Immune Checkpoint Blockade for Advanced NSCLC: A New Landscape for Elderly Patients

 ,
, 
 and
and 
Abstract
:1. Introduction
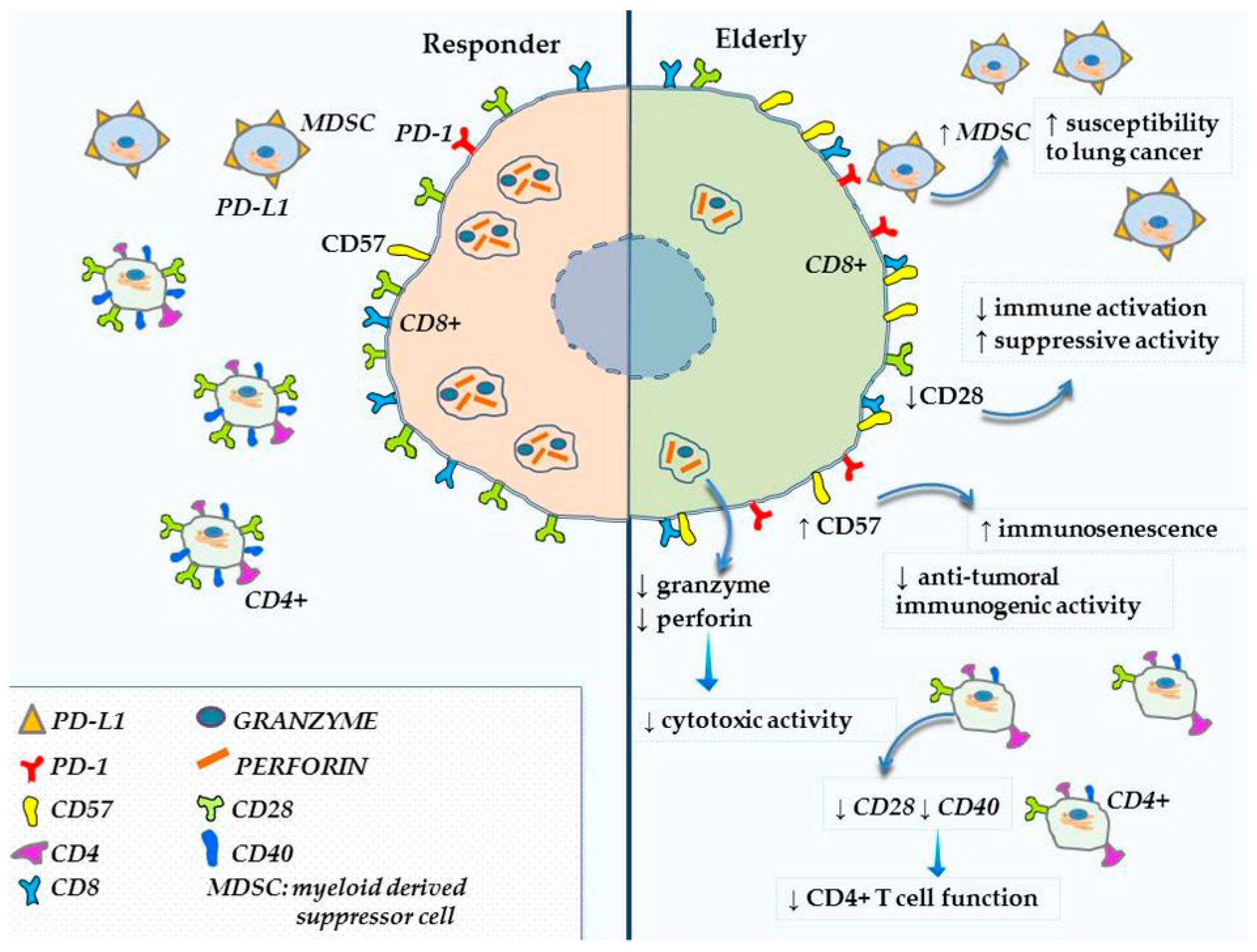
2. Immunosenescence and PD-1/PD-L1 Pathways
3. ICI’S for Advanced NSCLC in Elderly Population
3.1. Pembrolizumab
3.2. Nivolumab
3.3. Atezolizumab
3.4. Durvalumab
3.5. Recent Evidences in the Elderly Population
4. Comorbidities and Safety Profile
5. Gut microbiome and Immunosenescence: Implications for ICI’s
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Owonikoko, T.K.; Ragin, C.C.; Belani, C.P.; Oton, A.B.; Gooding, W.E.; Taioli, E.; Ramalingam, S.S. Lung cancer in elderly patients: An analysis of the surveillance, epidemiology, and end results database. J. Clin. Oncol. 2007, 25, 5570–5577. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Esposito, V.; Bianco, A.; Ferraraccio, F.; Prati, M.V.; Lucariello, A.; Manente, L.; Mezzogiorno, A.; De Luca, A. Inflammatory effects on human lung epithelial cells after exposure to diesel exhaust micron sub particles (PM(1).(0)) and pollen allergens. Environ. Pollut. 2012, 161, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Lucariello, A.; Bianco, A.; Calabrese, C.; Thanassoulas, T.; Savarese, L.; Fiumarella, A.; Esposito, V.; DE Luca, A. Exposure to submicron particles (PM1.0) from diesel exhaust and pollen allergens of human lung epithelial cells induces morphological changes of mitochondria tonifilaments and rough endoplasmic reticulum. In Vivo 2014, 28, 557–561. [Google Scholar] [PubMed]
- Esposito, V.; Lucariello, A.; Savarese, L.; Cinelli, M.P.; Ferraraccio, F.; Bianco, A.; De Luca, A.; Mazzarella, G. Morphology changes in human lung epithelial cells after exposure to diesel exhaust micron sub particles (PM(1).(0)) and pollen allergens. Environ. Pollut. 2012, 171, 162–167. [Google Scholar] [CrossRef]
- Nigro, E.; Stiuso, P.; Matera, M.G.; Monaco, M.L.; Caraglia, M.; Maniscalco, M.; Perrotta, F.; Mazzarella, G.; Daniele, A.; Bianco, A. The anti-proliferative effects of adiponectin on human lung adenocarcinoma A549cells and oxidative stress involvement. Pulm. Pharmacol. Ther. 2019, 55, 25–30. [Google Scholar] [CrossRef]
- Nigro, E.; Imperlini, E.; Scudiero, O.; Monaco, M.L.; Polito, R.; Mazzarella, G.; Orrù, S.; Bianco, A.; Daniele, A. Differentially expressed and activated proteins associated with non small cell lung cancer tissues. Respir. Res. 2015, 16, 74. [Google Scholar] [CrossRef]
- Illiano, M.; Nigro, E.; Sapio, L.; Caiafa, I.; Spina, A.; Scudiero, O.; Bianco, A.; Esposito, S.; Mazzeo, F.; Pedone, P.V.; et al. Adiponectin down-regulates CREB and inhibits proliferation of A549 lung cancer cells. Pulm. Pharmacol. Ther. 2017, 45, 114–120. [Google Scholar]
- Cardarella, S.; Johnson, B.E. The impact of genomic changes on treatment of lung cancer. Am. J. Respir. Crit. Care Med. 2013, 188, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, F.; Guerra, G.; Parisi, M.; Lucariello, A.; De Luca, A.; De Rosa, N.; Mazzarella, G.; Bianco, A.; Ammendola, R. Expression of Formyl-peptide receptors in human lung carcinoma. Anticancer Res. 2015, 35, 2769–2774. [Google Scholar] [PubMed]
