Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review

Abstract
:1. Introduction
2. Results
2.1. Preclinical Studies: Oral and Intraperitoneal Administration
2.2. Preclinical Studies: Intra-Articular Administration
2.3. Clinical Studies
3. Discussion
4. Materials and Methods
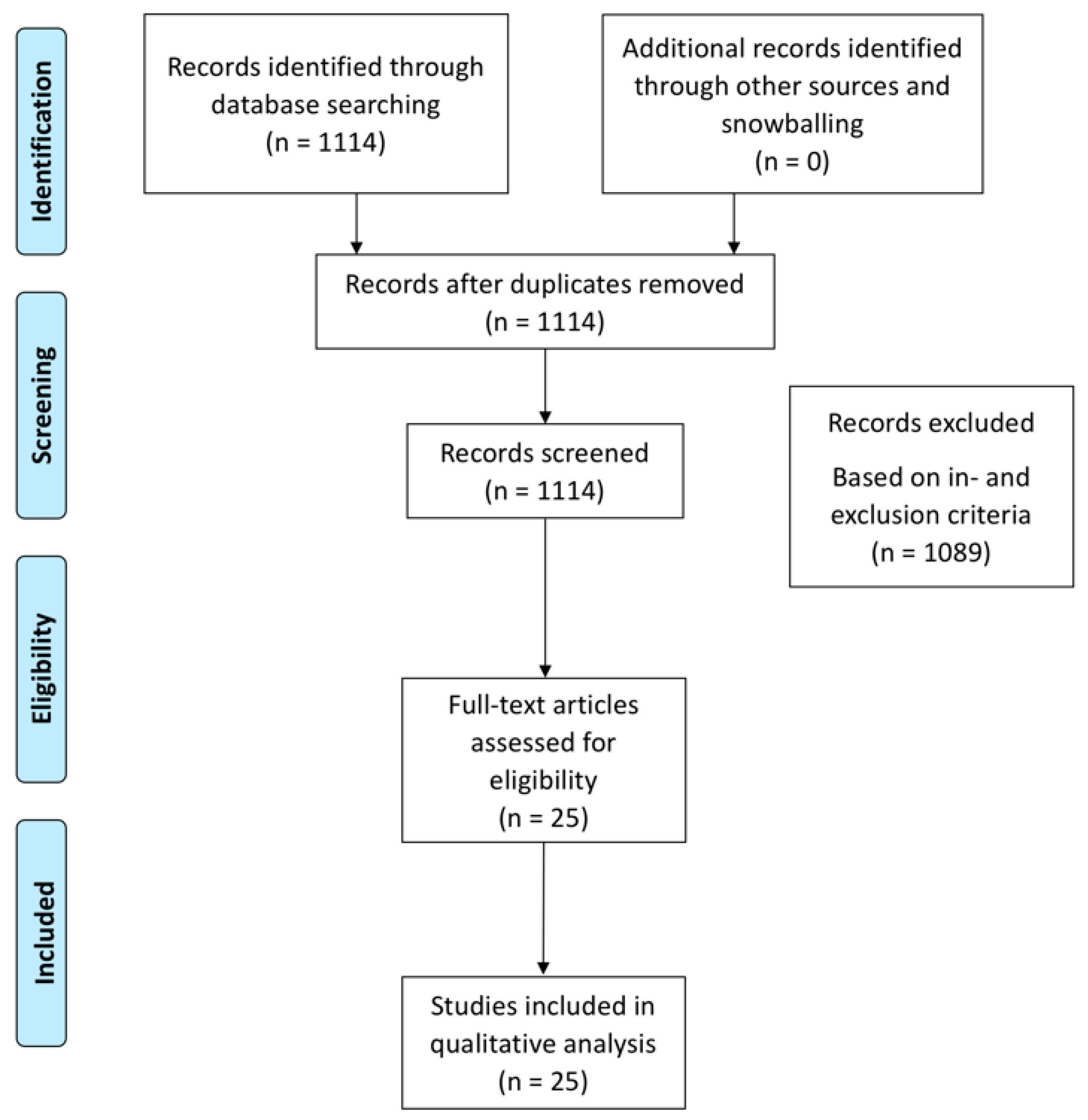
4.1. Search Strategy and Data Extraction
4.2. Articles Were Selected Based on Inclusion and Exclusion Criteria
- Presenting data about chondroprotective effects of COX-2 inhibitors;The chondroprotective effect is defined as any effect that leads to significantly less cartilage degradation evidenced either through imaging, biochemical analysis or on histology.
