Pravastatin Alleviates Radiation Proctitis by Regulating Thrombomodulin in Irradiated Endothelial Cells

 ,
,
Abstract
:1. Introduction
2. Results
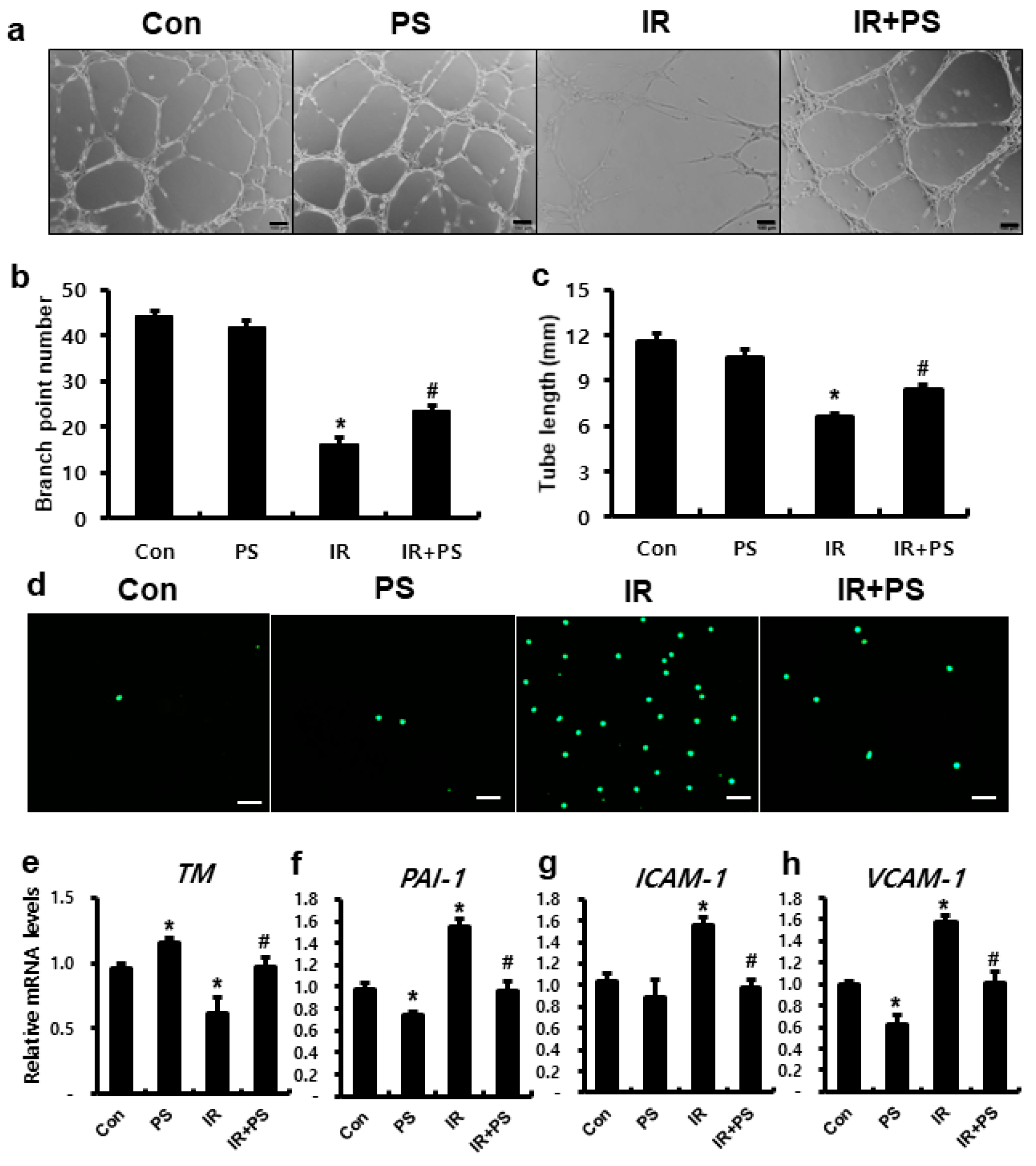
2.1. Pravastatin Inhibited Inflammation Response in Endothelial Cells by Regulating TM
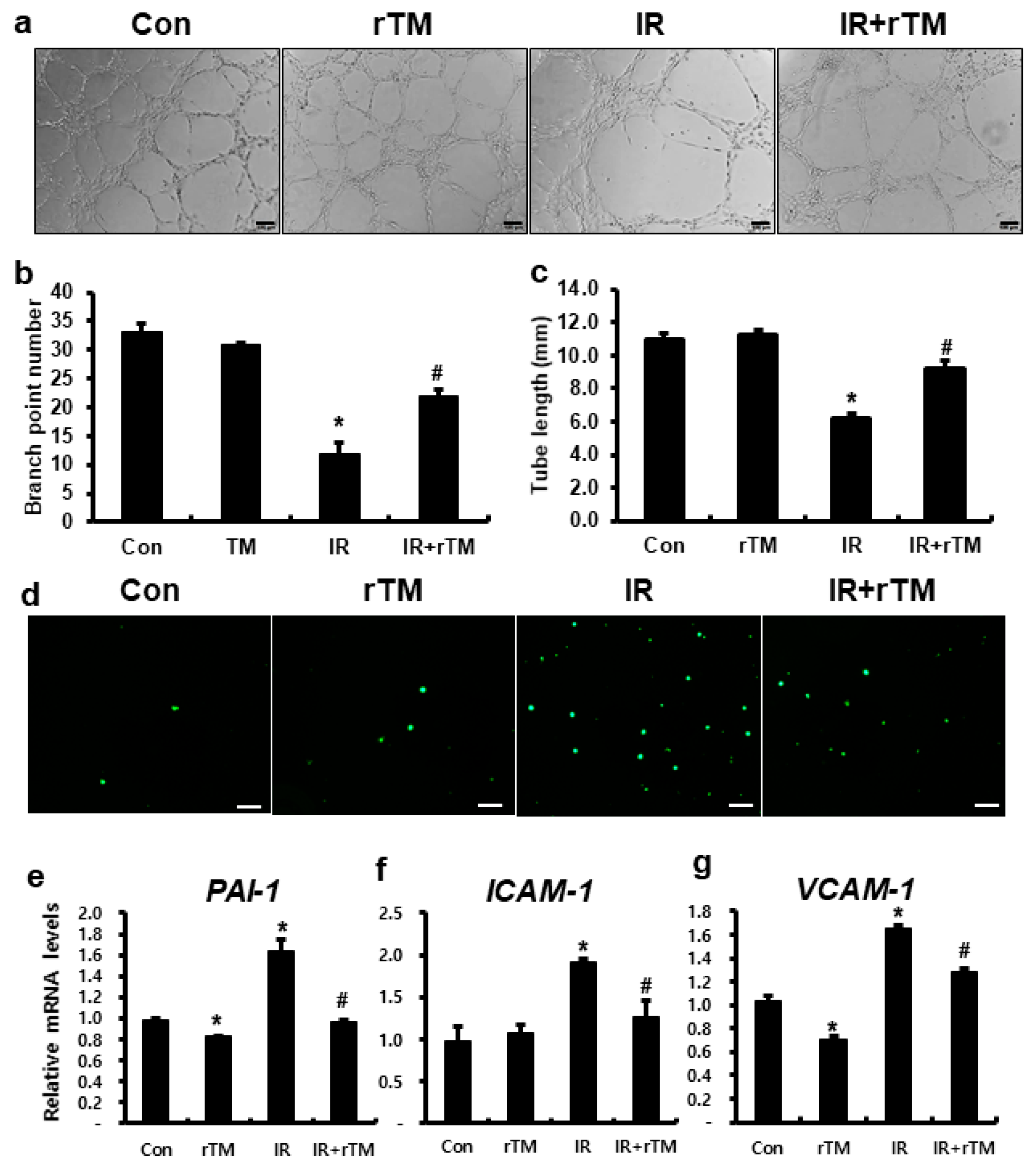
2.2. TM Improved Radiation-Induced Endothelial Dysfunction
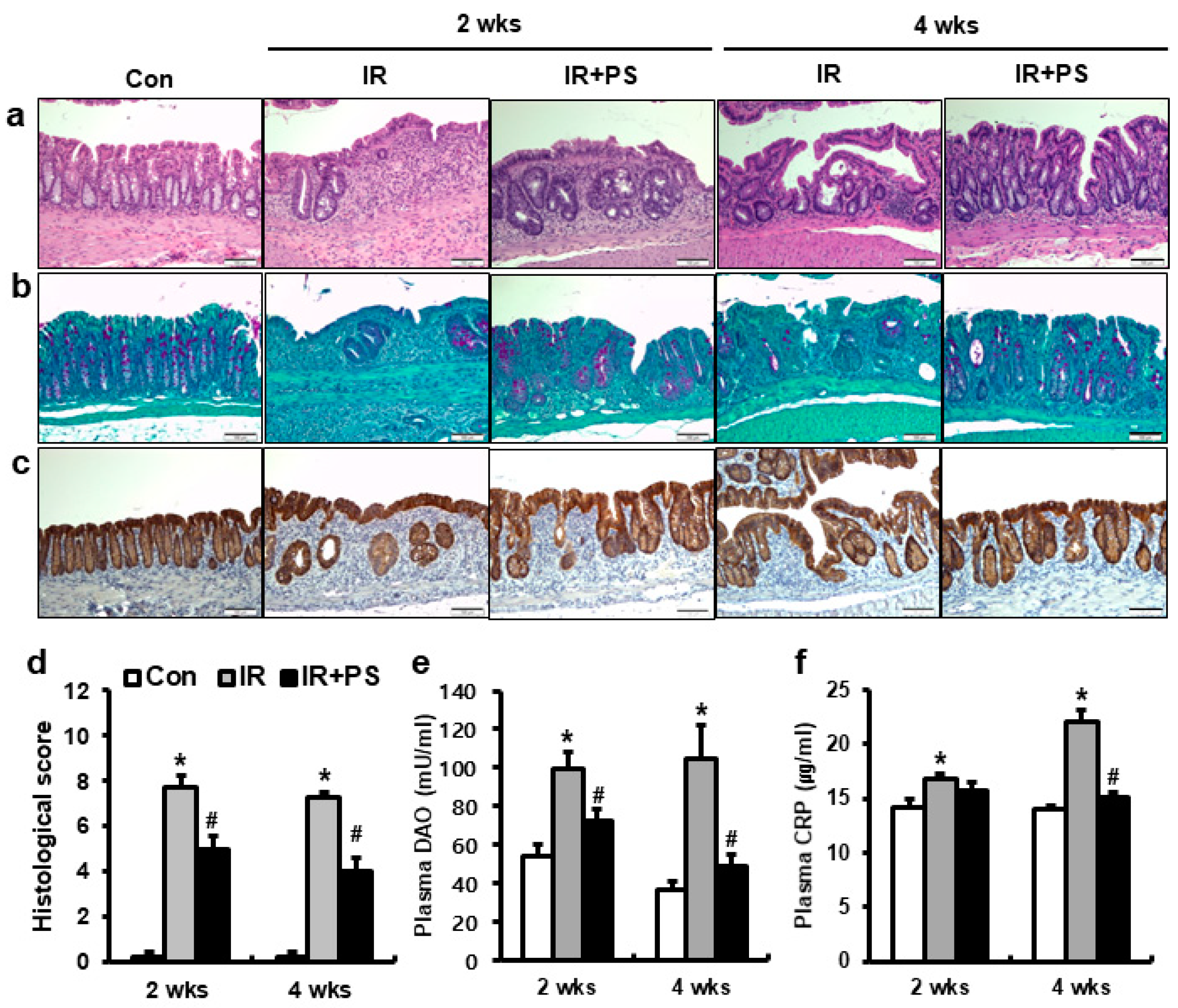
2.3. Pravastatin Mitigated Radiation Proctitis
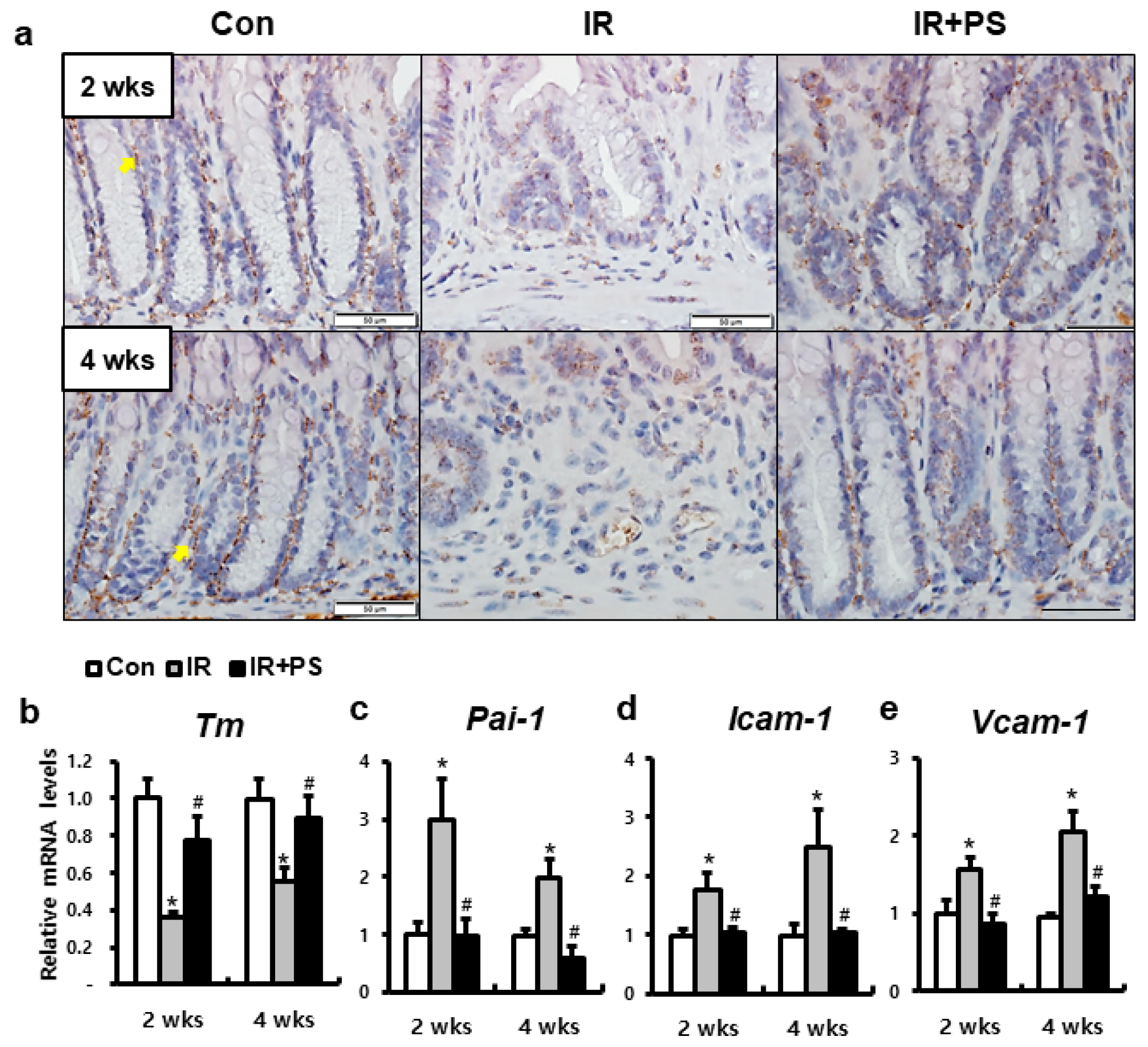
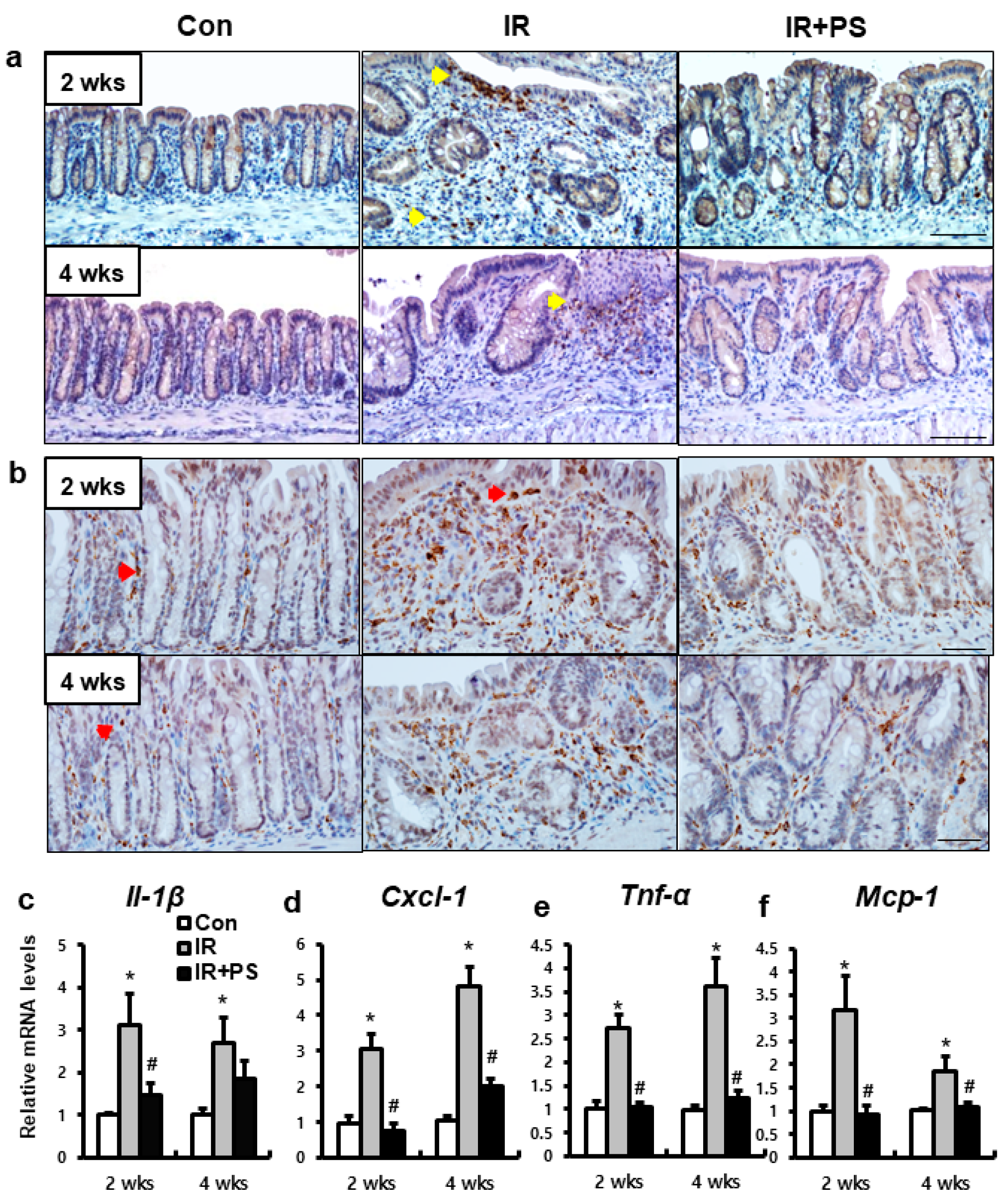
2.4. Pravastatin Accelerated TM Expression in Radiation-Induced Proctitis
2.5. Pravastatin Attenuated Inflammatory Response in Radiation-induced Colorectal Damage
3. Discussion
4. Materials and Methods
4.1. Cell Culture and Treatment
4.2. Capillary-Like Tube Formation Assay
4.3. Leukocyte Adhesion Assay
4.4. RNA Extraction, Reverse Transcription-Polymerase Chain Reaction (RT–PCR), and Real-Time PCR Quantification
4.5. Mice
4.6. Irradiation and Administration of Pravastatin
4.7. Histological Analysis
4.8. Measurements of Plasma DAO and CRP Levels
4.9. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| TM | Thrombomodulin |
| IR | Irradiated |
| PAS | Periodic acid-Schiff base |
| DAO | Diamine oxidase |
| CRP | C-reactive protein |
| ICAM1 | Intercellular adhesion molecule-1 |
| VCAM1 | Vascular cell adhesion molecule-1 |
| PAI-1 | Plasminogen activator inhibitor-1 |
| HUVECs | Human umbilical vein endothelial cells |
References
- Bentzen, S.M. Preventing or reducing late side effects of radiation therapy: Radiobiology meetsmolecular pathology. Nat. Rev. Cancer 2006, 6, 702–713. [Google Scholar] [CrossRef] [PubMed]
- Babb, R.R. Radiation proctitis: A review. Am. J. Gastroenterol. 1996, 91, 1309–1311. [Google Scholar]
