
Combination Chemotherapy with Cisplatin and Chloroquine: Effect of Encapsulation in Micelles Formed by Self-Assembling Hybrid Dendritic–Linear–Dendritic Block Copolymers

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Results
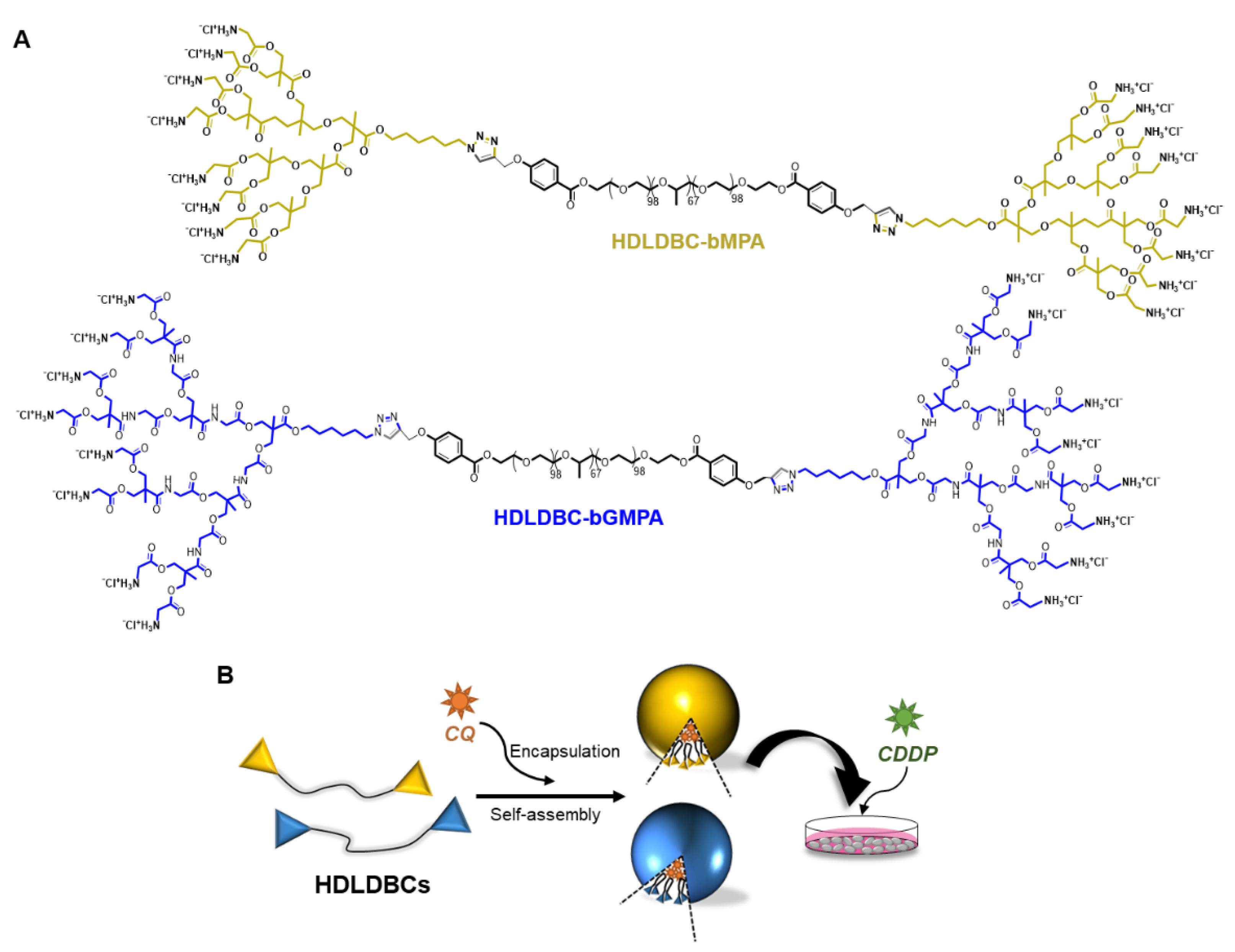
2.1. Synthesis and Design of the Hybrid Dendritic–Linear–Dendritic Block Copolymers (HDLDBCs)
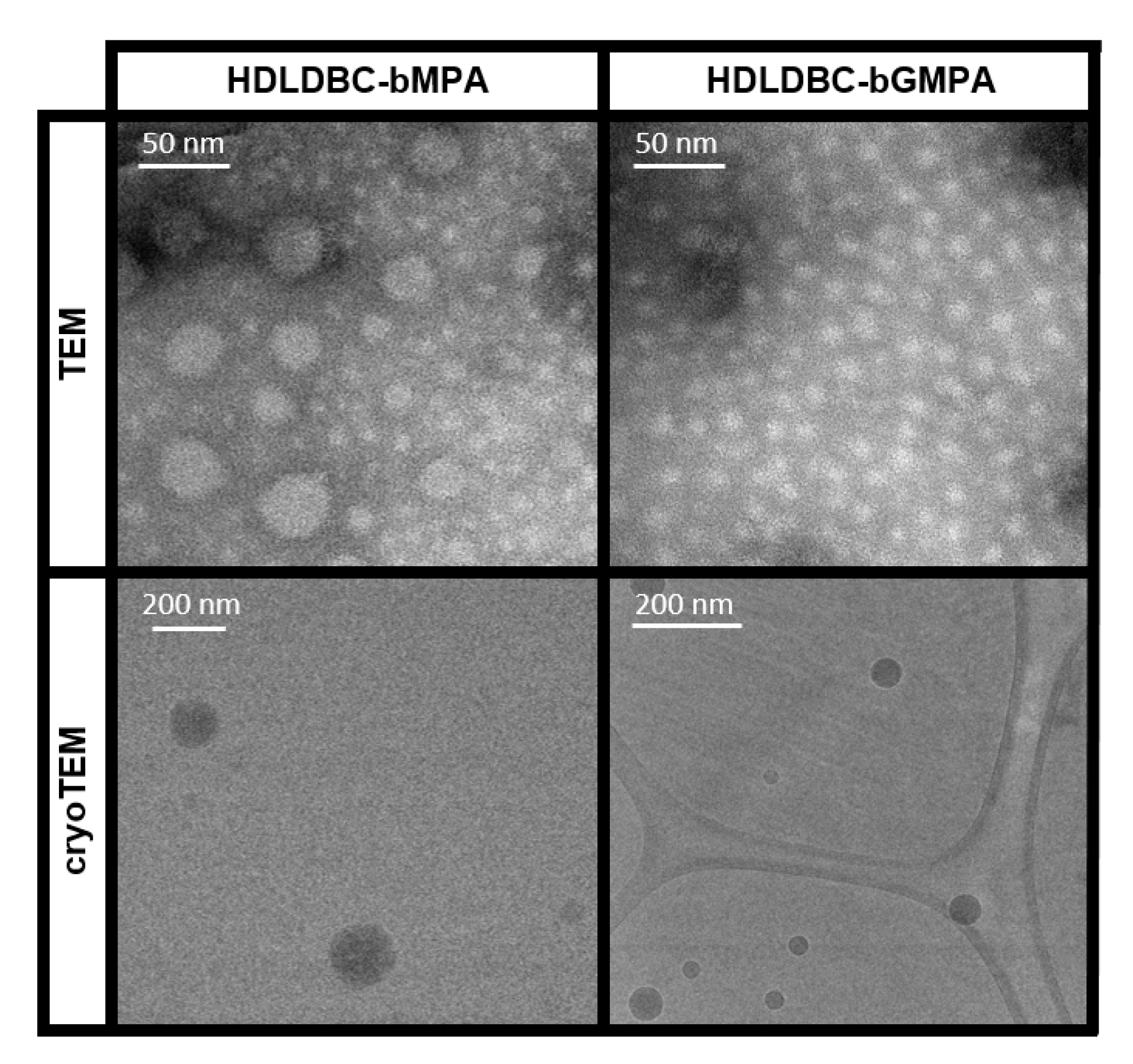
2.2. Self-Assembly of the HDLDBCs
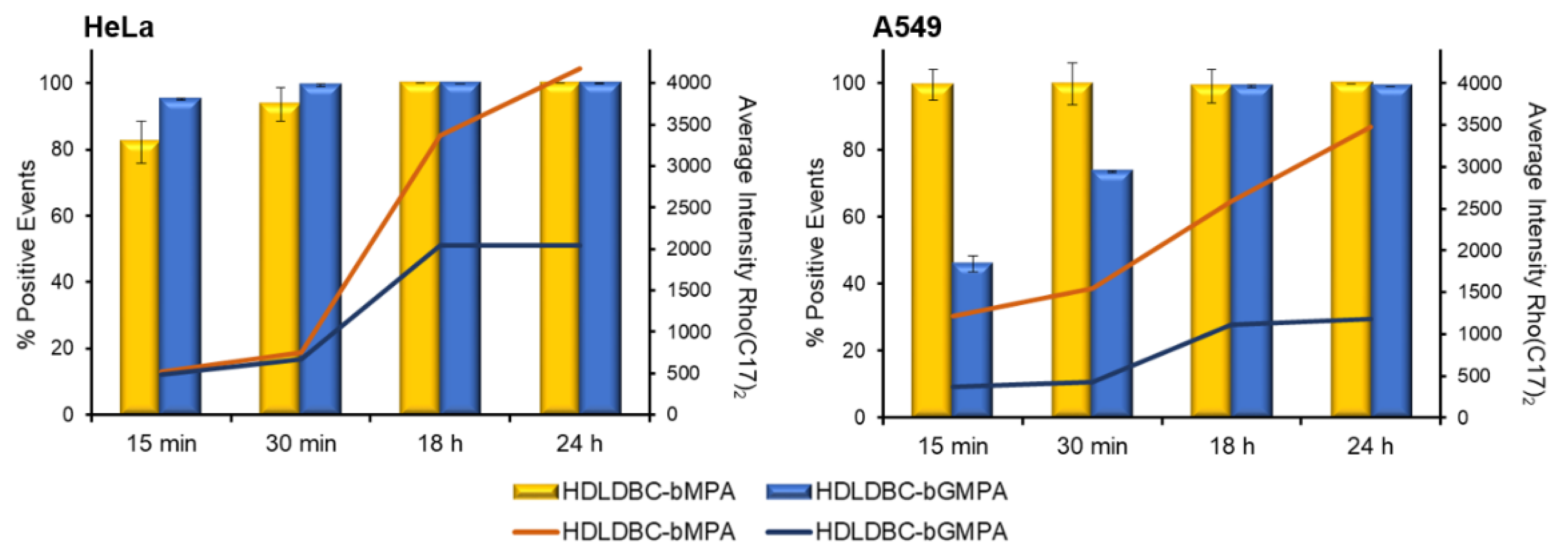
2.3. Cell Internalization of HDLDBC Micelles
2.4. Drug Encapsulation in HDLDBC Nanoaggregates and Releasing Profiles
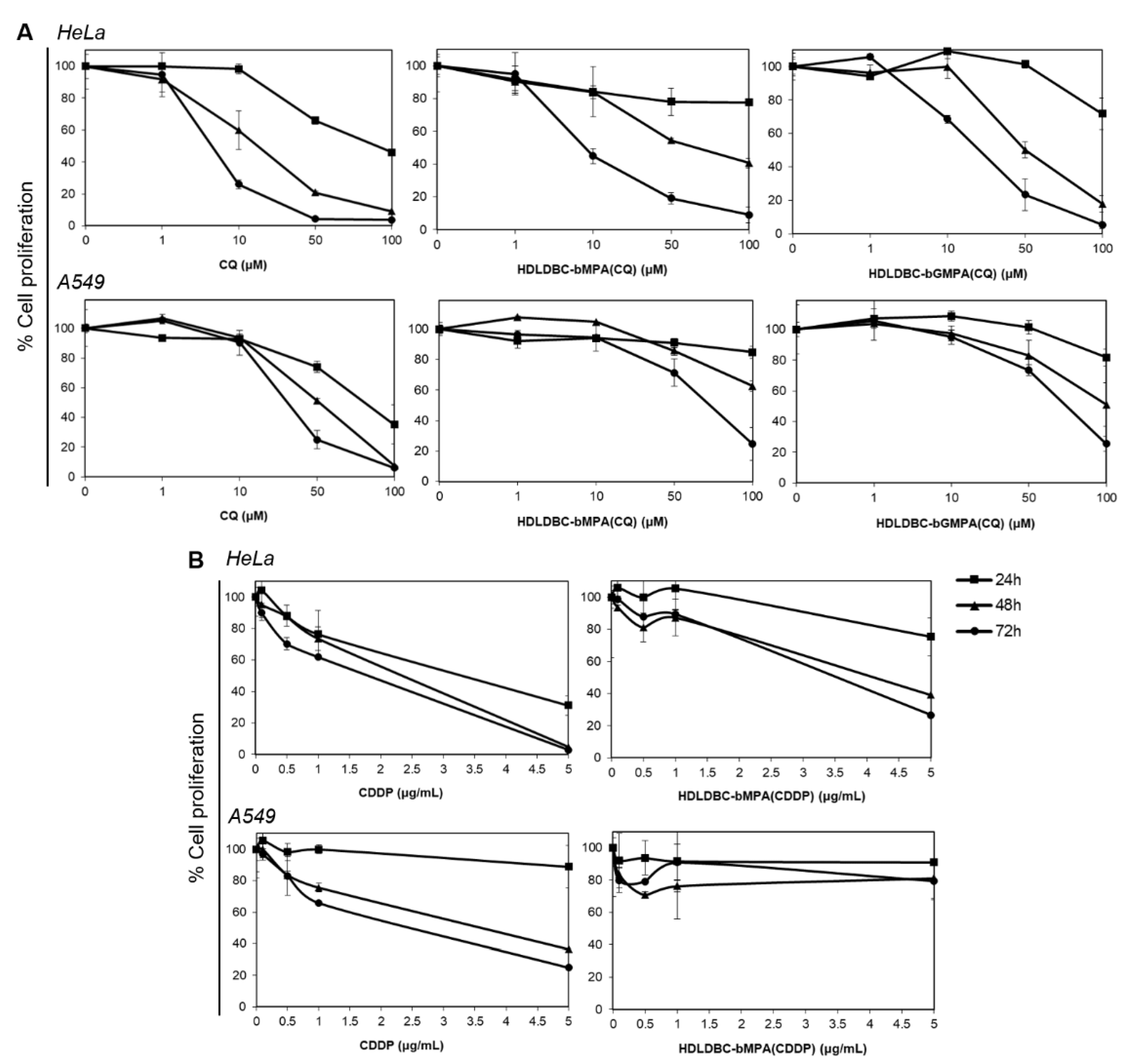
2.5. Effect of Free and Encapsulated CQ and CDDP on the Proliferation of HeLa and A549 Cells
2.6. Effect of Combination of CQ and CDDP on the Proliferation of Tumor Cells and Fibroblasts
2.7. Effect on Cell Proliferation of a Combined Treatment with CQ Encapsulated in HDLDBCs and Free CDDP Compared to the Use of Free Drugs and Degree of Interaction of the Drugs
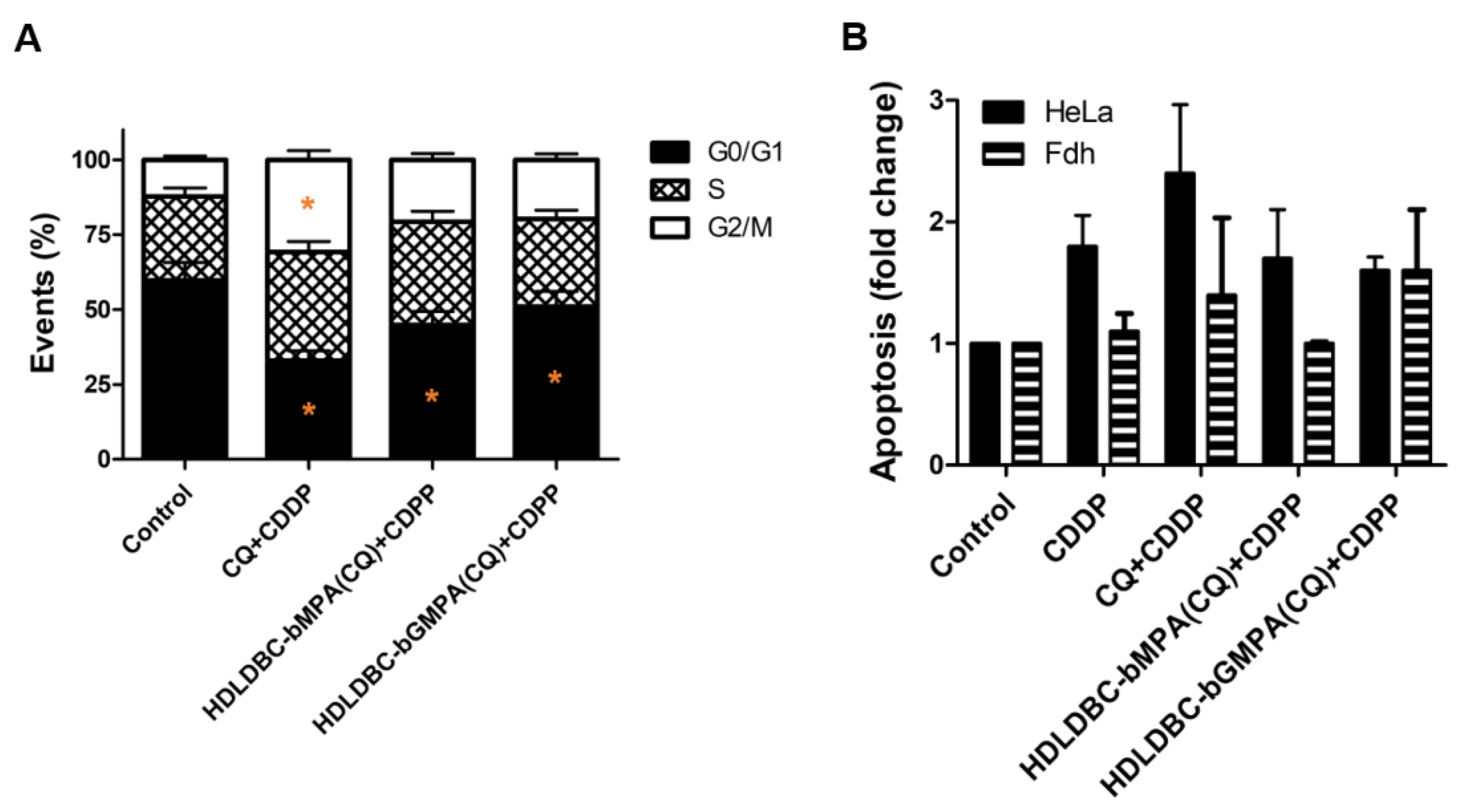
2.8. Cell Cycle Changes and Induction of Apoptosis after Combination Treatment with Encapsulated CQ and Free CDDP
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. Characterization of the Hybrid Dendritic–Linear–Dendritic Block Copolymers (HDLDBCs)
4.3. Preparation of Encapsulation of CQ, CDDP and Rhodamine and Drug Release Assays
4.4. Cell Lines and Cell Culture
4.5. Encapsulations Internalization
4.6. Cell Viability Determination Based on Proliferation Assay and Flow Cytometry
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jia, J.; Zhu, F.; Ma, X.; Cao, Z.W.; Li, Y.X.; Chen, Y.Z. Mechanisms of drug combinations: Interaction and network perspectives. Nat. Rev. Drug Discov. 2009, 8, 111–128. [Google Scholar] [CrossRef]
- Hu, Q.; Sun, W.; Wang, C.; Gu, Z. Recent advances of cocktail chemotherapy by combination drug delivery systems. Adv. Drug Deliv. Rev. 2016, 98, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Szakács, G.; Paterson, J.K.; Ludwig, J.A.; Booth-Genthe, C.; Gottesman, M.M. Targeting multidrug resistance in cancer. Nat. Rev. Drug Discov. 2006, 5, 219–234. [Google Scholar] [CrossRef]
- Al-Lazikani, B.; Banerji, U.; Workman, P. Combinatorial drug therapy for cancer in the post-genomic era. Nat. Biotechnol. 2012, 30, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Bozic, I.; Reiter, J.G.; Allen, B.; Antal, T.; Chatterjee, K.; Shah, P.; Nowak, M.A. Evolutionary dynamics of cancer in response to targeted combination therapy. elife 2013, 2, e00747. [Google Scholar] [CrossRef] [PubMed]
- Dear, R.F.; McGeechan, K.; Jenkins, M.C.; Barratt, A.; Tattersall, M.H.; Wilcken, N. Combination versus sequential single agent chemotherapy for metastatic breast cancer. Cochrane Database Syst. Rev. 2013, 12, CD008792. [Google Scholar] [CrossRef] [PubMed]
- Mayer, L.D.; Janoff, A.S. Optimizing Combination Chemotherapy by Controlling Drug Ratios. Mol. Interv. 2007, 7, 216–223. [Google Scholar] [CrossRef]
