BNP as a Major Player in the Heart-Kidney Connection

Abstract
:1. Introduction
2. Biochemical Characteristics of BNP
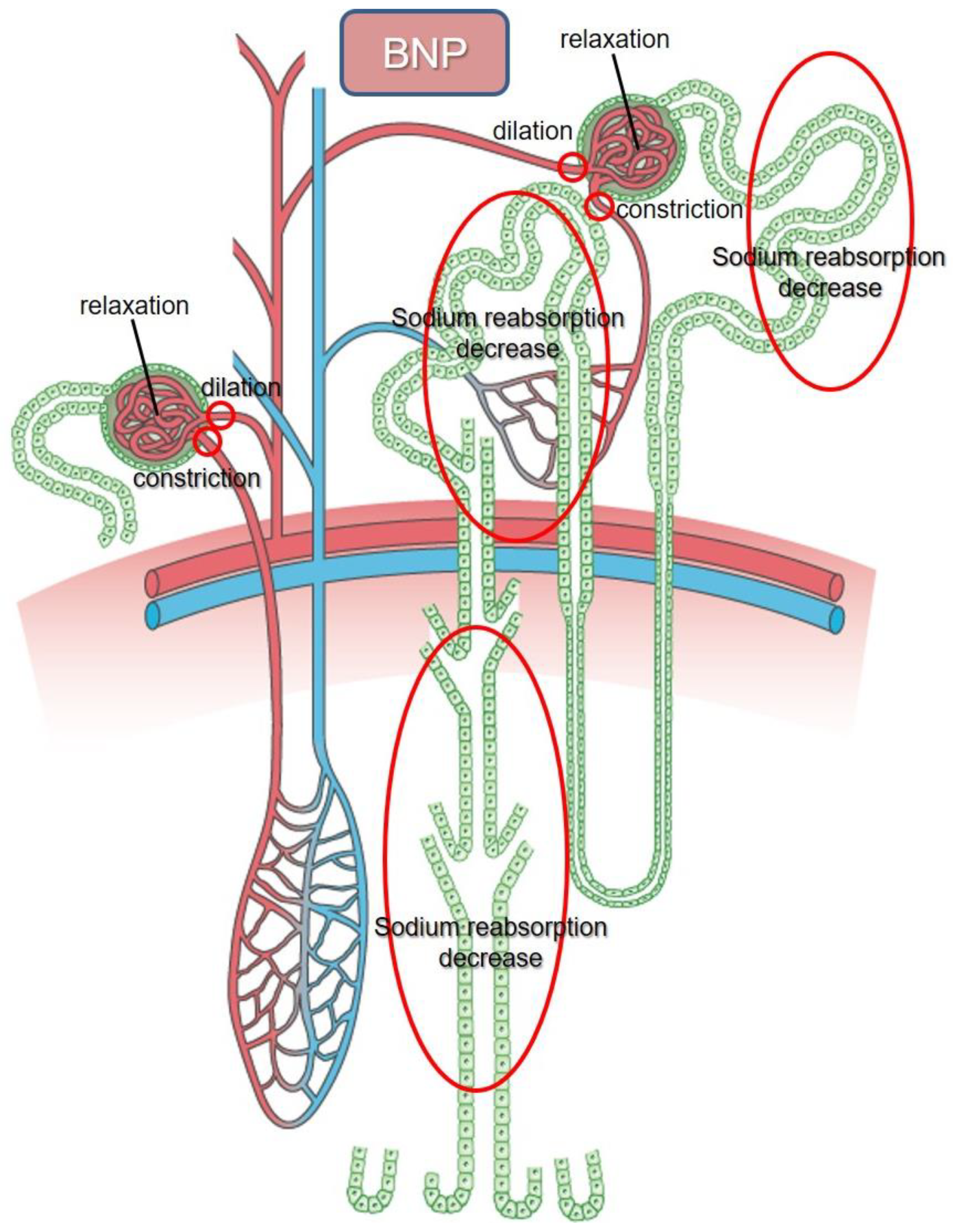
3. The Function of BNP in Kidneys
4. BNP Clearance from Kidneys
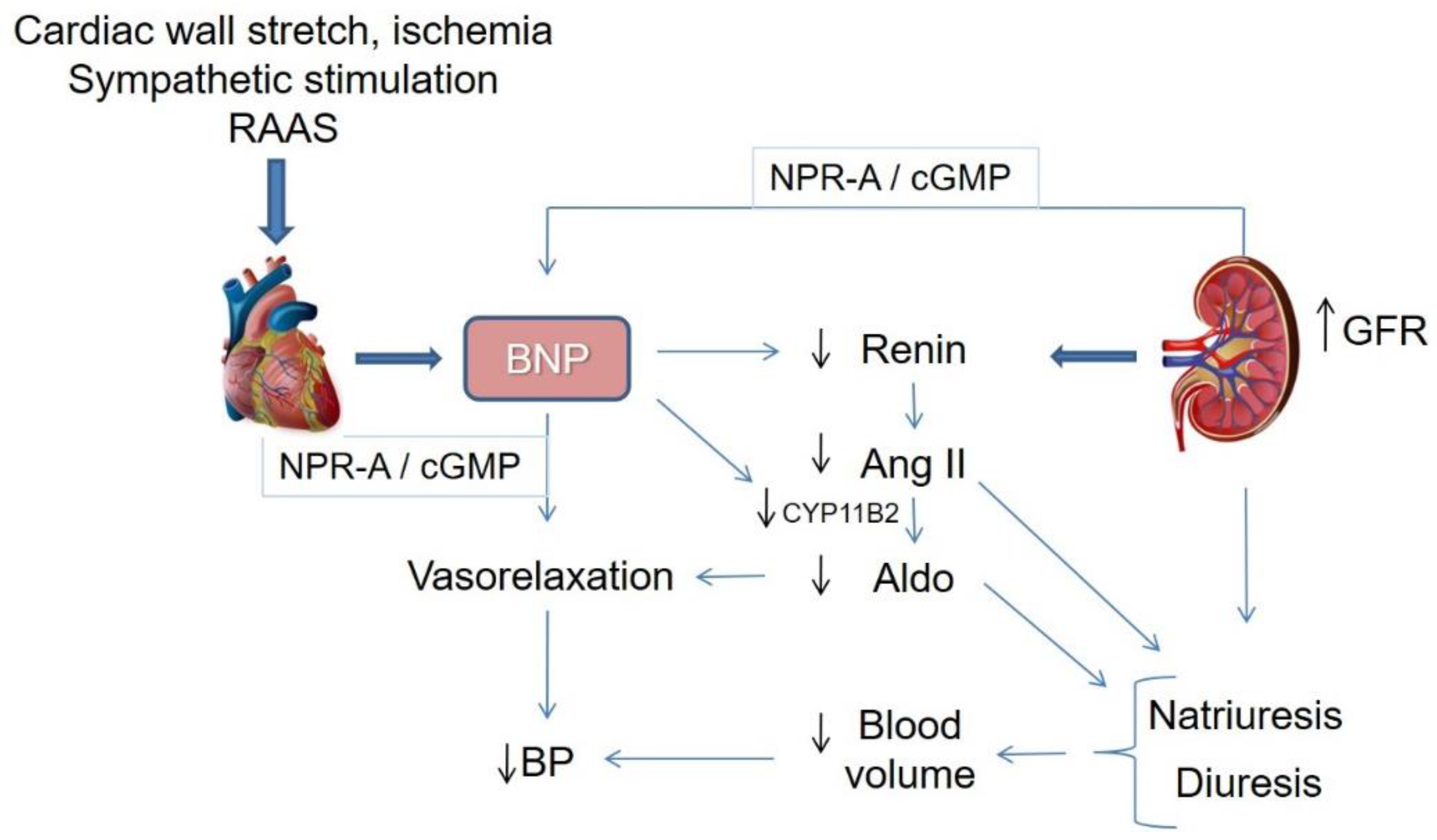
5. BNP System vs. RAA System
6. NPs Augmentation Combined with RAAS Blockade: Dual-Acting Angiotensin-Receptor/Neprilysin Inhibitors (ARNi)
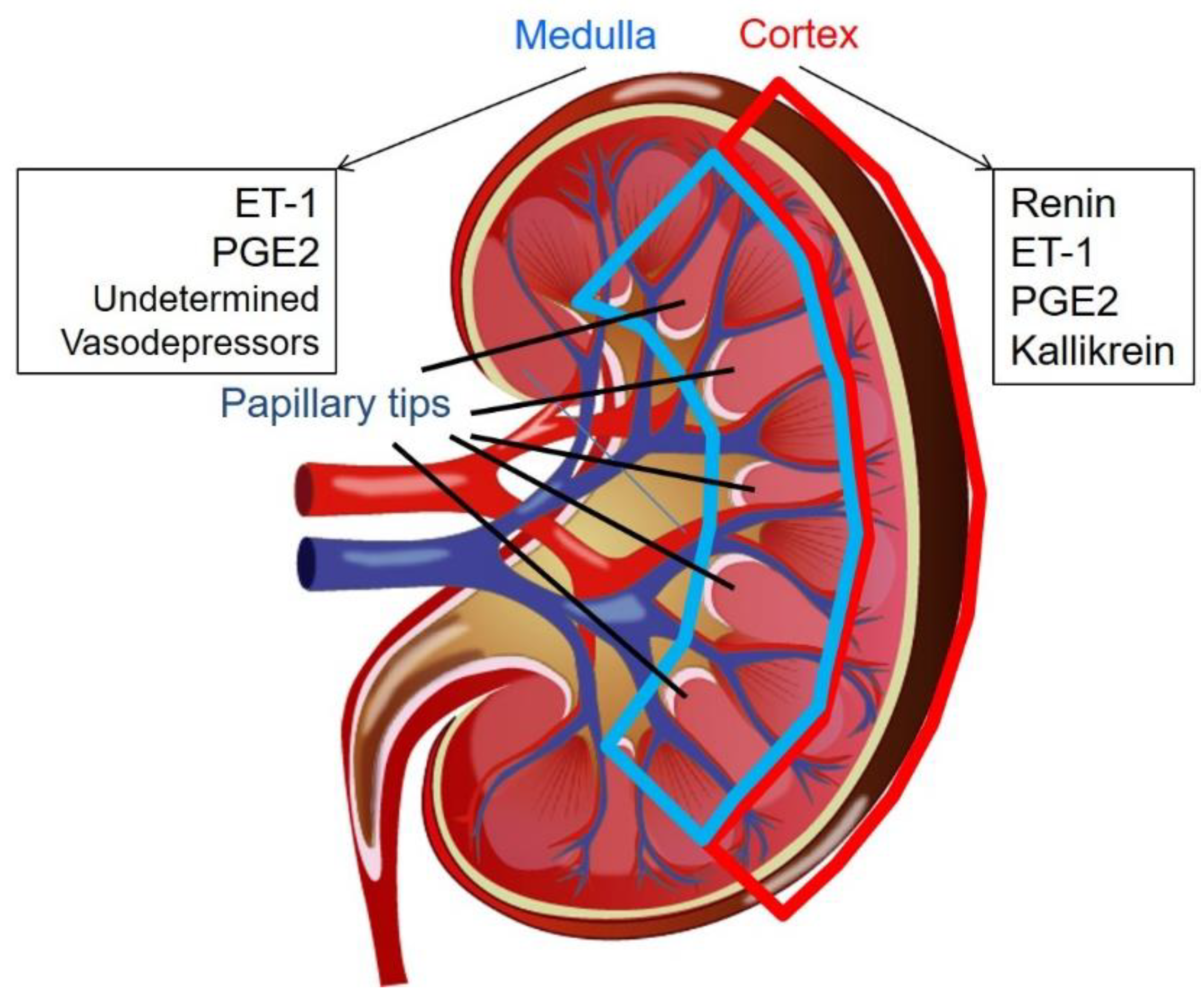
7. Vasopressor and Vasodepressor Derived from Kidneys
8. Renal Papillary Tip May Contribute to the Expression of BNP in Cardiomyocytes
9. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ANP | atrial natriuretic peptide |
| BNP | brain natriuretic peptide |
| cGMP | cyclic guanosine monophosphate |
| CHF | congestive heart failure |
| CKD | chronic kidney disease |
| CRS | cardiorenal syndrome |
| GFR | glomerular filtration rate |
| NP | natriuretic peptide |
| NPR | natriuretic peptide receptor |
| RAAS | renin-angiotensin-aldosterone system |
| RMIC | renal medullary interstitial cell |
| RPF | renal plasma flow |
| SNS | sympathetic nervous system |
References
- Sudoh, T.; Kangawa, K.; Minamino, N.; Matsuo, H. A new natriuretic peptide in porcine brain. Nature 1988, 332, 78–81. [Google Scholar] [CrossRef] [PubMed]
- LaPointe, M.C. Molecular regulation of the brain natriuretic peptide gene. Peptides 2005, 26, 944–956. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M. Natriuretic peptides and cardio-renal disease. Int. J. Cardiol. 2014, 176, 630–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatine, M.S.; Morrow, D.A.; de Lemos, J.A.; Omland, T.; Desai, M.Y.; Tanasijevic, M.; Hall, C.; McCabe, C.H.; Braunwald, E. Acute changes in circulating natriuretic peptide levels in relation to myocardial ischemia. J. Am. Coll. Cardiol. 2004, 44, 1988–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, K.T.; Eiskjaer, H.; Carstens, J.; Pedersen, E.B. Renal effects of brain natriuretic peptide in patients with congestive heart failure. Clin. Sci. 1999, 96, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikimi, T.; Kuwahara, K.; Nakao, K. Current biochemistry, molecular biology, and clinical relevance of natriuretic peptides. J. Cardiol. 2011, 57, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Levin, E.R.; Gardner, D.G.; Samson, W.K. Natriuretic peptides. N. Engl. J. Med. 1998, 339, 321–328. [Google Scholar]
- Brunner-La Rocca, H.P.; Kaye, D.M.; Woods, R.L.; Hastings, J.; Esler, M.D. Effects of intravenous brain natriuretic peptide on regional sympathetic activity in patients with chronic heart failure as compared with healthy control subjects. J. Am. Coll. Cardiol. 2001, 37, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Holmes, S.J.; Espiner, E.A.; Richards, A.M.; Yandle, T.G.; Frampton, C. Renal, endocrine, and hemodynamic effects of human brain natriuretic peptide in normal man. J. Clin. Endocrinol. Metab. 1993, 76, 91–96. [Google Scholar]
- Kohno, M.; Yokokawa, K.; Horio, T.; Yasunari, K.; Murakawa, K.; Takeda, T. Atrial and brain natriuretic peptides inhibit the endothelin-1 secretory response to angiotensin II in porcine aorta. Circ. Res. 1992, 70, 241–247. [Google Scholar] [CrossRef]
- De Arriba, G.; Barrio, V.; Olivera, A.; Rodriguez-Puyol, D.; Lopez-Novoa, J.M. Atrial natriuretic peptide inhibits angiotensin II-induced contraction of isolated glomeruli and cultured glomerular mesangial cells of rats: The role of calcium. J. Lab. Clin. Med. 1988, 111, 466–474. [Google Scholar] [PubMed]
- Ballermann, B.J.; Hoover, R.L.; Karnovsky, M.J.; Brenner, B.M. Physiologic regulation of atrial natriuretic peptide receptors in rat renal glomeruli. J. Clin. Investig. 1985, 76, 2049–2056. [Google Scholar] [CrossRef] [PubMed]
- Houben, A.J.; van der Zander, K.; de Leeuw, P.W. Vascular and renal actions of brain natriuretic peptide in man: Physiology and pharmacology. Fundam. Clin. Pharmacol. 2005, 19, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Doust, J.; Lehman, R.; Glasziou, P. The role of BNP testing in heart failure. Am. Fam. Physician 2006, 74, 1893–1898. [Google Scholar] [PubMed]
- Brenner, B.M.; Ballermann, B.J.; Gunning, M.E.; Zeidel, M.L. Diverse biological actions of atrial natriuretic peptide. Physiol. Rev. 1990, 70, 665–699. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.T.; Richards, A.M. Cardiac natriuretic peptides for cardiac health. Clin. Sci. 2005, 108, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Semenov, A.G.; Katrukha, A.G. Analytical Issues with Natriuretic Peptides—Has this been Overly Simplified? EJIFCC 2016, 27, 189–207. [Google Scholar]
