Biological and Clinical Changes in a Pediatric Series Treated with Off-Label JAK Inhibitors

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. Case Series
2.3. JAKinhibs Effect Reflected by Laboratory and Clinical Findings
2.4. JAKinhibs Effect Reflected on Gene Expression Patterns
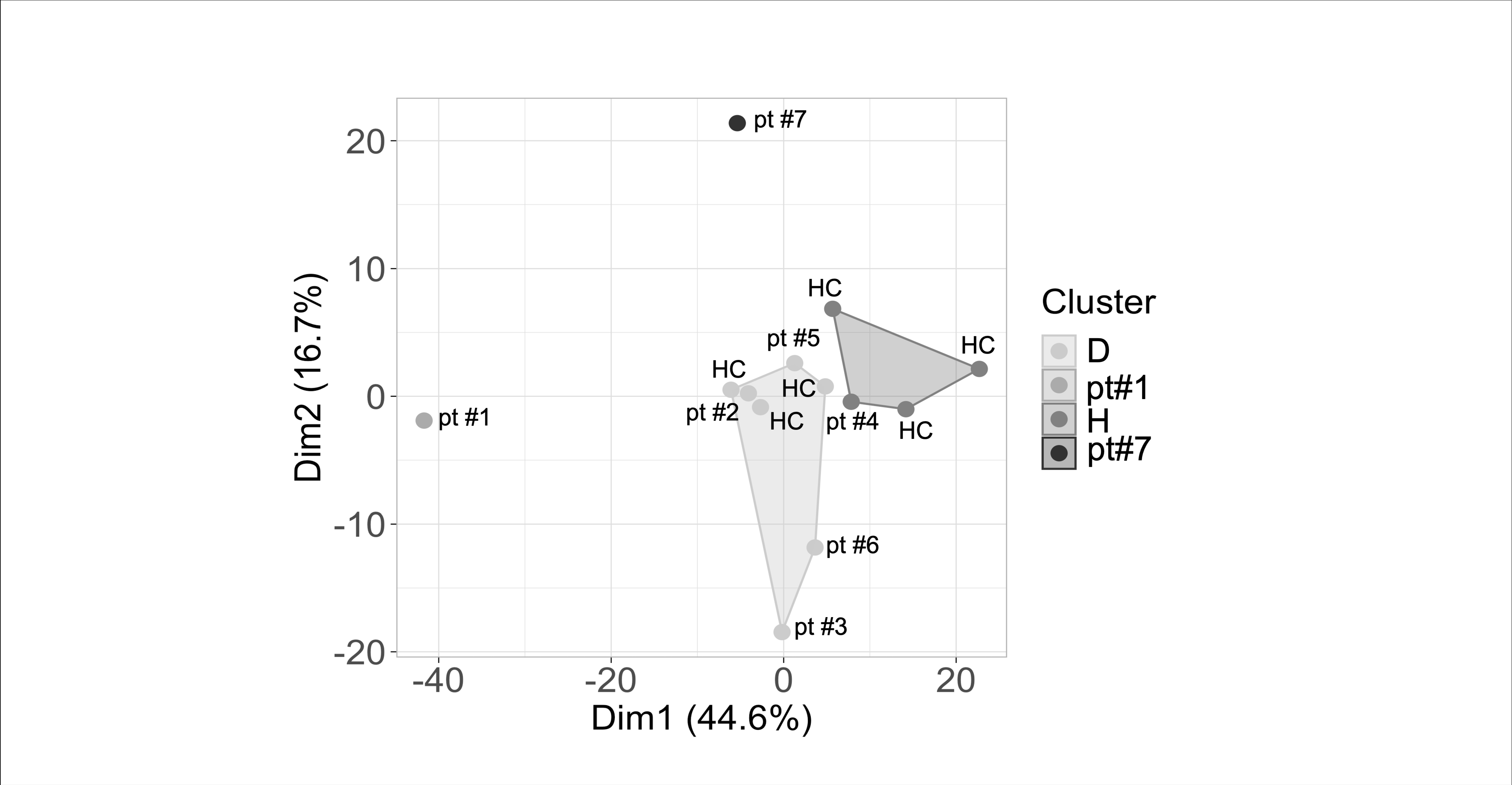
2.4.1. Transcriptomic Profile in Patients Compared with Control-Group Subjects: Cluster Analysis
