
Multiplex Autoantibody Detection in Patients with Autoimmune Polyglandular Syndromes

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Detection of Autoantibodies by the Microarray-Based Assay
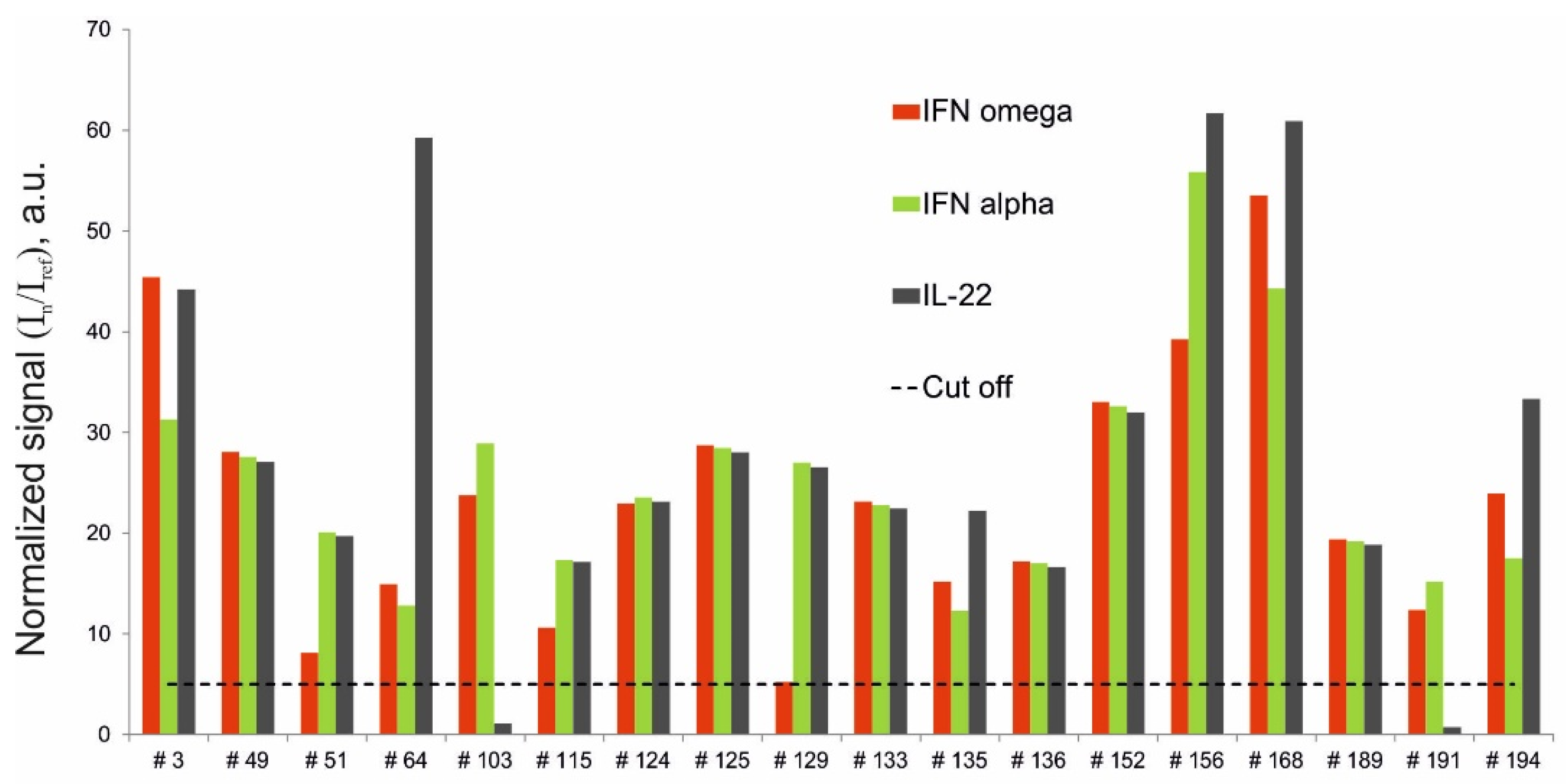