- Kitakaze, M.; Asakura, M.; Kim, J.; Shintani, Y.; Asanuma, H.; Hamasaki, T.; Seguchi, O.; Myoishi, M.; Minamino, T.; Ohara, T.; et al. Human atrial natriuretic peptide and nicorandil as adjuncts to reperfusion treatment for acute myocardial infarction (J-WIND): Two randomised trials. Lancet 2007, 370, 1483–1493. [Google Scholar] [CrossRef]
- Spanaus, K.S.; Kronenberg, F.; Ritz, E.; Schlapbach, R.; Fliser, D.; Hersberger, M.; Kollerits, B.; Konig, P.; von Eckardstein, A. B-type natriuretic peptide concentrations predict the progression of nondiabetic chronic kidney disease: The Mild-to-Moderate Kidney Disease Study. Clin. Chem. 2007, 53, 1264–1272. [Google Scholar] [CrossRef]
- Van Kimmenade, R.R.; Januzzi, J.L., Jr.; Bakker, J.A.; Houben, A.J.; Rennenberg, R.; Kroon, A.A.; Crijns, H.J.; van Dieijen-Visser, M.P.; de Leeuw, P.W.; Pinto, Y.M. Renal clearance of B-type natriuretic peptide and amino terminal pro-B-type natriuretic peptide a mechanistic study in hypertensive subjects. J. Am. Coll. Cardiol. 2009, 53, 884–890. [Google Scholar] [CrossRef]
- Takase, H.; Dohi, Y. Kidney function crucially affects B-type natriuretic peptide (BNP), N-terminal proBNP and their relationship. Eur. J. Clin. Investig. 2014, 44, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Niizuma, S.; Iwanaga, Y.; Yahata, T.; Miyazaki, S. Renocardiovascular Biomarkers: From the Perspective of Managing Chronic Kidney Disease and Cardiovascular Disease. Front. Cardiovasc. Med. 2017, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis, D.; Fraticelli, L.; Bassand, A.; Manzo-Silberman, S.; Peschanski, N.; Charpentier, S.; Elbaz, M.; Savary, D.; Bonnefoy-Cudraz, E.; Laribi, S.; et al. Impact of renal dysfunction on the management and outcome of acute heart failure: Results from the French prospective, multicentre, DeFSSICA survey. BMJ Open 2019, 9, e022776. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Carnovali, M.; Mastromarino, V. The natriuretic peptides system in the pathophysiology of heart failure: From molecular basis to treatment. Clin. Sci. 2016, 130, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Goto, I.; Okamoto, R.; Hashizume, R.; Suzuki, N.; Ito, R.; Yamanaka, K.; Saito, H.; Kiyonari, H.; Tawara, I.; Kageyama, Y.; et al. Renal papillary tip extract stimulates BNP production and excretion from cardiomyocytes. PLoS ONE 2018, 13, e0197078. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Passino, C.; Franzini, M.; Emdin, M. Cardiac biomarker testing in the clinical laboratory: Where do we stand? General overview of the methodology with special emphasis on natriuretic peptides. Clin. Chim. Acta 2015, 443, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Waldo, S.W.; Beede, J.; Isakson, S.; Villard-Saussine, S.; Fareh, J.; Clopton, P.; Fitzgerald, R.L.; Maisel, A.S. Pro-B-type natriuretic peptide levels in acute decompensated heart failure. J. Am. Coll. Cardiol. 2008, 51, 1874–1882. [Google Scholar] [CrossRef]
- Santaguida, P.L.; Don-Wauchope, A.C.; Oremus, M.; McKelvie, R.; Ali, U.; Hill, S.A.; Balion, C.; Booth, R.A.; Brown, J.A.; Bustamam, A.; et al. BNP and NT-proBNP as prognostic markers in persons with acute decompensated heart failure: A systematic review. Heart Fail. Rev. 2014, 19, 453–470. [Google Scholar] [CrossRef]
- Mueller, T.; Gegenhuber, A.; Poelz, W.; Haltmayer, M. Head-to-head comparison of the diagnostic utility of BNP and NT-proBNP in symptomatic and asymptomatic structural heart disease. Clin. Chim. Acta 2004, 341, 41–48. [Google Scholar] [CrossRef]
- Clerico, A.; Zaninotto, M.; Passino, C.; Plebani, M. New issues on measurement of B-type natriuretic peptides. Clin. Chem. Lab. Med. 2017, 56, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Kuwahara, K.; Nakagawa, Y.; Nishikimi, T. Cutting Edge of Brain Natriuretic Peptide (BNP) Research- The Diversity of BNP Immunoreactivity and Its Clinical Relevance. Circ. J. 2018, 82, 2455–2461. [Google Scholar] [CrossRef] [PubMed]
- Rubattu, S.; Forte, M.; Marchitti, S.; Volpe, M. Molecular Implications of Natriuretic Peptides in the Protection from Hypertension and Target Organ Damage Development. Int. J. Mol. Sci. 2019, 20, 798. [Google Scholar] [CrossRef] [PubMed]
- Santos-Araujo, C.; Leite-Moreira, A.; Pestana, M. Clinical value of natriuretic peptides in chronic kidney disease. Nefrologia 2015, 35, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Vanderheyden, M.; Bartunek, J.; Filippatos, G.; Goethals, M.; Vlem, B.V.; Maisel, A. Cardiovascular disease in patients with chronic renal impairment: Role of natriuretic peptides. Congest. Heart Fail. 2008, 14, 38–42. [Google Scholar] [CrossRef]
- Jensen, K.T.; Carstens, J.; Pedersen, E.B. Effect of BNP on renal hemodynamics, tubular function and vasoactive hormones in humans. Am. J. Physiol. 1998, 274, F63–F72. [Google Scholar] [CrossRef] [PubMed]