- Greco, F.; Vicent, M.J. Combination therapy: Opportunities and challenges for polymer–drug conjugates as anticancer nanomedicines. Adv. Drug Deliv. Rev. 2009, 61, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Honecker, F.; Kollmannsberger, C.; Quietzsch, D.; Haag, C.; Schroeder, M.; Spott, C.; Hartmann, J.T.; Baronius, W.; Hempel, V.; Kanz, L.; et al. Phase II study of weekly paclitaxel plus 24-h continuous infusion 5-fluorouracil, folinic acid and 3-weekly cisplatin for the treatment of patients with advanced gastric cancer. Anti-Cancer Drugs 2002, 13, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Ozols, R.F.; Bundy, B.N.; Greer, B.E.; Fowler, J.M.; Clarke-Pearson, D.; Burger, R.A.; Mannel, R.S.; DeGeest, K.; Hartenbach, E.M.; Baergen, R. Phase III Trial of Carboplatin and Paclitaxel Compared With Cisplatin and Paclitaxel in Patients With Optimally Resected Stage III Ovarian Cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2003, 21, 3194–3200. [Google Scholar] [CrossRef]
- Koopman, M.; Antonini, N.F.; Douma, J.; Wals, J.; Honkoop, A.H.; Erdkamp, F.L.; de Jong, R.S.; Rodenburg, C.J.; Vreugdenhil, G.; Loosveld, O.J. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced col-orectal cancer (CAIRO): A phase III randomised controlled trial. Lancet 2007, 370, 135–142. [Google Scholar] [CrossRef]
- Socinski, M.A.; Bondarenko, I.; Karaseva, N.A.; Makhson, A.M.; Vynnychenko, I.; Okamoto, I.; Hon, J.K.; Hirsh, V.; Bhar, P.; Zhang, H.; et al. Weekly nab-Paclitaxel in Combination With Carboplatin Versus Solvent-Based Paclitaxel Plus Carboplatin as First-Line Therapy in Patients With Advanced Non–Small-Cell Lung Cancer: Final Results of a Phase III Trial. J. Clin. Oncol. 2012, 30, 2055–2062. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Wang, B.; Sun, S.; Tang, L.; Zhang, J.; Lv, F.; Wang, Z.; Wang, L.; Zhang, Q.; Zheng, C.; et al. Cisplatin improves antitumor activity of weekly nab-paclitaxel in patients with metastatic breast cancer. Int. J. Nanomed. 2014, 9, 1443–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prestayko, A.; D’Aoust, J.; Issell, B.; Crooke, S. Cisplatin (cis-diamminedichloroplatinum II). Cancer Treat. Rev. 1979, 6, 17–39. [Google Scholar] [CrossRef]
- O’Brien, M.E.; Gaafar, R.M.; Popat, S.; Grossi, F.; Price, A.; Talbot, D.C.; Cufer, T.; Ottensmeier, C.; Danson, S.; Pallis, A. Phase II study of first-line bortezomib and cisplatin in malignant pleural mesothelioma and prospective validation of progression free survival rate as a primary end-point for mesothelioma clinical trials (European Organisation for Research and Treatment of Cancer 08052). Eur. J. Cancer 2013, 49, 2815–2822. [Google Scholar] [PubMed]
- Xu, Y.; Wang, N.; Ding, Y.; Wang, C.; Yü, Y.; Liu, S.; Wang, X.; Li, Z. Ammonium chloride enhances cisplatin cytotoxicity through DNA double-strand breaks in human cervical cancer cells. Oncol. Rep. 2013, 30, 1195–1200. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.-Q.; Fang, N.; Liu, X.-M.; Xiong, S.-P.; Liao, Y.-Q.; Jin, W.-J.; Song, R.-F.; Wan, Y.-Y. Antitumor Activity of Chloroquine in Combination with Cisplatin in Human Gastric Cancer Xenografts. Asian Pac. J. Cancer Prev. 2015, 16, 3907–3912. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.-G.; Sun, R.-J.; Yang, X.-Y.; Liu, D.-Y.; Lei, D.-P.; Jin, T.; Pan, X.-L. Chloroquine-enhanced efficacy of cisplatin in the treat-ment of hypopharyngeal carcinoma in xenograft mice. PLoS ONE 2015, 10, e0126147. [Google Scholar]