- Shadad, A.K.; Sullivan, F.J.; Martin, J.D.; Egan, L.J. Gastrointestinal radiation injury: Prevention and treatment. World J. Gastroenterol. 2013, 19, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Denham, J.W.; O’Brien, P.C.; Dunstan, R.H.; Johansen, J.; See, A.; Hamilton, C.S.; Bydder, S.; Wright, S. Is there more than one late radiation proctitis syndrome? Radiother. Oncol. 1999, 51, 43–53. [Google Scholar] [CrossRef]
- Moore, E.M.; Magrino, T.J.; Johnstone, P.A. Rectal bleeding after radiation therapy for prostate cancer: Endoscopic evaluation. Radiology 2000, 217, 215–218. [Google Scholar] [CrossRef]
- Hovdenak, N.; Fajardo, L.F.; Hauer-Jensen, M. Acute radiation proctitis: A sequential clinicopathologic study during pelvic radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 1111–1117. [Google Scholar] [CrossRef]
- Perez, C.A.; Lee, H.K.; Georgiou, A.; Lockett, M.A. Technical factors affecting morbidity in definitive irradiation for localized carcinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 811–819. [Google Scholar] [CrossRef]
- Garg, A.K.; Mai, W.Y.; McGary, J.E.; Grant, W.H.; Butler, E.B.; Teh, B.S. Radiation proctopathy in the treatment of prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1294–1305. [Google Scholar] [CrossRef]
- Wang, J.; Boerma, M.; Fu, Q.; Hauer-Jensen, M. Significance of endothelial dysfunction in the pathogenesis of early and delayed radiation enteropathy. World J. Gastroenterol. 2007, 13, 3047–3055. [Google Scholar] [CrossRef]
- Milliat, F.; François, A.; Tamarat, R.; Benderitter, M. Role of endothelium in radiation-inducednormal tissue damages. Ann. Cardiol. Angeiol 2008, 57, 139–148. [Google Scholar] [CrossRef]
- Patterson, C.E.; Lum, H. Update on pulmonary edema: The role and regulation of endothelial barrier function. Endothelium 2001, 8, 75–105. [Google Scholar] [CrossRef]