- McGregor, A.; Richards, M.; Espiner, E.; Yandle, T.; Ikram, H. Brain natriuretic peptide administered to man: Actions and metabolism. J. Clin. Endocrinol. Metab. 1990, 70, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, M.; Yasue, H.; Morita, E.; Sakaino, N.; Jougasaki, M.; Kurose, M.; Mukoyama, M.; Saito, Y.; Nakao, K.; Imura, H. Hemodynamic, renal, and hormonal responses to brain natriuretic peptide infusion in patients with congestive heart failure. Circulation 1991, 84, 1581–1588. [Google Scholar] [CrossRef]
- Cheung, B.M.; Dickerson, J.E.; Ashby, M.J.; Brown, M.J.; Brown, J. Effects of physiological increments in human alpha-atrial natriuretic peptide and human brain natriuretic peptide in normal male subjects. Clin. Sci. 1994, 86, 723–730. [Google Scholar] [CrossRef]
- Florkowski, C.M.; Richards, A.M.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Renal, endocrine, and hemodynamic interactions of atrial and brain natriuretic peptides in normal men. Am. J. Physiol. 1994, 266, R1244–R1250. [Google Scholar] [CrossRef]
- La Villa, G.; Fronzaroli, C.; Lazzeri, C.; Porciani, C.; Bandinelli, R.; Vena, S.; Messeri, G.; Franchi, F. Cardiovascular and renal effects of low dose brain natriuretic peptide infusion in man. J. Clin. Endocrinol. Metab. 1994, 78, 1166–1171. [Google Scholar]
- La Villa, G.; Stefani, L.; Lazzeri, C.; Zurli, C.; Guerra, C.T.; Barletta, G.; Bandinelli, R.; Strazzulla, G.; Franchi, F. Acute effects of physiological increments of brain natriuretic peptide in humans. Hypertension 1995, 26, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, C.; La Villa, G.; Bisi, G.; Boddi, V.; Messeri, G.; Strazzulla, G.; Franchi, F. Cardiovascular function during brain natriuretic peptide infusion in man. Cardiology 1995, 86, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Hunt, P.J.; Espiner, E.A.; Nicholls, M.G.; Richards, A.M.; Yandle, T.G. Differing biological effects of equimolar atrial and brain natriuretic peptide infusions in normal man. J. Clin. Endocrinol. Metab. 1996, 81, 3871–3876. [Google Scholar] [PubMed]
- Yasue, H.; Yoshimura, M. Natriuretic peptides in the treatment of heart failure. J. Card. Fail. 1996, 2, S277–S285. [Google Scholar] [CrossRef]
- Van der Zander, K.; Houben, A.J.; Hofstra, L.; Kroon, A.A.; de Leeuw, P.W. Hemodynamic and renal effects of low-dose brain natriuretic peptide infusion in humans: A randomized, placebo-controlled crossover study. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H1206–H1212. [Google Scholar] [CrossRef] [PubMed]
- Marcus, L.S.; Hart, D.; Packer, M.; Yushak, M.; Medina, N.; Danziger, R.S.; Heitjan, D.F.; Katz, S.D. Hemodynamic and renal excretory effects of human brain natriuretic peptide infusion in patients with congestive heart failure. A double-blind, placebo-controlled, randomized crossover trial. Circulation 1996, 94, 3184–3189. [Google Scholar] [CrossRef] [PubMed]
- Lainchbury, J.G.; Richards, A.M.; Nicholls, M.G.; Hunt, P.J.; Ikram, H.; Espiner, E.A.; Yandle, T.G.; Begg, E. The effects of pathophysiological increments in brain natriuretic peptide in left ventricular systolic dysfunction. Hypertension 1997, 30, 398–404. [Google Scholar] [CrossRef]
- Abraham, W.T.; Lowes, B.D.; Ferguson, D.A.; Odom, J.; Kim, J.K.; Robertson, A.D.; Bristow, M.R.; Schrier, R.W. Systemic hemodynamic, neurohormonal, and renal effects of a steady-state infusion of human brain natriuretic peptide in patients with hemodynamically decompensated heart failure. J. Card. Fail. 1998, 4, 37–44. [Google Scholar] [CrossRef]
- Wang, Y.; Gu, X.; Fan, W.; Fan, Y.; Li, W.; Fu, X. Effects of recombinant human brain natriuretic peptide on renal function in patients with acute heart failure following myocardial infarction. Am. J. Transl. Res. 2016, 8, 239–245. [Google Scholar]
- Richards, A.M.; Crozier, I.G.; Holmes, S.J.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Brain natriuretic peptide: Natriuretic and endocrine effects in essential hypertension. J. Hypertens. 1993, 11, 163–170. [Google Scholar] [CrossRef]
- Lazzeri, C.; Franchi, F.; Porciani, C.; Fronzaroli, C.; Casini Raggi, V.; De Feo, M.L.; Mannelli, M.; Cersosimo, R.M.; La Villa, G. Systemic hemodynamics and renal function during brain natriuretic peptide infusion in patients with essential hypertension. Am. J. Hypertens. 1995, 8, 799–807. [Google Scholar] [CrossRef]