- Di Zazzo, E.; Polito, R.; Bartollino, S.; Nigro, E.; Porcile, C.; Bianco, A.; Daniele, A.; Moncharmont, B. Adiponectin as Link Factor between Adipose Tissue and Cancer. Int. J. Mol. Sci. 2019, 20, 839. [Google Scholar] [CrossRef] [PubMed]
- Pawelec, G. Hallmarks of human “immunosenescence”: Adaptation or dysregulation? Immun. Ageing 2012, 9, 15. [Google Scholar] [CrossRef]
- Haynes, L.; Eaton, S.M. The effect of age on the cognate function of CD4(+) T cells. Immunol. Rev. 2005, 205, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Tomihara, K.; Curiel, T.J.; Zhang, B. Optimization of Immunotherapy in Elderly Cancer Patients. Crit. Rev. Oncog. 2013, 18, 573–583. [Google Scholar] [CrossRef] [Green Version]
- Fabrikant, M.S.; Wisnivesky, J.P.; Marron, T.; Taioli, E.; Veluswamy, R.R. Benefits and Challenges of Lung Cancer Screening in Older Adults. Clin. Ther. 2018, 40, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Izzo, A.; Perrotta, F.; Cennamo, A.; Cerqua, F.S.; Rinaldi, L.; Mazzella, A.; Grella, E.; Tranfa, C.; Bianco, A.; Stefanelli, F.; et al. Spirometry in elderly laryngectomized patients: A feasibility study. Int. J. Surg. 2016, 33 (Suppl. 1), S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Pilyugin, M.; Descloux, P.; André, P.-A.; Laszlo, V.; Dome, B.; Hegedus, B.; Sardy, S.; Janes, S.; Bianco, A.; Laurent, G.J.; et al. BARD1 serum autoantibodies for the detection of lung cancer. PLoS ONE 2017, 12, e0182356. [Google Scholar] [CrossRef]
- Davidoff, A.J.; Gardner, J.F.; Seal, B.; Edelman, M.J. Population-based estimates of survival benefit associated with combined modality therapy in elderly patients with locally advanced non-small cell lung cancer. J. Thorac. Oncol. 2011, 6, 934–941. [Google Scholar] [CrossRef]
- Zhang, Y.-Q.; Bianco, A.; Malkinson, A.M.; Leoni, V.P.; Frau, G.; De Rosa, N.; Andre, P.-A.; Versace, R.; Boulvain, M.; Laurent, G.J.; et al. BARD1: An independent predictor of survival in non-small cell lung cancer. Int. J. Cancer 2012, 131, 83–94. [Google Scholar] [CrossRef]
- Salvi, R.; Meoli, I.; Cennamo, A.; Perrotta, F.; Saverio Cerqua, F.; Montesano, R.; Curcio, C.; Lassandro, F.; Stefanelli, F.; Grella, E.; et al. Preoperative high-intensity training in frail old patients undergoing pulmonary resection for NSCLC. Open Med. 2016, 11, 443–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzella, A.; Izzo, A.; Amore, D.; Cennamo, A.; Cerqua, F.S.; Perrotta, F. Single port VATS resection of a sessile solitary fibrous tumour of the visceral pleura. A case report. Ann. Ital. Chir. 2015, 86. (ePub). [Google Scholar]
- Mazzella, A.; Izzo, A.; Amore, D.; Cerqua, F.S.; Perrotta, F. A new perspective on the treatment of complicated giant emphysematous bulla A case report. Ann. Ital. Chir. 2016, 87. (ePub). [Google Scholar]