- Shen, Z.; Qin, L.; Xu, T.; Xia, L.; Wang, X.; Zhang, X.; Zhang, X.; Zhu, Z.; Zhong, S.; Wang, C. Chloroquine enhances the efficacy of cisplatin by suppressing autophagy in human adrenocortical carcinoma treatment. Drug Des. Dev. Ther. 2016, 10, 1035–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, J.; Zheng, Y.; Zhang, H.; Zhu, J.; Sun, H. Low concentration of chloroquine enhanced efficacy of cisplatin in the treatment of human ovarian cancer dependent on autophagy. Am. J. Transl. Res. 2017, 9, 4046–4058. [Google Scholar]
- Fan, C.; Wang, W.; Zhao, B.; Zhang, S.; Miao, J. Chloroquine inhibits cell growth and induces cell death in A549 lung cancer cells. Bioorg. Med. Chem. 2006, 14, 3218–3222. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Zhao, Y.-L.; Deng, X.; Yang, S.; Mao, Y.; Li, Z.; Jiang, P.; Zhao, X.; Wei, Y. Chloroquine inhibits colon cancer cell growth in vitro and tumor growth in vivo via induction of apoptosis. Cancer Investig. 2009, 27, 286–292. [Google Scholar] [CrossRef]
- Sasaki, K.; Tsuno, N.H.; Sunami, E.; Tsurita, G.; Kawai, K.; Okaji, Y.; Nishikawa, T.; Shuno, Y.; Hongo, K.; Hiyoshi, M. Chloro-quine potentiates the anti-cancer effect of 5-fluorouracil on colon cancer cells. BMC Cancer 2010, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, L.; Wang, J.; Wu, T.; Wu, J.; Ling, J.; Cheng, B. In Vitro and in vivo antitumor effects of chloroquine on oral squamous cell carcinoma. Mol. Med. Rep. 2017, 16, 5779–5786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, H.; Kuchnio, A.; Peric, A.; Moens, S.; Nys, K.; De Bock, K.; Quaegebeur, A.; Schoors, S.; Georgiadou, M.; Wouters, J.; et al. Tumor Vessel Normalization by Chloroquine Independent of Autophagy. Cancer Cell 2014, 26, 190–206. [Google Scholar] [CrossRef] [Green Version]
- Palmer, A.; Sorger, P.K. Combination Cancer Therapy Can Confer Benefit via Patient-to-Patient Variability without Drug Additivity or Synergy. Cell 2017, 171, 1678–1691. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, N.; Wu, J.; Xu, X.; Kamaly, N.; Farokhzad, O.C. Cancer nanotechnology: The impact of passive and active targeting in the era of modern cancer biology. Adv. Drug Deliv. Rev. 2014, 66, 2–25. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.-M.J.; Zhang, L. Nanoparticle-based combination therapy toward overcoming drug resistance in cancer. Biochem. Pharmacol. 2012, 83, 1104–1111. [Google Scholar] [CrossRef]
- Xu, X.; Ho, W.; Zhang, X.; Bertrand, N.; Farokhzad, O. Cancer nanomedicine: From targeted delivery to combination therapy. Trends Mol. Med. 2015, 21, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.-J.; Chen, C.; Zhao, Y.; Wang, P.C. Circumventing Tumor Resistance to Chemotherapy by Nanotechnology. Methods Mol. Biol. 2009, 596, 467–488. [Google Scholar] [CrossRef] [Green Version]
- Senapati, S.; Mahanta, A.K.; Kumar, S.; Maiti, P. Controlled drug delivery vehicles for cancer treatment and their performance. Signal Transduct. Target. Ther. 2018, 3, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyer, A.K.; Singh, A.; Ganta, S.; Amiji, M.M. Role of integrated cancer nanomedicine in overcoming drug resistance. Adv. Drug Deliv. Rev. 2013, 65, 1784–1802. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Shen, J.; Wang, J.; Yang, X.; Dong, S.; Lu, S. Nanoparticle-Based Drug Delivery System: A Patient-Friendly Chemotherapy for Oncology. Dose-Response 2020, 18, 1559325820936161. [Google Scholar] [CrossRef]