- Pidgeon, G.B.; Richards, A.M.; Nicholls, M.G.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Differing metabolism and bioactivity of atrial and brain natriuretic peptides in essential hypertension. Hypertension 1996, 27, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Kamper, A.L.; Holstein-Rathlou, N.H.; Leyssac, P.P.; Strandgaard, S. Lithium clearance in chronic nephropathy. Clin. Sci. 1989, 77, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Totsune, K.; Takahashi, K.; Murakami, O.; Satoh, F.; Sone, M.; Saito, T.; Sasano, H.; Mouri, T.; Abe, K. Natriuretic peptides in the human kidney. Hypertension 1994, 24, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, S.S.; Stebbins, A.; Voors, A.A.; Hasselblad, V.; Ezekowitz, J.A.; Califf, R.M.; O’Connor, C.M.; Starling, R.C.; Hernandez, A.F. Effects of nesiritide and predictors of urine output in acute decompensated heart failure: Results from ASCEND-HF (acute study of clinical effectiveness of nesiritide and decompensated heart failure). J. Am. Coll. Cardiol. 2013, 62, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Kelesidis, I.; Mazurek, J.; Khullar, P.; Saeed, W.; Vittorio, T.; Zolty, R. The effect of nesiritide on renal function and other clinical parameters in patients with decompensated heart failure and preserved ejection fraction. Congest. Heart Fail. 2012, 18, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Fontoura, B.M.; Nussenzveig, D.R.; Pelton, K.M.; Maack, T. Atrial natriuretic factor receptors in cultured renomedullary interstitial cells. Am. J. Physiol. 1990, 258, C692–C699. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, F.H.; Dupont, M.; Steels, P.; Grieten, L.; Swennen, Q.; Tang, W.H.; Mullens, W. The kidney in congestive heart failure: ‘Are natriuresis, sodium, and diuretics really the good, the bad and the ugly?’. Eur. J. Heart Fail. 2014, 16, 133–142. [Google Scholar] [CrossRef]
- Cataliotti, A.; Boerrigter, G.; Costello-Boerrigter, L.C.; Schirger, J.A.; Tsuruda, T.; Heublein, D.M.; Chen, H.H.; Malatino, L.S.; Burnett, J.C., Jr. Brain natriuretic peptide enhances renal actions of furosemide and suppresses furosemide-induced aldosterone activation in experimental heart failure. Circulation 2004, 109, 1680–1685. [Google Scholar] [CrossRef]
- McKie, P.M.; Schirger, J.A.; Benike, S.L.; Harstad, L.K.; Slusser, J.P.; Hodge, D.O.; Redfield, M.M.; Burnett, J.C., Jr.; Chen, H.H. Chronic subcutaneous brain natriuretic peptide therapy in asymptomatic systolic heart failure. Eur. J. Heart Fail. 2016, 18, 433–441. [Google Scholar] [CrossRef]
- Liu, J.; Xie, Y.; He, F.; Gao, Z.; Hao, Y.; Zu, X.; Chang, L.; Li, Y. Recombinant Brain Natriuretic Peptide for the Prevention of Contrast-Induced Nephropathy in Patients with Chronic Kidney Disease Undergoing Nonemergent Percutaneous Coronary Intervention or Coronary Angiography: A Randomized Controlled Trial. Biomed Res. Int. 2016, 2016, 5985327. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.L.; Jones, M.J. Atrial, B-type, and C-type natriuretic peptides cause mesenteric vasoconstriction in conscious dogs. Am. J. Physiol. 1999, 276, R1443–R1452. [Google Scholar] [CrossRef] [PubMed]
- Marin-Grez, M.; Fleming, J.T.; Steinhausen, M. Atrial natriuretic peptide causes pre-glomerular vasodilatation and post-glomerular vasoconstriction in rat kidney. Nature 1986, 324, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Santos-Araujo, C.; Roncon-Albuquerque, R., Jr.; Moreira-Rodrigues, M.; Henriques-Coelho, T.; Quelhas-Santos, J.; Faria, B.; Sampaio-Maia, B.; Leite-Moreira, A.F.; Pestana, M. Local modulation of the natriuretic peptide system in the rat remnant kidney. Nephrol. Dial. Transplant. 2009, 24, 1774–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sackner-Bernstein, J.D.; Skopicki, H.A.; Aaronson, K.D. Risk of worsening renal function with nesiritide in patients with acutely decompensated heart failure. Circulation 2005, 111, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Anand-Srivastava, M.B. Natriuretic peptide receptor-C signaling and regulation. Peptides 2005, 26, 1044–1059. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.G.; Arfsten, A.; Fuller, F.; Miller, J.A.; Gregory, L.C.; Lewicki, J.A. Isolation and functional expression of the human atrial natriuretic peptide clearance receptor cDNA. Biochem. Biophys. Res. Commun. 1990, 171, 796–803. [Google Scholar] [CrossRef]
- Wilcox, J.N.; Augustine, A.; Goeddel, D.V.; Lowe, D.G. Differential regional expression of three natriuretic peptide receptor genes within primate tissues. Mol. Cell. Biol. 1991, 11, 3454–3462. [Google Scholar] [CrossRef]
- He, X.; Chow, D.; Martick, M.M.; Garcia, K.C. Allosteric activation of a spring-loaded natriuretic peptide receptor dimer by hormone. Science 2001, 293, 1657–1662. [Google Scholar] [CrossRef]