- Either in vivo animal studies or clinical studies involving human knee OA patients;
- Intra-articular therapies with COX-2 inhibitors;
- Systemic therapies with COX-2 inhibitors.
- Studies solely investigating non-selective cox-inhibitors;
- Studies investigating actions of celecoxib inhibitors on pain modulation in knee OA;
- Studies investigating other joints than the knee;
- Studies reporting solely in vitro data.
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACLT | Anterior cruciate ligament transection |
| CLX | Celecoxib |
| COX | Cyclooxygenase |
| DDS | Drug Delivery System |
| DMM | Destabilization of the medial meniscus |
| DMOAD | Disease modifying osteoarthritis drugs |
| ETX | Etoricoxib |
| HA | Hyaluronic acid |
| JSW | Joint space width |
| K&L | Kellgren and Lawrence |
| MCLT | Medial collateral ligament transection |
| MIA | Monosodiumiodoacetate |
| MMx | Medial meniscus transection |
| MRI | Magnetic Resonance Imaging |
| NP | Nanoparticle |
| NSAID | Non-steroidal anti-inflammatory drugs |
| OA | Osteoarthritis |
| PEA | Polyesteramide |
| Pg | Prostaglandin |
| PG | Proteoglycan |
| pMMx | Partial medial meniscus transection |
References
- Hunter, D.J.; Felson, D.T. Osteoarthritis. BMJ 2006, 332, 639–642. [Google Scholar] [CrossRef]
- Ricciotti, E.; FitzGerald, G.A. Prostaglandins and inflammation. Arterioscler Thromb Vasc. Biol. 2011, 31, 986–1000. [Google Scholar] [CrossRef]
- Martel-Pelletier, J.; Pelletier, J.P.; Fahmi, H. Cyclooxygenase-2 and prostaglandins in articular tissues. Semin. Arthritis Rheum. 2003, 33, 155–167. [Google Scholar] [CrossRef]
- Ayral, X.; Pickering, E.H.; Woodworth, T.G.; Mackillop, N.; Dougados, M. Synovitis: A potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis—Results of a 1 year longitudinal arthroscopic study in 422 patients. Osteoarthritis Cartilage 2005, 13, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.E.; Block, J.A.; Malfait, A.M. Nerve growth factor blockade for the management of osteoarthritis pain: What can we learn from clinical trials and preclinical models? Curr. Opin. Rheumatol. 2017, 29, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Ding, C. Do NSAIDs affect the progression of osteoarthritis? Inflammation 2002, 26, 139–142. [Google Scholar] [CrossRef]
- Zweers, M.C.; De Boer, T.N.; Van Roon, J.; Bijlsma, J.W.; Lafeber, F.P.; Mastbergen, S.C. Celecoxib: Considerations regarding its potential disease-modifying properties in osteoarthritis. Arthritis Res. Ther. 2011, 13, 239. [Google Scholar] [CrossRef] [Green Version]
- Buckwalter, J.A.; Mankin, H.J. Articular cartilage: Tissue design and chondrocyte-matrix interactions. Instr. Course Lect. 1998, 47, 477–486. [Google Scholar]
- Makris, E.A.; Hadidi, P.; Athanasiou, K.A. The knee meniscus: Structure-function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials 2011, 32, 7411–7431. [Google Scholar] [CrossRef] [Green Version]