- Vielhauer, V.; Kulkarni, O.; Reichel, C.A.; Anders, H.J. Targeting the recruitment of monocytes and macrophages in renal disease. Semin. Nephrol. 2010, 30, 318–333. [Google Scholar] [CrossRef]
- Yang, G.; Lucas, R.; Caldwell, R.; Yao, L.; Romero, M.J.; Caldwell, R.W. Novel mechanisms of endothelial dysfunction in diabetes. J. Cardiovasc. Dis. Res. 2010, 1, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Cotran, R.S.; Pober, J.S. Cytokine-endothelial interactions in inflammation, immunity, and vascular injury. J. Am. Soc. Nephrol. 1990, 1, 225–235. [Google Scholar]
- Ebnet, K.; Vestweber, D. Molecular mechanisms that control leukocyte extravasation: The selectins and the chemokines. Histochem. Cell Biol. 1999, 112, 1–23. [Google Scholar] [CrossRef]
- Jang, H.; Lee, J.; Park, S.; Kim, J.S.; Shim, S.; Lee, S.B.; Han, S.H.; Myung, H.; Kim, H.; Jang, W.S.; et al. Baicalein Mitigates Radiation-Induced Enteritis by Improving Endothelial Dysfunction. Front. Pharmacol. 2019, 10, 892. [Google Scholar] [CrossRef] [Green Version]
- Esmon, C.T. Coagulation and inflammation. J. Endotoxin Res. 2003, 9, 192–198. [Google Scholar] [CrossRef]
- Califano, F.; Giovanniello, T.; Pantone, P.; Campana, E.; Parlapiano, C.; Alegiani, F.; Vincentelli, G.M.; Turchetti, P. Clinical importance of thrombomodulin serum levels. Eur. Rev. Med. Pharmacol. Sci. 2000, 4, 59–66. [Google Scholar]
- Andrulis, M.; Dietrich, S.; Longerich, T.; Koschny, R.; Burian, M.; Schmitt-Gräf, A.; Schirmacher, P.; Ho, A.D.; Dreger, P.; Luft, T. Loss of endothelial thrombomodulin predicts response to steroid therapy and survival in acute intestinal graft-versus-host disease. Haematologica 2012, 97, 1674–1677. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.B.; Dhainaut, J.F. Activated protein C versus protein C in severe sepsis. Crit. Care Med. 2001, 29, S69–S74. [Google Scholar] [CrossRef]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R.; Hirayama, A.; Aoki, Y.; Aoki, N. Thrombomodulin alfa in the treatment of infectious patients complicated by disseminated intravascular coagulation: Subanalysis from the phase 3 trial. Shock 2011, 35, 349–354. [Google Scholar] [CrossRef]
- Casserly, B.; Gerlach, H.; Phillips, G.S.; Marshall, J.C.; Lemeshow, S.; Levy, M.M. Evaluating the use of recombinant human activated protein C in adult severe sepsis: Results of the Surviving Sepsis Campaign. Crit. Care Med. 2012, 40, 1417–1426. [Google Scholar] [CrossRef]
- Ogawa, Y.; Yamakawa, K.; Ogura, H.; Kiguchi, T.; Mohri, T.; Nakamori, Y. Recombinant human soluble thrombomodulin improves mortality and respiratory dysfunction in patients with severe sepsis. J. Trauma Acute Care Surg. 2012, 1150–1157. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.T.; Chae, H.S.; Kim, J.S.; Kim, H.K.; Cho, Y.S.; Choi, W.; Choi, K.Y.; Rho, S.Y.; Kang, S.J. Thalidomide effect in endothelial cell of acute radiation proctitis. World J. Gastroenterol. 2008, 14, 4779–4783. [Google Scholar] [CrossRef]
- Zhang, S.; Qiu, X.; Zhang, Y.; Fu, K.; Zhao, X.; Wu, J.; Hu, Y.; Zhu, W.; Guo, H. Basic Fibroblast Growth Factor Ameliorates Endothelial Dysfunction in Radiation-Induced Bladder Injury. Biomed. Res. Int. 2015, 2015, 967680. [Google Scholar] [CrossRef] [Green Version]
- Jang, H.; Lee, J.; Park, S.; Myung, H.; Kang, J.; Kim, K.; Kim, H.; Jang, W.S.; Lee, S.J.; Shim, S.; et al. Pravastatin Attenuates Acute Radiation-Induced Enteropathy and Improves Epithelial Cell Function. Front. Pharmacol. 2018, 9, 1215. [Google Scholar] [CrossRef]
