Behҫet’s Disease, and the Role of TNF-α and TNF-α Blockers


Abstract
:1. Introduction
2. Immuno-Pathogenesis of BD with Emphasis on TNF-α
Genetics of BD
3. Anti-TNF-α Treatment in BD
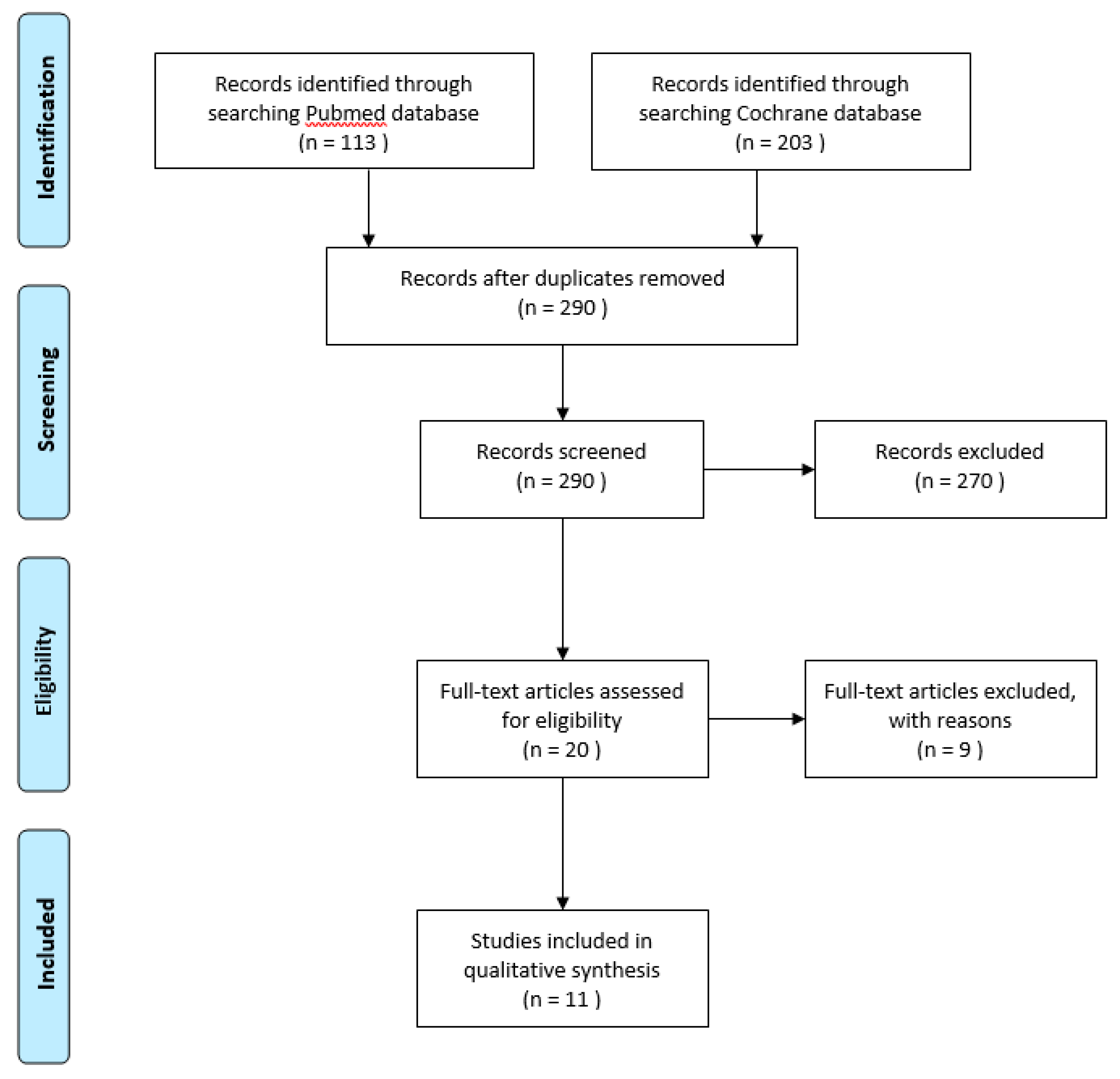
4. Systematic Review Into Anti-TNF-α Treatment
4.1. Efficacy of Treatment
4.2. Adverse Events
5. Discussion
Supplementary Materials
Funding
Conflicts of Interest
References
- Sakane, T.; Takeno, M.; Suzuki, N.; Inaba, G. Behçet’s Disease. N. Engl. J. Med. 1999, 341, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Gul, A. Behçet’s disease as an autoinflammatory disorder. Curr. Drug Target -Inflammation Allergy 2005, 4, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Tong, B.; Liu, X.; Xiao, J.; Su, G. Immunopathogenesis of Behcet’s Disease. Front. Immunol. 2019, 10, 665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evereklioglu, C. Current Concepts in the Etiology and Treatment of Behçet Disease. Surv. Ophthalmol. 2005, 50, 297–350. [Google Scholar] [CrossRef]
- Rivera-López, B.S. Uneven Writing Spaces in Academic Publishing: A Case Study on Internationalisation in the Disciplines of Biochemistry and Molecular Biology 2019. Master’s Thesis, University College London, London, UK, 2019. [Google Scholar]
- Emmi, G.; Silvestri, E.; Della Bella, C.; Grassi, A.; Benagiano, M.; Cianchi, F.; Squatrito, D.; Cantarini, L.; Emmi, L.; Selmi, C.; et al. Cytotoxic Th1 and Th17 cells infiltrate the intestinal mucosa of Behcet patients and exhibit high levels of TNF-α in early phases of the disease. Medicine 2016, 95, e5516. [Google Scholar] [CrossRef]
- Kucuksezer, U.C.; Aktas, E.; Bilgic-Gazioglu, S.; Tugal-Tutkun, I.; Gul, A.; Deniz, G. Natural killer cells dominate a Th-1 polarized response in Behçet’s disease patients with uveitis. Clin. Exp. Rheumatol. 2015, 33. [Google Scholar]
- Zelová, H.; Hošek, J. TNF-α signalling and inflammation: interactions between old acquaintances. Inflamm. Res. 2013, 62, 641–651. [Google Scholar] [CrossRef]
- Liu, X.; Wang, C.; Ye, Z.; Kijlstra, A.; Yang, P. Higher Expression of Toll-like Receptors 2, 3, 4, and 8 in Ocular Behcet’s Disease. Investig. Opthalmology Vis. Sci. 2013, 54, 6012–6017. [Google Scholar] [CrossRef]
- Seoudi, N.; Bergmeier, L.; Hagi-Pavli, E.; Bibby, D.; A Curtis, M.; Fortune, F. The role of TLR2 and 4 in Behçet’s disease pathogenesis. Innate Immun. 2013, 20, 412–422. [Google Scholar] [CrossRef]
- Aderem, A.; Ulevitch, R.J. Toll-like receptors in the induction of the innate immune response. Nature 2000, 406, 782–787. [Google Scholar] [CrossRef]
