Systematic Review: Allogenic Use of Stromal Vascular Fraction (SVF) and Decellularized Extracellular Matrices (ECM) as Advanced Therapy Medicinal Products (ATMP) in Tissue Regeneration

 ,
,  ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
- MSCs are disc-adherent in standard cultures;
- MSCs differentiate in adipocytes, chondroblasts, and osteoblasts;
- MSCs express CD73, CD90, and CD105;
- MSCs do not express CD11b, CD14, CD19, CD34, CD45, CD79, c-kit, and human leukocyte antigen-DR.
- Fat tissue could be obtained by selected donors, checked, and stored;
- On-demand, fat tissue, and in particular his SVF portion, could be used for autologous or allogenic use. In the last case, fat tissue should be undergone to decellularize so as to obtain a scaffold represented by the decellularized ECM;
- Decellularized ECM should be re-cellularized with the ASCs of the recipient.
2. Results
2.1. Description of Included Studies
2.2. Allogenic Human Clinical Use of Adipose Stem Cells (ASCs)
2.3. Critrical Assessment of Study Design
2.4. Side Effects
3. Discussion
4. Methods
4.1. Rules and Institutional Guidelines on How to Handle Adipose Tissue and Stromal Vascular Fraction
- Tissues and/or cells that have undergone significant handling;
- Tissues and/or cells that have not undergone the manipulations (minimal) listed in Annex I (centrifugation, filtration, cutting, separation, shaping, grinding, immersion in antimicrobial suspension, immersion in antibiotic, sterilization, vitrification irradiation, cell purification, cell concentration, freeze-drying, freezing, cryopreservation);
- Tissues and/or cells not intended to be used for the same/the same essential functions in the recipient and donor.
- sCTMP and TEP contain or consist of engineered tissues and/or cells. To be considered “engineered”, tissues or cells must meet at least one of the following criteria:
- Extensive manipulation (cell culture based on expansion of cells, genetic modification of these, their differentiation/stimulation with Growth Factors (GFs);
- Various essential functions (not homologous use).
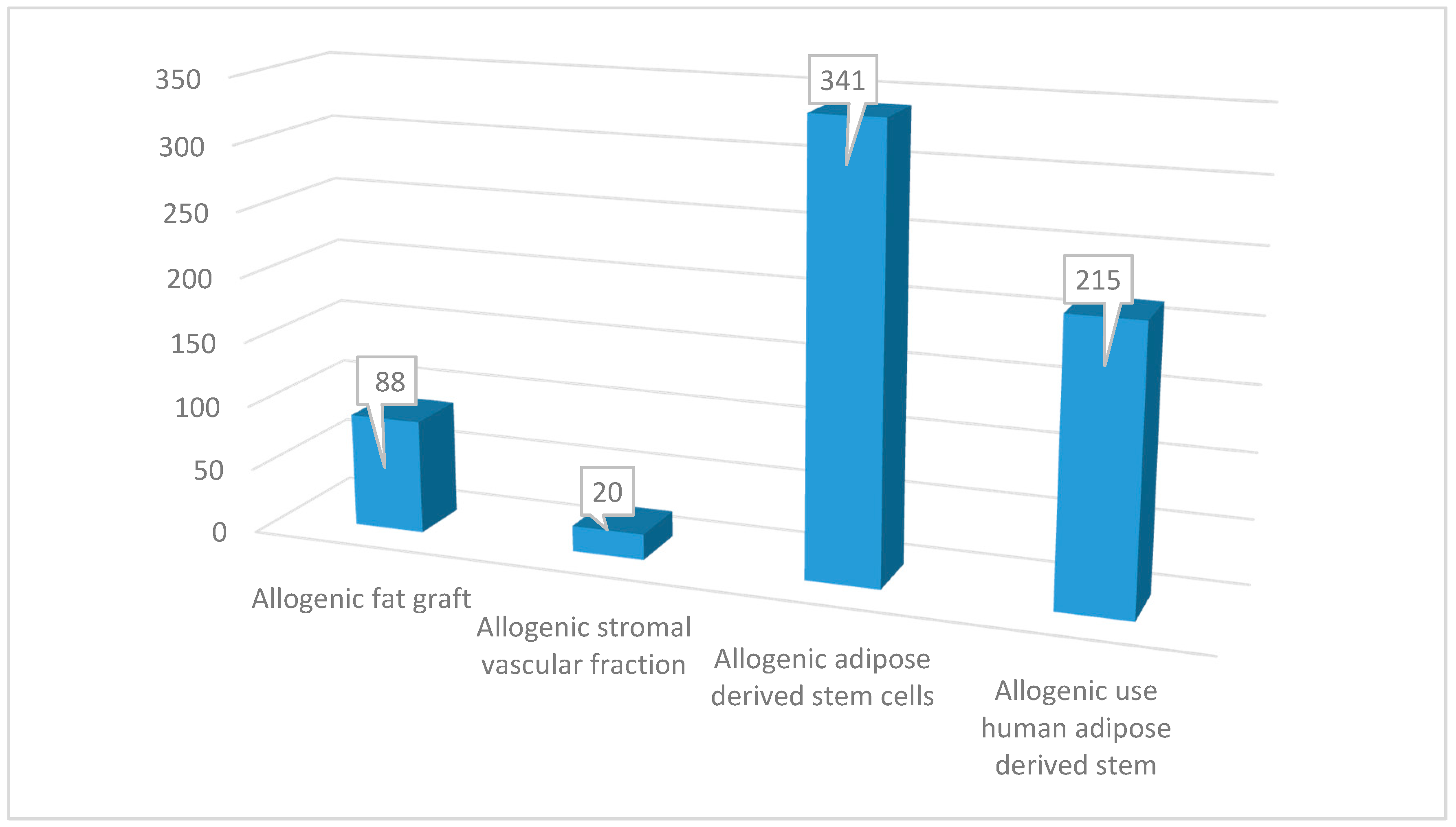
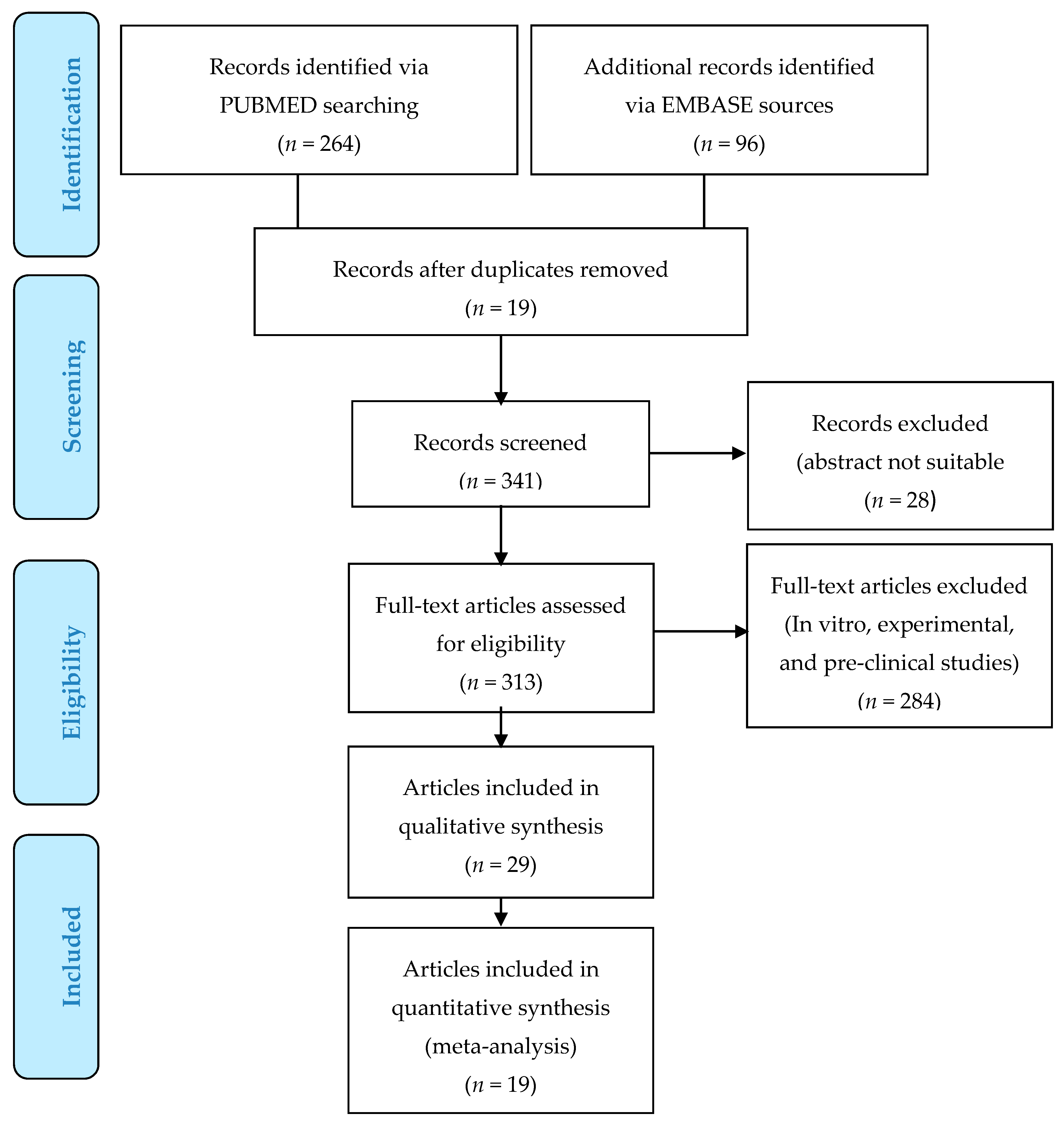
4.2. Search Strategy
4.2.1. Study Assessment
4.2.2. Study Selection
4.2.3. Data Extraction
4.2.4. Outcome Measures
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SVFs | Stromal Vascular Fraction Cells |
| ASCs | Adipose-Derived Stem Cells |
| SVF | Stromal Vascular Fraction |
| ISCT | International Society for Cellular Therapy |