- Lu, Y.; Aimetti, A.A.; Langer, R.; Gu, Z. Bioresponsive materials. Nat. Rev. Mater. 2017, 2, 16075. [Google Scholar] [CrossRef]
- Petschauer, J.S.; Madden, A.J.; Kirschbrown, W.P.; Song, G.; Zamboni, W.C. The effects of nanoparticle drug loading on the pharmacokinetics of anticancer agents. Nanomedicine 2015, 10, 447–463. [Google Scholar] [CrossRef] [Green Version]
- Xiao, W.; Zeng, X.; Lin, H.; Han, K.; Jia, H.-Z.; Zhang, X.-Z. Dual stimuli-responsive multi-drug delivery system for the indi-vidually controlled release of anti-cancer drugs. Chem. Commun. 2015, 51, 1475–1478. [Google Scholar] [CrossRef]
- Meng, J.; Guo, F.; Xu, H.; Liang, W.; Wang, C.; Yang, X.-D. Combination Therapy using Co-encapsulated Resveratrol and Paclitaxel in Liposomes for Drug Resistance Reversal in Breast Cancer Cells in vivo. Sci. Rep. 2016, 6, 22390. [Google Scholar] [CrossRef]
- Wu, Y.; Lv, S.; Li, Y.; He, H.; Ji, Y.; Zheng, M.; Liu, Y.; Yin, L. Co-delivery of dual chemo-drugs with precisely controlled, high drug loading polymeric micelles for synergistic anti-cancer therapy. Biomater. Sci. 2020, 8, 949–959. [Google Scholar] [CrossRef]
- Pacardo, D.B.; Ligler, F.S.; Gu, Z. Programmable nanomedicine: Synergistic and sequential drug delivery systems. Nanoscale 2015, 7, 3381–3391. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, H.; Chen, Y.; Ma, J.; Lin, J.; Zhang, Y.; Fan, Z.; Su, G.; Xie, L.; Zhu, X. Integration of phospholipid-hyaluronic ac-id-methotrexate nanocarrier assembly and amphiphilic drug–drug conjugate for synergistic targeted delivery and combinational tumor therapy. Biomater. Sci. 2018, 6, 1818–1833. [Google Scholar] [CrossRef]
- Akash, M.S.H.; Rehman, K. Recent progress in biomedical applications of Pluronic (PF127): Pharmaceutical perspectives. J. Control. Release 2015, 209, 120–138. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Bromberg, L.; Lin, S.; Hatton, T.A.; Tam, K.C. Complexation and release of doxorubicin from its complexes with plu-ronic P85-b-poly (acrylic acid) block copolymers. J. Control. Release 2007, 121, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Gitsov, I.; Wooley, K.L.; Fréchet, J.M. Novel polyether copolymers consisting of linear and dendritic blocks. Angew. Chem. Int. Ed. Engl. 1992, 31, 1200–1202. [Google Scholar] [CrossRef]
- Fan, X.; Zhao, Y.; Xu, W.; Li, L. Linear–dendritic block copolymer for drug and gene delivery. Mater. Sci. Eng. C 2016, 62, 943–959. [Google Scholar] [CrossRef] [PubMed]
- van/Hest, J.; Baars, M.; Elissen-Román, C.; van/Genderen, M.; Meijer, E. Acid-functionalized amphiphiles, derived from poly-styrene-poly (propylene imine) dendrimers, with a pH-dependent aggregation. Macromolecules 1995, 28, 6689–6691. [Google Scholar] [CrossRef] [Green Version]
- Newkome, G.R.; Moorefield, C.N.; Baker, G.R.; Behera, R.K.; Escamillia, G.H.; Saunders, M.J. Supramolecular Self-Assemblies of Two-Directional Cascade Molecules: Automorphogenesis. Angew. Chem. Int. Ed. 1992, 31, 917–919. [Google Scholar] [CrossRef]
- Movellan, J.; Urbán, P.; Moles, E.; Jesús, M.; Sierra, T.; Serrano, J.L.; Fernàndez-Busquets, X. Amphiphilic dendritic derivatives as nanocarriers for the targeted delivery of antimalarial drugs. Biomaterials 2014, 35, 7940–7950. [Google Scholar] [CrossRef]