- Perrotta, F.; Cerqua, F.S.; Cammarata, A.; Izzo, A.; Bergaminelli, C.; Curcio, C.; Guarino, C.; Grella, E.; Forzano, I.; Cennamo, A.; et al. Integrated therapeutic approach to giant solitary fibrous tumor of the pleura: Report of a case and review of the literature. Open Med. 2016, 11, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Guarino, C.; Mazzarella, G.; De Rosa, N.; Cesaro, C.; La Cerra, G.; Grella, E.; Perrotta, F.; Curcio, C.; Guerra, G.; Bianco, A. Pre-surgical bronchoscopic treatment for typical endobronchial carcinoids. Int. J. Surg. 2016, 33 (Suppl. 1), S30–S35. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, R.; Mezquita, L.; Auclin, E.; Chaput, N.; Besse, B. Immunosenescence and immunecheckpoint inhibitors in non-small cell lung cancer patients: Does age really matter? Cancer Treat. Rev. 2017, 60, 60–68. [Google Scholar] [CrossRef]
- Bianco, A.; Malapelle, U.; Rocco, D.; Perrotta, F.; Mazzarella, G. Targeting immune checkpoints in non small cell lung cancer. Curr. Opin. Pharmacol. 2018, 40, 46–50. [Google Scholar] [CrossRef]
- Fiorelli, A.; Perrotta, F.; Mollica, M.; Santini, M.; Vitiello, F.; Gilli, M.; Calabrese, C.; Bianco, A. Endoscopic central airway recanalization to enable first line pembrolizumab treatment in a PD-L1 strongly positive non-small cell lung cancer: A case report. J. Cardiothorac. Surg. 2019, 14, 50. [Google Scholar] [CrossRef]
- Gridelli, C.; Aapro, M.; Ardizzoni, A.; Balducci, L.; De Marinis, F.; Kelly, K.; Le Chevalier, T.; Manegold, C.; Perrone, F.; Rosell, R.; et al. Treatment of advanced non-small-cell lung cancer in the elderly: Results of an international expert panel. J. Clin. Oncol. 2005, 23, 3125–3137. [Google Scholar] [CrossRef]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A.J.; Albain, K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 1999, 341, 2061–2067. [Google Scholar] [CrossRef]
- Canaday, D.H.; Parker, K.E.; Aung, H.; Chen, H.E.; Nunez-Medina, D.; Burant, C.J. Age-dependent changes in the expression of regulatory cell surface ligands in activated human T-cells. BMC Immunol. 2013, 14, 45. [Google Scholar] [CrossRef]
- Barber, D.L.; Wherry, E.J.; Masopust, D.; Zhu, B.; Allison, J.P.; Sharpe, A.H.; Freeman, G.J.; Ahmed, R. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 2006, 439, 682–687. [Google Scholar] [CrossRef]
- Pawelec, G. Immunosenescence comes of age. Symposium on Aging Research in Immunology: The Impact of Genomics. EMBO Rep. 2007, 8, 220–223. [Google Scholar] [CrossRef] [Green Version]
- Muller, L.; Pawelec, G. As we age: Does slippage of quality control in the immune system lead to collateral damage? Ageing Res. Rev. 2015, 23, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Rossi, D.J.; Bryder, D.; Seita, J.; Nussenzweig, A.; Hoeijmakers, J.; Weissman, I.L. Deficiencies in DNA damage repair limit the function of haematopoietic stem cells with age. Nature 2007, 447, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Min, H.; Montecino-Rodriguez, E.; Dorshkind, K. Effects of aging on early B- and T-cell development. Immunol. Rev. 2005, 205, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Geiger, H.; de Haan, G.; Florian, M.C. The ageing haematopoietic stem cell compartment. Nat. Rev. Immunol. 2013, 13, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Guerra, G.; Perrotta, F.; Testa, G. Circulating endothelial progenitor cells biology and regenerative medicine in pulmonary vascular diseases. Curr. Pharm. Biotechnol. 2018, 19, 700–707. [Google Scholar] [CrossRef]
