Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review


Abstract
:1. Introduction
2. Methods
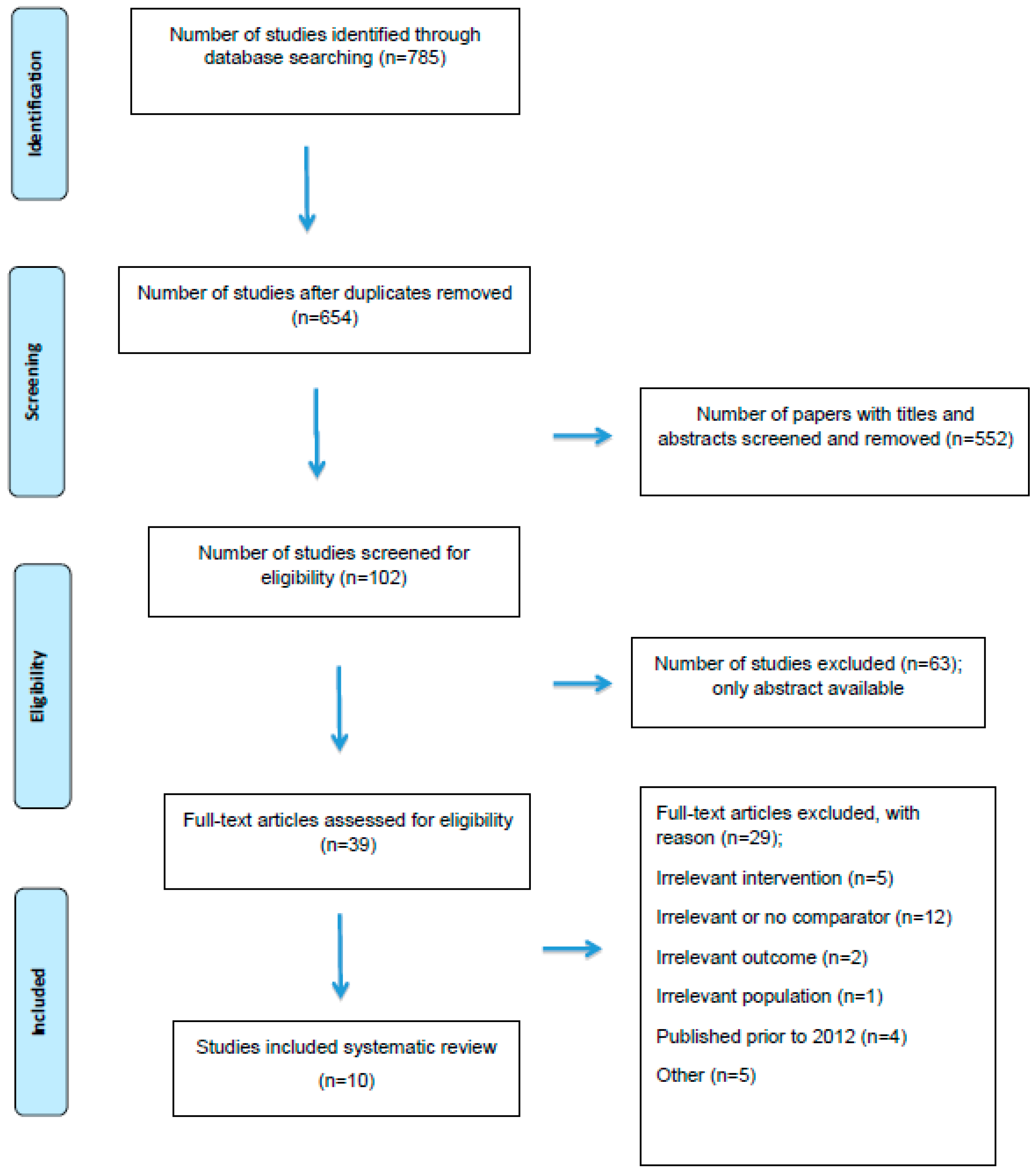
3. Results
3.1. Bias
3.2. General Characteristics
3.3. Participants
3.4. Study Objectives
3.5. Interventions
3.6. Serum 25(OH)D Levels
3.7. Immunologic Markers
3.8. Functional Measures
3.9. Relapse Rate
3.10. Disability
3.11. Safety and Tolerability
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mandia, D.; Ferraro, O.E.; Nosari, G.; Montomoli, C.; Zardini, E.; Bergamaschi, R. Environmental factors and multiple sclerosis severity: A descriptive study. Int. J. Environ. Res. Public Health 2014, 11, 6417–6432. [Google Scholar] [CrossRef] [PubMed]
- McDowell, T.Y.; Amr, S.; Culpepper, W.J.; Langenberg, P.; Royal, W.; Bever, C.; Bradham, D.D. Sun exposure, vitamin D intake and progression to disability among veterans with progressive multiple sclerosis. Neuroepidemiology 2011, 37, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Pierrot-Deseilligny, C.; Rivaud-Pechoux, S.; Clerson, P.; de Paz, R.; Souberbielle, J.C. Relationship between 25-OH-D serum level and relapse rate in multiple sclerosis patients before and after vitamin D supplementation. Adv. Neurol. Disord. 2012, 5, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Bagur, M.J.; Murcia, M.A.; Jimenez-Monreal, A.M.; Tur, J.A.; Bibiloni, M.M.; Alonso, G.L.; Martinez-Tome, M. Influence of diet in multiple sclerosis: A systematic review. Adv. Nutr. 2017, 8, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Runia, T.F.; Hop, W.C.; de Rijke, Y.B.; Buljevac, D.; Hintzen, R.Q. Lower serum vitamin D levels are associated with a higher relapse risk in multiple sclerosis. Neurology 2012, 79, 261–266. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and vitamin D: A global perspective for health. Dermatoendocrinol 2013, 5, 51–108. [Google Scholar] [CrossRef]
- Duan, S.; Lv, Z.; Fan, X.; Wang, L.; Han, F.; Wang, H.; Bi, S. Vitamin D status and the risk of multiple sclerosis: A systematic review and meta-analysis. Neurosci. Lett. 2014, 570, 108–113. [Google Scholar] [CrossRef]
- Harandi, A.A.; Harandi, A.A.; Pakdaman, H.; Sahraian, M.A. Vitamin D and multiple sclerosis. Iran. J. Neurol. 2014, 13, 1–6. [Google Scholar]
- Fitzgerald, K.C.; Munger, K.L.; Kochert, K.; Arnason, B.G.; Comi, G.; Cook, S.; Goodin, D.S.; Filippi, M.; Hartung, H.P.; Jeffery, D.R.; et al. Association of vitamin D levels with multiple sclerosis activity and progression in patients receiving interferon beta-1b. JAMA Neurol. 2015, 72, 1458–1465. [Google Scholar] [CrossRef]
- Pozuelo-Moyano, B.; Benito-Leon, J. Diet and multiple sclerosis. Rev. Neurol. 2014, 58, 455–464. [Google Scholar]
- McLaughlin, L.; Clarke, L.; Khalilidehkordi, E.; Butzkueven, H.; Taylor, B.; Broadley, S.A. Vitamin D for the treatment of multiple sclerosis: A meta-analysis. J. Neurol. 2018, 265, 2893–2905. [Google Scholar] [CrossRef]
- Golan, D.; Halhal, B.; Glass-Marmor, L.; Staun-Ram, E.; Rozenberg, O.; Lavi, I.; Dishon, S.; Barak, M.; Ish-Shalom, S.; Miller, A. Vitamin D supplementation for patients with multiple sclerosis treated with interferon-beta: A randomized controlled trial assessing the effect on flu-like symptoms and immunomodulatory properties. BMC Neurol. 2013, 13, 60. [Google Scholar] [CrossRef]
- Sotirchos, E.S.; Bhargava, P.; Eckstein, C.; Van Haren, K.; Baynes, M.; Ntranos, A.; Gocke, A.; Steinman, L.; Mowry, E.M.; Calabresi, P.A. Safety and immunologic effects of high- vs low-dose cholecalciferol in multiple sclerosis. Neurology 2016, 86, 382–390. [Google Scholar] [CrossRef]