- Dalghous, A.M.; Freysdottir, J.; Fortune, F. Expression of cytokines, chemokines, and chemokine receptors in oral ulcers of patients with Behcet’s disease (BD) and recurrent aphthous stomatitis is Th1-associated, although Th2-association is also observed in patients with BD. Scand. J. Rheumatol. 2007, 35, 472–475. [Google Scholar] [CrossRef] [PubMed]
- Hamzaoui, K.; Hamzaoui, A.; Guemira, F.; Bessioud, M.; Hamza, M.; Ayed, K. Cytokine profile in Behçet’s disease patients. Scand. J. Rheumatol. 2002, 31, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Düzgün, N.; Ayaslioglu, E.; Tutkak, H.; Aydintuğ, O.T. Cytokine inhibitors: soluble tumor necrosis factor receptor 1 and interleukin-1 receptor antagonist in Behçet’s disease. Rheumatol. Int. 2003, 25, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Gholijani, N.; Ataollahi, M.; Samiei, A.; Aflaki, E.; Shenavandeh, S.; Sarvestani, E.K. An elevated pro-inflammatory cytokines profile in Behcet’s disease: A multiplex analysis. Immunol. Lett. 2017, 186, 46–51. [Google Scholar] [CrossRef]
- Türkcü, F.M.; Şahin, A.; Cingü, A.K.; Kaya, S.; Yüksel, H.; Çinar, Y.; Batmaz, I. Serum omentin, resistin and tumour necrosis factor-α levels in Behcet patients with and without ocular involvement. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1565–1568. [Google Scholar] [CrossRef]
- Sayinalp, N.; I Ozcebe, O.; Ozdemir, O.; Haznedaroğlu, I.C.; Dündar, S.; Kirazli, S. Cytokines in Behçet’s disease. J. Rheumatol. 1996, 23. [Google Scholar]
- Oztas, M.O.; Onder, M.; Gürer, M.A.; Bukan, N.; Sancak, B. Serum interleukin 18 and tumour necrosis factor-alpha levels are increased in Behcet’s disease. Clin. Exp. Dermatol. 2005, 30, 61–63. [Google Scholar] [CrossRef]
- Evereklioglu, C.; Er, H.; Turkoz, Y.; Çekmen, M. Serum levels of TNF-alpha, sIL-2R, IL-6, and IL-8 are increased and associated with elevated lipid peroxidation in patients with Behçet’s disease. Mediat. Inflamm. 2002, 11, 87–93. [Google Scholar] [CrossRef] [Green Version]
- El Boghdady, N.A.; Shaker, O.G. Role of Serum miR-181b, Proinflammatory Cytokine, and Adhesion Molecules in Behçet’s Disease. J. Interf. Cytokine Res. 2019, 39, 347–354. [Google Scholar] [CrossRef]
- Mesquida, M.; Molins, B.; Llorenç, V.; De La Maza, M.S.; Hernández, M.V.; Espinosa, G.; Adán, A. Proinflammatory Cytokines and C-Reactive Protein in Uveitis Associated with Behçet’s Disease. Mediat. Inflamm. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Shaker, O.G.; Tawfic, S.O.; El-Tawdy, A.M.; El-Komy, M.; El Menyawi, M.; Heikal, A.A. Expression of TNF-α, April and BCMA in Behcet’s Disease. J. Immunol. Res. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu El-Asrar, A.M.; Struyf, S.; Kangave, D.; Al-Obeidan, S.S.; Opdenakker, G.; Geboes, K.; Van Damme, J. Cytokine profiles in aqueous humor of patients with different clinical entities of endogenous uveitis. Clin. Immunol. 2011, 139, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.K.; Yu, H.G.; Chung, H.; Park, Y.G. Intraocular Cytokine Environment in Active Behçet Uveitis. Am. J. Ophthalmol. 2006, 142, 429–434.e1. [Google Scholar] [CrossRef] [PubMed]