- Goronzy, J.J.; Fang, F.; Cavanagh, M.M.; Qi, Q.; Weyand, C.M. Naive T cell maintenance and function in human aging. J. Immunol. 2015, 194, 4073–4080. [Google Scholar] [CrossRef] [PubMed]
- Pfister, G.; Weiskopf, D.; Lazuardi, L.; Kovaiou, R.D.; Cioca, D.P.; Keller, M.; Lorbeg, B.; Parson, W.; Grubeck-Loebenstein, B. Naive T cells in the elderly: Are they still there? Ann. N. Y. Acad. Sci. 2006, 1067, 152–157. [Google Scholar] [CrossRef]
- Naylor, K.; Li, G.; Vallejo, A.N.; Lee, W.-W.; Koetz, K.; Bryl, E.; Witkowski, J.; Fulbright, J.; Weyand, C.M.; Goronzy, J.J. The influence of age on T cell generation and TCR diversity. J. Immunol. 2005, 174, 7446–7452. [Google Scholar] [CrossRef] [PubMed]
- Czesnikiewicz-Guzik, M.; Lee, W.-W.; Cui, D.; Hiruma, Y.; Lamar, D.L.; Yang, Z.-Z.; Ouslander, J.G.; Weyand, C.M.; Goronzy, J.J. T cell subset-specific susceptibility to aging. Clin. Immunol. 2008, 127, 107–118. [Google Scholar] [CrossRef] [Green Version]
- Koch, S.; Larbi, A.; Derhovanessian, E.; Ozcelik, D.; Naumova, E.; Pawelec, G. Multiparameter flow cytometric analysis of CD4 and CD8 T cell subsets in young and old people. Immun. Ageing 2008, 5, 6. [Google Scholar] [CrossRef]
- Weng, N.-P.; Akbar, A.N.; Goronzy, J. CD28(-) T cells: Their role in the age-associated decline of immune function. Trends Immunol. 2009, 30, 306–312. [Google Scholar] [CrossRef]
- Johnstone, J.; Millar, J.; Lelic, A.; Verschoor, C.P.; Walter, S.D.; Devereaux, P.J.; Bramson, J.; Loeb, M. Immunosenescence in the nursing home elderly. BMC Geriatr. 2014, 14, 50. [Google Scholar] [CrossRef]
- Gupta, S.; Gollapudi, S. CD95-mediated apoptosis in naive, central and effector memory subsets of CD4+ and CD8+ T cells in aged humans. Exp. Gerontol. 2008, 43, 266–274. [Google Scholar] [CrossRef]
- Filaci, G.; Fravega, M.; Negrini, S.; Procopio, F.; Fenoglio, D.; Rizzi, M.; Brenci, S.; Contini, P.; Olive, D.; Ghio, M.; et al. Nonantigen specific CD8+ T suppressor lymphocytes originate from CD8+CD28- T cells and inhibit both T-cell proliferation and CTL function. Hum. Immunol. 2004, 65, 142–156. [Google Scholar] [CrossRef]
- Brenchley, J.M.; Karandikar, N.J.; Betts, M.R.; Ambrozak, D.R.; Hill, B.J.; Crotty, L.E.; Casazza, J.P.; Kuruppu, J.; Migueles, S.A.; Connors, M.; et al. Expression of CD57 defines replicative senescence and antigen-induced apoptotic death of CD8+ T cells. Blood 2003, 101, 2711–2720. [Google Scholar] [CrossRef]
- Henson, S.M.; Macaulay, R.; Riddell, N.E.; Nunn, C.J.; Akbar, A.N. Blockade of PD-1 or p38 MAP kinase signaling enhances senescent human CD8(+) T-cell proliferation by distinct pathways. Eur. J. Immunol. 2015, 45, 1441–1451. [Google Scholar] [CrossRef]