- Hayashi, T.; Kusunoki, Y.; Hakoda, M.; Morishita, Y.; Kubo, Y.; Maki, M.; Kasagi, F.; Kodama, K.; Macphee, D.G.; Kyoizumi, S. Radiation dose-dependent increases in inflammatory response markers in A-bomb survivors. Int. J. Radiat. Biol. 2003, 79, 129–136. [Google Scholar] [CrossRef]
- Conway, E.M.; Van de Wouwer, M.; Pollefeyt, S.; Jurk, K.; Van Aken, H.; De Vriese, A.; Weitz, J.I.; Weiler, H.; Hellings, P.W.; Schaeffer, P.; et al. The lectin-like domain of thrombomodulin confers protection from neutrophil-mediated tissue damage by suppressing adhesion molecule expression via nuclear factor kappaB and mitogen-activated protein kinase pathways. J. Exp. Med. 2002, 196, 565–577. [Google Scholar] [CrossRef] [Green Version]
- Vozenin-Brotons, M.C.; Milliat, F.; Linard, C.; Strup, C.; François, A.; Sabourin, J.C.; Lasser, P.; Lusinchi, A.; Deutsch, E.; Girinsky, T.; et al. Gene expression profile in human late radiation enteritis obtained by high-density cDNA array hybridization. Radiat. Res. 2004, 161, 299–311. [Google Scholar] [CrossRef]
- Abderrahmani, R.; François, A.; Buard, V.; Tarlet, G.; Blirando, K.; Hneino, M.; Vaurijoux, A.; Benderitter, M.; Sabourin, J.C.; Milliat, F. PAI-1-dependent endothelial cell death determines severity of radiation-induced intestinal injury. PLoS ONE 2012, 7, e35740. [Google Scholar] [CrossRef]
- Allaire, J.M.; Crowley, S.M.; Law, H.T.; Chang, S.Y.; Ko, H.J.; Vallance, B.A. The Intestinal Epithelium: Central Coordinator of Mucosal Immunity. Trends Immunol. 2018, 39, 677–696. [Google Scholar] [CrossRef]
- Shim, S.; Lee, J.G.; Bae, C.H.; Lee, S.B.; Jang, W.S.; Lee, S.J.; Lee, S.S.; Park, S. Claudin-3 expression in radiation-exposed rat models: A potential marker for radiation-induced intestinal barrier failure. Biochem Biophys Res Commun. 2015, 456, 351–354. [Google Scholar] [CrossRef]