- Hooijmans, C.R.; Rovers, M.M.; De Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- Van der Kraan, P.M.; Buma, P.; Van Kuppevelt, T.; Van den Berg, W.B. Interaction of chondrocytes, extracellular matrix and growth factors: Relevance for articular cartilage tissue engineering. Osteoarthritis Cartilage 2002, 10, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Mastbergen, S.C.; Marijnissen, A.C.; Vianen, M.E.; Zoer, B.; Van Roermund, P.M.; Bijlsma, J.W.; Lafeber, F.P. Inhibition of COX-2 by celecoxib in the canine groove model of osteoarthritis. Rheumatology 2006, 45, 405–413. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.E.; Baek, Y.H.; Kim, Y.J.; Lee, J.D.; Choi, D.Y.; Park, D.S. Protective effects of butanol fraction from Betula platyphyla var. japonica on cartilage alterations in a rabbit collagenase-induced osteoarthritis. J. Ethnopharmacol 2009, 123, 515–521. [Google Scholar] [CrossRef]
- Fukai, A.; Kamekura, S.; Chikazu, D.; Nakagawa, T.; Hirata, M.; Saito, T.; Hosaka, Y.; Ikeda, T.; Nakamura, K.; Chung, U.; et al. Lack of a chondroprotective effect of cyclooxygenase 2 inhibition in a surgically induced model of osteoarthritis in mice. Arthritis Rheum. 2012, 64, 198–203. [Google Scholar] [CrossRef]
- Ou, Y.; Tan, C.; An, H.; Jiang, D.; Quan, Z.; Tang, K.; Luo, X. Selective COX-2 inhibitor ameliorates osteoarthritis by repressing apoptosis of chondrocyte. Med. Sci. Monit. 2012, 18, BR247–BR252. [Google Scholar] [CrossRef] [Green Version]
- Ashkavand, Z.; Malekinejad, H.; Amniattalab, A.; Rezaei-Golmisheh, A.; Vishwanath, B.S. Silymarin potentiates the anti-inflammatory effects of Celecoxib on chemically induced osteoarthritis in rats. Phytomedicine 2012, 19, 1200–1205. [Google Scholar] [CrossRef]
- Moon, S.J.; Park, J.S.; Jeong, J.H.; Yang, E.J.; Park, M.K.; Kim, E.K.; Park, S.H.; Kim, H.Y.; Cho, M.L.; Min, J.K. Augmented chondroprotective effect of coadministration of celecoxib and rebamipide in the monosodium iodoacetate rat model of osteoarthritis. Arch. Pharm. Res. 2013, 36, 116–124. [Google Scholar] [CrossRef]
- Panahifar, A.; Jaremko, J.L.; Tessier, A.G.; Lambert, R.G.; Maksymowych, W.P.; Fallone, B.G.; Doschak, M.R. Development and reliability of a multi-modality scoring system for evaluation of disease progression in pre-clinical models of osteoarthritis: Celecoxib may possess disease-modifying properties. Osteoarthritis Cartilage 2014, 22, 1639–1650. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Meng, D.; Li, G.; Xu, J.; Tian, K.; Li, Y. Celecoxib Combined with Diacerein Effectively Alleviates Osteoarthritis in Rats via Regulating JNK and p38MAPK Signaling Pathways. Inflammation 2015, 38, 1563–1572. [Google Scholar] [CrossRef]
- Dai, M.W.; Chu, J.G.; Tian, F.M.; Song, H.P.; Wang, Y.; Zhang, Y.Z.; Zhang, L. Parathyroid hormone(1-34) exhibits more comprehensive effects than celecoxib in cartilage metabolism and maintaining subchondral bone micro-architecture in meniscectomized guinea pigs. Osteoarthritis Cartilage 2016, 24, 1103–1112. [Google Scholar] [CrossRef] [Green Version]
- Tu, M.; Yang, M.; Yu, N.; Zhen, G.; Wan, M.; Liu, W.; Ji, B.; Ma, H.; Guo, Q.; Tong, P.; et al. Inhibition of cyclooxygenase-2 activity in subchondral bone modifies a subtype of osteoarthritis. Bone Res. 2019, 7, 29. [Google Scholar] [CrossRef]
- Jones, M.D.; Tran, C.W.; Li, G.; Maksymowych, W.P.; Zernicke, R.F.; Doschak, M.R. In vivo microfocal computed tomography and micro-magnetic resonance imaging evaluation of antiresorptive and antiinflammatory drugs as preventive treatments of osteoarthritis in the rat. Arthritis Rheum. 2010, 62, 2726–2735. [Google Scholar] [CrossRef] [Green Version]