- Lages, C.S.; Lewkowich, I.; Sproles, A.; Wills-Karp, M.; Chougnet, C. Partial restoration of T-cell function in aged mice by in vitro blockade of the PD-1/PD-L1 pathway. Aging Cell 2010, 9, 785–798. [Google Scholar] [CrossRef]
- Vukmanovic-Stejic, M.; Sandhu, D.; Seidel, J.A.; Patel, N.; Sobande, T.O.; Agius, E.; Jackson, S.E.; Fuentes-Duculan, J.; Suarez-Farinas, M.; Mabbott, N.A.; et al. The Characterization of Varicella Zoster Virus-Specific T Cells in Skin and Blood during Aging. J. Invest. Dermatol. 2015, 135, 1752–1762. [Google Scholar] [CrossRef]
- Benson, D.M.J.; Bakan, C.E.; Mishra, A.; Hofmeister, C.C.; Efebera, Y.; Becknell, B.; Baiocchi, R.A.; Zhang, J.; Yu, J.; Smith, M.K.; et al. The PD-1/PD-L1 axis modulates the natural killer cell versus multiple myeloma effect: A therapeutic target for CT-011, a novel monoclonal anti-PD-1 antibody. Blood 2010, 116, 2286–2294. [Google Scholar] [CrossRef]
- Terme, M.; Ullrich, E.; Aymeric, L.; Meinhardt, K.; Desbois, M.; Delahaye, N.; Viaud, S.; Ryffel, B.; Yagita, H.; Kaplanski, G.; et al. IL-18 induces PD-1-dependent immunosuppression in cancer. Cancer Res. 2011, 71, 5393–5399. [Google Scholar] [CrossRef]
- Fanoni, D.; Tavecchio, S.; Recalcati, S.; Balice, Y.; Venegoni, L.; Fiorani, R.; Crosti, C.; Berti, E. New monoclonal antibodies against B-cell antigens: Possible new strategies for diagnosis of primary cutaneous B-cell lymphomas. Immunol. Lett. 2011, 134, 157–160. [Google Scholar] [CrossRef]
- Verschoor, C.P.; Johnstone, J.; Millar, J.; Dorrington, M.G.; Habibagahi, M.; Lelic, A.; Loeb, M.; Bramson, J.L.; Bowdish, D.M.E. Blood CD33(+)HLA-DR(-) myeloid-derived suppressor cells are increased with age and a history of cancer. J. Leukoc. Biol. 2013, 93, 633–637. [Google Scholar] [CrossRef]
- Chen, S.; Liu, H.; Su, N.; Zhang, G.; Wang, L. Myeloid-derived suppressor cells promote age-related increase of lung cancer growth via B7-H1. Exp. Gerontol. 2015, 61, 84–91. [Google Scholar] [CrossRef]
- Elias, R.; Karantanos, T.; Sira, E.; Hartshorn, K.L. Immunotherapy comes of age: Immune aging & checkpoint inhibitors. J. Geriatr. Oncol. 2017, 8, 229–235. [Google Scholar]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Bianco, A.; Campbell, S.F.M. Atezolizumab plus platinum-based regimen and bevacizumab: Is it time to consider immunotherapy in a concurrent approach for lung cancer? Transl. Cancer Res. 2018, 8 (Suppl. 2), S103–S105. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Moschos, S.J. Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2016, 45, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.; Giobbie-Hurder, A.; McCleary, N.J.; Ott, P.; Hodi, F.S.; Rahma, O. Efficacy of PD-1 & PD-L1 inhibitors in older adults: A meta-analysis. J. Immunother. Cancer 2018, 6, 26. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, Q.; Tang, X.; Xu, R.; Zhang, L.; Chen, X.; Xue, Q.; Wang, Z.; Shi, R.; Wang, F.; et al. Correlation between patients’ age and cancer immunotherapy efficacy. Oncoimmunology 2019. [Google Scholar] [CrossRef]