2.4.2. Transcriptomic Profile in Patients Compared with Control-Group Subjects: Pathway Analysis
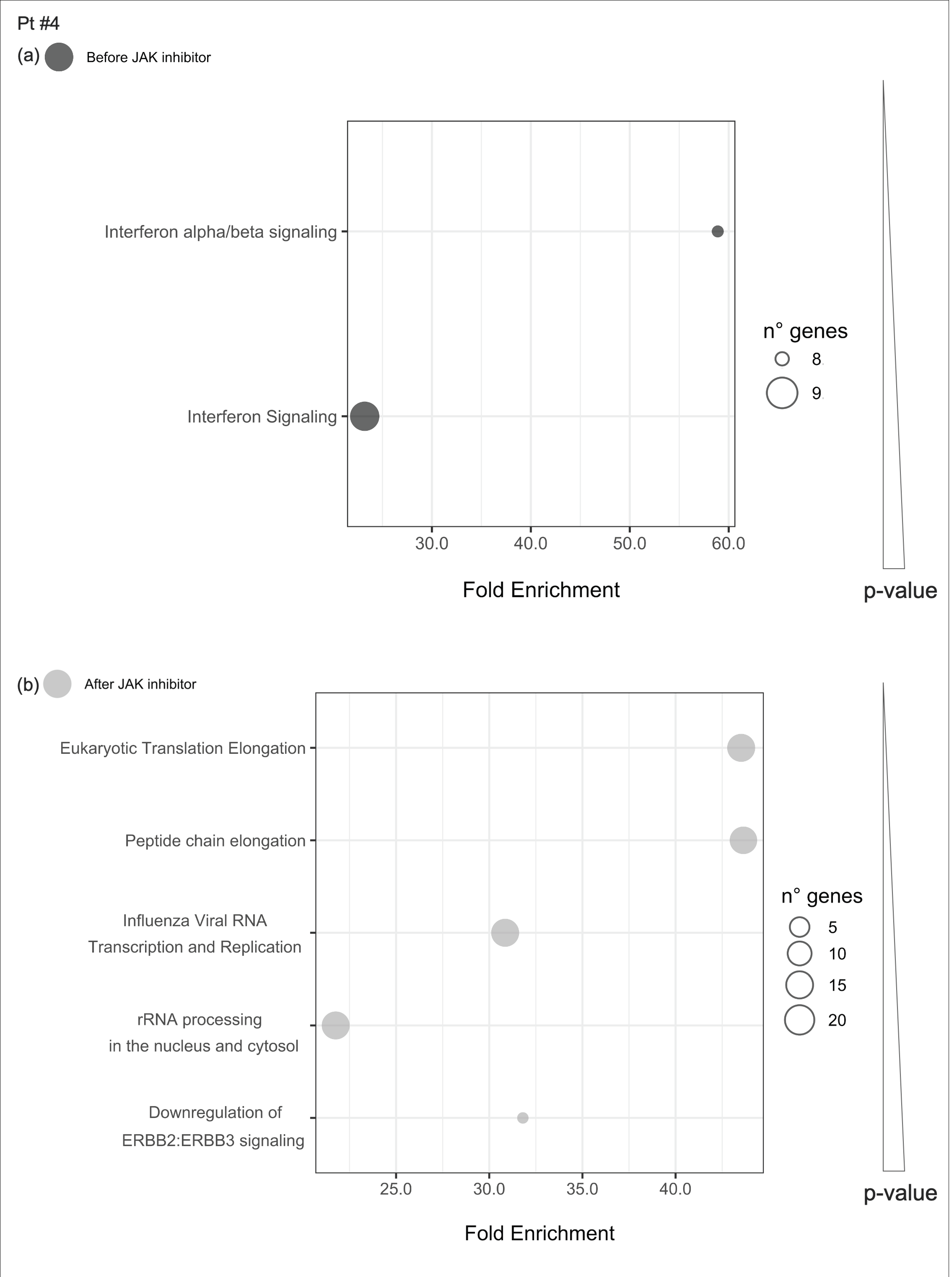
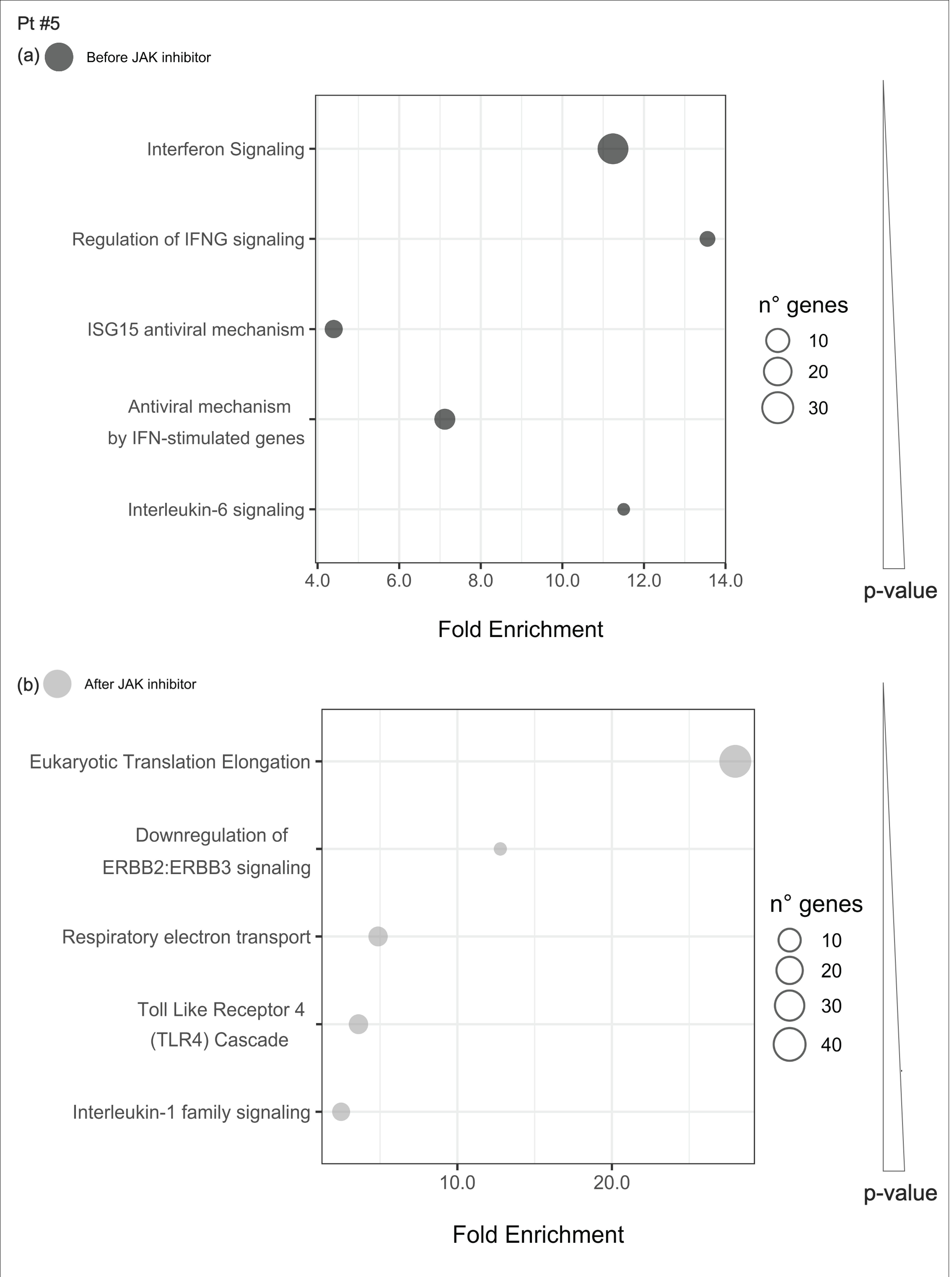
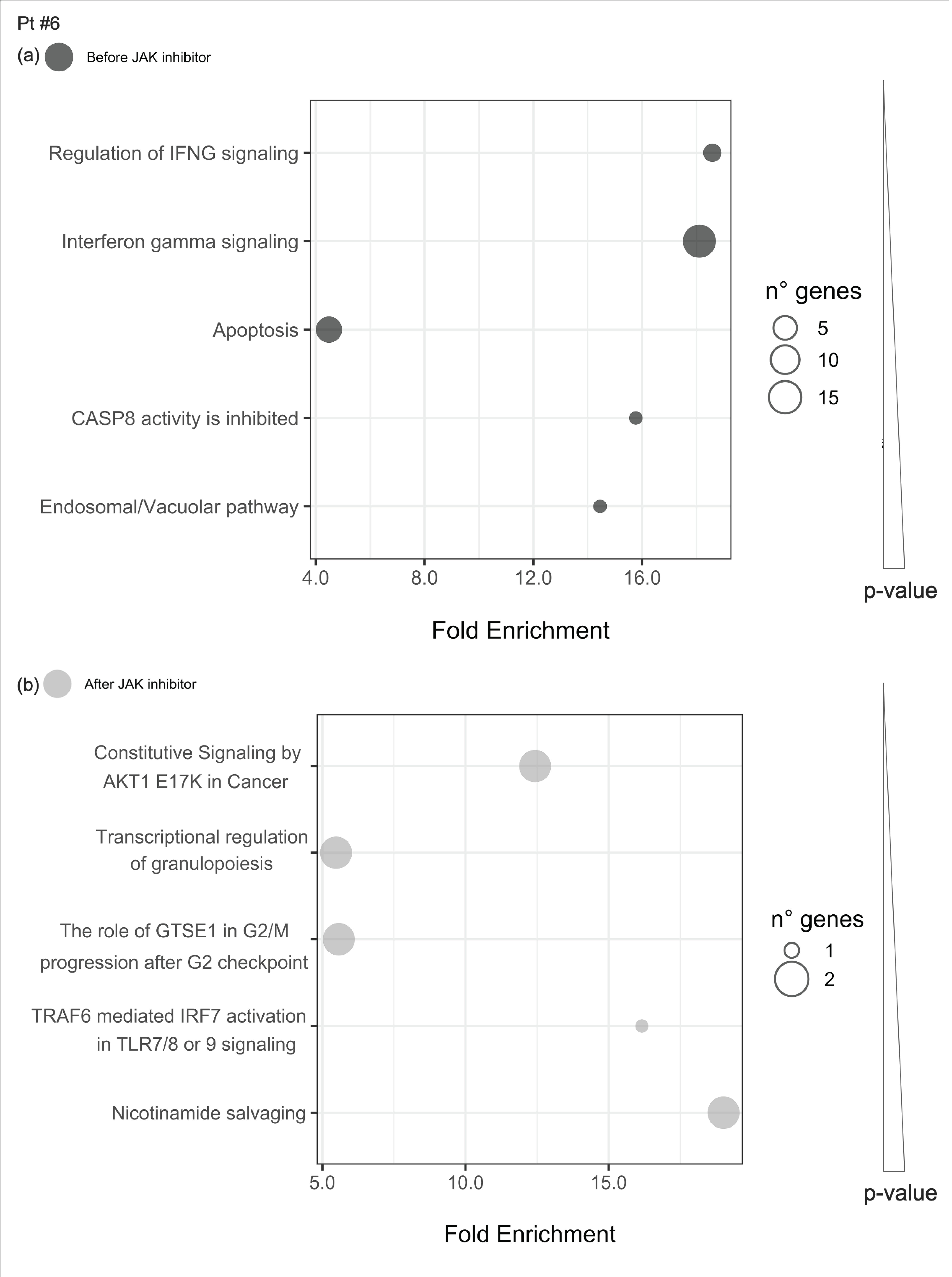
2.4.3. Enriched Pathways before and after JAKinhibs Therapy in Each Patient
2.4.4. Pathways Enriched of Differentially Expressed Genes Either before or after JAKinhibs in Each Patient
2.5. Concomitant Medications and Reported Adverse Events
3. Discussion
4. Materials and Methods
4.1. Off-Label Use of JAK Inhibitors
4.2. Patients
4.3. Sample Collection, RNA Isolation and cDNA Preparation
4.4. IFN Signature Analysis
4.5. RNAseq Analysis
4.6. Cluster Analysis
4.7. Pathway Enrichment Analysis
- The fold enrichment value calculated considering the list of enriched genes in a specific pathway and the number of total input genes.