| MSCs | Mesenchymal Stem Cells |
| HAT | Human Adipose Tissue |
| COVID-19 | Coronavirus Disease 2019 |
| UC | Umbilical-Cord |
| BM | Bone-Marrow |
| BM-MSCs | Bone-Marrow MSCs |
| UC-MSCs | Umbilical-Cord MSCs |
| AD | Adipose Tissue |
| AD-MSCs | Adipose-Derived Mesenchymal Stem Cells |
| ECM | Extracellular Matrix |
| FDA | Food and Drug Administration |
| EMA | European Medical Agency |
| CAT | Committee for Advanced Therapies |
| EC | European Parliament |
| GMP | Good Manufacturing Practices |
| GCP | Good Clinical Practices |
| sCTMP | Somatic Cell Therapy Medicines |
| TEP | Tissue Engineering products |
| ATMPs | Advanced Therapy Medicinal Products |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| PRISMA | Preferred Reporting for Items for Systematic Reviews and Meta-Analyses |
| EBM | Evidence-Based Medicine |
| OCEBM | Oxford Centre for Evidence-Based Medicine |
| ARDS | Acute Respiratory Distress Syndrome |
| haMPCs | allogenic human Adipose-Derived Mesenchymal Progenitor Cells |
| e-ASC | expanded Adipose-derived Stem Cells |
| RA | Rheumatoid Arthritis |
| OA | Osteoarthritic |
| e-a-MSCs | expanded-allogenic Mesenchymal Stem Cells |
| CSCC_ASC | Cardiology Stem Cell Centre Adipose-derived Stromal Cell |
| IHF | Ischemic Heart Failure |
| GvHD | Graft-versus-Host disease |
| ADSCs | Adipose-derived Stromal Cells |
| NRVMs | Neonatal Rat Ventricular Myocytes |
| HC | Hypertrophic cartilage |
| LE | Lateral Epicondylosis |
| VAS | Visual Analog Scale |
| LPS | Lipopolysaccharide |
References
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The international society for cellular therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; De Angelis, B.; Pasin, M.; Cervelli, G.; Curcio, C.B.; Floris, M.; Di Pasquali, C.; Bocchini, I.; Balzani, A.; Nicoli, F.; et al. Adipose-derived stromal vascular fraction cells and platelet-rich plasma: Basic and clinical evaluation for cell-based therapies in patients with scars on the face. J. Craniofac. Surg. 2014, 25, 267–272. [Google Scholar] [CrossRef]
- Gentile, P.; Piccinno, M.S.; Calabrese, C. Characteristics and Potentiality of Human Adipose-Derived Stem Cells (hASCs) Obtained from Enzymatic Digestion of Fat Graft. Cells 2019, 8, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, P.; Sterodimas, A. Adipose Stem Cells (ASCs) and Stromal Vascular Fraction (SVF) as a Potential Therapy in Combating (COVID-19)-Disease. Aging Dis. 2020, 11, 465–469. [Google Scholar] [CrossRef]