- Kappen, J.H.; Dik, W.A.; Dingjan, G.M.; Van Daele, P.L.; Hooijkaas, H.; Van Hagen, P.M.; A Van Laar, J. Cytokines in the colon of a patient with Behçet’s disease. Arthritis Res. Ther. 2009, 11, 412. [Google Scholar] [CrossRef] [Green Version]
- Imamura, Y.; Kurokawa, M.S.; Yoshikawa, H.; Nara, K.; Takada, E.; Masuda, C.; Tsukikawa, S.; Ozaki, S.; Matsuda, T.; Suzuki, N. Involvement of Th1 cells and heat shock protein 60 in the pathogenesis of intestinal Behçet’s disease. Clin. Exp. Immunol. 2005, 139, 371–378. [Google Scholar] [CrossRef]
- Ferrante, A.; Ciccia, F.; Principato, A.; Giardina, A.; Impastato, R.; Peralta, S.; Triolo, G. A Th1 but not a Th17 response is present in the gastrointestinal involvement of Behçet’s disease. Clin. Exp. Rheumatol. 2010, 28. [Google Scholar]
- Ertenli, I.; Kiraz, S.; Calgüneri, M.; Celik, I.; Erman, M.; Haznedaroglu, I.C.; Kirazli, S. Synovial fluid cytokine levels in Behçet’s disease. Clin. Exp. Rheumatol. 2002, 19. [Google Scholar]
- Pay, S.; Erdem, H.; Pekel, A.; Simsek, I.; Musabak, U.; Sengul, A.; Dinc, A. Synovial proinflammatory cytokines and their correlation with matrix metalloproteinase-3 expression in Behçet’s disease. Does interleukin-1β play a major role in Behçet’s synovitis? Rheumatol. Int. 2005, 26, 608–613. [Google Scholar] [CrossRef]
- Borhani-Haghighi, A.; Ittehadi, H.; Nikseresht, A.; Rahmati, J.; Poorjahromi, S.G.; Pourabbas, B.; Nazarinia, M.; Habibagahi, Z.; Fattahi, M.J.; Ghaderi, A. CSF levels of cytokines in neuro-Behçet’s disease. Clin. Neurol. Neurosurg. 2009, 111, 507–510. [Google Scholar] [CrossRef]
- Rowlands, D.J.; Islam, M.N.; Das, S.R.; Huertas, A.; Quadri, S.K.; Horiuchi, K.; Inamdar, N.; Emin, M.T.; Lindert, J.; Ten, V.S.; et al. Activation of TNFR1 ectodomain shedding by mitochondrial Ca2+ determines the severity of inflammation in mouse lung microvessels. J. Clin. Investig. 2011, 121, 1986–1999. [Google Scholar] [CrossRef] [Green Version]
- Van Zee, K.J.; Kohno, T.; Fischer, E.; Rock, C.S.; Moldawer, L.L.; Lowry, S.F. Tumor necrosis factor soluble receptors circulate during experimental and clinical inflammation and can protect against excessive tumor necrosis factor alpha in vitro and in vivo. Proc. Natl. Acad. Sci. USA 1992, 89, 4845–4849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turan, B.; Pfister, K.; Diener, P.; Hell, M.; Möller, B.; Boyvat, A.; Ergin, Ş.; Villiger, P.M. Soluble tumour necrosis factor receptors sTNFR1 and sTNFR2 are produced at sites of inflammation and are markers of arthritis activity in Behçet’s disease. Scand. J. Rheumatol. 2008, 37, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Lopalco, G.; Lucherini, O.M.; Lopalco, A.; Venerito, V.; Fabiani, C.; Frediani, B.; Galeazzi, M.; Lapadula, G.; Cantarini, L.; Iannone, F. Cytokine Signatures in Mucocutaneous and Ocular Behçet’s Disease. Front. Immunol. 2017, 8, 431. [Google Scholar] [CrossRef] [PubMed]
