Effect of a Cognitive Training Program on the Platelet APP Ratio in Patients with Alzheimer’s Disease


Abstract
:1. Introduction
2. Results
2.1. Baseline Assessment
2.2. Effects of the Cognitive Training Intervention
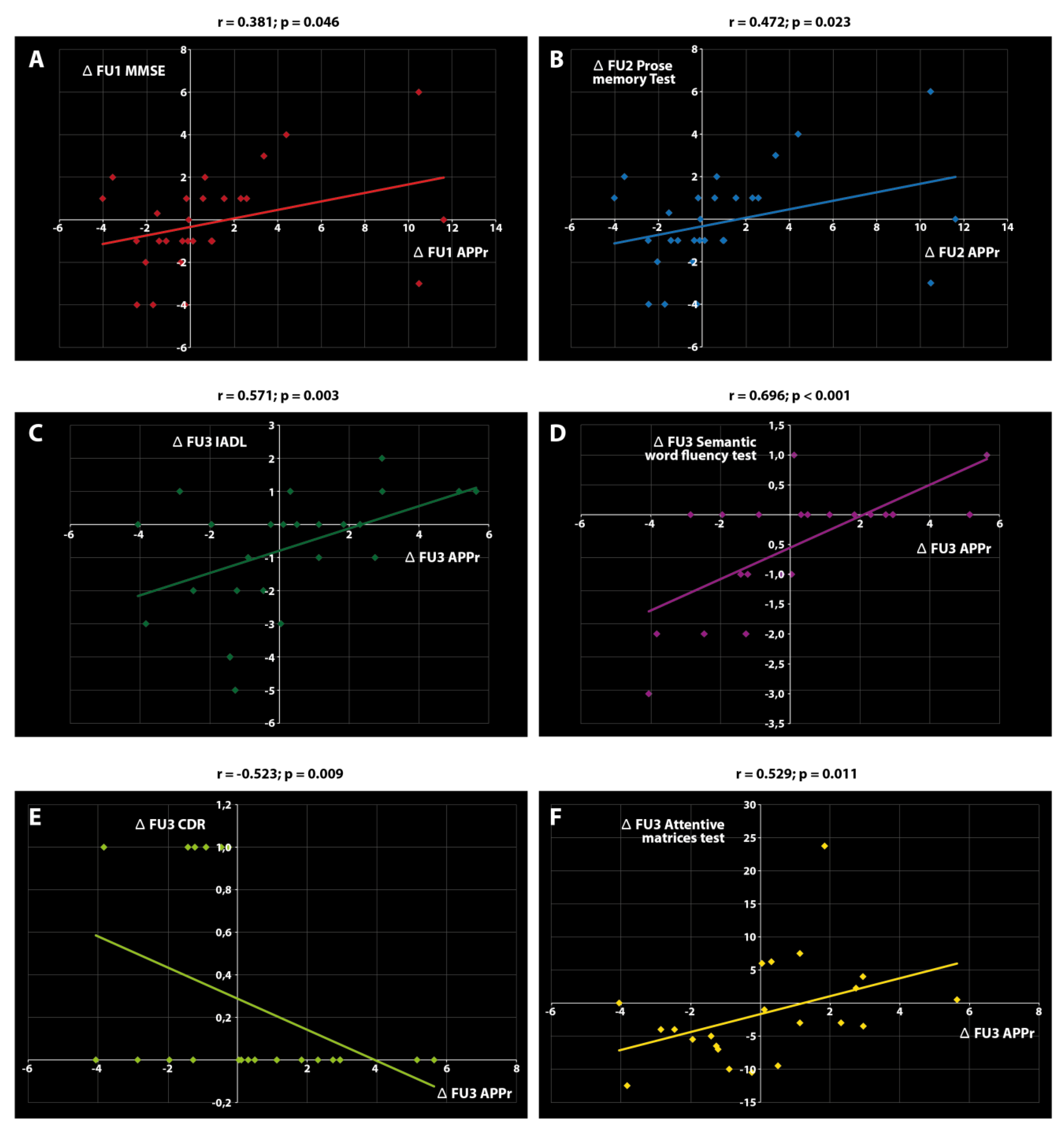
2.3. Associations between APPr and Clinical Variables
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
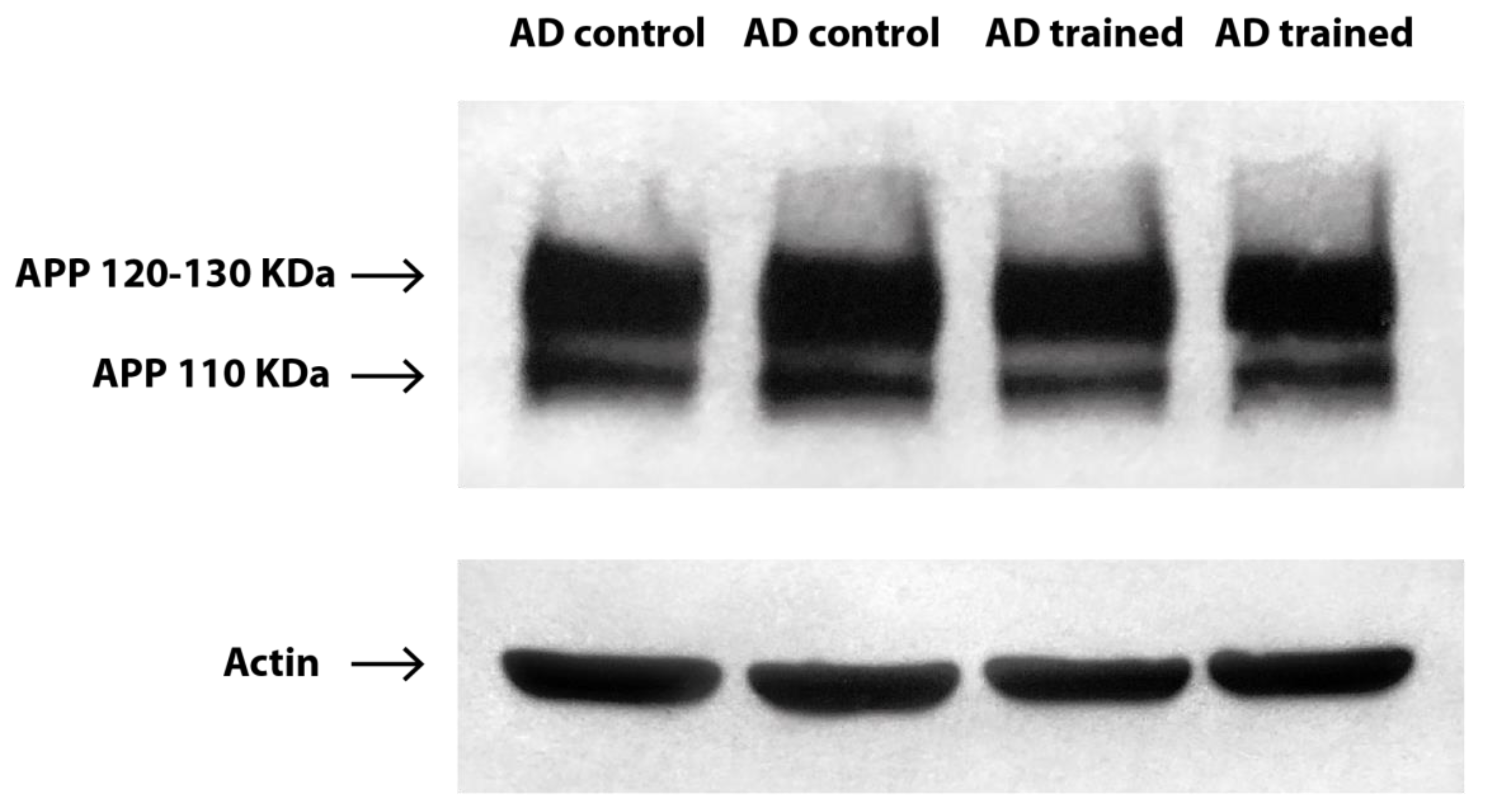
4.2. Western Blot Analysis and Calculation of the APP Ratio
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| APP | Amyloid precursor protein |
| APPr | Amyloid precursor protein ratio |
| FU1 | Follow-up 1 |
| FU2 | Follow-up 2 |
| FU3 | Follow-up 3 |
| MMSE | Mini Mental State Examination |
| IADL | Instrumental Activities of Daily Living |
| CDR | Clinical Dementia Rating |
| SEM | Standard Error of the Mean |
| sAPPα | Soluble amyloid precursor protein α |
| BACE1 | β -secretase 1 |
| PRP | Platelet-Rich Plasma |
| EDTA | Ethylenediaminetetraacetic acid |
| PMSF | Phenylmethylsulfonyl fluoride |
| PVDF | Polyvinylidene fluoride |
References
- Gates, N.J.; Sachdev, P. Is cognitive training an effective treatment for preclinical and early Alzheimer’s disease? J. Alzheimers Dis. 2014, 42, S551–S559. [Google Scholar] [CrossRef] [Green Version]
- Vemuri, P.; Fields, J.; Peter, J.; Klöppel, S. Cognitive interventions in Alzheimer’s and Parkinson’s diseases: Emerging mechanisms and role of imaging. Curr. Opin. Neurol. 2016, 29, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Train the Brain Consortium. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabir, M.T.; Uddin, M.S.; Mamun, A.A.; Jeandet, P.; Aleya, L.; Mansouri, R.A.; Ashraf, G.M.; Mathew, B.; Bin-Jumah, M.N.; Abdel-Daim, M.M. Combination Drug Therapy for the Management of Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 3272. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Woods, R.T.; Moniz Cook, E.D.; Orrell, M.; Spector, A. Cognitive rehabilitation and cognitive training for early-stage Alzheimer’s disease and vascular dementia. Cochrane Database Syst. Rev. 2003, 4, CD003260. [Google Scholar] [CrossRef]
- Balietti, M.; Giuli, C.; Fattoretti, P.; Fabbietti, P.; Papa, R.; Postacchini, D.; Conti, F. Effect of a Comprehensive Intervention on Plasma BDNF in Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2017, 57, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef]