- Nagy, E.; Vajda, E.; Vari, C.; Sipka, S.; Farr, A.M.; Horvath, E. Meloxicam ameliorates the cartilage and subchondral bone deterioration in monoiodoacetate-induced rat osteoarthritis. PeerJ 2017, 5, e3185. [Google Scholar] [CrossRef] [Green Version]
- Wen, Z.H.; Lin, Y.Y.; Chang, Y.C.; Tang, C.C.; Hsieh, S.P.; Lee, H.P.; Sung, C.S.; Chen, W.F.; Lee, C.H.; Jean, J.H. The COX-2 inhibitor etoricoxib reduces experimental osteoarthritis and nociception in rats: The roles of TGF-beta1 and NGF expressions in chondrocytes. Eur. J. Pain. 2020, 24, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Ji, C.; Shao, Y.; Liang, T.; He, J.; Jiang, H.; Chen, G.; Luo, Z. Etoricoxib decreases subchondral bone mass and attenuates biomechanical properties at the early stage of osteoarthritis in a mouse model. Biomed Pharmacother 2020, 127, 110144. [Google Scholar] [CrossRef]
- Jiang, D.; Zou, J.; Huang, L.; Shi, Q.; Zhu, X.; Wang, G.; Yang, H. Efficacy of intra-articular injection of celecoxib in a rabbit model of osteoarthritis. Int. J. Mol. Sci. 2010, 11, 4106. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.; Jiang, D.; Wang, Z.; Wu, G.; Miao, L.; Huang, L. Intra-articular delivery of liposomal celecoxib-hyaluronate combination for the treatment of osteoarthritis in rabbit model. Int. J. Pharm. 2013, 441, 285–290. [Google Scholar] [CrossRef]
- Janssen, M.; Timur, U.T.; Woike, N.; Welting, T.J.; Draaisma, G.; Gijbels, M.; van Rhijn, L.W.; Mihov, G.; Thies, J.C.; Emans, P.J. Celecoxib-loaded PEA microspheres as an auto regulatory drug-delivery system after intra-articular injection. J. Control Release. 2016, 244, 30–40. [Google Scholar] [CrossRef]
- Tellegen, A.R.; Rudnik-Jansen, I.; Pouran, B.; De Visser, H.M.; Weinans, H.H.; Thomas, R.E.; Kik, M.J.L.; Grinwis, G.C.M.; Thies, J.C.; Woike, N.; et al. Controlled release of celecoxib inhibits inflammation, bone cysts and osteophyte formation in a preclinical model of osteoarthritis. Drug Deliv. 2018, 25, 1438–1447. [Google Scholar] [CrossRef] [Green Version]
- Jean, Y.H.; Wen, Z.H.; Chang, Y.C.; Hsieh, S.P.; Tang, C.C.; Wang, Y.H.; Wong, C.S. Intra-articular injection of the cyclooxygenase-2 inhibitor parecoxib attenuates osteoarthritis progression in anterior cruciate ligament-transected knee in rats: Role of excitatory amino acids. Osteoarthritis Cartilage 2007, 15, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Wen, Z.H.; Tang, C.C.; Chang, Y.C.; Huang, S.Y.; Chen, C.H.; Wu, S.C.; Hsieh, S.P.; Hsieh, C.S.; Wang, K.Y.; Lin, S.Y.; et al. Intra-articular injection of the selective cyclooxygenase-2 inhibitor meloxicam (Mobic) reduces experimental osteoarthritis and nociception in rats. Osteoarthritis Cartilage 2013, 21, 1976–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; Gu, L.; Ren, L.; Chen, J.; Li, T.; Wang, X.; Yang, J.; Chen, C.; Sun, L. Intra-articular injection of etoricoxib-loaded PLGA-PEG-PLGA triblock copolymeric nanoparticles attenuates osteoarthritis progression. Am. J. Transl. Res. 2019, 11, 6775–6789. [Google Scholar] [PubMed]
- Tindall, E.A.; Sharp, J.T.; Burr, A.; Katz, T.K.; Wallemark, C.B.; Verburg, K.; Lefkowith, J. A 12-month, multicenter, prospective, open-label trial of radiographic analysis of disease progression in osteoarthritis of the knee or hip in patients receiving celecoxib. Clin Ther. 2002, 24, 2051–2063. [Google Scholar] [CrossRef]