- Ihnatko, R.; Kubes, M. TNF signaling: early events and phosphorylation. Gen. Physiol. Biophys. 2007, 26. [Google Scholar]
- Grell, M.; Douni, E.; Wajant, H.; Löhden, M.; Clauss, M.; Maxeiner, B.; Georgopoulos, S.; Lesslauer, W.; Kollias, G.; Pfizenmaier, K.; et al. The transmembrane form of tumor necrosis factor is the prime activating ligand of the 80 kDa tumor necrosis factor receptor. Cell 1995, 83, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Grell, M.; Wajant, H.; Zimmermann, G.; Scheurich, P. The type 1 receptor (CD120a) is the high-affinity receptor for soluble tumor necrosis factor. Proc. Natl. Acad. Sci. USA 1998, 95, 570–575. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, J.; Takai, K.; Takada, E.; Fujiwara, N.; Arimitsu, N.; Ueda, Y.; Wakisaka, S.; Suzuki, T.; Suzuki, N. Possible association of proinflammatory cytokines including IL1β and TNFα with enhanced Th17 cell differentiation in patients with Behcet’s disease. Clin. Rheumatol. 2015, 35, 1857–1863. [Google Scholar] [CrossRef]
- Duhen, T.; Geiger, R.; Jarrossay, D.; Lanzavecchia, A.; Sallusto, F. Production of interleukin 22 but not interleukin 17 by a subset of human skin-homing memory T cells. Nat. Immunol. 2009, 10, 857–863. [Google Scholar] [CrossRef]
- Trifari, S.; Kaplan, C.D.; Tran, E.H.; Crellin, N.K.; Spits, H. Identification of a human helper T cell population that has abundant production of interleukin 22 and is distinct from TH-17, TH1 and TH2 cells. Nat. Immunol. 2009, 10, 864–871. [Google Scholar] [CrossRef]
- Eyerich, S.; Eyerich, K.; Pennino, D.; Carbone, T.; Nasorri, F.; Pallotta, S.; Cianfarani, F.; Odorisio, T.; Traidl-Hoffmann, C.; Behrendt, H.; et al. Th22 cells represent a distinct human T cell subset involved in epidermal immunity and remodeling. J. Clin. Investig. 2009, 119, 3573–3585. [Google Scholar] [CrossRef] [Green Version]
- Sugita, S.; Kawazoe, Y.; Imai, A.; Kawaguchi, T.; Horie, S.; Keino, H.; Takahashi, M.; Mochizuki, M. Role of IL-22– and TNF-α–Producing Th22 Cells in Uveitis Patients with Behçet’s Disease. J. Immunol. 2013, 190, 5799–5808. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Wang, Q.; Zhou, Q.; Wang, C.; Hou, S.; Qi, J.; Kijlstra, A.; Yang, P. Increased Expression of IL-22 Is Associated with Disease Activity in Behcet’s Disease. PLoS ONE 2013, 8, e59009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetin, E.A.; Cosan, F.; Cefle, A.; Deniz, G. IL-22-secreting Th22 and IFN-γ-secreting Th17 cells in Behçet’s disease. Mod. Rheumatol. 