- Hou, Y.; Wang, L.; Zhang, W.; Yang, Z.; Ding, B.; Zhu, H.; Liu, Y.; Qiu, Y.; Yin, Y.; Wu, G. Protective effects of N-acetylcysteine on intestinal functions of piglets challenged with lipopolysaccharide. Amino Acids. 2012, 43, 1233–1242. [Google Scholar] [CrossRef]
- Leiper, K.; Morris, A.I. Treatment of radiation proctitis. Clin. Oncol. 2007, 19, 724–729. [Google Scholar] [CrossRef]
- Moussa, L.; Usunier, B.; Demarquay, C.; Benderitter, M.; Tamarat, R.; Sémont, A.; Mathieu, N. Bowel Radiation Injury: Complexity of the Pathophysiology and Promises of Cell and Tissue Engineering. Cell Transplant. 2016, 25, 1723–1746. [Google Scholar] [CrossRef] [Green Version]
- Cengiz, M.; Akbulut, S.; Atahan, I.L.; Grigsby, P.W. Acute phase response during radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1093–1096. [Google Scholar] [CrossRef]
- Gaugler, M.H.; Vereycken-Holler, V.; Squiban, C.; Vandamme, M.; Vozenin-Brotons, M.C.; Benderitter, M. Pravastatin limits endothelial activation after irradiation and decreases the resulting inflammatory and thrombotic responses. Radiat. Res. 2005, 163, 479–487. [Google Scholar] [CrossRef]
- Holler, V.; Buard, V.; Gaugler, M.H.; Guipaud, O.; Baudelin, C.; Sache, A.; Perez Mdel, R.; Squiban, C.; Tamarat, R.; Milliat, F.; et al. Pravastatin limits radiation-induced vascular dysfunction in the skin. J. Investig. Dermatol. 2009, 129, 1280–1291. [Google Scholar] [CrossRef] [Green Version]
- Weiler, H.; Lindner, V.; Kerlin, B.; Isermann, B.H.; Hendrickson, S.B.; Cooley, B.C.; Meh, D.A.; Mosesson, M.W.; Shworak, N.W.; Post, M.J.; et al. Characterization of a mouse model for thrombomodulin deficiency. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1531–1537. [Google Scholar] [CrossRef] [Green Version]
- Conway, E.M.; Rosenberg, R.D. Tumor necrosis factor suppresses transcription of the thrombomodulin gene in endothelial cells. Mol. Cell Biol. 1988, 8, 5588–5592. [Google Scholar] [CrossRef] [Green Version]