- The p-value that assesses the strength of the association between the genes of interest and the pathway is not random. The smaller the p-value, the more the probability that the overrepresentation of certain pathways might underline a real biological effect.
- The most enhanced shared pathways before and after the JAKinhib in each patient to evaluate signaling that may be independent of this pharmacological treatment.
- The enriched pathways either before or after JAK treatments in each patient considering up to five signaling, ranked according to their lowest adjusted p-value to examine the possible modulation of JAKinhibs.
4.8. Common DEGs and Pathways Altered Only after JAKinhibs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BCL2A1 | BCL2 Related Protein A1 |
| BRCA2 | Breast cancer gene 2 |
| CAMP | Cathelicidin Antimicrobial Peptide |
| CANDLE | Chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature |
| COPA | COPI coat complex subunit alpha |
| CRP | C-reactive protein |
| CSF | Cerebrospinal fluid |
| CTNNAL1 | Catenin Alpha Like 1 |
| DEFA3 | Defensin Alpha 3 |
| DEG | Differential expressed genes |
| EEF1B2 | Eukaryotic Translation Elongation Factor 1 Beta 2 |
| ESR | Erythrocyte sedimentation rate |
| FBXO7 | F-Box Protein 7 |
| FCRL1 | Fc Receptor Like 1 |
| FUP | Follow-up |
| G6PD | Glucose-6-phosphate dehydrogenase |
| GNG11 | G Protein Subunit Gamma 11 |
| HAGH | Hydroxyacylglutathione Hydrolase |
| HB | Hemoglobin |
| HP | Haptoglobin |
| HPRT1 | Hypoxanthine phosphoribosyl transferase 1 |
| JIA | Juvenile idiopathic arthritis |
| JAK | Janus kinase |
| IFI27 | Interferon alpha inducible protein 27 |
| IFI44L | Interferon inducible protein 44 like |
| IFIH1 | Interferon induced with helicase C domain 1 |
| IFIT1 | Interferon induced protein with tetratricopeptide repeats 1 |
| IFITM3 | Interferon Induced Transmembrane Protein 3 |
| IFN | Interferon |
| IFNGR1 | Interferon gamma receptor 1 |
| IGF2BP2 | Insulin Like Growth Factor 2 MRNA Binding Protein 2 |
| IL1R | Interleukin 1 receptor |
| IL1RAP | Interleukin 1 receptor accessory protein |
| IS | Interferon score |
| ISG15 | Interferon stimulated gene 15 |
| LGALS3 | Galectin 3 |
| LTF | Lactotransferrin |
| MAPK | Mitogen-activated protein kinase |
| MBNL3 | Muscleblind Like Splicing Regulator 3 |
| MRI | Magnetic resonance imaging |
| MXI1 | MAX Interactor 1, Dimerization Protein |
| ND | Not Done |
| PAX5 | Paired Box 5 |
| PDCD10 | Programmed Cell Death 10 |
| PDGFB | Platelet derived growth factor subunit B |
| PDK4 | Pyruvate Dehydrogenase Kinase 4 |
| PI3K | Phosphoinositide 3-kinase |
| PLEKHG1 | Pleckstrin Homology And RhoGEF Domain Containing G1 |
| RIG-1 | Retinoic acid-inducible gene I |
| RMI2 | RecQ mediated genome instability 2 |
| RPL41 | Ribosomal Protein L41 |
| RPS21 | Ribosomal Protein S21 |
| RPS29 | Ribosomal Protein S29 |
| RSAD2 | Radical s-adenosyl methionine domain containing 2 |
| RSL24D1 | Ribosomal L24 Domain Containing 1 |
| SIAH2 | Siah E3 Ubiquitin Protein Ligase 2 |
| SIGLEC1 | Sialic acid binding Ig like lectin 1 |
| SLC14A1 | Solute Carrier Family 14 Member 1 (Kidd Blood Group) |
| SLE | Systemic lupus erythematosus |
| SSA | Anti-Sjögren’s syndrome type A |
| STAT1 | Signal transducer and activator of transcription 1 |
| TMA7 | Translation Machinery Associated 7 Homolog |
| TNFa | Tumor necrosis factor alpha |
| UPL | Universal probe library |
| VWCE | Von Willebrand Factor C And EGF Domains |
| WBC | White blood cells |
| ZNF117 | Zinc Finger Protein 117 |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt#1 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 9 | 83 | 9.9 | 3350 | 12.7 | 107,000 | 855 | 124 |
| After JAKinhibs | 13 | 62 | 0.3 | 2610 | 12.2 | 146,000 | 459 | 69 |
| Last FUP | 12 | 22.4 | 5.5 | 1680 | 14.0 | 130,000 | 702 | 61 |