2014, 24, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Remmers, E.F.; Cosan, F.; Kirino, Y.; Ombrello, M.; Abaci, N.; Satorius, C.; Le, J.M.; Yang, B.; Korman, B.D.; Çakiris, A.; et al. Genome-wide association study identifies variants in the MHC class I, IL10, and IL23R-IL12RB2 regions associated with Behçet’s disease. Nat. Genet. 2010, 42, 698–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizuki, N.; Meguro, A.; Ota, M.; Ohno, S.; Shiota, T.; Kawagoe, T.; Ito, N.; Kera, J.; Okada, E.; Yatsu, K.; et al. Genome-wide association studies identify IL23R-IL12RB2 and IL10 as Behçet’s disease susceptibility loci. Nat. Genet. 2010, 42, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Kirino, Y.; Bertsias, G.; Ishigatsubo, Y.; Mizuki, N.; Tugal-Tutkun, I.; Seyahi, E.; Özyazgan, Y.; Sacli, F.S.; Erer, B.; Inoko, H.; et al. Genome-wide association analysis identifies new susceptibility loci for Behçet’s disease and epistasis between HLA-B*51 and ERAP1. Nat. Genet. 2013, 45, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Guasp, P.; Barnea, E.; González-Escribano, M.F.; Reinoso, A.J.; Regueiro, J.; Admon, A.; De Castro, J.A.L. The Behçet’s disease-associated variant of the aminopeptidase ERAP1 shapes a low-affinity HLA-B*51 peptidome by differential subpeptidome processing. J. Boil. Chem. 2017, 292, 9680–9689. [Google Scholar] [CrossRef] [Green Version]
- Allen, R.D. Polymorphism of the human TNF-α promoter — random variation or functional diversity? Mol. Immunol. 1999, 36, 1017–1027. [Google Scholar] [CrossRef]
- Higuchi, T.; Seki, N.; Kamizono, S.; Yamada, A.; Kimura, A.; Kato, H.; Itoh, K. Polymorphism of the 5′-flanking region of the human tumor necrosis factor (TNF)-α gene in Japanese. Tissue Antigens 1998, 51, 605–612. [Google Scholar] [CrossRef]
- Zhang, M.; Xu, W.-D.; Wen, P.-F.; Liang, Y.; Liu, J.; Pan, H.-F.; Ye, N.-Q. Polymorphisms in the tumor necrosis factor gene and susceptibility to Behcet’s disease: An updated meta-analysis. Mol. Vis. 2013, 19, 1913–1924. [Google Scholar]
- Abdolmohammadi, R.; Bonyadi, M. Polymorphisms of Promoter Region ofTNF-αGene in Iranian Azeri Turkish Patients with Behçet’s Disease. J. Korean Med Sci. 2017, 32, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tracey, D.; Klareskog, L.; Sasso, E.H.; Salfeld, J.G.; Tak, P.-P. Tumor necrosis factor antagonist mechanisms of action: A comprehensive review. Pharmacol. Ther. 2008, 117, 244–279. [Google Scholar] [CrossRef] [PubMed]
- Criteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s Disease. Lancet 1990, 335.