- Aguirre, E.; Woods, R.T.; Spector, A.; Orrell, M. Cognitive stimulation for dementia: A systematic review of the evidence of effectiveness from randomised controlled trials. Ageing Res. Rev. 2013, 12, 253–262. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Jones, M.; Wen, W.; Rae, C.; Graham, S.; Shnier, R.; Sachdev, P. Memory training alters hippocampal neurochemistry in healthy elderly. Neuroreport 2003, 14, 1333–1337. [Google Scholar] [CrossRef]
- Nithianantharajah, J.; Hannan, A. Enriched environments, experience dependent plasticity and disorders of the nervous system. Nat. Rev. Neurosci. 2006, 7, 697–709. [Google Scholar] [CrossRef]
- Di Garbo, A.; Mainardi, M.; Chillemi, S.; Maffei, L.; Caleo, M. Environmental enrichment modulates cortico-cortical interactions in the mouse. PLoS ONE 2011, 6, e25285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suo, C.; Valenzuela, M.J. Neuroimaging outcomes of brain training trials. In Neuroimaging-Cognitive and Clinical Neuroscience; Bright, P., Ed.; InTech: Rijeka, Croatia, 2012; pp. 417–430. [Google Scholar]
- Sale, A.; Berardi, N.; Maffei, L. Environment and brain plasticity: Towards an endogenous pharmacotherapy. Physiol. Rev. 2014, 94, 189–234. [Google Scholar] [CrossRef] [PubMed]
- Bruel-Jungerman, E.; Davis, S.; Laroche, S. Brain plasticity mechanisms and memory: A party of four. Neuroscientist 2007, 13, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.B.; Aslan, S.; Spence, J.S.; Hart, J.J., Jr.; Bartz, E.K.; Didehbani, N.; Keebler, M.W.; Gardner, C.M.; Strain, J.F.; DeFina, L.F.; et al. Neural mechanisms of brain plasticity with complex cognitive training in healthy seniors. Cereb. Cortex 2015, 25, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, B.; Yang, L.; Guo, Q.; Aithmitti, N.; Songyang, Z.; Zheng, H. Presynaptic and postsynaptic interaction of the amyloid precursor protein promotes peripheral and central synaptogenesis. J. Neurosci. 2009, 29, 10788–10801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Strooper, B.; Annaert, W. Proteolytic processing and cell biological functions of the amyloid precursor protein. J. Cell Sci. 2000, 113, 1857–1870. [Google Scholar]
- Herms, J.; Anliker, B.; Heber, S.; Ring, S.; Fuhrmann, M.; Kretzschmar, H.; Sisodia, S.; Muller, U. Cortical dysplasia resembling human type 2 lissencephaly in mice lacking all three APP family members. EMBO J. 2004, 23, 4106–4115. [Google Scholar] [CrossRef]