- Leng, Z.; Zhu, R.; Hou, W.; Feng, Y.; Yang, Y.; Han, Q.; Shan, G.; Meng, F.; Du, D.; Wang, S.; et al. Transplantation of ACE2-mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis. 2020, 11, 216–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hass, R.; Kasper, C.; Bohm, S.; Jacobs, R. Different populations and sources of human mesenchymal stem cells (MSC): A comparison of adult and neonatal tissue-derived MSC. Cell Commun. Signal. 2011, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Cervelli, V.; Bocchini, I.; Di Pasquali, C.; De Angelis, B.; Cervelli, G.; Curcio, C.B.; Orlandi, A.; Scioli, M.G.; Tati, E.; Delogu, P.; et al. P.R.L. platelet rich lipotransfert: Our experience and current state of art in the combined use of fat and PRP. BioMed Res. Int. 2013, 2013, 434191. [Google Scholar] [CrossRef] [Green Version]
- Cervelli, V.; Gentile, P. Use of cell fat mixed with platelet gel in progressive hemifacial atrophy. Aesthetic Plast. Surg. 2009, 33, 22–27. [Google Scholar] [CrossRef]
- Turner, A.; Abu-Ghname, A.; Davis, M.J.; Winocour, S.J.; Hanson, S.E.; Chu, C.K. Fat grafting in breast reconstruction. Semin. Plast. Surg. 2020, 34, 17–23. [Google Scholar] [CrossRef]
- Gentile, P.; Garcovich, S. Concise Review: Adipose-Derived Stem Cells (ASCs) and Adipocyte-Secreted Exosomal microRNA (A-SE-miR) Modulate Cancer Growth and promote Wound Repair. J. Clin. Med. 2019, 8, 855. [Google Scholar] [CrossRef] [Green Version]
- Gentile, P. Autologous Cellular Method Using Micrografts of Human Adipose Tissue Derived Follicle Stem Cells in Androgenic Alopecia. Int. J. Mol. Sci. 2019, 20, 3446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, M.J.; Perdanasari, A.T.; Abu-Ghname, A.; Gonzalez, S.R.; Chamata, E.; Rammos, C.K.; Winocour, S.J. Application of Fat Grafting in Cosmetic Breast Surgery. Semin. Plast. Surg. 2020, 34, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Scioli, M.G.; Bielli, A.; Gentile, P.; Cervelli, V.; Orlandi, A. Combined treatment with platelet-rich plasma and insulin favours chondrogenic and osteogenic differentiation of human adipose-derived stem cells in three-dimensional collagen scaffolds. J. Tissue Eng. Regen. Med. 2017, 11, 2398–2410. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Tanaka, M. Designing Smart Biomaterials for Tissue Engineering. Int. J. Mol. Sci. 2017, 19, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryksin, A.V.; Brown, A.C.; Baksh, M.M.; Finn, M.G.; Barker, T.H. Learning from nature—Novel synthetic biology approaches for biomaterial design. Acta Biomater. 2014, 10, 1761–1769. [Google Scholar] [CrossRef] [Green Version]