- Aivo, J.; Hanninen, A.; Ilonen, J.; Soilu-Hanninen, M. Vitamin D3 administration to ms patients leads to increased serum levels of latency activated peptide (lap) of TGF-β. J. Neuroimmunol. 2015, 280, 12–15. [Google Scholar] [CrossRef]
- Rosjo, E.; Steffensen, L.H.; Jorgensen, L.; Lindstrom, J.C.; Saltyte Benth, J.; Michelsen, A.E.; Aukrust, P.; Ueland, T.; Kampman, M.T.; Torkildsen, O.; et al. Vitamin D supplementation and systemic inflammation in relapsing-remitting multiple sclerosis. J. Neurol. 2015, 262, 2713–2721. [Google Scholar] [CrossRef]
- Ashtari, F.; Toghianifar, N.; Zarkesh-Esfahani, S.H.; Mansourian, M. Short-term effect of high-dose vitamin D on the level of interleukin 10 in patients with multiple sclerosis: A randomized, double-blind, placebo-controlled clinical trial. Neuroimmunomodulation 2015, 22, 400–404. [Google Scholar] [CrossRef]
- Muris, A.H.; Smolders, J.; Rolf, L.; Thewissen, M.; Hupperts, R.; Damoiseaux, J.; SOLARIUM Study Group. Immune regulatory effects of high dose vitamin D3 supplementation in a randomized controlled trial in relapsing remitting multiple sclerosis patients receiving ifnbeta; the solarium study. J. Neuroimmunol. 2016, 300, 47–56. [Google Scholar] [CrossRef]
- Toghianifar, N.; Ashtari, F.; Zarkesh-Esfahani, S.H.; Mansourian, M. Effect of high dose vitamin D intake on interleukin-17 levels in multiple sclerosis: A randomized, double-blind, placebo-controlled clinical trial. J. Neuroimmunol. 2015, 285, 125–128. [Google Scholar] [CrossRef]
- Kampman, M.T.; Steffensen, L.H.; Mellgren, S.I.; Jorgensen, L. Effect of vitamin D3 supplementation on relapses, disease progression, and measures of function in persons with multiple sclerosis: Exploratory outcomes from a double-blind randomised controlled trial. Mult. Scler. 2012, 18, 1144–1151. [Google Scholar] [CrossRef]
- Soilu-Hanninen, M.; Aivo, J.; Lindstrom, B.M.; Elovaara, I.; Sumelahti, M.L.; Farkkila, M.; Tienari, P.; Atula, S.; Sarasoja, T.; Herrala, L.; et al. A randomised, double blind, placebo controlled trial with vitamin D3 as an add on treatment to interferon beta-1b in patients with multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2012, 83, 565–571. [Google Scholar] [CrossRef]
- Shaygannejad, V.; Janghorbani, M.; Ashtari, F.; Dehghan, H. Effects of adjunct low-dose vitamin D on relapsing-remitting multiple sclerosis progression: Preliminary findings of a randomized placebo-controlled trial. Mult. Scler. Int. 2012, 2012, 452541. [Google Scholar] [CrossRef] [PubMed]
- Jagannath, V.A.; Filippini, G.; Di Pietrantonj, C.; Asokan, G.V.; Robak, E.W.; Whamond, L.; Robinson, S.A. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst. Rev. 2018, 9, CD008422. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; He, L.; Liu, L.; Zhu, J.; Jin, T. The efficacy of vitamin D in multiple sclerosis: A meta-analysis. Mult. Scler. Relat. Disord. 2018, 23, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Burton, J.M.; Kimball, S.; Vieth, R.; Bar-Or, A.; Dosch, H.M.; Cheung, R.; Gagne, D.; D’Souza, C.; Ursell, M.; O’Connor, P. A phase i/ii dose-escalation trial of vitamin D3 and calcium in multiple sclerosis. Neurology 2010, 74, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Loken-Amsrud, K.I.; Holmoy, T.; Bakke, S.J.; Beiske, A.G.; Bjerve, K.S.; Bjornara, B.T.; Hovdal, H.; Lilleas, F.; Midgard, R.; Pedersen, T.; et al. Vitamin D and disease activity in multiple sclerosis before and during interferon-beta treatment. Neurology 2012, 79, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Mosayebi, G.; Ghazavi, A.; Ghasami, K.; Jand, Y.; Kokhaei, P. Therapeutic effect of vitamin D3 in multiple sclerosis patients. Immunol. Investig. 