- Coma-Cros, E.M.; Lancelot, A.; San Anselmo, M.; Borgheti-Cardoso, L.N.; Valle-Delgado, J.J.; Serrano, J.L.; Fernàn-dez-Busquets, X.; Sierra, T. Micelle carriers based on dendritic macromolecules containing bis-MPA and glycine for antimalarial drug delivery. Biomater. Sci. 2019, 7, 1661–1674. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Pardo, I.; González-Pastor, R.; Lancelot, A.; Claveria-Gimeno, R.; Velázquez-Campoy, A.; Abian, O.; Sierra, T. Shell Cross-Linked Polymeric Micelles as Camptothecin Nanocarriers for Anti-HCV Therapy. Macromol. Biosci. 2015, 15, 1381–1391. [Google Scholar] [CrossRef] [Green Version]
- Franken, L.E.; Boekema, E.J.; Stuart, M.C. Transmission electron microscopy as a tool for the characterization of soft materials: Application and interpretation. Adv. Sci. 2017, 4, 1600476. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, S. Cisplatin: The first metal based anticancer drug. Bioorganic Chem. 2019, 88, 102925. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-H.; Chang, J.-Y. New Insights into Mechanisms of Cisplatin Resistance: From Tumor Cell to Microenvironment. Int. J. Mol. Sci. 2019, 20, 4136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florea, A.-M.; Büsselberg, D. Cisplatin as an Anti-Tumor Drug: Cellular Mechanisms of Activity, Drug Resistance and Induced Side Effects. Cancers 2011, 3, 1351–1371. [Google Scholar] [CrossRef]
- Mizushima, N.; Komatsu, M. Autophagy: Renovation of Cells and Tissues. Cell 2011, 147, 728–741. [Google Scholar] [CrossRef] [Green Version]
- Cetintas, V.B.; Kucukaslan, A.S.; Kosova, B.; Tetik, A.; Selvi, N.; Cok, G.; Gunduz, C.; Eroglu, Z. Cisplatin resistance induced by decreased apoptotic activity in non-small-cell lung cancer cell lines. Cell Biol. Int. 2012, 36, 261–265. [Google Scholar] [CrossRef]
- Pennati, M.; Lopergolo, A.; Profumo, V.; De Cesare, M.; Sbarra, S.; Valdagni, R.; Zaffaroni, N.; Gandellini, P.; Folini, M. miR-205 impairs the autophagic flux and enhances cisplatin cytotoxicity in castration-resistant prostate cancer cells. Biochem. Pharmacol. 2014, 87, 579–597. [Google Scholar] [CrossRef]
- Yu, L.; Gu, C.; Zhong, D.; Shi, L.; Kong, Y.; Zhou, Z.; Liu, S. Induction of autophagy counteracts the anticancer effect of cisplatin in human esophageal cancer cells with acquired drug resistance. Cancer Lett. 2014, 355, 34–45. [Google Scholar] [CrossRef]
- Zhao, J.; Nie, Y.; Wang, H.; Lin, Y. miR-181a suppresses autophagy and sensitizes gastric cancer cells to cisplatin. Gene 2016, 576, 828–833. [Google Scholar] [CrossRef]
- Mezencev, R.; Matyunina, L.; Wagner, G.; McDonald, J. Acquired resistance of pancreatic cancer cells to cisplatin is multifac-torial with cell context-dependent involvement of resistance genes. Cancer Gene Ther. 2016, 23, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Mauthe, M.; Orhon, I.; Rocchi, C.; Zhou, X.; Luhr, M.; Hijlkema, K.-J.; Coppes, R.P.; Engedal, N.; Mari, M.; Reggiori, F. Chloro-quine inhibits autophagic flux by decreasing autophagosome-lysosome fusion. Autophagy 2018, 14, 1435–1455. [Google Scholar] [CrossRef] [PubMed]
- Gąsiorkiewicz, B.M.; Koczurkiewicz-Adamczyk, P.; Piska, K.; Pękala, E. Autophagy modulating agents as chemosensitizers for cisplatin therapy in cancer. Investig. New Drugs 2021, 39, 538–563. [Google Scholar] [CrossRef] [PubMed]