- Dan, P.; Velot, É.; Francius, G.; Menu, P.; Decot, V. Human-derived extracellular matrix from Wharton’s jelly: An untapped substrate to build up a standardized and homogeneous coating for vascular engineering. Acta Biomater. 2017, 48, 227–237. [Google Scholar] [CrossRef]
- Schenke-Layland, K.; Nerem, R.M. In vitro human tissue models—Moving towards personalized regenerative medicine. Adv. Drug Deliv. Rev. 2011, 63, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Ruan, J.; Tang, H.; Li, J.; Shi, Y.; Li, M.; Li, S.; Xu, C.; Lu, Q.; Dai, C. Multi-compositional MRI evaluation of repair cartilage in knee osteoarthritis with treatment of allogeneic human adipose-derived mesenchymal progenitor cells. Stem Cell Res. Ther. 2019, 10, 308. [Google Scholar] [CrossRef] [Green Version]
- Kuah, D.; Sivell, S.; Longworth, T.; James, K.; Guermazi, A.; Cicuttini, F.; Wang, Y.; Craig, S.; Comin, G.; Robinson, D.; et al. Safety, tolerability and efficacy of intra-articular Progenza in knee osteoarthritis: A randomized double-blind placebo-controlled single ascending dose study. J. Transl. Med. 2018, 16, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvaro-Gracia, J.M.; Jover, J.A.; García-Vicuña, R.; Carreño, L.; Alonso, A.; Marsal, S.; Blanco, F.; Martínez-Taboada, V.M.; Taylor, P.; Martín-Martín, C.; et al. Intravenous administration of expanded allogeneic adipose-derived mesenchymal stem cells in refractory rheumatoid arthritis (Cx611): Results of a multicentre, dose escalation, randomised, single-blind, placebo-controlled phase Ib/IIa clinical trial. Ann. Rheum. Dis. 2017, 76, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Manferdini, C.; Maumus, M.; Gabusi, E.; Piacentini, A.; Filardo, G.; Peyrafitte, J.A.; Jorgensen, C.; Bourin, P.; Fleury-Cappellesso, S.; Facchini, A.; et al. Adipose-derived mesenchymal stem cells exert antiinflammatory effects on chondrocytes and synoviocytes from osteoarthritis patients through prostaglandin E2. Arthritis Rheum. 2013, 65, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Dige, A.; Hougaard, H.T.; Agnholt, J.; Pedersen, B.G.; Tencerova, M.; Kassem, M.; Krogh, K.; Lundby, L. Efficacy of Injection of Freshly Collected Autologous Adipose Tissue into Perianal Fistulas in Patients with Crohn’s Disease. Gastroenterology 2019, 156, 2208–2216. [Google Scholar] [CrossRef] [Green Version]