- Sawitzke, A.D.; Shi, H.; Finco, M.F.; Dunlop, D.D.; 3rd Bingham, C.O.; Harris, C.L.; Singer, N.G.; Bradley, J.D.; Silver, D.; Jackson, C.G.; et al. The effect of glucosamine and/or chondroitin sulfate on the progression of knee osteoarthritis: A report from the glucosamine/chondroitin arthritis intervention trial. Arthritis Rheum. 2008, 58, 3183–3191. [Google Scholar] [CrossRef] [PubMed]
- De Boer, T.N.; Huisman, A.M.; Polak, A.A.; Niehoff, A.G.; Van Rinsum, A.C.; Saris, D.; Bijlsma, J.W.J.; Lafeber, F.J.P.G.; Mastbergen, S.C. The chondroprotective effect of selective COX-2 inhibition in osteoarthritis: Ex vivo evaluation of human cartilage tissue after in vivo treatment. Osteoarthritis Cartilage 2009, 17, 482–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raynauld, J.P.; Martel-Pelletier, J.; Beaulieu, A.; Bessette, L.; Morin, F.; Choquette, D.; Haraoui, B.; Abram, F.; Pelletier, J.P. An open-label pilot study evaluating by magnetic resonance imaging the potential for a disease-modifying effect of celecoxib compared to a modelized historical control cohort in the treatment of knee osteoarthritis. Semin. Arthritis Rheum. 2010, 40, 185–192. [Google Scholar] [CrossRef]
- Riendeau, D.; Percival, M.D.; Brideau, C.; Charleson, S.; Dubé, D.; Ethier, D.; Falgueyret, J.P.; Friesen, R.W.; Gordon, R.; Greig, G.; et al. Etoricoxib (MK-0663): Preclinical Profile and Comparison with other agents that selectively inhibit Cyclooxygenase-2. J. Pharmacol. Exp. Ther. 2001, 296, 558–566. [Google Scholar]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- Clockaerts, S.; Bastiaansen-Jenniskens, Y.M.; Runhaar, J.; Van Osch, G.J.; Van Offel, J.F.; Verhaar, J.A.; de Clerck, L.S.; Somville, J. The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: A narrative review. Osteoarthritis Cartilage 2010, 18, 876–882. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, J.B.; Fermor, B.; Guilak, F. Nitric oxide synthase and cyclooxygenase interactions in cartilage and meniscus: Relationships to joint physiology, arthritis, and tissue repair. Subcell Biochem. 2007, 42, 31–62. [Google Scholar]
- De Lange-Brokaar, B.J.; Ioan-Facsinay, A.; Van Osch, G.J.; Zuurmond, A.M.; Schoones, J.; Toes, R.E.; Huizinga, T.W.J.; Kloppenburg, M. Synovial inflammation, immune cells and their cytokines in osteoarthritis: A review. Osteoarthritis Cartilage 2012, 20, 1484–1499. [Google Scholar] [CrossRef] [Green Version]
- Bastiaansen-Jenniskens, Y.M.; Wei, W.; Feijt, C.; Waarsing, J.H.; Verhaar, J.A.; Zuurmond, A.M.; Hanemaaijer, R.; Stoop, R.; van Osch, G.J.V.M. Stimulation of fibrotic processes by the infrapatellar fat pad in cultured synoviocytes from patients with osteoarthritis: A possible role for prostaglandin f2alpha. Arthritis Rheum. 2013, 65, 2070–2080. [Google Scholar] [CrossRef] [Green Version]
- Welting, T.J.; Caron, M.M.; Emans, P.J.; Janssen, M.P.; Sanen, K.; Coolsen, M.M.; Voss, L.; Surtel, D.A.; Cremers, A.; Voncken, J.; et al. Inhibition of cyclooxygenase-2 impacts chondrocyte hypertrophic differentiation during endochondral ossification. Eur. Cell Mater. 2011, 22, 420–437. [Google Scholar] [CrossRef]