- Weyer, S.W.; Zagrebelsky, M.; Herrmann, U.; Hick, M.; Ganss, L.; Gobbert, J.; Gruber, M.; Altmann, C.; Korte, M.; Deller, T.; et al. Comparative analysis of single and combined APP/APLP knockouts reveals reduced spine density in APP-KO mice that is prevented by APPsα expression. Acta Neuropathol. Commun. 2014, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Schrenk-Siemens, K.; Perez-Alcala, S.; Richter, J.; Lacroix, E.; Rahuel, J.; Korte, M.; Müller, U.; Barde, Y.A.; Bibel, M. Embryonic stem cell-derived neurons as a cellular system to study gene function: Lack of amyloid precursor proteins APP and APLP2 leads to defective synaptic transmission. Stem Cells 2008, 26, 2153–2163. [Google Scholar] [CrossRef]
- Müller, U.C.; Zheng, H. Physiological functions of APP family proteins. Cold Spring Harb. Perspect. Med. 2012, 2, a006288. [Google Scholar] [CrossRef] [Green Version]
- Hick, M.; Herrmann, U.; Weyer, S.W.; Mallm, J.P.; Tschäpe, J.A.; Borgers, M.; Mercken, M.; Roth, F.C.; Draguhn, A.; Slomianka, L.; et al. Acute function of secreted amyloid precursor protein fragment APPsα in synaptic plasticity. Acta Neuropathol. 2015, 129, 21–37. [Google Scholar] [CrossRef]
- Van Nostrand, W.E.; Schmaier, A.H.; Farrow, J.S.; Cunningham, D.D. Protease nexin-II (amyloid beta-protein precursor): A platelet alpha-granule protein. Science 1990, 248, 745–748. [Google Scholar] [CrossRef]
- Humpel, C. Platelets: Their Potential Contribution to the Generation of Beta-amyloid Plaques in Alzheimer’s Disease. Curr. Neurovasc. Res. 2017, 14, 290–298. [Google Scholar] [CrossRef]
- Rosenberg, R.N.; Baskin, F.; Fosmire, J.A.; Risser, R.; Adams, P.; Svetlik, D.; Honig, L.S.; Cullum, C.M.; Weiner, M.F. Altered amyloid protein processing in platelets of patients with Alzheimer disease. Arch. Neurol. 1997, 54, 139–144. [Google Scholar] [CrossRef]
- Srisawat, C.; Junnu, S.; Peerapittayamongkol, C.; Futrakul, A.; Soi-ampornkul, R.; Senanarong, V.; Praditsuwan, R.; Assantachai, P.; Neungton, N. The platelet amyloid precursor protein ratio as a diagnostic marker for Alzheimer’s disease in Thai patients. J. Clin. Neurosci. 2013, 20, 644–648. [Google Scholar] [CrossRef]