- Jalal, F.; Dehbi, M.; Berteloot, A.; Crine, P. Biosynthesis and polarized distribution of neutral endopeptidase in primary cultures of kidney proximal tubule cells. Biochem. J. 1994, 302, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Dickey, D.M.; Potter, L.R. Human B-type natriuretic peptide is not degraded by meprin A. Biochem. Pharmacol. 2010, 80, 1007–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.W.; Espiner, E.A.; Yandle, T.G.; Charles, C.J.; Richards, A.M. Delayed metabolism of human brain natriuretic peptide reflects resistance to neutral endopeptidase. J. Endocrinol. 2000, 167, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralat, L.A.; Guo, Q.; Ren, M.; Funke, T.; Dickey, D.M.; Potter, L.R.; Tang, W.J. Insulin-degrading enzyme modulates the natriuretic peptide-mediated signaling response. J. Biol. Chem. 2011, 286, 4670–4679. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.; Ping, P.; Wang, F.; Luo, L. Synthesis, secretion, function, metabolism and application of natriuretic peptides in heart failure. J. Biol. Eng. 2018, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Linssen, G.C.; Damman, K.; Hillege, H.L.; Navis, G.; van Veldhuisen, D.J.; Voors, A.A. Urinary N-terminal prohormone brain natriuretic peptide excretion in patients with chronic heart failure. Circulation 2009, 120, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Jungbauer, C.G.; Buchner, S.; Birner, C.; Resch, M.; Heinicke, N.; Debl, K.; Buesing, M.; Biermeier, D.; Schmitz, G.; Riegger, G.; et al. N-terminal pro-brain natriuretic peptide from fresh urine for the biochemical detection of heart failure and left ventricular dysfunction. Eur. J. Heart Fail. 2010, 12, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, P.C.; Guo, J.; Zhang, A. The renal and cardiovascular effects of natriuretic peptides. Adv. Physiol. Educ. 2017, 41, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Volpe, M.; Battistoni, A.; Mastromarino, V. Natriuretic peptides and volume handling in heart failure: The paradigm of a new treatment. Eur. J. Heart Fail. 2016, 18, 442–444. [Google Scholar] [CrossRef]
- Von Lueder, T.G.; Sangaralingham, S.J.; Wang, B.H.; Kompa, A.R.; Atar, D.; Burnett, J.C., Jr.; Krum, H. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: Novel therapeutic concepts to combat heart failure. Circ. Heart Fail. 2013, 6, 594–605. [Google Scholar] [CrossRef]
- Corti, R.; Burnett, J.C., Jr.; Rouleau, J.L.; Ruschitzka, F.; Luscher, T.F. Vasopeptidase inhibitors: A new therapeutic concept in cardiovascular disease? Circulation 2001, 104, 1856–1862. [Google Scholar] [CrossRef]
- Tokudome, T.; Kishimoto, I.; Horio, T.; Arai, Y.; Schwenke, D.O.; Hino, J.; Okano, I.; Kawano, Y.; Kohno, M.; Miyazato, M.; et al. Regulator of G-protein signaling subtype 4 mediates antihypertrophic effect of locally secreted natriuretic peptides in the heart. Circulation 2008, 117, 2329–2339. [Google Scholar] [CrossRef] [PubMed]
- Akabane, S.; Matsushima, Y.; Matsuo, H.; Kawamura, M.; Imanishi, M.; Omae, T. Effects of brain natriuretic peptide on renin secretion in normal and hypertonic saline-infused kidney. Eur. J. Pharmacol. 1991, 198, 143–148. [Google Scholar] [CrossRef]
- Kurtz, A.; Della Bruna, R.; Pfeilschifter, J.; Taugner, R.; Bauer, C. Atrial natriuretic peptide inhibits renin release from juxtaglomerular cells by a cGMP-mediated process. Proc. Natl. Acad. Sci. USA 1986, 83, 4769–4773. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Yoshimura, M.; Nakamura, S.; Nakayama, M.; Shimasaki, Y.; Harada, E.; Mizuno, Y.; Yamamuro, M.; Harada, M.; Saito, Y.; et al. Inhibitory effect of natriuretic peptides on aldosterone synthase gene expression in cultured neonatal rat cardiocytes. Circulation 2003, 107, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Kapoun, A.M.; Lam, A.; Damm, D.L.; Quan, D.; O’Connell, M.; Protter, A.A. B-Type natriuretic peptide inhibited angiotensin II-stimulated cholesterol biosynthesis, cholesterol transfer, and steroidogenesis in primary human adrenocortical cells. Endocrinology 2007, 148, 3722–3729. [Google Scholar] [CrossRef] [PubMed]
- Takekoshi, K.; Ishii, K.; Isobe, K.; Nomura, F.; Nammoku, T.; Nakai, T. Effects of natriuretic peptides (ANP, BNP, CNP) on catecholamine synthesis and TH mRNA levels in PC12 cells. Life Sci. 2000, 66, PL303–PL311. [Google Scholar] [CrossRef]
- Han, B.; Hasin, Y. Cardiovascular effects of natriuretic peptides and their interrelation with endothelin-1. Cardiovasc. Drugs Ther. 2003, 17, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.I.; Hodsman, P.G.; Kohzuki, M.; Casley, D.J.; Fabris, B.; Phillips, P.A. Interaction between atrial natriuretic peptide and the renin angiotensin aldosterone system. Endogenous antagonists. Am. J. Med. 1989, 87, 24S–28S. [Google Scholar] [PubMed]