- Melikoglu, M.; Fresko, I.; Mat, C.; Ozyazgan, Y.; Gogus, F.; Yurdakul, S.; Hamuryudan, V.; Yazici, H. Short-term trial of etanercept in Behçet’s disease: a double blind, placebo controlled study. J. Rheumatol. 2005, 32, 98–105. [Google Scholar]
- Markomichelakis, N.; Delicha, E.; Masselos, S.; Fragiadaki, K.; Kaklamanis, P.; Sfikakis, P.P. A single infliximab infusion vs corticosteroids for acute panuveitis attacks in Behcet’s disease: a comparative 4-week study. Rheumatol. 2010, 50, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.; Ji, D.-N.; Shen, Y.; Guan, J.-I.; Zheng, S.b. Mucosal Healing at 14 Weeks Predicts better Outcome in Low-dose Infliximab Treatment for Chinese Patients with Active Intestinal Behcet’s Disease. Ann. Clin. Lab. Sci. 2017, 47, 171–177. [Google Scholar]
- Martín-Varillas, J.L.; Calvo-Río, V.; Beltran, E.; Sánchez-Bursón, J.; Mesquida, M.; Adan, A.; Hernández, M.V.; Garfella, M.H.; Pascual, E.V.; Martínez-Costa, L.; et al. Successful Optimization of Adalimumab Therapy in Refractory Uveitis Due to Behçet’s Disease. Ophthalmol. 2018, 125, 1444–1451. [Google Scholar] [CrossRef] [Green Version]
- Miyagawa, I.; Nakano, K.; Iwata, S.; Nakayamada, S.; Saito, K.; Hanami, K.; Fukuyo, S.; Kubo, S.; Kawabe, A.; Miyazaki, Y.; et al. Comparative study of corticosteroid monotherapy, and TNF inhibitors with or without corticosteroid in patients with refractory entero-Behcet’s disease. Arthritis Res. Ther. 2019, 21, 151. [Google Scholar] [CrossRef] [Green Version]
- Tabbara, K.; Al-Hemidan, A.I. Infliximab Effects Compared to Conventional Therapy in the Management of Retinal Vasculitis in Behçet Disease. Am. J. Ophthalmol. 2008, 146, 845–850.e1. [Google Scholar] [CrossRef]
- Yamada, Y.; Sugita, S.; Tanaka, H.; Kamoi, K.; Kawaguchi, T.; Mochizuki, M. Comparison of infliximab versus ciclosporin during the initial 6-month treatment period in Behcet disease. Br. J. Ophthalmol. 2009, 94, 284–288. [Google Scholar] [CrossRef]
- Takeuchi, M.; Asukata, Y.; Kawagoe, T.; Ito, N.; Nishide, T.; Mizuki, N. Infliximab Monotherapy Versus Infliximab and Colchicine Combination Therapy in Patients with Behçet’s Disease. Ocul. Immunol. Inflamm. 2012, 20, 193–197. [Google Scholar] [CrossRef]
- Emmi, G.; Vitale, A.; Silvestri, E.; Boddi, M.; Becatti, M.; Fiorillo, C.; Fabiani, C.; Frediani, B.; Emmi, L.; Di Scala, G.; et al. Adalimumab-Based Treatment Versus Disease-Modifying Antirheumatic Drugs for Venous Thrombosis in Behçet’s Syndrome. Arthritis Rheumatol. 2018, 70, 1500–1507. [Google Scholar] [CrossRef] [Green Version]
- Keino, H.; A Okada, A.; Watanabe, T.; Taki, W. Decreased ocular inflammatory attacks and background retinal and disc vascular leakage in patients with Behcet’s disease on infliximab therapy. Br. J. Ophthalmol. 2010, 95, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Guzelant, G.; Ucar, D.; Esatoglu, S.N.; Hatemi, G.; Ozyazgan, Y.; Yurdakul, S.; Seyahi, E.; Yazici, H.; Hamuryudan, V. Infliximab for uveitis of Behçet’s syndrome: a trend for earlier initiation. Clin Exp Rheumatol. 2017, 35, 86–89. [Google Scholar] [PubMed]
- Accardo-Palumbo, A.; Giardina, A.; Ciccia, F.; Ferrante, A.; Principato, A.; Impastato, R.; Giardina, E.; Triolo, G. Phenotype and functional changes of Vγ9/Vδ2 T lymphocytes in Behçet’s disease and the effect of infliximab on Vγ9/Vδ2 T cell expansion, activation and cytotoxicity. Arthritis Res. Ther. 2010, 12, R109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Houwen, T.B.; Van Hagen, P.M.; Timmermans, W.M.; Bartol, S.J.; Lam, K.H.; Kappen, J.H.; Van Laar, J.A.M.; Van Zelm, M.C. Chronic signs of memory B cell activation in patients with Behçet’s disease are partially restored by anti-tumour necrosis factor treatment. Rheumatol. 2016, 56, 134–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugita, S.; Kawazoe, Y.; Imai, A.; Yamada, Y.; Horie, S.; Mochizuki, M. Inhibition of Th17 differentiation by anti-TNF-alpha therapy in uveitis patients with Behçet’s disease. Arthritis Res. Ther. 2012, 14, R99. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author (Trial) | Year | Patients | Study | Duration of Follow Up | Numbers Included | Outcome | Treatment | Comparator | p-Value | Adverse Events |