2011, 40, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Laursen, J.H.; Sondergaard, H.B.; Sorensen, P.S.; Sellebjerg, F.; Oturai, A.B. Vitamin D supplementation reduces relapse rate in relapsing-remitting multiple sclerosis patients treated with natalizumab. Mult. Scler. Relat. Disord. 2016, 10, 169–173. [Google Scholar] [CrossRef]
- Simpson, S., Jr.; Taylor, B.; Blizzard, L.; Ponsonby, A.L.; Pittas, F.; Tremlett, H.; Dwyer, T.; Gies, P.; van der Mei, I. Higher 25-hydroxyvitamin D is associated with lower relapse risk in multiple sclerosis. Ann. Neurol. 2010, 68, 193–203. [Google Scholar]
- Thouvenot, E.; Orsini, M.; Daures, J.P.; Camu, W. Vitamin D is associated with degree of disability in patients with fully ambulatory relapsing-remitting multiple sclerosis. Eur. J. Neurol. 2015, 22, 564–569. [Google Scholar] [CrossRef]
- Smolders, J.; Peelen, E.; Thewissen, M.; Cohen Tervaert, J.W.; Menheere, P.; Hupperts, R.; Damoiseaux, J. Safety and t cell modulating effects of high dose vitamin D3 supplementation in multiple sclerosis. PLoS ONE 2010, 5, e15235. [Google Scholar] [CrossRef]


{kind=link}
| Database Searched | Search Terms Used | Number of Results | Date of Search |
|---|---|---|---|
| PubMed |
| 215 | 01/11/2017 |
| Web of Science | • As above | 197 | 04/11/2017 |
| CINAHL | • As above | 19 | 12/11/2017 |
| Science Direct | • As above | 354 | 12/11/2017 |
| Total | 785 |
| Reference | Participant Demographics | Study Design, Duration and Country of Origin | Intervention | Outcome Measures |
|---|---|---|---|---|
| [19] | 68 participants (48f, 20m) with MS; Age mean (range) in vitamin D group 40 (21–50) and placebo 41 (26–50); BMI in vitamin D group 28 and placebo group 26 | Double-blind placebo- controlled RCT; 96 weeks; Norway | 35 participants received supplementation with 20,000 IU vitamin D3 (cholecalciferol)per week; comparator 33 participants received placebo | Serum levels of 25(OH)D; ARR; EDSS; MSFC components; grip strength; FSS |
| [21] | 50 participants (424f, 6m) with RRMS; Age mean (SD) in vitamin D 38.6 (8.4) and placebo 37.9 (7.9); No BMI | Double-blind placebo-controlled RCT; 48 weeks; Iran | 25 participants received 0.25 μg/d of calcitriol for 2 weeks and then 0.5 μg/d; comparator 25 participants received placebo | EDSS; relapse rate |
| [12] | 45 participants (32f, 13m) with RRMS; Age mean in high-dose group 43.1 (21.7–63.7) and in low-dose group 43.6 (26.7–63.9); No BMI | Double-blind placebo-controlled RCT; 48 weeks; Israel | High-dose group, 24 participants received 75,000IU vitamin D3 solution every 3 weeks in addition to 800 IU vitamin D3 per day (total 4370 IU); comparator low dose group, 21 participants received placebo every 3 weeks in addition to 800 IU/d of vitamin D3 | Serum levels of 25(OH)D; FLS; serum calcium, PTH, cytokine levels (IL-17, IL-10, and IFN-γ); EDSS, relapses, adverse events; QoL |
| [14] | 59 participants (37f, 22m) with RRMS; Age mean (range) in vitamin D 38 (22–53) and in placebo 35 (24–53); BMI 24 kg/m2 | Double-blind RCT; 48 weeks; Finland | 30 participants received 20,000 IU of vitamin D3 (cholecalciferol) per week; comparator 29 participants received placebo | Serum levels of 25(OH)D; inflammatory cytokine: Serum concentrations of LAP (TGF-β); IFN-γ, IL-17A, IL-2, IL-10, IL-9, IL-22, IL-6, IL-13, IL-4, IL-5, IL-1β and TNF-α |