- Li, M.L.; Xu, Y.Z.; Lu, W.J.; Li, Y.H.; Tan, S.S.; Lin, H.J.; Wu, T.M.; Li, Y.; Wang, S.Y.; Zhao, Y.L. Chloroquine potentiates the anti-cancer effect of sunitinib on renal cell carcinoma by inhibiting autophagy and inducing apoptosis. Oncol. Lett. 2018, 15, 2839–2846. [Google Scholar]
- Fu, Z.; Chenghong, P.; Kuang, J.; Feng, H.; Chen, L.; Liang, J.; Shen, X.; Yuen, S.; Peng, C.; Shen, B.; et al. CQ sensitizes human pancreatic cancer cells to gemcitabine through the lysosomal apoptotic pathway via reactive oxygen species. Mol. Oncol. 2018, 12, 529–544. [Google Scholar] [CrossRef] [PubMed]
- White, E.; DiPaola, R.S. The Double-Edged Sword of Autophagy Modulation in Cancer. Clin. Cancer Res. 2009, 15, 5308–5316. [Google Scholar] [CrossRef] [Green Version]
- Stathopoulos, G.P.; Boulikas, T. Lipoplatin Formulation Review Article. J. Drug Deliv. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Parhizkar, M.; Reardon, P.J.; Knowles, J.C.; Browning, R.J.; Stride, E.; Barbara, P.R.; Harker, A.H.; Edirisinghe, M. Electrohydro-dynamic encapsulation of cisplatin in poly (lactic-co-glycolic acid) nanoparticles for controlled drug delivery, Nanomedi-cine: Nanotechnology. Biol. Med. 2016, 12, 1919–1929. [Google Scholar]
- Duan, X.; He, C.; Kron, S.J.; Lin, W. Nanoparticle formulations of cisplatin for cancer therapy. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2016, 8, 776–791. [Google Scholar] [CrossRef] [Green Version]
- Stevens, D.M.; Crist, R.M.; Stern, S.T. Nanomedicine Reformulation of Chloroquine and Hydroxychloroquine. Molecules 2020, 26, 175. [Google Scholar] [CrossRef]
- Cabral, H.; Miyata, K.; Osada, K.; Kataoka, K. Block Copolymer Micelles in Nanomedicine Applications. Chem. Rev. 2018, 118, 6844–6892. [Google Scholar] [CrossRef] [Green Version]
- Qiu, L.; Gao, M.; Xu, Y. Enhanced combination therapy effect on paclitaxel-resistant carcinoma by chloroquine co-delivery via liposomes. Int. J. Nanomed. 2015, 10, 6615–6632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panagiotaki, K.N.; Sideratou, Z.; Vlahopoulos, S.A.; Paravatou-Petsotas, M.; Zachariadis, M.; Khoury, N.; Zoumpourlis, V.; Tsiourvas, D. A Triphenylphosphonium-Functionalized Mitochondriotropic Nanocarrier for Efficient Co-Delivery of Doxorubicin and Chloroquine and Enhanced Antineoplastic Activity. Pharmaceuticals 2017, 10, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, M.; Zhu, W.; Lv, X.; Yang, Q.; Liu, X.; Xie, Y.; Tang, P.; Sun, L. Encapsulation of chloroquine and doxorubicin by MPEG-PLA to enhance anticancer effects by lysosomes inhibition in ovarian cancer. Int. J. Nanomed. 2018, 13, 8231–8245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, X.Y.; Tam, K.C.; Gan, L.H.; Tam, M.K. Hydrolytic Degradation of Pluronic F127/Poly(lactic acid) Block Copolymer Nanoparticles. Macromolecules 2004, 37, 3425–3430. [Google Scholar] [CrossRef]
- Xiong, X.; Tam, K.; Gan, L.; Tam, M.K. Effect of enzymatic degradation on the release kinetics of model drug from Pluronic F127/poly(lactic acid) nano-particles. J. Control. Release 2005, 108, 263–270. [Google Scholar] [CrossRef]
- Diniz, I.M.A.; Chen, C.; Xu, X.; Ansari, S.; Zadeh, H.H.; Marques, M.M.; Shi, S.; Moshaverinia, A. Pluronic F-127 hydrogel as a promising scaffold for encapsulation of dental-derived mesenchymal stem cells. J. Mater. Sci. Mater. Med. 2015, 26, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancelot, A.; González-Pastor, R.; Concellón, A.; Sierra, T.; Martín-Duque, P.; Serrano, J.L. DNA transfection to mesenchymal stem cells using a novel type of pseudodendrimer based on 2,2-bis (hydroxymethyl) propionic acid. Bioconjugate Chem. 2017, 28, 1135–1150. [Google Scholar] [CrossRef]