- Felson, D.T.; Niu, J.; Neogi, T.; Goggins, J.; Nevitt, M.C.; Roemer, F.; Torner, J.; Lewis, C.E.; Guermazi, A. Synovitis and the risk of knee osteoarthritis: The MOST Study. Osteoarthritis Cartilage 2016, 24, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Karin, M.; Clevers, H. Reparative inflammation takes charge of tissue regeneration. Nature 2016, 529, 307–315. [Google Scholar] [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Christiansen, C.; Ladel, C.; Henriksen, K.; Kraus, V.B.; Bay-Jensen, A.C. Osteoarthritis--a case for personalized health care? Osteoarthritis Cartilage 2014, 22, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Waarsing, J.H.; Bierma-Zeinstra, S.M.; Weinans, H. Distinct subtypes of knee osteoarthritis: Data from the Osteoarthritis Initiative. Rheumatology 2015, 54, 1650–1658. [Google Scholar] [CrossRef] [Green Version]
- Oei, E.H.G.; Wick, M.C.; Muller-Lutz, A.; Schleich, C.; Miese, F.R. Cartilage Imaging: Techniques and Developments. Semin. Musculoskelet. Radiol. 2018, 22, 245–260. [Google Scholar] [CrossRef]


{kind=link}
| Preclinical Studies Using Oral Administration | ||||||||
| Authors | Species | COX-2 Inhibitor | OA Model | Dosing Regime | Start of Treatment | Timepoint of Evaluation | Evaluation of Cartilage Degradation | Main Findings |
| Mastbergen et al. [12] | Canine | Celecoxib | Groove | Daily 200 mg | Directly after surgery | 15 weeks after OA induction | Histology:Modified Mankin Biochemistry: PG content, synthesis and release | No difference in histological scores, no difference in PG content, synthesis or release |
| Huh et al. [13] | Rabbit | Celecoxib | Collagenase | Daily 100 mg/kg | Directly after OA induction | 4 weeks after OA induction | Histology: Colombo score for cartilage and synovitis score for synoviummRNA analysis PTGS1, PTGS2, MMP1 and MMP3 | Improved histological score in celecoxib group vs. control, decreased MMP-1 mRNA expression in celecoxib group vs. control |
| Jones et al. [22] | Rat | Meloxicam | MCLT + ACLT + MMx | Daily 3 mg/kg | Directly after OA induction | 8 weeks after OA induction | Histology:Modified Mankin | No difference in histological score meloxicam vs. control |
| Fukai et al. [14] | Mouse | Celecoxib | MCLT + MMx | Daily 10 mg/kg or 30 mg/ kg | Directly after surgery | 12 weeks after OA induction | Histology:Pritzker score | No difference in Pritzker score celecoxib vs. control. |
| Ou et al. [15] | Rat | Celecoxib | Achilles tendon transection | Daily 24 mg/kg | Directly after surgery | Histology:Type II collagen Tunel staining | No difference in type II collagen content in celecoxib vs. control, decreased chondrocyte apoptosis in celecoxib group. | |
| Ashkavand et al. [16] | Rat | Celecoxib | MIA | Daily 100 mg/kg | Directly after OA induction | 15 days after OA induction | Histology: Own developed score | Improved histological score in the celecoxib group. Superior chondroprotective effects when celecoxib is combined with silymarin |
| Moon et al. [17] | Rat | Celecoxib | MIA | Daily 2.5 mg/kg | Directly after OA induction | 7 days after OA induction | Histology:Modified Mankin | No difference in Modified Mankin celecoxib vs. control. Synergistic beneficial action when celecoxib is added to rebamipide |
| Panahifar et al. [18] | Rat | Celecoxib | ACLT + MCLT + MMx | Daily 2.86 mg/kg | Directly after surgery | 4,8 and 12 weeks after OA induction | Histology: Modified Mankin | No difference in histological score celecoxib vs. control. |