- Shi, Y.; Gu, L.; Alsharif, A.A.; Zhang, Z. The Distinction of Amyloid-β Protein Precursor (AβPP) Ratio in Platelet Between Alzheimer’s Disease Patients and Controls: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2017, 59, 1037–1044. [Google Scholar] [CrossRef]
- Baskin, F.; Rosenberg, R.N.; Iyer, L.; Hynan, L.; Cullum, C.M. Platelet APP isoform ratios correlate with declining cognition in AD. Neurology 2000, 54, 1907–1909. [Google Scholar] [CrossRef]
- Borroni, B.; Colciaghi, F.; Pastorino, L.; Archetti, S.; Corsini, P.; Cattabeni, F.; Di Luca, M.; Padovani, A. ApoE genotype influences the biological effect of donepezil on APP metabolism in Alzheimer disease: Evidence from a peripheral model. Eur. Neuropsychopharmacol. 2002, 12, 195–200. [Google Scholar] [CrossRef]
- Liu, H.C.; Chi, C.W.; Ko, S.Y.; Wang, H.C.; Hong, C.J.; Lin, K.N.; Wang, P.N.; Liu, T.Y. Cholinesterase inhibitor affects the amyloid precursor protein isoforms in patients with Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2005, 19, 345–348. [Google Scholar] [CrossRef]
- Casoli, T.; Giuli, C.; Balietti, M.; Giorgetti, B.; Solazzi, M.; Fattoretti, P. Effect of cognitive training on the expression of brain-derived neurotrophic factor in lymphocytes of mild cognitive impairment patients. Rejuvenation Res. 2014, 17, 235–238. [Google Scholar] [CrossRef]
- Balietti, M.; Giuli, C.; Fattoretti, P.; Fabbietti, P.; Postacchini, D.; Conti, F. Cognitive Stimulation modulates Platelet Total Phospholipases A2 Activity in Subjects with Mild Cognitive Impairment. J. Alzheimers Dis. 2016, 50, 957–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuli, C.; Fattoretti, P.; Gagliardi, C.; Mocchegiani, E.; Venarucci, D.; Balietti, M.; Casoli, T.; Costarelli, L.; Giacconi, R.; Malavolta, M.; et al. My Mind Project: The effects of cognitive training for elderly—The study protocol of a prospective randomized intervention study. Aging Clin. Exp. Res. 2017, 29, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattoretti, P.; Malavolta, M.; Fabbietti, P.; Papa, R.; Giacconi, R.; Costarelli, L.; Galeazzi, R.; Paoloni, C.; Postacchini, D.; Lattanzio, F.; et al. Oxidative Stress in Elderly with Different Cognitive Status: My Mind Project. J. Alzheimers Dis. 2018, 63, 1405–1414. [Google Scholar] [CrossRef] [PubMed]