- Panés, J.; García-Olmo, D.; Van Assche, G.; Colombel, J.F.; Reinisch, W.; Baumgart, D.C.; Dignass, A.; Nachury, M.; Ferrante, M.; Kazemi-Shirazi, L.; et al. Long-term Efficacy and Safety of Stem Cell Therapy (Cx601) for Complex Perianal Fistulas in Patients with Crohn’s Disease. Gastroenterology 2018, 154, 1334–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panés, J.; García-Olmo, D.; Van Assche, G.; Colombel, J.F.; Reinisch, W.; Baumgart, D.C.; Dignass, A.; Nachury, M.; Ferrante, M.; Kazemi-Shirazi, L.; et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: A phase 3 randomised, double-blind controlled trial. Lancet 2016, 388, 1281–1290. [Google Scholar] [CrossRef]
- Park, K.J.; Ryoo, S.B.; Kim, J.S.; Kim, T.I.; Baik, S.H.; Kim, H.J.; Lee, K.Y.; Kim, M.; Kim, W.H. Allogeneic adipose-derived stem cells for the treatment of perianal fistula in Crohn’s disease: A pilot clinical trial. Colorectal Dis. 2016, 18, 468–476. [Google Scholar] [CrossRef]
- de la Portilla, F.; Alba, F.; García-Olmo, D.; Herrerías, J.M.; González, F.X.; Galindo, A. Expanded allogeneic adipose-derived stem cells (eASCs) for the treatment of complex perianal fistula in Crohn’s disease: Results from a multicenter phase I/IIa clinical trial. Int. J. Colorectal Dis. 2013, 28, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Kastrup, J.; Haack-Sørensen, M.; Juhl, M.; Harary Søndergaard, R.; Follin, B.; Drozd Lund, L.; Mønsted Johansen, E.; Ali Qayyum, A.; Bruun Mathiasen, A.; Jørgensen, E.; et al. Cryopreserved Off-the-Shelf Allogeneic Adipose-Derived Stromal Cells for Therapy in Patients with Ischemic Heart Disease and Heart Failure-A Safety Study. Stem Cells Transl. Med. 2017, 6, 1963–1971. [Google Scholar] [CrossRef]
- Jurado, M.; De La Mata, C.; Ruiz-García, A.; López-Fernández, E.; Espinosa, O.; Remigia, M.J.; Moratalla, L.; Goterris, R.; García-Martín, P.; Ruiz-Cabello, F.; et al. Adipose tissue-derived mesenchymal stromal cells as part of therapy for chronic graft-versus-host disease: A phase I/II study. Cytotherapy 2017, 19, 927–936. [Google Scholar] [CrossRef]
- Tsai, Y.A.; Liu, R.S.; Lirng, J.F.; Yang, B.H.; Chang, C.H.; Wang, Y.C.; Wu, Y.S.; Ho, J.H.; Lee, O.K.; Soong, B.W. Treatment of Spinocerebellar Ataxia With Mesenchymal Stem Cells: A Phase I/IIa Clinical Study. Cell Transplant. 2017, 26, 503–512. [Google Scholar] [CrossRef] [Green Version]