- Lancelot, A.; González-Pastor, R.; Clavería-Gimeno, R.; Romero, P.; Abian, O.; Martín-Duque, P.; Sierra, T. Cationic poly(ester amide) dendrimers: Alluring materials for biomedical applications. J. Mater. Chem. B 2018, 6, 3956–3968. [Google Scholar] [CrossRef]
- Nagai, N.; Kinoshita, M.; Ogata, H.; Tsujino, D.; Wada, Y.; Someya, K.; Ohno, T.; Masuhara, K.; Tanaka, Y.; Kato, K. Relationship between pharmacokinetics of unchanged cisplatin and nephrotoxicity after intravenous infusions of cisplatin to cancer pa-tients. Cancer Chemother. Pharmacol. 1996, 39, 131–137. [Google Scholar] [CrossRef]
- Ledezma-Gallegos, F.; Jurado, R.; Mir, R.; Medina, L.A.; Mondragon-Fuentes, L.; Garcia-Lopez, P. Liposomes Co-Encapsulating Cisplatin/Mifepristone Improve the Effect on Cervical Cancer: In Vitro and In Vivo Assessment. Pharmaceutics 2020, 12, 897. [Google Scholar] [CrossRef]
- Song, W.; Tang, Z.; Li, M.; Lv, S.; Sun, H.; Deng, M.; Liu, H.; Chen, X. Polypeptide-based combination of paclitaxel and cisplatin for enhanced chemotherapy efficacy and reduced side-effects. Acta Biomater. 2014, 10, 1392–1402. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Luo, L.; Xue, Y.; Han, J.; Liu, Y.; Zhang, Y.; Yin, T.; Wang, L.; Cun, D.; Gou, J. Cisplatin-loaded polymeric complex mi-celles with a modulated drug/copolymer ratio for improved in vivo performance. Acta Biomater. 2019, 92, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Alba, E.; Martín, M.; Ramos, M.; Adrover, E.; Balil, A.; Jara, C.; Barnadas, A.; Fernández-Aramburo, A.; Sánchez-Rovira, P.; Amenedo, M. Multicenter randomized trial comparing sequential with concomitant administration of doxorubicin and docet-axel as first-line treatment of metastatic breast cancer: A Spanish Breast Cancer Research Group (GEICAM-9903) phase III study. J. Clin. Oncol. 2004, 22, 2587–2593. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Malka, D.; Mendiboure, J.; Etienne, P.-L.; Texereau, P.; Auby, D.; Rougier, P.; Gasmi, M.; Castaing, M.; Abbas, M.; et al. Sequential versus combination chemotherapy for the treatment of advanced colorectal cancer (FFCD 2000–05): An open-label, randomised, phase 3 trial. Lancet Oncol. 2011, 12, 1032–1044. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, F.; Altucci, L.; Cobellis, G. Autophagy Function and Dysfunction: Potential Drugs as Anti-Cancer Therapy. Cancers 2019, 11, 1465. [Google Scholar] [CrossRef] [Green Version]
- Abraham, R.T. Cell cycle checkpoint signaling through the ATM and ATR kinases. Genes Dev. 2001, 15, 2177–2196. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Han, C.; Yu, H.; Zhu, W.; Cui, H.; Zheng, L.; Zhang, C.; Yue, L. Chloroquine inhibits cell growth in human A549 lung cancer cells by blocking autophagy and inducing mitochondrial-mediated apoptosis. Oncol. Rep. 2018, 39, 2807–2816. [Google Scholar] [CrossRef]