| Pt#2 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 27 | 29.1 | 1.7 | 5700 | 11.1 | 195,000 | 1645 | 399 |
| After JAKinhibs | 46 | 1.0 | 0.2 | 5110 | 12.4 | 337,000 | 1538 | 368 |
| Last FUP | 22 | 3.0 | 0.2 | 5400 | 12.9 | 252,000 | 1752 | 314 |
| Pt#3 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 68 | 33.4 | 5.2 | 5320 | 12.5 | 357,000 | 1860 | 207 |
| After JAKinhibs | 60 | 32.0 | 2.4 | 10,220 | 11.4 | 318,000 | 1812 | 169 |
| Last FUP | 20 | ND | 12.0 | ND | ND | ND | ND | ND |
| Pt#4 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 120 | 5.5 | 7.9 | 8050 | 11.3 | 499,000 | 1480 | 187 |
| After JAKinhibs | 65 | 2.0 | 3.7 | 7390 | 11.1 | 361,000 | 1613 | 107 |
| Last FUP | 38 | 1.7 | 1.0 | 6450 | 11.8 | 342,000 | 1527 | 91 |
| Pt#5 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 56 | 3.4 | 46.6 | 11,030 | 12.3 | 216,000 | 1870 | 162 |
| After JAKinhibs | 81 | 2.0 | 16.0 | 7650 | 10.3 | 362,000 | 1323 | 185 |
| Last FUP | 69 | 4.0 | 11.6 | 5750 | 11.3 | 507,000 | 1334 | 172 |
| Pt#6 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 33 | 38.8 | 1.4 | 11,030 | 14.3 | 424,000 | 948 | 197 |
| After JAKinhibs | 11 | 47.0 | 0.3 | 7650 | 12.2 | 362,000 | 953 | 147 |
| Last FUP | 10 | 44.2 | 0.3 | 4270 | 13.0 | 359,000 | 1061 | 176 |
| Pt#7 | ESR mm/h | IS | CRP mg/L | WBC/μL | HB g/dL | PLT/μL | IgG mg/dL | IgA mg/dL |
|---|---|---|---|---|---|---|---|---|
| Before JAKinhibs | 39 | 17.7 | 3.9 | 6150 | 12.2 | 272,000 | 863 | 177 |
| After JAKinhibs | 12 | 1.0 | 0.7 | 7550 | 13.0 | 215,000 | 901 | 138 |
| Last FUP | 8 | 1.0 | 0.3 | 9100 | 14.7 | 174,000 | 910 | 125 |
Appendix B

References
- Pandit, A.; Radstake, T.R.D.J. Machine learning in rheumatology approaches the clinic. Nat. Rev. Rheumatol. 2020, 16, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Vanderver, A.; Adang, L.; Gavazzi, F.; McDonald, K.; Helman, G.; Frank, D.B.; Jaffe, N.; Yum, S.W.; Collins, A.; Keller, S.R.; et al. Janus Kinase Inhibition in the Aicardi-Goutières Syndrome. N. Engl. J. Med. 2020, 383, 986–989. [Google Scholar] [CrossRef] [PubMed]
- Karageorgas, T.P.; Tseronis, D.D.; Mavragani, C.P. Activation of type I interferon pathway in systemic lupus erythematosus: Association with distinct clinical phenotypes. J. Biomed. Biotechnol. 2011, 2011, 273907. [Google Scholar] [CrossRef] [PubMed]
- La Torre, F.; Martini, G.; Russo, R.; Katsicas, M.M.; Corona, F.; Calcagno, G.; Falcini, F.; Vittadello, F.; Zulian, F. A preliminary disease severity score for juvenile systemic sclerosis. Arthritis Rheum. 2012, 64, 4143–4150. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; de Jesus, A.A.; Brooks, S.R.; Liu, Y.; Huang, Y.; VanTries, R.; Montealegre Sanchez, G.A.; Rotman, Y.; Gadina, M.; Goldbach-Mansky, R. Development of a Validated Interferon Score Using NanoString Technology. J. Interferon Cytokine Res. 2018, 38, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Higgs, B.W.; Morehouse, C.; de Los Reyes, M.; Trigona, W.; Brohawn, P.; White, W.; Zhang, J.; White, B.; Coyle, A.J.; et al. Development of Potential Pharmacodynamic and Diagnostic Markers for Anti-IFN-α Monoclonal Antibody Trials in Systemic Lupus Erythematosus. Hum. Genom. Proteom. 2009, 2009, 374312. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Morris, J.H.; Cook, H.; Kuhn, M.; Wyder, S.; Simonovic, M.; Santos, A.; Doncheva, N.T.; Roth, A.; Bork, P.; et al. The STRING database in 2017: Quality-controlled protein-protein association networks, made broadly accessible. Nucleic Acids Res. 2017, 45, D362–D368. [Google Scholar] [CrossRef]
- Huang, D.W.; Sherman, B.T.; Lempicki, R.A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 2009, 4, 44–57. [Google Scholar] [CrossRef]