| Li [19] | Rat | Celecoxib | Collagenase | Daily 0.25 mg | 6 weeks after surgery | 10 weeks after OA induction | Histology: Colombo score and Biochemistry:CTX-II content in serum, Caspase 3 activity in tissue homogenate | Improved histological score in celecoxib group vs. control, higher CTX-II content in celecoxib group, lower Caspase 3 activity in celecoxib group. More pronounced effects when celecoxib is combined with diacerein |
| Dai [20] | Pig | Celecoxib | MMx | 20 mg/kg daily | 1 week after surgery | 12 weeks after surgery | Macroscopic:|OARSI scoreHistology:OARSI scoreCOL-II and AGC immunohistochemistry | Improved macroscopic and histological score celecoxib group vs. control, no difference in COL-II and AGC expression |
| Nagy [23] | Rat | Meloxicam | MIA | Daily 0.2 mg/kg or 1 mg/kg | 3 weeks after OA induction | 11 weeks after OA induction | Histology: OARSI score | Improved histological score at both doses meloxicam compared to control |
| Tu [21] | Mouse | Celecoxib | Spontaneous OA (STR/Ort mouse) | Daily 8 mg/kg | 3 months old mice | 4 weeks after start treatment | Histology: OARSI score | Improved OARSI score in celecoxib group vs. controls, |
| Wen [24] | Rat | Etoricoxib | ACLT | 6.7 mg/kg or 33.3 mg/kg three times per week | 8 weeks after surgery | 21 weeks after surgery | Histology: Pritzker score for cartilage | Improved histological score in the etoricoxib group versus control |
| Preclinical Studies Using Intra-Peritoneal Injections | ||||||||
| Liu [25] | Mouse | Etoricoxib | DMM | 5 mg/kg, 10 mg/kg, 20 mg/kg three times per week | 2 days after OA induction | 30 days after surgery | Histology: OARSI score | No difference in histological score etoricoxib versus control. |
| Preclinical Studies Using Intra-Articular Injections | ||||||||
|---|---|---|---|---|---|---|---|---|
| Authors | Species | COX-2 Inhibitor | OA Model | Dosing Regime | Start of Treatment | Timepoint of Evaluation | Evaluation of Cartilage Damage | Main Findings |
| Jean et al. [30] | Rat | Parecoxib | ACLT | Weekly 100 µg parecoxib for 5 consecutive weeks | Eight weeks after surgery | 20 weeks after surgery | Histology: Mankin score | Improved histological scores in the parecoxib group compared to controls |
| Jiang et al. [26] | Rabbit | Celecoxib | ACLT+ PCLT + MMx | Weekly 1.2 mg celecoxib for 5 consecutive weeks | Directly after surgery | 12 weeks after surgery | Histology: Mankin score | Improved histological scores in the Celecoxib group compared to controls |
| Dong et al. [27] | Rat | Celecoxib | ACLT+ PCLT+ MCLT + MMx | Single injection: 0.15 mg celecoxib incorporated in DDS | One week after surgery | 2 weeks after surgery | Histology: Colombo score | Improved histological score only when celecoxib is combined with HA in a DDS compared to controls |
| Wen et al. [31] | Rat | Meloxicam | ACLT | Weekly 0.25 or 1 mg meloxicam for 5 consecutive weeks | Five weeks after surgery | 20 weeks after surgery | Histology: Pritzker score | Lower Pritzker score in the meloxicam group versus control |
| Janssen et al. [28] | Rat | Celecoxib | ACLT + pMMx | Single injection: 0.015 mg celecoxib incorporated in DDS | Four weeks after surgery | 16 weeks after surgery | Histology: OARSI score | No difference in histological score in celecoxib loaded microspheres vs. control |