- Bromma, K.; Bannister, A.; Kowalewski, A.; Cicon, L.; Chithrani, D.B. Elucidating the fate of nanoparticles among key cell components of the tumor microenvironment for promoting cancer nanotechnology. Cancer Nanotechnol. 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Martinho, N.; Santos, T.C.; Florindo, H.F.; Silva, L.C. Cisplatin-membrane interactions and their influence on platinum com-plexes activity and toxicity. Front. Physiol. 2019, 9, 1898. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, N.; Kato, Y.; Sugiyama, Y.; Kataoka, K. Cisplatin-Loaded Polymer-Metal Complex Micelle with Time-Modulated Decaying Property as a Novel Drug Delivery System. Pharm. Res. 2001, 18, 1035–1041. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HDLDBC-bMPA | |||
| TEM | cryoTEM | DLS | |
| Intensity | Number | ||
| 13 ± 3 22 ± 4 | 60 and 150 | 28 ± 4 (7%) 223 ± 80 (90%) | 21 ± 6 (57%) 125 ± 54 (33%) |
| HDLDBC-bGMPA | |||
| TEM | cryoTEM | DLS | |
| Intensity | Number | ||
| 13 ± 3 | 40–70 | 225 ± 89 (96%) | 88 ± 49 (100%) |
| HDLDBC-bMPA | |||
| Drug | EE (%) 1 | mg drug/mg HDLDBC | Hydrodynamic Diameter (nm) |
| CQ | 49 ± 4% | 0.49 ± 0.04 | 45 ± 8 (12%) and 200 ± 49 (88%) |
| CDDP | 13 ± 11% | 0.043 ± 0.014 | 18 ± 3 nm (3%) and 276 ± 76 nm (91%) |
| HDLDBC-bGMPA | |||
| Drug | EE (%) 1 | mg drug/mg HDLDBC | Hydrodynamic Diameter (nm) |
| CQ | 67 ± 6% | 0.67 ± 0.06 | 48 ± 18 nm (14%) and 318 ± 22 nm (86%) |
| CDDP | 7% | 0.017 | 49 ± 6 nm (8%) and 371 ± 20 nm (92%) |
| Cell Line | Time | CQ (µM) | HDLDBC-bMPA(CQ) (µM) | HDLDBC-bGMPA(CQ) (µM) | CDDP (µg/mL) | HDLDBC-bMPA(CDDP) (µg/mL) |
|---|---|---|---|---|---|---|
| HeLa | 24 h | 88.5 | >100 | >100 | 3.7 | >5 |
| 48 h | 16.4 | 57.9 | 53.7 | 2.1 | 3.9 | |
| 72 h | 7.8 | 19.5 | 33.9 | 2.3 | 3.5 | |
| A549 | 24 h | 60.3 | >100 | >100 | >5 | >5 |
| 48 h | 44.7 | >100 | >100 | 3.3 | >5 | |
| 72 h | 41.0 | 70.0 | 100 | 2.6 | >5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Pastor, R.; Lancelot, A.; Morcuende-Ventura, V.; San Anselmo, M.; Sierra, T.; Serrano, J.L.; Martin-Duque, P. Combination Chemotherapy with Cisplatin and Chloroquine: Effect of Encapsulation in Micelles Formed by Self-Assembling Hybrid Dendritic–Linear–Dendritic Block Copolymers. Int. J. Mol. Sci. 2021, 22, 5223. https://doi.org/10.3390/ijms22105223
González-Pastor R, Lancelot A, Morcuende-Ventura V, San Anselmo M, Sierra T, Serrano JL, Martin-Duque P. Combination Chemotherapy with Cisplatin and Chloroquine: Effect of Encapsulation in Micelles Formed by Self-Assembling Hybrid Dendritic–Linear–Dendritic Block Copolymers. International Journal of Molecular Sciences. 2021; 22(10):5223. https://doi.org/10.3390/ijms22105223
Chicago/Turabian StyleGonzález-Pastor, Rebeca, Alexandre Lancelot, Violeta Morcuende-Ventura, María San Anselmo, Teresa Sierra, José L. Serrano, and Pilar Martin-Duque. 2021. "Combination Chemotherapy with Cisplatin and Chloroquine: Effect of Encapsulation in Micelles Formed by Self-Assembling Hybrid Dendritic–Linear–Dendritic Block Copolymers" International Journal of Molecular Sciences 22, no. 10: 5223. https://doi.org/10.3390/ijms22105223
APA StyleGonzález-Pastor, R., Lancelot, A., Morcuende-Ventura, V., San Anselmo, M., Sierra, T., Serrano, J. L., & Martin-Duque, P. (2021). Combination Chemotherapy with Cisplatin and Chloroquine: Effect of Encapsulation in Micelles Formed by Self-Assembling Hybrid Dendritic–Linear–Dendritic Block Copolymers. International Journal of Molecular Sciences, 22(10), 5223. https://doi.org/10.3390/ijms22105223