- Huang, d.W.; Sherman, B.T.; Lempicki, R.A. Bioinformatics enrichment tools: Paths toward the comprehensive functional analysis of large gene lists. Nucleic Acids Res. 2009, 37, 1–13. [Google Scholar] [CrossRef]
- Trombetta, A.; Ghirardo, S.; Pastore, S.; Tesser, A.; Piscianz, E.; Tommasini, A.; Bobbo, M.; Taddio, A. Pulmonary arterial hypertension in interferonophaties: A case report and a review of the literature. Pulm. Circ. 2019, 9. [Google Scholar] [CrossRef]
- Tomasi, P.A.; Egger, G.F.; Pallidis, C.; Saint-Raymond, A. Enabling Development of Paediatric Medicines in Europe: 10 Years of the EU Paediatric Regulation. Paediatr. Drugs 2017, 19, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Corny, J.; Lebel, D.; Bailey, B.; Bussières, J.F. Unlicensed and Off-Label Drug Use in Children Before and After Pediatric Governmental Initiatives. J. Pediatr. Pharmacol. Ther. 2015, 20, 316–328. [Google Scholar] [CrossRef]
- Dooms, M.; Cassiman, D.; Simoens, S. Off-label use of orphan medicinal products: A Belgian qualitative study. Orphanet J. Rare Dis. 2016, 11, 144. [Google Scholar] [CrossRef] [PubMed]
- Valencic, E.; Smid, A.; Jakopin, Z.; Tommasini, A.; Mlinaric-Rascan, I. Repositioning Drugs for Rare Immune Diseases: Hopes and Challenges for a Precision Medicine. Curr. Med. Chem. 2018, 25, 2764–2782. [Google Scholar] [CrossRef]
- Claussnitzer, M.; Cho, J.H.; Collins, R.; Cox, N.J.; Dermitzakis, E.T.; Hurles, M.E.; Kathiresan, S.; Kenny, E.E.; Lindgren, C.M.; MacArthur, D.G.; et al. A brief history of human disease genetics. Nature 2020, 577, 179–189. [Google Scholar] [CrossRef]
- Demirkaya, E.; Arici, Z.S.; Romano, M.; Berard, R.A.; Aksentijevich, I. Current State of Precision Medicine in Primary Systemic Vasculitides. Front. Immunol. 2019, 10, 2813. [Google Scholar] [CrossRef] [PubMed]
- Yeo, J.G.; Ng, C.T.; Albani, S. Precision medicine in pediatric rheumatology. Curr. Opin. Rheumatol. 2017, 29, 500–505. [Google Scholar] [CrossRef]
- Carnovale, C.; Brusadelli, T.; Zuccotti, G.; Beretta, S.; Sullo, M.G.; Capuano, A.; Rossi, F.; Moschini, M.; Mugelli, A.; Vannacci, A.; et al. The importance of monitoring adverse drug reactions in pediatric patients: The results of a national surveillance program in Italy. Expert Opin. Drug Saf. 2014, 13 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- McInnes, I.B.; Schett, G. Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet 2017, 389, 2328–2337. [Google Scholar] [CrossRef]
- Muskardin, T.L.W.; Niewold, T.B. Type I interferon in rheumatic diseases. Nat. Rev. Rheumatol. 2018, 14, 214–228. [Google Scholar] [CrossRef]
- Sanchez, G.A.M.; Reinhardt, A.; Ramsey, S.; Wittkowski, H.; Hashkes, P.J.; Berkun, Y.; Schalm, S.; Murias, S.; Dare, J.A.; Brown, D.; et al. JAK1/2 inhibition with baricitinib in the treatment of autoinflammatory interferonopathies. J. Clin. Investig. 2018, 128, 3041–3052. [Google Scholar] [CrossRef] [PubMed]
- Volpi, S.; Insalaco, A.; Caorsi, R.; Santori, E.; Messia, V.; Sacco, O.; Terheggen-Lagro, S.; Cardinale, F.; Scarselli, A.; Pastorino, C.; et al. Efficacy and Adverse Events During Janus Kinase Inhibitor Treatment of SAVI Syndrome. J. Clin. Immunol. 2019, 39, 476–485. [Google Scholar] [CrossRef]
- Landolt-Marticorena, C.; Bonventi, G.; Lubovich, A.; Ferguson, C.; Unnithan, T.; Su, J.; Gladman, D.D.; Urowitz, M.; Fortin, P.R.; Wither, J. Lack of association between the interferon-alpha signature and longitudinal changes in disease activity in systemic lupus erythematosus. Ann. Rheum. Dis. 2009, 68, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Niewold, T.B.; Hua, J.; Lehman, T.J.; Harley, J.B.; Crow, M.K. High serum IFN-alpha activity is a heritable risk factor for systemic lupus erythematosus. Genes Immun. 2007, 8, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, S.; Ohnishi, S.; Ma, N.; Hiraku, Y.; Murata, M. Crosstalk between DNA Damage and Inflammation in the Multiple Steps of Carcinogenesis. Int. J. Mol. Sci. 2017, 18, 1808. [Google Scholar] [CrossRef]