| [16] | 89 participants (75f, 14m) with RRMS; Age mean (SD) in vitamin D group 31.50 (7.60) and placebo 34.60 (10.12); No BMI | Double-blind placebo-controlled RCT; 12 weeks; Iran | High-dose vitamin D group, 44 participants received 50,000 IU of vitamin D3 every 5 days; comparator 45 participants received placebo | Serum levels of 25(OH)D; serum calcium; serum interleukin 10 (IL-10) levels |
| [15] | 68 participants (48f, 20m) with RRMS; Age mean (range) in vitamin D group 40 (21–50) and placebo 41 (28–50); BMI vitamin D group 25.9 and placebo 26.5 | Double-blind placebo-controlled RCT; 96 weeks; Norway | 36 participants received 20,000 IU vitamin D3 per week; comparator 32 participants received placebo | Serum 25(OH)D; 11 serum markers of inflammation, bone mineral density, clinical disease activity, disease progression: ALCAMd, CCL21e, CXCL16f, IL-1Rag, MMP-9h, OPGi, OPNj, PTX3k, sFRP3l, sTNF-R1m, TGF-b1n |
| [18] | 89 participants (75f, 14m) with RRMS; Age mean (SD) in vitamin D group 31.50 (7.60) and placebo 34.60 (10.12); No BMI | Double-blind placebo-controlled RCT; 12 weeks; Iran | 44 participants received oral vitamin D3 50,000 IU every 5 days; comparator 45 participants received placebo | Serum levels of 25(OH)D, serum calcium, IL-17 |
| [17] | 53 participants (35f, 18m) with RRMS; Age mean (SD) in vitamin D group 37.7 (7.2) and placebo 37.2 (9.6); BMI ≥ 25 kg/m2 | Double-blind placebo-controlled RCT; 48 weeks; Netherlands | 30 participants received high-dose vitamin D3 supplementation 7000 IU/d for 4 weeks, followed by 14,000 IU/d; comparator 23 participants received placebo | Serum 25(OH)D; serum interleukin 10 (IL-10) levels; cytokine expression of IL4, IFNγ, IL17, IL22, GMCSF and TNFα by CD3+ CD8− T lymphocytes |
| [13] | 40 participants (28f, 12m) with RRMS; Age mean (SD) in high-dose group 41.3 (8.1) and placebo 38.8 (8.8); No BMI | Double-blind RCT; 24 weeks; United States | High-dose group, 19 participants received 10,000 IU/d of cholecalciferol; comparator low-dose group, 21 participants received 400 IU/d of cholecalciferol | Serum 25(OH)D levels; adverse events, relapses, IFN-γ+ IL-17+ CD4+ T cells |
| [20] | 66 participants (41f, 15m) with RRMS; Age median (range) in vitamin D group 39 (22–53) and placebo 35 (24–53); BMI median (range) in vitamin D group 24 (18–40) and placebo 24 (19–38) | Double-blind placebo controlled RCT; 48 weeks; Finland | 34 participants received oral vitamin D3 (cholecalciferol) 20,000 IU once a week; comparator group 32 participants received placebo | Serum levels of 25(OH)D; PTH level, T2 BOD; total number of Gd enhancing T1 lesions; new/enlarging T2 lesions; Gd enhancing lesion volume; MRI activity; ARR, EDSS, T25FW and TTW10 |
| Study | Age | MS Diagnosis | EDSS Score | Serum 25(OH)D Level | Other Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|---|---|
| [19] | 18–50 years | MS | ≤4.5 | n/a | n/a | Inability to walk 500 m or more; conditions or medication affecting bone health; pregnancy, lactating during the past 6 months; menopause; unwillingness to use contraception |
| [21] | 15–60 years | RRMS | ≤6 | >40 ng/mL | RRMS for 1–12 years, no relapse for at least one month; continue current medications | SPMS and PPMS; other conditions; use of vitamin D supplements; pregnancy |