- Giacconi, R.; Giuli, C.; Casoli, T.; Balietti, M.; Costarelli, L.; Provinciali, M.; Basso, A.; Piacenza, F.; Postacchini, D.; Galeazzi, R.; et al. Acetylcholinesterase inhibitors in Alzheimer’s disease influence Zinc and Copper homeostasis. J. Trace Elem. Med. Biol. 2019, 55, 58–63. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Banach, M. Botanicals and phytochemicals active on cognitive decline: The clinical evidence. Pharmacol. Res. 2018, 130, 204–212. [Google Scholar] [CrossRef]
- Di Luca, M.; Pastorino, L.; Bianchetti, A.; Perez, J.; Vignolo, L.A.; Lenzi, G.L.; Trabucchi, M.; Cattabeni, F.; Padovani, A. Differential level of platelet amyloid beta precursor protein isoforms: An early marker for Alzheimer disease. Arch. Neurol. 1998, 55, 1195–1200. [Google Scholar] [CrossRef]
- Baskin, F.; Rosenberg, R.N.; Iyer, L.; Schellenberg, G.D.; Hynan, L.; Nee, L.E. Platelet APP Isoform Ratios in Asymptomatic Young Adults Expressing an AD-related presenilin-1 Mutation. J. Neurol. Sci. 2001, 183, 85–88. [Google Scholar] [CrossRef]
- Liu, H.C.; Wang, H.C.; Ko, S.Y.; Wang, P.N.; Chi, C.W.; Hong, C.J.; Lin, K.N.; Liu, T.Y. Correlation between platelet amyloid precursor protein isoform ratio and cognition in Alzheimer’s disease. J. Alzheimers Dis. 2007, 11, 77–84. [Google Scholar] [CrossRef]
- Barthet, G.; Jordà-Siquier, T.; Rumi-Masante, J.; Bernadou, F.; Müller, U.; Mulle, C. Presenilin-mediated cleavage of APP regulates synaptotagmin-7 and presynaptic plasticity. Nat. Commun. 2018, 9, 4780. [Google Scholar] [CrossRef] [Green Version]
- Deyts, C.; Clutter, M.; Pierce, N.; Chakrabarty, P.; Ladd, T.B.; Goddi, A.; Rosario, A.M.; Cruz, P.; Vetrivel, K.; Wagner, S.L.; et al. APP-Mediated Signaling Prevents Memory Decline in Alzheimer’s Disease Mouse Model. Cell Rep. 2019, 27, 1345–1355.e6. [Google Scholar] [CrossRef] [Green Version]
- Montagna, E.; Dorostkar, M.M.; Herms, J. The Role of APP in Structural Spine Plasticity. Front. Mol. Neurosci. 2017, 10, 136. [Google Scholar] [CrossRef] [Green Version]
- Fielder, E.; von Zglinicki, T.; Jurk, D. The DNA Damage Response in Neurons: Die by Apoptosis or Survive in a Senescence-Like State? J. Alzheimers Dis. 2017, 60, S107–S131. [Google Scholar] [CrossRef]