- Díez-Tejedor, E.; Gutiérrez-Fernández, M.; Martínez-Sánchez, P.; Rodríguez-Frutos, B.; Ruiz-Ares, G.; Lara, M.L.; Gimeno, B.F. Reparative therapy for acute ischemic stroke with allogeneic mesenchymal stem cells from adipose tissue: A safety assessment: A phase II randomized, double-blind, placebo-controlled, single-center, pilot clinical trial. J. Stroke Cerebrovasc. Dis. 2014, 23, 2694–2700. [Google Scholar] [CrossRef] [PubMed]
- Ten Sande, J.N.; Smit, N.W.; Parvizi, M.; van Amersfoorth, S.C.; Plantinga, J.A.; van Dessel, P.F.; de Bakker, J.M.; Harmsen, M.C.; Coronel, R. Differential Mechanisms of Myocardial Conduction Slowing by Adipose Tissue-Derived Stromal Cells Derived from Different Species. Stem Cells Transl. Med. 2017, 6, 22–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todorov, A.; Kreutz, M.; Haumer, A.; Scotti, C.; Barbero, A.; Bourgine, P.E.; Scherberich, A.; Jaquiery, C.; Martin, I. Fat-Derived Stromal Vascular Fraction Cells Enhance the Bone-Forming Capacity of Devitalized Engineered Hypertrophic Cartilage Matrix. Stem Cells Transl. Med. 2016, 5, 1684–1694. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kim, W.; Lim, C.; Chung, S.G. Treatment of Lateral Epicondylosis by Using Allogeneic Adipose-Derived Mesenchymal Stem Cells: A Pilot Study. Stem Cells 2015, 33, 2995–3005. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Huang, L.; Tong, H.; Shu, Q.; Hu, Y.; Ge, M.; Deng, K.; Zhang, L.; Zou, B.; Cheng, B.; et al. Treatment of acute respiratory distress syndrome with allogeneic adipose-derived mesenchymal stem cells: A randomized, placebo-controlled pilot study. Respir. Res. 2014, 15, 39. [Google Scholar] [CrossRef] [Green Version]
- Rozier, P.; Maria, A.; Goulabchand, R.; Jorgensen, C.; Guilpain, P.; Noël, D. Mesenchymal Stem Cells in Systemic Sclerosis: Allogenic or Autologous Approaches for Therapeutic Use? Front. Immunol. 2018, 9, 2938. [Google Scholar] [CrossRef] [Green Version]
- Porzionato, A.; Stocco, E.; Barbon, S.; Grandi, F.; Macchi, V.; De Caro, R. Tissue-Engineered Grafts from Human Decellularized Extracellular Matrices: A Systematic Review and Future Perspectives. Int. J. Mol. Sci. 2018, 19, 4117. [Google Scholar] [CrossRef] [Green Version]
- Perlee, D.; van Vught, L.A.; Scicluna, B.P.; Maag, A.; Lutter, R.; Kemper, E.M.; van’t Veer, C.; Punchard, M.A.; González, J.; Richard, M.P.; et al. Intravenous Infusion of Human Adipose Mesenchymal Stem Cells Modifies the Host Response to Lipopolysaccharide in Humans: A Randomized, Single-Blind, Parallel Group, Placebo Controlled Trial. Stem Cells 2018, 36, 1778–1788. [Google Scholar] [CrossRef] [Green Version]