- Rossi, F.; Mascolo, A.; Mollace, V. The pathophysiological role of natriuretic peptide-RAAS cross talk in heart failure. Int. J. Cardiol. 2017, 226, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, G.; Farmakis, D.; Parissis, J.; Lekakis, J. Drug therapy for patients with systolic heart failure after the PARADIGM-HF trial: In need of a new paradigm of LCZ696 implementation in clinical practice. BMC Med. 2015, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Bayes-Genis, A.; Barallat, J.; Galan, A.; de Antonio, M.; Domingo, M.; Zamora, E.; Urrutia, A.; Lupon, J. Soluble neprilysin is predictive of cardiovascular death and heart failure hospitalization in heart failure patients. J. Am. Coll. Cardiol. 2015, 65, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Colucci, W.S.; Elkayam, U.; Horton, D.P.; Abraham, W.T.; Bourge, R.C.; Johnson, A.D.; Wagoner, L.E.; Givertz, M.M.; Liang, C.S.; Neibaur, M.; et al. Intravenous nesiritide, a natriuretic peptide, in the treatment of decompensated congestive heart failure. Nesiritide Study Group. N. Engl. J. Med. 2000, 343, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Partovian, C.; Li, S.X.; Xu, X.; Lin, H.; Strait, K.M.; Hwa, J.; Krumholz, H.M. Patterns of change in nesiritide use in patients with heart failure: How hospitals react to new information. JACC Heart Fail. 2013, 1, 318–324. [Google Scholar] [CrossRef]
- Kostis, J.B.; Packer, M.; Black, H.R.; Schmieder, R.; Henry, D.; Levy, E. Omapatrilat and enalapril in patients with hypertension: The Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am. J. Hypertens. 2004, 17, 103–111. [Google Scholar] [CrossRef] [PubMed]
- McCormack, P.L. Sacubitril/Valsartan: A Review in Chronic Heart Failure with Reduced Ejection Fraction. Drugs 2016, 76, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Rubattu, S.; Battistoni, A. ARNi: A Novel Approach to Counteract Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 2092. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. The path to an angiotensin receptor antagonist-neprilysin inhibitor in the treatment of heart failure. J. Am. Coll. Cardiol. 2015, 65, 1029–1041. [Google Scholar] [CrossRef]
- Roksnoer, L.C.; van Veghel, R.; van Groningen, M.C.; de Vries, R.; Garrelds, I.M.; Bhaggoe, U.M.; van Gool, J.M.; Friesema, E.C.; Leijten, F.P.; Hoorn, E.J.; et al. Blood pressure-independent renoprotection in diabetic rats treated with AT1 receptor-neprilysin inhibition compared with AT1 receptor blockade alone. Clin. Sci. 2016, 130, 1209–1220. [Google Scholar] [CrossRef]
- Von Lueder, T.G.; Wang, B.H.; Kompa, A.R.; Huang, L.; Webb, R.; Jordaan, P.; Atar, D.; Krum, H. Angiotensin receptor neprilysin inhibitor LCZ696 attenuates cardiac remodeling and dysfunction after myocardial infarction by reducing cardiac fibrosis and hypertrophy. Circ. Heart Fail. 2015, 8, 71–78. [Google Scholar] [CrossRef]
- Haynes, R.; Judge, P.K.; Staplin, N.; Herrington, W.G.; Storey, B.C.; Bethel, A.; Bowman, L.; Brunskill, N.; Cockwell, P.; Hill, M.; et al. Effects of Sacubitril/Valsartan Versus Irbesartan in Patients With Chronic Kidney Disease. Circulation 2018, 138, 1505–1514. [Google Scholar] [CrossRef]
- Ruilope, L.M.; Dukat, A.; Bohm, M.; Lacourciere, Y.; Gong, J.; Lefkowitz, M.P. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: A randomised, double-blind, placebo-controlled, active comparator study. Lancet 2010, 375, 1255–1266. [Google Scholar] [CrossRef]
- Solomon, S.D.; Zile, M.; Pieske, B.; Voors, A.; Shah, A.; Kraigher-Krainer, E.; Shi, V.; Bransford, T.; Takeuchi, M.; Gong, J.; et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: A phase 2 double-blind randomised controlled trial. Lancet 2012, 380, 1387–1395. [Google Scholar] [CrossRef]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Miller, R.; Solomon, S.D. Combined neprilysin and renin-angiotensin system inhibition for the treatment of heart failure. JACC Heart Fail. 2014, 2, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; McMurray, J.J.; Packer, M.; Swedberg, K.; Rouleau, J.L.; Chen, F.; Gong, J.; Rizkala, A.R.; Brahimi, A.; Claggett, B.; et al. Effect of the angiotensin-receptor-neprilysin inhibitor LCZ696 compared with enalapril on mode of death in heart failure patients. Eur. Heart J. 2015, 36, 1990–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; McMurray, J.J.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015, 131, 54–61. [Google Scholar] [CrossRef]