- Boehme, M.W.; Schmitt, W.H.; Youinou, P.; Stremmel, W.R.; Gross, W.L. Clinical relevance of elevated serum thrombomodulin and soluble E-selectin in patients with Wegener’s granulomatosis and other systemic vasculitides. Am. J. Med. 1996, 101, 387–394. [Google Scholar] [CrossRef]
- Ross, C.C.; MacLeod, S.L.; Plaxco, J.R.; Froude, J.W.; Fink, L.M.; Wang, J.; Stites, W.E.; Hauer-Jensen, M. Inactivation of thrombomodulin by ionizing radiation in a cell-free system: Possible implications for radiation responses in vascular endothelium. Radiat. Res. 2008, 169, 408–416. [Google Scholar] [CrossRef]
- Richter, K.K.; Fink, L.M.; Hughes, B.M.; Sung, C.C.; Hauer-Jensen, M. Is the loss of endothelial thrombomodulin involved in the mechanism of chronicity in late radiation enteropathy? Radiother. Oncol. 1997, 44, 65–71. [Google Scholar] [CrossRef]
- Hauer-Jensen, M.; Fink, L.M.; Wang, J. Radiation injury and the protein C pathway. Crit. Care Med. 2004, 32, S325–S330. [Google Scholar] [CrossRef]
- Geiger, H.; Pawar, S.A.; Kerschen, E.J.; Nattamai, K.J.; Hernandez, I.; Liang, H.P.; Fernández, J.Á.; Cancelas, J.A.; Ryan, M.A.; Kustikova, O.; et al. Pharmacological targeting of the thrombomodulin-activated protein C pathway mitigates radiation toxicity. Nat. Med. 2012, 18, 1123–1129. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Species | Primer | Forward (5′–3′) | Reverse (5′–3′) |
|---|---|---|---|
| Human | TM | GGAGCAGCAGTGCGAAGT | GTGGCTGGGAAGTGGAACT |
| PAI-1 | CCCAGCTCATCAGCCACT | GAGGTCGACTTCAGTCTCCAG | |
| ICAM-1 | GGCCGGCCAGCTTATACAC | TAGACACTTGAGCTCGGGCA | |
| VCAM-1 | TCAGATTGGAGACTCAGTCATGT | ACTCCTCACCTTCCCGCTC | |
| GAPDH | GGACTCATGACCACAGTCCATGCC | TCAGGGATGACCTTGCCCACAG | |
| Mouse | Il-1 β | GCAACTGTTCCTGAACTCA | CTCGGAGCCTGTAGTGCAG |