- Lichtenstein, M.R.L.; Nipp, R.D.; Muzikansky, A.; Goodwin, K.; Anderson, D.; Newcomb, R.A.; Gainor, J.F. Impact of Age on Outcomes with Immunotherapy in Patients with Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 14, 547–552. [Google Scholar] [CrossRef]
- Champiat, S.; Lambotte, O.; Barreau, E.; Belkhir, R.; Berdelou, A.; Carbonnel, F.; Cauquil, C.; Chanson, P.; Collins, M.; Durrbach, A.; et al. Management of immune checkpoint blockade dysimmune toxicities: A collaborative position paper. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 559–574. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Mazieres, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): A phase 2, single-arm trial. Lancet. Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef]
- Singh, H.; Kim, G.; Maher, V.E.; Beaver, J.A.; Pai-Scherf, L.H.; Balasubramaniam, S.; Theoret, M.R.; Blumenthal, G.M.; Pazdur, R. FDA subset analysis of the safety of nivolumab in elderly patients with advanced cancers. J. Clin. Oncol. 2016, 34, 10010. [Google Scholar] [CrossRef]
- Sgambato, A.; Casaluce, F.; Gridelli, C. The role of checkpoint inhibitors immunotherapy in advanced non-small cell lung cancer in the elderly. Expert Opin. Biol. Ther. 2017, 17, 565–571. [Google Scholar] [CrossRef]
- Claesson, M.J.; Cusack, S.; O’Sullivan, O.; Greene-Diniz, R.; de Weerd, H.; Flannery, E.; Marchesi, J.R.; Falush, D.; Dinan, T.; Fitzgerald, G.; et al. Composition, variability, and temporal stability of the intestinal microbiota of the elderly. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4586–4591. [Google Scholar] [CrossRef]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef]
- Claesson, M.J.; Jeffery, I.B.; Conde, S.; Power, S.E.; O’Connor, E.M.; Cusack, S.; Harris, H.M.B.; Coakley, M.; Lakshminarayanan, B.; O’Sullivan, O.; et al. Gut microbiota composition correlates with diet and health in the elderly. Nature 2012, 488, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Hua, Y.; Zeng, B.; Ning, R.; Li, Y.; Zhao, J. Gut microbiota signatures of longevity. Curr. Biol. 2016, 26, R832–R833. [Google Scholar] [CrossRef]
- Biagi, E.; Nylund, L.; Candela, M.; Ostan, R.; Bucci, L.; Pini, E.; Nikkila, J.; Monti, D.; Satokari, R.; Franceschi, C.; et al. Through ageing, and beyond: Gut microbiota and inflammatory status in seniors and centenarians. PLoS ONE 2010, 5, e10667. [Google Scholar] [CrossRef]
- Gopalakrishnan, V.; Spencer, C.N.; Nezi, L.; Reuben, A.; Andrews, M.C.; Karpinets, T.V.; Prieto, P.A.; Vicente, D.; Hoffman, K.; Wei, S.C.; et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science 2018, 359, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.P.M.; Alou, M.T.; Daillere, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 2018, 359, 91–97. [Google Scholar] [CrossRef]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.-L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science 2018, 359, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Stingele, F.; Corthesy, B.; Kusy, N.; Porcelli, S.A.; Kasper, D.L.; Tzianabos, A.O. Zwitterionic polysaccharides stimulate T cells with no preferential V beta usage and promote anergy, resulting in protection against experimental abscess formation. J. Immunol. 2004, 172, 1483–1490. [Google Scholar] [CrossRef]