- Baker, D.J.; Petersen, R.C. Cellular senescence in brain aging and neurodegenerative diseases: Evidence and perspectives. J. Clin. Investig. 2018, 128, 1208–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kern, A.; Roempp, B.; Prager, K.; Walter, J.; Behl, C. Down-regulation of endogenous amyloid precursor protein processing due to cellular aging. J. Biol. Chem. 2006, 281, 2405–2413. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; He, T.; Pan, Y.; Katusic, Z.S. Effects of senescence and angiotensin II on expression and processing of amyloid precursor protein in human cerebral microvascular endothelial cells. Aging (Albany NY) 2018, 10, 100–1140. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Cué, C.; Rueda, N. Cellular Senescence in Neurodegenerative Diseases. Front. Cell Neurosci. 2020, 14, 16. [Google Scholar] [CrossRef]
- Alladi, S.; Xuereb, J.; Bak, T.; Nestor, P.; Knibb, J.; Patterson, K.; Hodges, J.R. Focal cortical presentations of Alzheimer’s disease. Brain 2007, 130, 2636–2645. [Google Scholar] [CrossRef] [Green Version]
- Cure, S.; Abrams, K.; Belger, M.; Dell’agnello, G.; Happich, M. Systematic literature review and meta-analysis of diagnostic test accuracy in Alzheimer’s disease and other dementia using autopsy as standard of truth. J. Alzheimers Dis. 2014, 42, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Vignini, A.; Sartini, D.; Morganti, S.; Nanetti, L.; Luzzi, S.; Provinciali, L.; Mazzanti, L.; Emanuelli, M. Platelet amyloid precursor protein isoform expression in Alzheimer’s disease: Evidence for peripheral marker. Int. J. Immunopathol. Pharmacol. 2011, 24, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Colciaghi, F.; Borroni, B.; Pastorino, L.; Marcello, E.; Zimmermann, M.; Cattabeni, F.; Padovani, A.; Di Luca, M. α-Secretase ADAM10 as well as αAPPs is reduced in platelets and CSF of Alzheimer disease patients. Mol. Med. 2002, 8, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padovani, A.; Borroni, B.; Colciaghi, F.; Pettenati, C.; Cottini, E.; Agosti, C.; Lenzi, G.L.; Caltagirone, C.; Trabucchi, M.; Cattabeni, F.; et al. Abnormalities in the pattern of platelet amyloid precursor protein forms in patients with mild cognitive impairment and Alzheimer disease. Arch. Neurol. 2002, 59, 71–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s Disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuli, C.; Papa, R.; Lattanzio, F.; Postacchini, D. The Effects of Cognitive Training for Elderly: Results from My Mind Project. Rejuvenation Res. 2016, 19, 485–494. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| AD Control (n = 31) | AD Trained (n = 28) | p | |