| [12] | ≥18 years | RRMS | <7 | <75 nmol/L or (<30 ng/mL) | IFN-β therapy or those who continue to suffer from FLS beyond 4 months of treatment with IFN-β | Abnormalities of vitamin D related hormonal system; use of medications that influence vitamin D metabolism; conditions of increased susceptibility to hypercalcemia; pregnancy |
| [14] | 18–55 years | RRMS | <5 | <85 nmol/L or (<34 ng/mL) | IFN-β therapy for at least 1month and no neutralizing antibodies; contraception; at least one relapse during the year prior the study and/or MRI activity defined as presence of Gd-enhancing lesions on brain MRI | Serum calcium > 2.6 mmol/L; other conditions; pregnancy; use of other immunomodulatory therapy than INFB-1β; allergy to cholecalciferol or peanuts; alcohol or drug abuse |
| [16] | 18–55 years | RRMS | <4 | n/a | No relapse 30 days before inclusion; negative β-HCG test for women; calcium < 11 mg/dL | Pregnancy; lactation; other disease; receiving > 4000 IU of vitamin D, corticosteroids treatment in the previous 30 days; aspartate or alanine transaminase > 3xnormal values, ALP > 2.5xnormal values |
| [15] | 18–50 years | RRMS | <4.5 | n/a | n/a | Disease or medication affecting bone health; menopause; pregnancy; lactation; nephrolithiasis |
| [18] | 18–55 years | RRMS | <4 | <85 ng/mL | No relapse 30 days prior to study day; negative β-HCG test for women; calcium < 11 mg/dL; no relapse during the study | Pregnancy; lactation; other diseases; receiving >4000 IU of vitamin D, corticosteroids therapy in the previous 30 days; AST > 3xnormal values, ALP > 2.5xnormal values |
| [17] | 18–50 years | RRMS | ≤4 | n/a | No relapse within 30 days prior to study day; first clinical event occurring within 5 years prior to screening; have had at least one relapse, or one or more Gd-enhancing or new T2 MRI lesions within the 12 months; receiving IFNβ-1a > 90 days and <12 months | Pregnancy or lactation; other diseases; use of corticosteroids or adrenocorticotrophic hormone within 30 days prior to SD1 abnormalities of vitamin D-related hormonal system; use of medications that influence vitamin D metabolism; taking N400 IU (N10 μg) of vitamin D supplement daily |
| [13] | 18–55 years | RRMS | n/a | 20–50 ng/mL | No relapse within 30 days; serum creatinine >1.5 mg/dL | Daily intake of vitamin D > 1000 IU or change of immunomodulatory therapy within the past 3 months, systemic glucocorticoid therapy; pregnancy, other condition |
| [20] | 18–55 years | RRMS | ≤5.0 | <85 nmol/L | IFNB-1b use for at least 1month; no neutralising antibodies to IFNβ, as measured by the indirect myxovirus A (MxA) test, using appropriate contraceptive methods. | Pregnancy; serum calcium >2.6 mmol/L; primary hyperparathyroidism; alcohol or drug abuse; use of immunomodulatory therapy other than IFNB-1b; known allergy to cholecalciferol or peanuts; therapy with digitalis, calcitonin, vitamin D3 analogues or vitamin D; any condition predisposing to hypercalcaemia; significant hypertension (blood pressure < 180/110 mm Hg); hyperthyroidism or hypothyroidism in the year before the study began; a history of kidney stones in the previous 5 years; cardiac insufficiency or significant cardiac dysrhythmia; unstable ischaemic heart disease; depression; and inability to perform serial MRI scans. |
| References | Within Group Differences | Between Group Differences |
|---|---|---|
| [19] | Intervention: 20,000 IU of vitamin D significantly increased serum 25(OH)D levels from a mean of 55.56 to 123.17 nmol/L. Control: there was only a minor increase from 57.33 to 61.80 nmol/L. | Significant difference in serum levels of 25(OH)D after 96 weeks between the intervention and control groups (p < 0.001). |