- Voors, A.A.; Gori, M.; Liu, L.C.; Claggett, B.; Zile, M.R.; Pieske, B.; McMurray, J.J.; Packer, M.; Shi, V.; Lefkowitz, M.P.; et al. Renal effects of the angiotensin receptor neprilysin inhibitor LCZ696 in patients with heart failure and preserved ejection fraction. Eur. J. Heart Fail. 2015, 17, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Ishii, M.; Kaikita, K.; Sato, K.; Sueta, D.; Fujisue, K.; Arima, Y.; Oimatsu, Y.; Mitsuse, T.; Onoue, Y.; Araki, S.; et al. Cardioprotective Effects of LCZ696 (Sacubitril/Valsartan) After Experimental Acute Myocardial Infarction. JACC Basic Transl. Sci. 2017, 2, 655–668. [Google Scholar] [CrossRef]
- Campbell, D.J.; Krum, H.; Esler, M.D. Losartan increases bradykinin levels in hypertensive humans. Circulation 2005, 111, 315–320. [Google Scholar] [CrossRef]
- Grimm, M.O.; Mett, J.; Stahlmann, C.P.; Haupenthal, V.J.; Zimmer, V.C.; Hartmann, T. Neprilysin and Abeta Clearance: Impact of the APP Intracellular Domain in NEP Regulation and Implications in Alzheimer’s Disease. Front. Aging Neurosci. 2013, 5, 98. [Google Scholar] [CrossRef]
- Kuwahara, M.; Marumo, F. Biosynthesis of hormones in renal tubular and interstitial cells. Nihon Rinsho 1995, 53, 1873–1878. [Google Scholar] [PubMed]
- Marks, L.S.; Maxwell, M.H. Tigerstedt and the discovery of renin. An historical note. Hypertension 1979, 1, 384–388. [Google Scholar] [CrossRef] [PubMed]
- De Miguel, C.; Speed, J.S.; Kasztan, M.; Gohar, E.Y.; Pollock, D.M. Endothelin-1 and the kidney: New perspectives and recent findings. Curr. Opin. Nephrol. Hypertens. 2016, 25, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Boesen, E.I. Endothelin receptors, renal effects and blood pressure. Curr. Opin. Pharmacol. 2015, 21, 25–34. [Google Scholar] [CrossRef]
- Nasrallah, R.; Hassouneh, R.; Hebert, R.L. PGE2, Kidney Disease, and Cardiovascular Risk: Beyond Hypertension and Diabetes. J. Am. Soc. Nephrol. 2016, 27, 666–676. [Google Scholar] [CrossRef]
- Li, Y.; Xia, W.; Zhao, F.; Wen, Z.; Zhang, A.; Huang, S.; Jia, Z.; Zhang, Y. Prostaglandins in the pathogenesis of kidney diseases. Oncotarget 2018, 9, 26586–26602. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wei, Y.; Zheng, F.; Guan, Y.; Zhang, X. Prostaglandin E2 in the Regulation of Water Transport in Renal Collecting Ducts. Int. J. Mol. Sci. 2017, 18, 2539. [Google Scholar] [CrossRef]
- Tomita, K.; Endou, H.; Sakai, F. Localization of kallikrein-like activity along a single nephron in rabbits. Pflug. Arch. 1981, 389, 91–95. [Google Scholar] [CrossRef]
- Omata, K.; Carretero, O.A.; Scicli, A.G.; Jackson, B.A. Localization of active and inactive kallikrein (kininogenase activity) in the microdissected rabbit nephron. Kidney Int. 1982, 22, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Proud, D.; Perkins, M.; Pierce, J.V.; Yates, K.N.; Highet, P.F.; Herring, P.L.; Mangkornkanok/Mark, M.; Bahu, R.; Carone, F.; Pisano, J.J. Characterization and localization of human renal kininogen. J. Biol. Chem. 1981, 256, 10634–10639. [Google Scholar]
- Rhaleb, N.E.; Yang, X.P.; Carretero, O.A. The kallikrein-kinin system as a regulator of cardiovascular and renal function. Compr. Physiol. 2011, 1, 971–993. [Google Scholar] [PubMed]
- Kauker, M.L. Bradykinin action on the efflux of luminal 22Na in the rat nephron. J. Pharmacol. Exp. Ther. 1980, 214, 119–123. [Google Scholar] [PubMed]
- Sinaiko, A.R.; Glasser, R.J.; Gillum, R.F.; Prineas, R.J. Urinary kallikrein excretion in grade school children with high and low blood pressure. J. Pediatr. 1982, 100, 938–940. [Google Scholar] [CrossRef]
- Sharma, J.N.; Narayanan, P. The kallikrein-kinin pathways in hypertension and diabetes. Prog. Drug Res. 2014, 69, 15–36. [Google Scholar] [PubMed]
- Wollheim, E.; Peterknecht, S.; Dees, C.; Wiener, A.; Wollheim, C.B. Defect in the excretion of a vasoactive polypeptide fraction A possible genetic marker of primary hypertension. Hypertension 1981, 3, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.J.; Woods, R.L.; Evans, R.G.; Alcorn, D.; Christy, I.J.; Anderson, W.P. Evidence for a renomedullary vasodepressor hormone. Clin. Exp. Pharmacol. Physiol. 1996, 23, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Muirhead, E.E. Renal vasodepressor mechanisms: The medullipin system. J. Hypertens. Suppl. 1993, 11, S53–S58. [Google Scholar] [CrossRef] [PubMed]
- Maric, C.; Harris, P.J.; Alcorn, D. Changes in mean arterial pressure predict degranulation of renomedullary interstitial cells. Clin. Exp. Pharmacol. Physiol. 2002, 29, 1055–1059. [Google Scholar] [CrossRef]
- Glodny, B.; Pauli, G.F. The vasodepressor function of the kidney: Prostaglandin E2 is not the principal vasodepressor lipid of the renal medulla. Acta Physiol. 2006, 187, 419–430. [Google Scholar] [CrossRef]
- Pitcock, J.A.; Brown, P.S.; Byers, W.; Brooks, B.; Muirhead, E.E. Degranulation of renomedullary interstitial cells during reversal of hypertension. Hypertension 1981, 3, II-75. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Leip, E.P.; Benjamin, E.J.; Wilson, P.W.; Sutherland, P.; Omland, T.; Vasan, R.S. Impact of age and sex on plasma natriuretic peptide levels in healthy adults. Am. J. Cardiol. 2002, 90, 254–258. [Google Scholar] [CrossRef]