| Cxcl-1 | TGAGCTGCGCTGTCAGTGCCT | AGAAGCCAGCGTTCACCAGA | |
| Tnf-α | GCCTCTTCTCATTCCTGCTT | CACTTGGTGGTTTGCTACGA | |
| Mcp-1 | AGGTCCCTGTCATGCTTCT | CTGCTGGTGATCCTCTTGT | |
| Tm | TCCCAAGTTTCCATGTTTCC | GCATGAGTTGTGTGCTTCGT | |
| Pai-1 | AGGATCGAGGTAAACGAGAGC | GCGGGCTGAGATGACAAA | |
| Icam-1 | GTGATGCTCAGGTATCCATCCA | CACAGTTCTCAAAGCACAGCG | |
| Vcam-1 | GTTCCAGCGAGGGTCTACC | AACTCTTGGCAAACATTAGGTGT | |
| b-actin | TCCCTGGAGAAGAGCTATGA | CGATAAAGGAAGGCTGGAA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.; Kwak, S.-Y.; Park, S.; Kim, K.; Kim, Y.-h.; Na, J.; Kim, H.; Jang, W.-S.; Lee, S.-J.; Kim, M.J.; et al. Pravastatin Alleviates Radiation Proctitis by Regulating Thrombomodulin in Irradiated Endothelial Cells. Int. J. Mol. Sci. 2020, 21, 1897. https://doi.org/10.3390/ijms21051897
Jang H, Kwak S-Y, Park S, Kim K, Kim Y-h, Na J, Kim H, Jang W-S, Lee S-J, Kim MJ, et al. Pravastatin Alleviates Radiation Proctitis by Regulating Thrombomodulin in Irradiated Endothelial Cells. International Journal of Molecular Sciences. 2020; 21(5):1897. https://doi.org/10.3390/ijms21051897
Chicago/Turabian StyleJang, Hyosun, Seo-Young Kwak, Sunhoo Park, Kyuchang Kim, Young-heon Kim, Jiyoung Na, Hyewon Kim, Won-Suk Jang, Sun-Joo Lee, Min Jung Kim, and et al. 2020. "Pravastatin Alleviates Radiation Proctitis by Regulating Thrombomodulin in Irradiated Endothelial Cells" International Journal of Molecular Sciences 21, no. 5: 1897. https://doi.org/10.3390/ijms21051897
APA StyleJang, H., Kwak, S. -Y., Park, S., Kim, K., Kim, Y. -h., Na, J., Kim, H., Jang, W. -S., Lee, S. -J., Kim, M. J., Myung, J. K., & Shim, S. (2020). Pravastatin Alleviates Radiation Proctitis by Regulating Thrombomodulin in Irradiated Endothelial Cells. International Journal of Molecular Sciences, 21(5), 1897. https://doi.org/10.3390/ijms21051897