| [21] | n/a | n/a |
| [12] | Intervention: serum 25(OH)D levels significantly increased in a high-dose (4370 IU/d) groups from a mean of 48.2 to 122.6 nmol/L Control: low-dose (800 IU/d) from 48 to 68 nmol/L. | Significantly higher serum 25(OH-D) levels were reported in high dose group compared to low-dose arm after 48 weeks (p < 0.001). |
| [14] | Intervention: serum 25(OH)D levels increased significantly from a mean of 54 to 109 nmol/L. Placebo: decreased from a mean of 55 to 51 nmol/L after 48 weeks. | n/a |
| [16] | Intervention: Serum 25(OH)D levels rose from a median of 28.27 to 84.67 nmol/L. Placebo: fell from 39.6 to 28.66 nmol/L. | A significant difference after 12 weeks between groups (p < 0.001). |
| [15] | Intervention: serum levels of 25(OH)D significantly increased from 56 to 123nmol/L. Placebo: levels slightly increased from 57 to 63 nmol/L. | A significant difference in serum levels after 96 weeks between groups (p < 0.001). |
| [18] | Intervention: serum 25(OH)D levels significantly increased from a median of 28.27 to 84.67 ng/mL. Placebo: a decrease from 39.6 to 28.66 ng/mL. | These differences were significant between groups after 12 weeks (p < 0.001). |
| [17] | Intervention: serum 25(OH)D concentration increased significantly in the vitamin D group from 60 to 231 nmol/L. Placebo: changed to a lesser degree (54 to 60 nmol/L). | The was a significant difference after 48 weeks between the groups (p < 0.001). |
| [13] | High dose: Mean change of 34.9 ng/mL. Low dose: mean change of 6.9 ng/mL | A high dose of vitamin D resulted in significantly higher serum 25(OH-D) levels versus low-dose after 24 weeks (p < 0.00001). |
| [20] | Intervention: serum 25(OH)D levels increased from a mean of 54 to 110 nmol/L. Placebo: decreased from a mean of 56 to 50 nmol/L after 48 weeks | A significant difference between groups (p < 0.001). |
| Reference | Key findings | Significance | Conclusion |
|---|---|---|---|
| [19] | 1. Serum 25(OH)D level significantly increased in intervention group vs control | 1. p < 0.001 | Supplementation did not result in beneficial effects on the measured MS-related outcomes; no significant difference between groups in ARR, EDSS, MSFC components, grip strength or fatigue |
| 2. ARR increased in intervention group vs control | 2. p = 0.25 | ||
| 3. EDSS decreased in intervention group vs control | 3. p = 0.97 | ||
| 4. MSFC components: 25ft timed walk decreased in intervention group vs control; 9-HPT increased in intervention group vs control; PASAT increased in intervention vs control; | 4. p = 0.87; p = 0.35; p = 0.21 | ||
| 5. Grip strength decreased in intervention group vs control; | 5. p = 0.76 | ||
| 6. Fatigue increased in intervention group vs control | 6. p = 0.9 | ||
| [21] | 1. Relapse rate significantly decreased in intervention and control groups; no significant difference in relapse rate between the groups; | 1. p < 0.001; p < 0.001; p > 0.05; | No significant differences in the EDSS score or relapse rate between the vitamin D and control groups at the end of the study period; vitamin D supplementation at the doses used seems safe |
| 2. EDSS unchanged in intervention group and increased in control | 2. N/A; p < 0.01 | ||
| [12] | 1. Serum 25(OH)D levels increased in HDVD group vs LDVD group; | 1. p < 0.001 | Vitamin D supplementation was associated with dose-dependent changes in IL-17 serum levels, while not affecting IFN−β related FLS; vitamin D supplementation at the doses used seems safe |