- Souliotis, V.L.; Vlachogiannis, N.I.; Pappa, M.; Argyriou, A.; Ntouros, P.A.; Sfikakis, P.P. DNA Damage Response and Oxidative Stress in Systemic Autoimmunity. Int. J. Mol. Sci. 2019, 21, 55. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, H.C. Chronic inflammation as a promotor of mutagenesis in essential thrombocythemia, polycythemia vera and myelofibrosis. A human inflammation model for cancer development? Leuk Res. 2013, 37, 214–220. [Google Scholar] [CrossRef]
- Ni, L.; Zheng, Y.; Gong, T.; Xiu, C.; Li, K.; Saijilafu; Li, B.; Yang, H.; Chen, J. Proinflammatory macrophages promote degenerative phenotypes in rat nucleus pulpous cells partly through ERK and JNK signaling. J. Cell. Physiol. 2019, 234, 5362–5371. [Google Scholar] [CrossRef]
- Reynolds, J.A.; Briggs, T.A.; Rice, G.I.; Darmalinggam, S.; Bondet, V.; Bruce, E.; Khan, M.; Haque, S.; Chinoy, H.; Herrick, A.L.; et al. Type I interferon in patients with systemic autoimmune rheumatic disease is associated with haematological abnormalities and specific autoantibody profiles. Arthritis Res. Ther. 2019, 21, 147. [Google Scholar] [CrossRef]
- Simonetti, S.; Seijas, A.B.B.; Natalini, A.; Vitale, S.; Runci, D.; Soriani, A.; Di Virgilio, A.; Aricò, E.; Gabriele, L.; Santoni, A.; et al. Dendritic cells modulate c-kit expression on the edge between activation and death. Eur. J. Immunol. 2019, 49, 534–545. [Google Scholar] [CrossRef]
- Shearin, A.L.; Monks, B.R.; Seale, P.; Birnbaum, M.J. Lack of AKT in adipocytes causes severe lipodystrophy. Mol. Metab. 2016, 5, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Dobin, A.; Davis, C.A.; Schlesinger, F.; Drenkow, J.; Zaleski, C.; Jha, S.; Batut, P.; Chaisson, M.; Gingeras, T.R. STAR: Ultrafast universal RNA-seq aligner. Bioinformatics 2013, 29, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Smyth, G.K.; Shi, W. featureCounts: An efficient general purpose program for assigning sequence reads to genomic features. Bioinformatics 2014, 30, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Hartigan, J.A. A k-means clustering algorithm. J. R. Stat. Soc. Ser. C (Appl. Stat.) 1979, 28, 100–108. [Google Scholar]
- Ulgen, E.; Ozisik, O.; Sezerman, O.U. pathfindR: An R Package for Comprehensive Identification of Enriched Pathways in Omics Data Through Active Subnetworks. Front. Genet. 2019, 10, 858. [Google Scholar] [CrossRef]
- Morand, E.F.; Furie, R.; Tanaka, Y.; Bruce, I.N.; Askanase, A.D.; Richez, C.; Bae, S.C.; Brohawn, P.Z.; Pineda, L.; Berglind, A.; et al. Trial of Anifrolumab in Active Systemic Lupus Erythematosus. N. Engl. J. Med. 2020, 382, 211–221. [Google Scholar] [CrossRef]














| Pt | Diagnosis and Symptoms | Medications | |||
|---|---|---|---|---|---|
| Previous Medications | JAKinhib | Concomitant Medications | Adverse Events | ||
| #1 | Monogenic lupus (DNase2 deficiency) Lipodystrophy, arthritis, lupus pernio, distal ulcers, hepatosplenomegaly, recurrent fever, growth deficiency | Corticosteroids, methotrexate, mycophenolate, hydroxychloroquine, etanercept, anakinra, thalidomide, canakinumab, abatacept | Ruxolitinib (7.5 mg/BID) | Corticosteroids, hydroxychloroquine, mepacrine, ambrisentan, tadalafil, iloprost, furosemide, cotrimoxazole | Worsening of lymphopenia |
| #2 | CANDLE Lipodystrophy, arthritis, lupus pernio, distal ulcers, growth deficiency | Cyclosporine, anakinra, IVIG, cyclophosphamide, azathioprine, infliximab, hydroxychloroquine, abatacept, hyperbaric oxygen | Tofacitinib (7.5 mg/BID) | Atorvastatin, corticosteroids | Transient increase of gamma glutamyltransferase and dyslipidemia |
| #3 | COPA Arthritis, cough | Corticosteroids, mycophenolate, hydroxychloroquine, methotrexate | Baricitinib (2 mg/BID) | Mycophenolate, corticosteroids | None |