| Tellegen et al. [29] | Rat | Celecoxib | ACLT + pMMx | Single injection: 0.015, 0.115 or 0.195 mg celecoxib incorporated in DDS | Four weeks after surgery | 16 weeks after surgery | Histology: OARSI score | No difference in histological score in celecoxib loaded microspheres vs. control |
| Liu et al. [32] | Rat | Etoricoxib | ACLT | Three injections: - 10 µM etoricoxib in 100 µL NaCl- 6.93 μg ETX-NPs, drug loading unclear | Three, six and nine weeks after surgery | 12 weeks after surgery | Histology: OARSI score Immunohistochemistry | Improved histological score in ETX-NP, but not ETX, compared to control. |
| Clinical Studies Using Oral Administration | |||||||
|---|---|---|---|---|---|---|---|
| Authors | Species | COX-2 Inhibitor | OA Grade | Dosing Regime | Treatment Duration | Evaluation of Cartilage Damage | Chondroprotection |
| Tindall et al. [33] | Human | Celecoxib | K&L 2 and 3 | Daily 200 or 400 mg | 12 months | Radiographs of the knee | No difference in JSW, subchondral sclerosis, cysts, malalignment or tilting after 12 months of treatment with celecoxib |
| Sawitzke et al. [34] | Human | Celecoxib | K&L 2 and 3 | Daily 200 mg | 24 months | Radiographs of the knee | No significant differences in JSW loss in celecoxib vs. controls |
| De Boer et al. [35] | Human | Celecoxib | Not specified | Daily 200 mg | 4 weeks | Biochemical cartilage analysis:PG synthesis rate, PG release and PG content | Increased PG synthesis rate, decreased PG release and increased PG content in the celecoxib group vs. controls. Decreased release of il-1, TNF-α and mmp-activity in celecoxib group vs. control |
| Raynauld et al. [36] | Human | Celecoxib | K&L 2 and 3 | Daily 200 mg | 12 months | Quantitative MRI | No difference in cartilage volume loss in celecoxib group vs. a historical cohort control group |
| Drug | IC50 COX-1 (µM) | IC50 COX-2 (µM) | COX-1/COX-2 IC50 Ratio |
|---|---|---|---|
| Meloxicam | 1.4 | 0.7 | 2 |
| Celecoxib | 6.7 | 0.87 | 7.7 |
| Etoricoxib | 116 | 1.1 | 105 |
| Parecoxib | 26.1 | 0.87 | 30 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timur, U.T.; Caron, M.M.J.; Jeuken, R.M.; Bastiaansen-Jenniskens, Y.M.; Welting, T.J.M.; van Rhijn, L.W.; van Osch, G.J.V.M.; Emans, P.J. Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 6962. https://doi.org/10.3390/ijms21186962
Timur UT, Caron MMJ, Jeuken RM, Bastiaansen-Jenniskens YM, Welting TJM, van Rhijn LW, van Osch GJVM, Emans PJ. Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review. International Journal of Molecular Sciences. 2020; 21(18):6962. https://doi.org/10.3390/ijms21186962
Chicago/Turabian StyleTimur, Ufuk Tan, Marjolein M. J. Caron, Ralph M. Jeuken, Yvonne M. Bastiaansen-Jenniskens, Tim J. M. Welting, Lodewijk W. van Rhijn, Gerjo J. V. M. van Osch, and Pieter J. Emans. 2020. "Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review" International Journal of Molecular Sciences 21, no. 18: 6962. https://doi.org/10.3390/ijms21186962
APA StyleTimur, U. T., Caron, M. M. J., Jeuken, R. M., Bastiaansen-Jenniskens, Y. M., Welting, T. J. M., van Rhijn, L. W., van Osch, G. J. V. M., & Emans, P. J. (2020). Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review. International Journal of Molecular Sciences, 21(18), 6962. https://doi.org/10.3390/ijms21186962