| 2. PTH decreased in HDVD group but no significant change with LDVD; | 2. p = 0.04; p = 0.17 | ||
| 3. No change in FLS | 3. N/A | ||
| 4. IL-17 levels increased in HDVD and LDVD groups; | 4. p = 0.75; p = 0.04 | ||
| 5. No significant differences in relapse rate, EDSS, QoL, serum IL-10 and IFNγ; | 5. p > 0.05 | ||
| 6. Serum calcium levels remained stable and within normal range in both dosage groups | 6. p = 0.2; p = 0.4 | ||
| [14] | 1. Serum levels of 25(OH)D increased in intervention group and edcreased in control; | 1. N/A | Serum LAP (TGF-β) levels increased significantly in people receiving vitamin D; Therefore vitamin D might be useful in improving MRI outcomes; The levels of the other cytokines did not change significantly in either group |
| 2. Serum levels of LAP (TGF-β) increased in intervention and control group; | 2. p = 0.0249; p = 0.173 | ||
| 3. The levels of serum IFN-gamma; IL-17A and in IL-9 increased in intervention group | 3. p = 0.0519; p = 0.0666; p = 0.0679 | ||
| [16] | 1. Serum 25(OH)D levels increased in intervention group; | 1. p < 0.001 | 25(OH)D levels increased significantly in those treated with vitamin D; IL-10 level increased significantly in the intervention group and its anti-inflammatory effect may play a role in improving outcomes in MS |
| 2. IL-10 levels increased in intervention group; | 2. p = 0.015 | ||
| 3. No significant differences in serum calcium between groups at baseline or after 3 months | 3. p = 0.980; p = 0.302 | ||
| [15] | 1. Serum 25(OH)D level increased in intervention versus control; | 1. p < 0.001 | 25(OH)D levels increased significantly in vitamin D group versus control; No significant differences for any inflammation markers between groups |
| 2. The inflammation marker averages did not differ significantly between groups | 2. p > 0.05 | ||
| [18] | 1. Serum 25(OH)D level increased in intervention versus control group; | 1. p < 0.001 | 25(OH)D levels increased significantly in people in the intervention group; Significant difference in EDSS between groups; No difference in IL-17 levels between vitamin D and control group |
| 2. EDSS scores differ between groups; | 2. p = 0.033 | ||
| 3. Serum levels of IL-17 changed in intervention group; | 3. p = 0.002 | ||
| 4. No significant differences in serum calcium between groups at baseline and after 12 weeks | 4. p = 0.980; p = 0.302 | ||
| [17] | 1. Serum 25(OH)D level increased in intervention versus control group; | 1. p < 0.001 | 25(OH)D levels increased significantly in the vitamin D group; Supplementation of vitamin D did not result in a relative increase in the total amount of lymphocytes |
| 2. The total amount of lymphocytes are similar between baseline and week 48; | 2. p > 0.05 | ||
| 3. The proportion of cells in the immune regulatory cell compartment (nTreg, iTreg and Breg) did not change in either group; | 3. p > 0.05 | ||
| 4. IL4+ Th cells decreased in the control but not the intervention group; | 4. p = 0.04; p = 0.92 | ||
| 5. T cell cytokine secretion increased (IL5, LAP (TGF-β)) in the control but not the intervention group | 5. p = 0.02; p < 0.001 p = 0.06; p < 0.01 | ||
| [13] | 1. Serum 25(OH)D level increased in HDVD group vs LDVD; | 1. p < 0.00001 | 25(OH)D levels increased significantly in the vitamin D group; Vitamin D supplementation exhibited immunomodulatory effects including reduction of interleukin-17 and decreased the proportion of effector memory CD4+ T cells with concomitant increase in central memory CD4+ T cells and naive CD4+ T cells; 10,400 IU daily is safe and tolerable |
