | |||
| Intrahepatic metastasis | + | 21 | 10 | 11 | 0.11 | 13 | 8 | 0.065 |
| − | 27 | 19 | 8 | 23 | 4 | |||
| Lymph node metastasis | + | 14 | 6 | 8 | 0.11 | 9 | 5 | 0.93 |
| − | 34 | 23 | 11 | 27 | 7 | |||
| Alcian blue stain | ≤10% | 12 | 11 | 1 | 0.011 * | 12 | 0 | 0.018 * |
| >10% | 36 | 18 | 18 | 24 | 12 | |||
| EMA | Luminal pattern | 11 | 10 | 1 | 0.018 * | 10 | 1 | 0.16 |
| Cytoplasmic pattern | 37 | 19 | 18 | 26 | 11 | |||
| Laminin-5 | ≤25% | 22 | 21 | 1 | <0.001 *** | n.d. | n.d. | |
| >25% | 26 | 8 | 18 | n.d. | n.d. | |||
| Tenascin-C | ≤25% | 30 | n.d. | n.d. | 26 | 4 | 0.016 * | |
| >25% | 18 | n.d. | n.d. | 10 | 8 | |||
| Number of Cases (n = 48) | Laminin-5 Expression | Tenascin-C Expression | ||||||
|---|---|---|---|---|---|---|---|---|
| ≤25% (n = 22) | >25% (n = 26) | p-Value | ≤25% (n = 30) | >25% (n = 18) | p-Value | |||
| Gender | Male | 36 | 17 | 19 | 0.74 | 21 | 15 | 0.25 |
| Female | 12 | 5 | 7 | 9 | 3 | |||
| Age (mean) (years) | 72.5 (59–84) | 68.9 (39–84) | 0.21 | 72.5 (53–84) | 67.3 (39–83) | 0.084 | ||
| Tumor size (mean) (mm) | 64.6 (20–220) | 53.9 (18–140) | 0.37 | 56.9 (20–150) | 61.9 (18–220) | 0.68 | ||
| Localization | Peripheral | 38 | 18 | 20 | 0.48 | 25 | 13 | 0.29 |
| Non-peripheral | 10 | 4 | 6 | 5 | 5 | |||
| Macroscopic type | MF | 42 | 22 | 20 | 0.019 * | 27 | 15 | 0.40 |
| MF+PI, IG+PI, PI | 6 | 0 | 6 | 3 | 3 | |||
| Histological differentiation | Well | 6 | 3 | 3 | 0.74 | 3 | 3 | 0.15 |
| Moderate | 29 | 12 | 17 | 16 | 13 | |||
| Poor | 13 | 7 | 6 | 11 | 2 | |||
| Growth type | Expansive | 23 | 14 | 9 | 0.045 * | 18 | 5 | 0.031 * |
| Infiltrative | 25 | 8 | 17 | 12 | 13 | |||
| Serosa invasion | + | 24 | 10 | 14 | 0.56 | 14 | 10 | 0.55 |
| − | 24 | 12 | 12 | 16 | 8 | |||
| Portal vein invasion | + | 39 | 18 | 21 | 0.61 | 24 | 15 | 0.55 |
| − | 9 | 4 | 5 | 6 | 3 | |||
| Hepatic vein invasion | + | 21 | 6 | 15 | 0.034 * | 12 | 9 | 0.50 |
| − | 27 | 16 | 11 | 18 | 9 | |||
| Hepatic artery invasion | + | 4 | 2 | 2 | 0.63 | 2 | 2 | 0.48 |
| − | 44 | 20 | 24 | 28 | 16 | |||
| Bile duct invasion | + | 26 | 10 | 16 | 0.27 | 14 | 12 | 0.18 |
| − | 22 | 12 | 10 | 16 | 6 | |||
| Intrahepatic metastasis | + | 21 | 7 | 14 | 0.59 | 11 | 10 | 0.20 |
| − | 27 | 15 | 22 | 19 | 8 | |||
| Lymph node metastasis | + | 14 | 3 | 11 | 0.029 * | 7 | 7 | 0.21 |
| − | 34 | 19 | 15 | 23 | 11 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soejima, Y.; Takeuchi, M.; Akashi, T.; Sawabe, M.; Fukusato, T. β4 and β6 Integrin Expression Is Associated with the Subclassification and Clinicopathological Features of Intrahepatic Cholangiocarcinoma. Int. J. Mol. Sci. 2018, 19, 1004. https://doi.org/10.3390/ijms19041004
Soejima Y, Takeuchi M, Akashi T, Sawabe M, Fukusato T. β4 and β6 Integrin Expression Is Associated with the Subclassification and Clinicopathological Features of Intrahepatic Cholangiocarcinoma. International Journal of Molecular Sciences. 2018; 19(4):1004. https://doi.org/10.3390/ijms19041004
Chicago/Turabian StyleSoejima, Yurie, Miho Takeuchi, Takumi Akashi, Motoji Sawabe, and Toshio Fukusato. 2018. "β4 and β6 Integrin Expression Is Associated with the Subclassification and Clinicopathological Features of Intrahepatic Cholangiocarcinoma" International Journal of Molecular Sciences 19, no. 4: 1004. https://doi.org/10.3390/ijms19041004
APA StyleSoejima, Y., Takeuchi, M., Akashi, T., Sawabe, M., & Fukusato, T. (2018). β4 and β6 Integrin Expression Is Associated with the Subclassification and Clinicopathological Features of Intrahepatic Cholangiocarcinoma. International Journal of Molecular Sciences, 19(4), 1004. https://doi.org/10.3390/ijms19041004