|---|---|---|---|---|---|---|---|---|---|---|
| Melikoglu | 2005 | Muco- cutaneous BD | Treatment | 3 months | Treatment group | Primary outcome | decrease in pathergy positivity | Treatment | ||
| ETC (25 mg, twice a week) | 20 patients | suppression of pathergy and MSU | 58% | 58% | ns | 1 diarrhoe | ||||
| decrease in MSU, mm2 | ||||||||||
| 1144 | 944 | ns | ||||||||
| Comparator | Comparator group | Secundary outcome | % patients free of nodular lesions | Comparator | ||||||
| Placebo | 20 patients | difference in mean numbers of mucocutaneous lesions and swollen joints | 85% | 25% | p = 0.0002 | 1 elevated liver enzymes | ||||
| % patients free of oral ulceration | ||||||||||
| 45% | 5% | p = 0.0017 | ||||||||
| Markomichelakis | 2011 | BD uveitis | Treatment | 1 month | Treatment group | Primary outcome | decrease in logMAR transformed VA | Treatment | ||
| IFX 5 mg/kg single gift | 19 eyes | visual acuity, logMAR transformed | 1.2 -> 0.5 | 1.6 -> 0.7 | ns | None | ||||
| Comparator | Comparator group | Secundary outcome | decrease in total inflammation score | Comparator | ||||||
| CCS* | 8/8 eyes | ao total inflammation score | largest decrease in IFX on day 14 | p = 0.010 | ocular hypertension in 4 triamcinolon treated eyes | |||||
| Zou | 2017 | Intestinal BD | Treatment | 30 weeks | Treatment group | Primary outcome | corticosteroid-free clinical remission, no (%) | Treatment | ||
| IFX 3.5 mg/kg | 10 patients | corticosteroid-free clinical remission | 4 (40%) | 6 (60%) | p = 0.371 | 1 eczema; topical therapy and 1 common cold | ||||
| Comparator | Comparator group | Secundary outcome | mucosal healing at week 14, no (%) | Comparator | ||||||
| IFX 5 mg/kg | 10 patients | endoscopic mucosal healing | 6 (60%) | 6 (60%) | p = 1.0 | none | ||||
| Martin Varillas | 2018 | BD uveitis | Treatment | 34 months | Treatment group | Primary outcome | relapses, n (per 100 patients/year) | Treatment | ||
| ADA optimized dose | 23 patients | relapse of uveitis | 2 (3.0) | 4 (4.4) | p = 0.66 | None | ||||
| Comparator | 26 months | Comparator group | Secundary outcome | costs (mean), euros per year | Comparator | |||||
| Non optimized ADA | 42 patients | costs | 6101,25 | 12339,48 | p < 0.01 | lymphoma, pneumonia, Ecoli, local reaction (1 each) | ||||
| Author (Trial) | Year | Patients | Study | Duration of Follow Up | Numbers Included | Outcome | Treatment | Comparator | p-Value | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tabbara | 2008 | BD uveitis | Treatment | 36 months | Treatment | Primary outcome | Mean no. of relapses (range) | Treatment | |||
| IFX*, CCS, AZA | 10 patients | number of relapse | 1.2 (0 to 4) | 6.3 (4 to 7) | p < 0.001 | 2 mild infusion reactions, 1 infection (perianal abces) | |||||
| Comparator | 30 months | Comparator | Secundary outcome | Patients with good BCVA¥ (%) | Comparator | ||||||
| CCS, CsA, AZA, MTX | 33 patients | BCVA | 50% | 6% | p = 0.0059 | 4 hypertension, 5 renal function decrease, 3 elevated liver enzymes, 7 hyperglycemia | |||||
| Yamada | 2010 | BD uveitis | Treatment | 6 months | Treatment | Primary outcome | Mean no. of relapses (SD) | Treatment | |||
| IFX** | 17 patients | number of relapse | 0.4 (±1.0) | 1.2 (±1.2) | p < 0.05 | 9 skin symptoms (eruptions, itching, atopic dermatitis); topical therapy | |||||
| Comparator | Comparator | Secundary outcome | Improved/unchanged BCVA (%) | Comparator | |||||||