|---|---|---|---|
| Age (years) | 78.74 ± 1.02 | 76.32 ± 0.86 | 0.078 |
| Gender (females) | 19 (61.29) | 18 (64.28) | 0.812 |
| Schooling (years) | 5.00 (3.00, 5.00) | 5.00 (3.00, 5.00) | 0.847 |
| MMSE | 20.70 ± 0.76 | 20.14 ± 0.86 | 0.627 |
| GDS-30 | 8.06 ± 1.15 | 10.18 ± 1.33 | 0.231 |
| ADL | 6.00 (4.00, 6.00) | 5.50 (5.00, 6.00) | 0.622 |
| IADL | 4.00 (1.00, 5.00) | 3.00 (2.00, 4.00) | 0.639 |
| PASE | 61.22 ± 7.74 | 54.64 ± 7.15 | 0.537 |
| ADAS-Cog | 20.61 ± 1.85 | 20.39 ± 1.79 | 0.932 |
| CDR | 1.00 (1.00, 2.00) | 1.00 (1.00, 2.00) | 0.837 |
| Age at onset (years) | 76.52 ± 1.11 | 75.00 ± 0.87 | 0.294 |
| Disease duration (months) | 20.00 (4.00, 48.00) | 10.00 (3.25, 28.75) | 0.096 |
| APPr | 2.82 ± 0.30 | 3.38 ± 0.45 | 0.643 |
| Test | AD Control (n = 31) | AD Trained (n = 28) | p |
|---|---|---|---|
| Forward verbal span | 4.39 ± 0.14 | 3.88 ± 0.19 | 0.033 |
| Backward verbal span | 2.00 (2.00, 3.00) | 2.00 (2.00, 2.00) | 0.393 |
| Prose memory | 1.60 (1.00, 6.35) | 3.38 (1.25, 7.33) | 0.386 |
| Word pairing learning | 3.66 (2.50, 6.12) | 3.86 (2.36, 5.86) | 0.762 |
| SWF | 1.00 (0.00, 2.00) | 1.00 (0.00, 2.00) | 0.625 |
| Attentive matrices | 31.24 ± 1.78 | 27.26 ± 1.76 | 0.118 |
| Corsi Supra Span | 4.50 (3.50, 4.75) | 4.13 (2.75, 5.31) | 0.789 |
| Δ FU1 | Δ FU2 | Δ FU3 | ||||
|---|---|---|---|---|---|---|
| AD Control (n = 31) | AD Trained (n = 28) | AD Control (n = 31) | AD Trained (n = 28) | AD Control (n = 31) | AD Trained (n = 28) | |
| MMSE | −0.14 ± 2.29 | −0.63 ± 2.30 | −1.42 ± 2.99 | −1.92 ± 2.69 | −1.95 ± 3.07 | −4.75 ± 4.76 * |
| GDS-30 | 2.00 (−1.00, 4.00) | 0.00 (−2.00, 3.00) | 2.00 (−0.75, 4.75) | 0.00 (−2.50, 3.50) | 1.00 (−2.00, 3.00) | 2.00 (−1.00, 4.00) |
| ADL | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (−1.00, 0.00) | 0.00 (−1.00, 0.00) | −1.00 (−2.00, 0.00) | −1.00 (−2.00, 0.00) |
| IADL | 0.00 (−0.50, 0.00) | 0.00 (0.00, 1.00) * | 0.00 (−1.00, 0.00) | 0.00 (−1.00, 1.00) | 0.00 (−2.00, 0.00) | −1.00 (−3.00, 0.00) |
| PASE | 16.27 ± 8.30 | 17.11 ± 7.75 | −14.76 ± 7.94 | −14.31 ± 5.42 | −38.90 ± 8.39 | −32.91 ± 7.69 |
| ADAS-Cog | 0.00 (−4.00, 3.50) | −3.00 (−6.00, −1.00) | 0.00 (−4.00, 4.50) | −2.00 (−3.50, 1.50) | 1.50 (−3.00, 6.00) | 2.00 (−1.00, 23.00) |