| 2. The proportion of interleukin-17+CD4+ T cells, CD161+CD4+ T cells, and effector memory CD4+ T cells, the proportion of central memory CD4+ T cells and naive CD4+ T cells increased in HDVD group | 2. p = 0.016; p = 0.03; p = 0.021; p = 0.018; p = 0.04 | ||
| [20] | 1. Serum 25(OH)D level significantly increased in intervention group vs control; | 1. p < 0.001 | Vitamin D3 add on treatment to IFNB reduces MRI T1 enhancing lesions. Vitamin D supplementation at the doses used seems safe. |
| 2. T2 BOD reduced in intervention group vs control; | 2. p = 0.105 | ||
| 3. Total number of Gd enhancing T1 lesions significantly decreased in the intervention group vs control; | 3. p = 0.004 | ||
| 4. Fewer new/enlarging T2 lesions in the intervention group vs control; | 4. p = 0.286 | ||
| 5. Gd enhancing lesion volume decreased in intervention group vs control; | 5. p = 0.320 | ||
| 6. MRI activity lower in intervention group vs control; | 6. p = 0.322 | ||
| 7. ARR decreased in intervention group vs control; | 7. N/A | ||
| 8. EDSS decreased in intervention group vs control; | 8. p = 0.071 | ||
| 9. TTW10 decreased in intervention group vs control; | 9. p = 0.076 | ||
| 10. T25FW decreased in intervention group vs control | 10. p = 0.932 |
| Study | High-Dose of Vitamin D | Low-Dose of Vitamin D | Placebo | Concomitant Immunomodulatory Therapy and Vitamin D/Calcium Supplements |
|---|---|---|---|---|
| [19] | 20,000 IU of vitamin D3 per week | ✗ | ✔ | 500 mg/d calcium; no restrictions on vitamin D supplements |
| [21] | 0.25 μg/d of calcitriol for 2 weeks and then 0.5 μg/d | ✗ | ✔ | IFNβ (86.0% of participants), statins (10.0%), or immunosuppressive drugs (4.0%) |
| [12] | 4370 IU/d of vitamin D3 | 800 IU/d of vitamin D3 | ✗ | IFNβ |
| [14] | 20,000 IU of vitamin D3 per week | ✗ | ✔ | IFNβ |
| [16] | 50,000 IU of vitamin D3 every 5days | ✗ | ✔ | IFNβ; interferon-β; participants were not allowed to take any other vitamin D supplements; |
| [15] | 20,000 IU vitamin D3 per week | ✗ | ✔ | calcium supplementation (500 mg/d); no restrictions on regular vitamin D supplementation or immunomodulatory treatment (i.e., IFN-b, glatiramer acetate, or natalizumab) |
| [18] | 50,000 IU of vitamin D3 every 5days | ✗ | ✔ | IFNβ |
| [17] | 7000 IU/d of vitamin D3 for 4 weeks, followed by 14,000 IU/d of vitamin D3; | ✗ | ✔ | IFNβ-1a |
| [13] | 10,400 IU/d of vitamin D3 | 400 IU/d of vitamin D3 | ✗ | 89% of participants received immunomodulatory therapy; multivitamin containing 400 IU of D3 and 1000 mg/d of calcium |
| [20] | 20,000 IU of vitamin D3 per week | ✗ | ✔ | IFNβ-1b |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berezowska, M.; Coe, S.; Dawes, H. Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 1301. https://doi.org/10.3390/ijms20061301
Berezowska M, Coe S, Dawes H. Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review. International Journal of Molecular Sciences. 2019; 20(6):1301. https://doi.org/10.3390/ijms20061301
Chicago/Turabian StyleBerezowska, Monika, Shelly Coe, and Helen Dawes. 2019. "Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review" International Journal of Molecular Sciences 20, no. 6: 1301. https://doi.org/10.3390/ijms20061301
APA StyleBerezowska, M., Coe, S., & Dawes, H. (2019). Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review. International Journal of Molecular Sciences, 20(6), 1301. https://doi.org/10.3390/ijms20061301