| CsA | 20 patients | BCVA | 97% | 93% | ns | 1 neurologic symptoms and renal toxicity; dose reduction | |||||
| Takeuchi | 2012 | BD uveitis | Treatment | 25 months | Treatment | Primary outcome | Mean no. of relapses/6 months (SD) | Treatment | |||
| IFX** | 7 patients | number of relapse | 0.22 (±0.28) | 0.18 (±0.19) | ns | 1 infusion reaction | |||||
| Comparator | 33 months | Comparator | Secundary outcome | Improved/unchanged BCVA (%) | Comparator | ||||||
| IFX**, colchicine | 7 patients | BCVA | 100% | 83.3% | ns | CMV infection; cured by valganciclovir | |||||
| Emmi | 2018 | Vascular BD | Treatment | 26 months | Treatment | Primary outcome | Complete or partial response, no (%) | Treatment | |||
| ADA | 35 patients | vascular response (ultrasound) | 34 (97.1%) | 23 (66%) | p = 0.001 | 2 urticarial skin rash, 1 pneumonia, 1 HSV reactivation | |||||
| Comparator | Comparator | Secundary outcome | Mean time (SD), weeks | Comparator | |||||||
| DMARDs | 35 patients | time to achieve vascular response | 3.7 (±1.7) | 6.3 (±1.2) | p < 0.0001 | 2 adverse events | |||||
| Miyagawa | 2019 | Intestinal BD | Treatment | 12 months | Treatment | Primary outcome | Patients with cured ulcer, no (%) | Treatment | |||
| TNF-i with CCS | 20 patients | ulcer cure rate (endoscopic) | 12 (60%) | 13 (45%) | 3 (13.6%) | 1 bacterial infection | |||||
| Comparator | Comparator | Secundary outcome | Patients with improvement of ulcer, no (%) | Comparator | |||||||
| TNF-i without CCS | 29 patients | ulcer improvement rate | 12 (60%) | 15 (57%) | 6 (27%) | none described | |||||
| Comparator | Comparator | Comparator | |||||||||
| CCS | 22 patients | ||||||||||
| Author (Trial) | Year | Patients | Study | Duration of Follow Up | Numbers Included | Outcome | Treatment | Comparator | p-Value | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Keino | 2017 | BD uveitis | Treatment | 24 months | Treatment | Primary outcome | Mean no. of relapses/6 months (SD) | Treatment | |||
| Uveitis <18 months | 6 patients | number of relapse | no significant differences | 5 viral infection | |||||||
| Comparator | Comparator | Secundary outcome | Vascular leakage score | Comparator | |||||||
| Uveitis >18 months | 7 patients | ao vascular leakage score | significant decrease in <18mcompared to >18m after year 1 and 2 | 1 viral infection, 1 bacterial pharyngitis responding to antibiotic therapy | |||||||
| Guzelant | 2017 | BD uveitis | Treatment | 12 months | Treatment | Primary outcome | Stable VA after IFX in R eye, n (%) | Treatment | |||
| After January 2013 | 14 patients | BCVA | 9 (64) | 12 (28) | p = 0.01 | 3 allergic reactions, 1 pulmonary TBC | |||||
| Comparator | 40 months | Comparator | Secundary outcome | Number of relapses, n (%) | Comparator | ||||||
| Before January 2013 | 43 patients | number of relapse | 1 (7) | 23 (53.4) | p = 0.002 | 2 allergic reactions, 1 pulmonary TBC, 1 lung nodule | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Houwen, T.; van Laar, J. Behҫet’s Disease, and the Role of TNF-α and TNF-α Blockers. Int. J. Mol. Sci. 2020, 21, 3072. https://doi.org/10.3390/ijms21093072
van der Houwen T, van Laar J. Behҫet’s Disease, and the Role of TNF-α and TNF-α Blockers. International Journal of Molecular Sciences. 2020; 21(9):3072. https://doi.org/10.3390/ijms21093072
Chicago/Turabian Stylevan der Houwen, Tim, and Jan van Laar. 2020. "Behҫet’s Disease, and the Role of TNF-α and TNF-α Blockers" International Journal of Molecular Sciences 21, no. 9: 3072. https://doi.org/10.3390/ijms21093072
APA Stylevan der Houwen, T., & van Laar, J. (2020). Behҫet’s Disease, and the Role of TNF-α and TNF-α Blockers. International Journal of Molecular Sciences, 21(9), 3072. https://doi.org/10.3390/ijms21093072