| CDR | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (0.00, 1.00) | 0.00 (0.00, 0.00) * | 0.00 (0.00, 1.00) | 1.00 (0.00, 1.00) |
| APPr | 1.01 ± 0.75 | 0.40 ± 0.72 | −0.11 ± 0.47 | −0.56 ± 0.50 | 0.25 ± 0.52 | −1.79 ± 0.75 * |
| Forward verbal span | 0.00 (−1.00, 1.00) | 1.00 (0.00, 1.00) * | 0.00 (−1.00, 1.00) | 0.00 (−0.63, 1.00) | 0.00 (−1.00, 0.43) | 0.00 (−0.75, 0.83) |
| Backward verbal span | 0.00 (−0.50, 0.00) | 1.00 (0.00, 1.00) * | 0.00 (−1.00, 0.00) | 0.00 (0.00, 1.00) * | 0.00 (−1.25, 0.00) | 0.00 (−1.00, 0.00) |
| Prose memory | 0.00 (−0.87, 0.43) | 2.00 (0.00, 4.00) * | 0.00 (−0.15, 1.83) | 0.00 (−2.00, −2.55) | 0.00 (−3.47, 1.83) | 0.00 (−2.00, 2.00) |
| Word pairing learning | 0.00 (−1.75, 1.01) | 0.50 (−0.50, 2.00) | 0.02 (−1.98, 1.52) | 0.00 (−0.99, 1.75) | 0.04 (−2.47, 1.79) | −0.47 (−1.97, 0.54) |
| SWF | 0.00 (−0.50, 0.00) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (−0.50, 0.00) | 0.00 (−1.00, 0.00) | −0.50 (−1.00, 0.00) |
| Attentive matrices | −1.00 (−2.25, 0.00) | 2.00 (0.00, 5.00) * | 0.00 (−3.50, 2.00) | 2.00 (−6.00, 8.00) | −3.75 (−8.13, 0.38) | −4.00 (−6.00, 1.50) |
| Corsi Supra Span | 0.00 (−1.00, 0.13) | 0.00 (0.00, 1.00) | 0.00 (−1.00, 0.00) | 0.00 (−1.00, 1.00) | −1.00 (−1.87, 0.00) | −1.00 (−1.00, 0.00) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casoli, T.; Giuli, C.; Balietti, M.; Fabbietti, P.; Conti, F. Effect of a Cognitive Training Program on the Platelet APP Ratio in Patients with Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 5110. https://doi.org/10.3390/ijms21145110
Casoli T, Giuli C, Balietti M, Fabbietti P, Conti F. Effect of a Cognitive Training Program on the Platelet APP Ratio in Patients with Alzheimer’s Disease. International Journal of Molecular Sciences. 2020; 21(14):5110. https://doi.org/10.3390/ijms21145110
Chicago/Turabian StyleCasoli, Tiziana, Cinzia Giuli, Marta Balietti, Paolo Fabbietti, and Fiorenzo Conti. 2020. "Effect of a Cognitive Training Program on the Platelet APP Ratio in Patients with Alzheimer’s Disease" International Journal of Molecular Sciences 21, no. 14: 5110. https://doi.org/10.3390/ijms21145110
APA StyleCasoli, T., Giuli, C., Balietti, M., Fabbietti, P., & Conti, F. (2020). Effect of a Cognitive Training Program on the Platelet APP Ratio in Patients with Alzheimer’s Disease. International Journal of Molecular Sciences, 21(14), 5110. https://doi.org/10.3390/ijms21145110