| #4 | Polyarticular JIA Arthritis, articular deformity | Corticosteroids, methotrexate, etanercept, tocilizumab | Tofacitinib (5 mg/BID) | Methotrexate | None |
| #5 | Weber-Christian Panniculitis Recurrent panniculitis, recurrent fever, arthralgia, fatigue | Corticosteroids, mycophenolate, cyclosporine, anakinra | Baricitinib (2 mg/TID) | Cyclosporine, cotrimoxazole | None |
| #6 | SLE Headache, fatigue, social isolation, fever, malar rash | Corticosteroids, mycophenolate, hydroxychloroquine | Baricitinib (4 mg/QD) | Mycophenolate, Hydroxychloroquine | None |
| #7 | Juvenile systemic sclerosis Raynaud, distal ulcers, stiffness, arthritis | Mycophenolate, corticosteroids, rituximab * | Tofacitinib (5 mg/BID) | Mycophenolate, corticosteroids | None |
| Gene | Patient #1 | Patient #2 | Patient #3 | Patient #4 | Patient #5 | Patient #6 | Patient #7 |
|---|---|---|---|---|---|---|---|
| BCL2A1 | Up-reg | Up-reg | |||||
| CAMP | Up-reg | Up-reg | |||||
| CTNNAL1 | Up-reg | Up-reg | |||||
| DEFA3 | Up-reg | Up-reg | |||||
| EEF1B2 | Up-reg | Up-reg | |||||
| FBXO7 | Up-reg | Up-reg | |||||
| FCRL1 | Up-reg | Up-reg | |||||
| GNG11 | Up-reg | Up-reg | |||||
| HAGH | Up-reg | Up-reg | |||||
| HP | Up-reg | Up-reg | |||||
| IFITM3 | Down-reg | Up-reg | |||||
| IGF2BP2 | Up-reg | Up-reg | |||||
| LGALS3 | Up-reg | Up-reg | |||||
| LTF | Up-reg | Down-reg | |||||
| MBNL3 | Up-reg | Up-reg | |||||
| MXI1 | Up-reg | Up-reg | |||||
| PAX5 | Up-reg | Up-reg | |||||
| PDCD10 | Up-reg | Up-reg | |||||
| PDK4 | Up-reg | Up-reg | |||||
| PLEKHG1 | Up-reg | Up-reg | |||||
| RPL41 | Up-reg | Up-reg | |||||
| RPS21 | Up-reg | Up-reg | |||||
| RPS29 | Up-reg | Up-reg | |||||
| RSL24D1 | Up-reg | Up-reg | Up-reg | ||||
| SIAH2 | Up-reg | Up-reg | |||||
| SLC14A1 | Up-reg | Up-reg | |||||
| TMA7 | Up-reg | Up-reg | |||||
| VWCE | Up-reg | Down-reg | |||||
| ZNF117 | Up-reg | Up-reg |
| Datasets | Subjects | RNAseq Details | |||
|---|---|---|---|---|---|
| Sample/n | Female (n = 9) | Male (n = 4) | Whole Blood Collection/RNA Extraction | RNAseq Library Preparation/Platform | Read Length/Coverage |
| Rheumatologic patient sample before JAKinhibs/ n = 7 | 6 | 1 | PAXgene blood RNA tube/PAXgene Blood RNA Kit | Illumina TruSeq stranded mRNA library protocol/Novaseq | Paired-end 100 bp reads/ 30 M or 60 M reads |
| Rheumatologic patient sample after JAKinhibs/ n = 7 | |||||
| Healthy subjects/ n = 6 | 3 | 3 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pin, A.; Tesser, A.; Pastore, S.; Moressa, V.; Valencic, E.; Arbo, A.; Maestro, A.; Tommasini, A.; Taddio, A. Biological and Clinical Changes in a Pediatric Series Treated with Off-Label JAK Inhibitors. Int. J. Mol. Sci. 2020, 21, 7767. https://doi.org/10.3390/ijms21207767
Pin A, Tesser A, Pastore S, Moressa V, Valencic E, Arbo A, Maestro A, Tommasini A, Taddio A. Biological and Clinical Changes in a Pediatric Series Treated with Off-Label JAK Inhibitors. International Journal of Molecular Sciences. 2020; 21(20):7767. https://doi.org/10.3390/ijms21207767
Chicago/Turabian StylePin, Alessia, Alessandra Tesser, Serena Pastore, Valentina Moressa, Erica Valencic, Anna Arbo, Alessandra Maestro, Alberto Tommasini, and Andrea Taddio. 2020. "Biological and Clinical Changes in a Pediatric Series Treated with Off-Label JAK Inhibitors" International Journal of Molecular Sciences 21, no. 20: 7767. https://doi.org/10.3390/ijms21207767
APA StylePin, A., Tesser, A., Pastore, S., Moressa, V., Valencic, E., Arbo, A., Maestro, A., Tommasini, A., & Taddio, A. (2020). Biological and Clinical Changes in a Pediatric Series Treated with Off-Label JAK Inhibitors. International Journal of Molecular Sciences, 21(20), 7767. https://doi.org/10.3390/ijms21207767