- Pizzicannella, J.; Gugliandolo, A.; Orsini, T.; Fontana, A.; Ventrella, A.; Mazzon, E.; Bramanti, P.; Diomede, F.; Trubiani, O. Engineered extracellular vesicles from human periodontal-ligament stem cells increase VEGF/VEGFR2 expression during bone regeneration. Front. Physiol. 2019, 10, 512. [Google Scholar] [CrossRef] [Green Version]
- Trubiani, O.; Ballerini, P.; Murmura, G.; Pizzicannella, J.; Giuliani, P.; Buccella, S.; Caputi, S. Toll-like receptor 4 expression, interleukin-6, -8 and Ccl-20 release, and NF-KB translocation in human periodontal ligament mesenchymal stem cells stimulated with LPS-P. gingivalis. Eur. J. Inflamm. 2012, 10, 81–89. [Google Scholar] [CrossRef]
- Schücklenk, U.; Ashcroft, R. International Research Ethics. Bioethics 2000, 14, 158–172. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, U.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentile, P.; Sterodimas, A.; Pizzicannella, J.; Dionisi, L.; De Fazio, D.; Calabrese, C.; Garcovich, S. Systematic Review: Allogenic Use of Stromal Vascular Fraction (SVF) and Decellularized Extracellular Matrices (ECM) as Advanced Therapy Medicinal Products (ATMP) in Tissue Regeneration. Int. J. Mol. Sci. 2020, 21, 4982. https://doi.org/10.3390/ijms21144982
Gentile P, Sterodimas A, Pizzicannella J, Dionisi L, De Fazio D, Calabrese C, Garcovich S. Systematic Review: Allogenic Use of Stromal Vascular Fraction (SVF) and Decellularized Extracellular Matrices (ECM) as Advanced Therapy Medicinal Products (ATMP) in Tissue Regeneration. International Journal of Molecular Sciences. 2020; 21(14):4982. https://doi.org/10.3390/ijms21144982
Chicago/Turabian StyleGentile, Pietro, Aris Sterodimas, Jacopo Pizzicannella, Laura Dionisi, Domenico De Fazio, Claudio Calabrese, and Simone Garcovich. 2020. "Systematic Review: Allogenic Use of Stromal Vascular Fraction (SVF) and Decellularized Extracellular Matrices (ECM) as Advanced Therapy Medicinal Products (ATMP) in Tissue Regeneration" International Journal of Molecular Sciences 21, no. 14: 4982. https://doi.org/10.3390/ijms21144982
APA StyleGentile, P., Sterodimas, A., Pizzicannella, J., Dionisi, L., De Fazio, D., Calabrese, C., & Garcovich, S. (2020). Systematic Review: Allogenic Use of Stromal Vascular Fraction (SVF) and Decellularized Extracellular Matrices (ECM) as Advanced Therapy Medicinal Products (ATMP) in Tissue Regeneration. International Journal of Molecular Sciences, 21(14), 4982. https://doi.org/10.3390/ijms21144982