- Ilag, L.L. Are Long-Chain Polyunsaturated Fatty Acids the Link between the Immune System and the Microbiome towards Modulating Cancer? Medicines 2018, 5, 102. [Google Scholar] [CrossRef]
- Guesdon, W.; Kosaraju, R.; Brophy, P.; Clark, A.; Dillingham, S.; Aziz, S.; Moyer, F.; Willson, K.; Dick, J.R.; Patil, S.P.; et al. Effects of fish oils on ex vivo B-cell responses of obese subjects upon BCR/TLR stimulation: A pilot study. J. Nutr. Biochem. 2018, 53, 72–80. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MoAbs Targeting PD-1/PD-L1 | Clinical Trial | Target Population | OS (HR 95%IC) | Median Age in Treated Arm (Range) |
|---|---|---|---|---|
| Nivolumab monotherapy | CheckMate017 | Squamous NSCLC | 62.0 (39–85) | |
| <65 yr | 0.62 (0.44–0.89) | |||
| ≥65 <75 yr | 0.51 (0.32–0.82) | |||
| ≥75 yr | 1.76 (0.77–4.05) | |||
| Nivolumab monotherapy | CheckMate057 | Nonsquamous NSCLC | 61.0 (37–84) | |
| <65 yr | 0.81 (0.62–1.04) | |||
| ≥65 <75 yr | 0.63 (0.45–0.89) | |||
| ≥75 yr | 0.90 (0.43–1.87) | |||
| Pembrolizumab monotherapy | KEYNOTE-024 | Nonsquamous and squamous NSCLC | 64.5 (33–90) | |
| < 65 yr | 0.61 (0.40–0.92) | |||
| ≥65 yr | 0.45 (0.29–0.70) | |||
| Pembrolizumab monotherapy | KEYNOTE-010 | Nonsquamous and squamous NSCLC | 63.0 (56–69) | |
| < 65 yr | 0·63 (0·50–0·79) | |||
| ≥65 yr | 0·76 (0·57–1·02) | |||
| Atezolizumab monotherapy | OAK | Nonsquamous and squamous NSCLC | 63.0 (33–82) | |
| < 65 yr | 0·80 (0·64–1·00) | |||
| ≥65 yr | 0·66 (0·52–0·83) | |||
| Durvalumab monotherapy | PACIFIC | Nonsquamous and squamous NSCLC | 64.0 (31–84) | |
| < 65 yr | 0.62 (0.44–0.86) | |||
| ≥65 yr | 0.76 (0.55–1.06) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrotta, F.; Rocco, D.; Vitiello, F.; De Palma, R.; Guerra, G.; De Luca, A.; Navani, N.; Bianco, A. Immune Checkpoint Blockade for Advanced NSCLC: A New Landscape for Elderly Patients. Int. J. Mol. Sci. 2019, 20, 2258. https://doi.org/10.3390/ijms20092258
Perrotta F, Rocco D, Vitiello F, De Palma R, Guerra G, De Luca A, Navani N, Bianco A. Immune Checkpoint Blockade for Advanced NSCLC: A New Landscape for Elderly Patients. International Journal of Molecular Sciences. 2019; 20(9):2258. https://doi.org/10.3390/ijms20092258
Chicago/Turabian StylePerrotta, Fabio, Danilo Rocco, Fabiana Vitiello, Raffaele De Palma, Germano Guerra, Antonio De Luca, Neal Navani, and Andrea Bianco. 2019. "Immune Checkpoint Blockade for Advanced NSCLC: A New Landscape for Elderly Patients" International Journal of Molecular Sciences 20, no. 9: 2258. https://doi.org/10.3390/ijms20092258
APA StylePerrotta, F., Rocco, D., Vitiello, F., De Palma, R., Guerra, G., De Luca, A., Navani, N., & Bianco, A. (2019). Immune Checkpoint Blockade for Advanced NSCLC: A New Landscape for Elderly Patients. International Journal of Molecular Sciences, 20(9), 2258. https://doi.org/10.3390/ijms20092258