- Redfield, M.M.; Rodeheffer, R.J.; Jacobsen, S.J.; Mahoney, D.W.; Bailey, K.R.; Burnett, J.C., Jr. Plasma brain natriuretic peptide concentration: Impact of age and gender. J. Am. Coll. Cardiol. 2002, 40, 976–982. [Google Scholar] [CrossRef]
- Sayama, H.; Nakamura, Y.; Saito, N.; Kinoshita, M. Why is the concentration of plasma brain natriuretic peptide in elderly inpatients greater than normal? Coron. Artery Dis. 1999, 10, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Sobhani, K.; Nieves Castro, D.K.; Fu, Q.; Gottlieb, R.A.; Van Eyk, J.E.; Merz, C.N.B. Sex differences in ischemic heart disease and heart failure biomarkers. Biol. Sex Differ. 2018, 9, 43. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study/Reference | Dosage of BNP pmol/kg/min | GFR | RPF | Urine Volume | Urine Na | Urine cGMP | Urine Aldo | Plasma cGMP | PRA | AngII | Plasma Aldo | MAP | HR | CO | SVR | PCWP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal Subjects | ||||||||||||||||
| McGregor. J. Clin. Endocrinol. Metab. 1990 [36] | 2 | ↑↔ * | ↑ | ↓ | ↓ | ↔ | ↔ | |||||||||
| Yoshimura. Circulation. 1991 [37] | 30 | ↑ | ↑ | ↑ | ↔ | ↓ | ↓ | ↑ | ↑ | ↓ | ↓ | |||||
| Holmes. J. Clin. Endocrinol. Metab. 1993 [9] | 2 | ↔ | ↑ | ↑ | ↑ | ↓↔ * | ↓ | ↔ | ↑ | |||||||
| Cheung. Clin. Sci. 1994 [38] | 0.4 | ↔ | ↔ | ↑ | ↔ | ↔ | ||||||||||
| Florkowski. Am. J. Physiol. 1994 [39] | 2(+ANP(2)) ** | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↓ | ↔ | ||||||
| La Villa. J. Clin. Endocrinol. Metab. 1994 [40] | 4 | ↑ | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↔ | ↔ | ↔ | ||||
| La Villa. Hypertension. 1995 [41] | 0.25 and 0.5 | ↔ | ↔ | ↔ | ↑ | ↑ | ↓ | ↓ | ↔ | ↔ | ||||||
| Lazzeri. Cardiology. 1995 [42] | 4, 8, 10, 12 | ↑ | ↔ | ↔ | ↑ | ↔ | ↔ | |||||||||
| Hunt. J Clin. Endocrinol. Metab. 1996 [43] | 2 | ↔ | ↑ | ↑ | ↑ | ↓↔ * | ↓ | ↓ | ↔ | ↑ | ||||||
| Yasue. J Card. Fail. 1996 [44] | 30 | ↑ | ↑ | ↑ | ↑ | ↓ | ↑ | ↓ | ↓ | |||||||
| Jensen. Am. J. Phy.1998 [35] | 1, 2 and 4 | ↑ | ↓ | ↑ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↔ | ↔ | ||||
| Jensen. Clin. Sci. 1999 [5] | 2 | ↑ | ↓ *** | ↔ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↑ | ↔ | ||||
| van der Zander. Am. J. Physiol. 2003 [45] | 4 | ↑ | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓↔ * | ↔ | ||||||
| Summarized | ↑ | ↔ | ↑ | ↑ | ↑ | ↑ | ↓↔ | ↔ | ↓ | ↔ | ↔ | ↔ | ↔ | ↓ | ||
| Patients with Heart Failure | ||||||||||||||||
| Yoshimura. Circulation. 1991 [37] | 30 | ↑ | ↑ | ↑ | ↔ | ↓ | ↓ | ↑ | ↑ | ↓ | ↓ | |||||
| Marcus. Circulation. 1996 [46] | 1 to 30 | ↔ | ↑ | ↑ | ↑ | ↓ | ↓ | ↑ | ↓ | ↓ | ||||||
| Yasue. J. Card. Fail. 1996 [44] | 30 | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓ | ↓ | |||||||
| Lainchbury. HTN 1997 [47] | 3.3 | ↔ | ↔ | ↑ | ↔ | ↔ | ↓ | ↔ | ↔ | ↓ | ↓ | |||||
| Abraham. J. Cardiac. fail. 1998 [48] | 7.5, 15 | ↔ | ↔ | ↔ | ↔ | ↑ | ↔ | ↓ | ↓ | ↔ | ↑ | ↓ | ↓ | |||
| Jensen. Clin. Sci. 1999 [5] | 2 | ↔ | ↔ | ↔ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↑ | ↔ | ||||
| Wang. Am. J. Trans. Res. 2016 [49] | A bolus followed by 2 to 6 for 72 h | ↓ | ↓ | |||||||||||||
| Summarized | ↔ | ↔ | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓ | ↓ | ↔ | ↑ | ↓ | ↓ | ||
| Patients with Hypertension | ||||||||||||||||
| Richards. J. Hypertension. 1993 [50] | 2 | ↔ | ↑ | ↑ | ↔ | ↑ | ↔ # | ↓ | ↔ | ↔ | ||||||
| Lazzeri. Am. J. Hypertension. 1995 [51] | 4 | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↔ | ↔ | ||||||
| Pidgeon. Hypertension. 1996 [52] | 2 | ↑ | ↑ | ↔ | ↑ | ↓ | ↓ | ↓ | ↑ | |||||||
| Summarized | ↑ | ↑ | ↑ | ↑ | ↔ | ↓ | ↔ | ↔ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, R.; Ali, Y.; Hashizume, R.; Suzuki, N.; Ito, M. BNP as a Major Player in the Heart-Kidney Connection. Int. J. Mol. Sci. 2019, 20, 3581. https://doi.org/10.3390/ijms20143581
Okamoto R, Ali Y, Hashizume R, Suzuki N, Ito M. BNP as a Major Player in the Heart-Kidney Connection. International Journal of Molecular Sciences. 2019; 20(14):3581. https://doi.org/10.3390/ijms20143581
Chicago/Turabian StyleOkamoto, Ryuji, Yusuf Ali, Ryotaro Hashizume, Noboru Suzuki, and Masaaki Ito. 2019. "BNP as a Major Player in the Heart-Kidney Connection" International Journal of Molecular Sciences 20, no. 14: 3581. https://doi.org/10.3390/ijms20143581
APA StyleOkamoto, R., Ali, Y., Hashizume, R., Suzuki, N., & Ito, M. (2019). BNP as a Major Player in the Heart-Kidney Connection. International Journal of Molecular Sciences, 20(14), 3581. https://doi.org/10.3390/ijms20143581