2.2. Detection of Autoantibodies Against IFN-ω, IFN-α-2a and IL-22
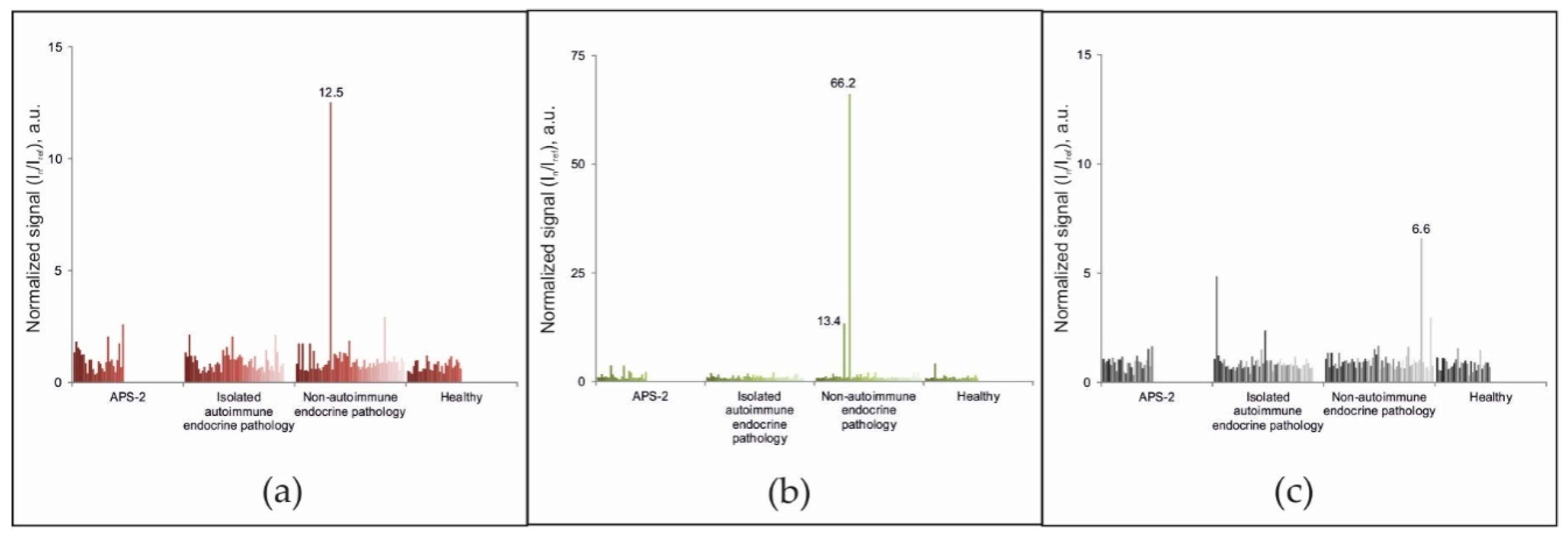
2.3. Detection of Organ-Specific Autoantibodies by Microarray-Based Assay and ELISA
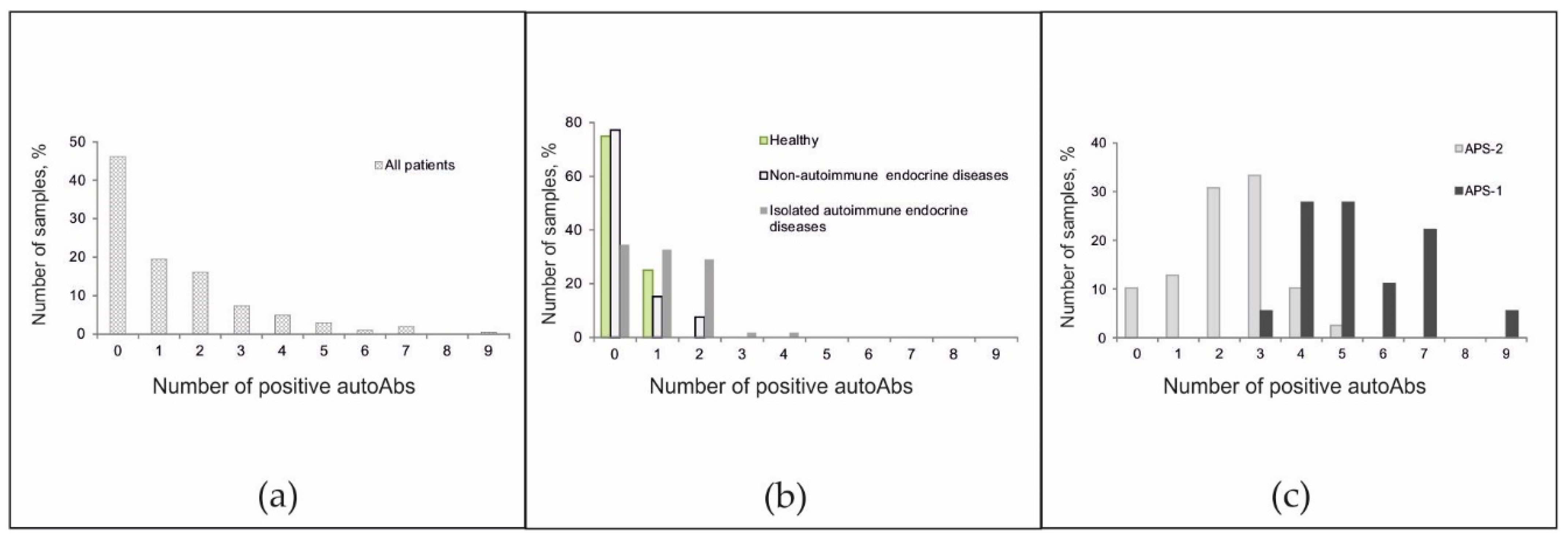
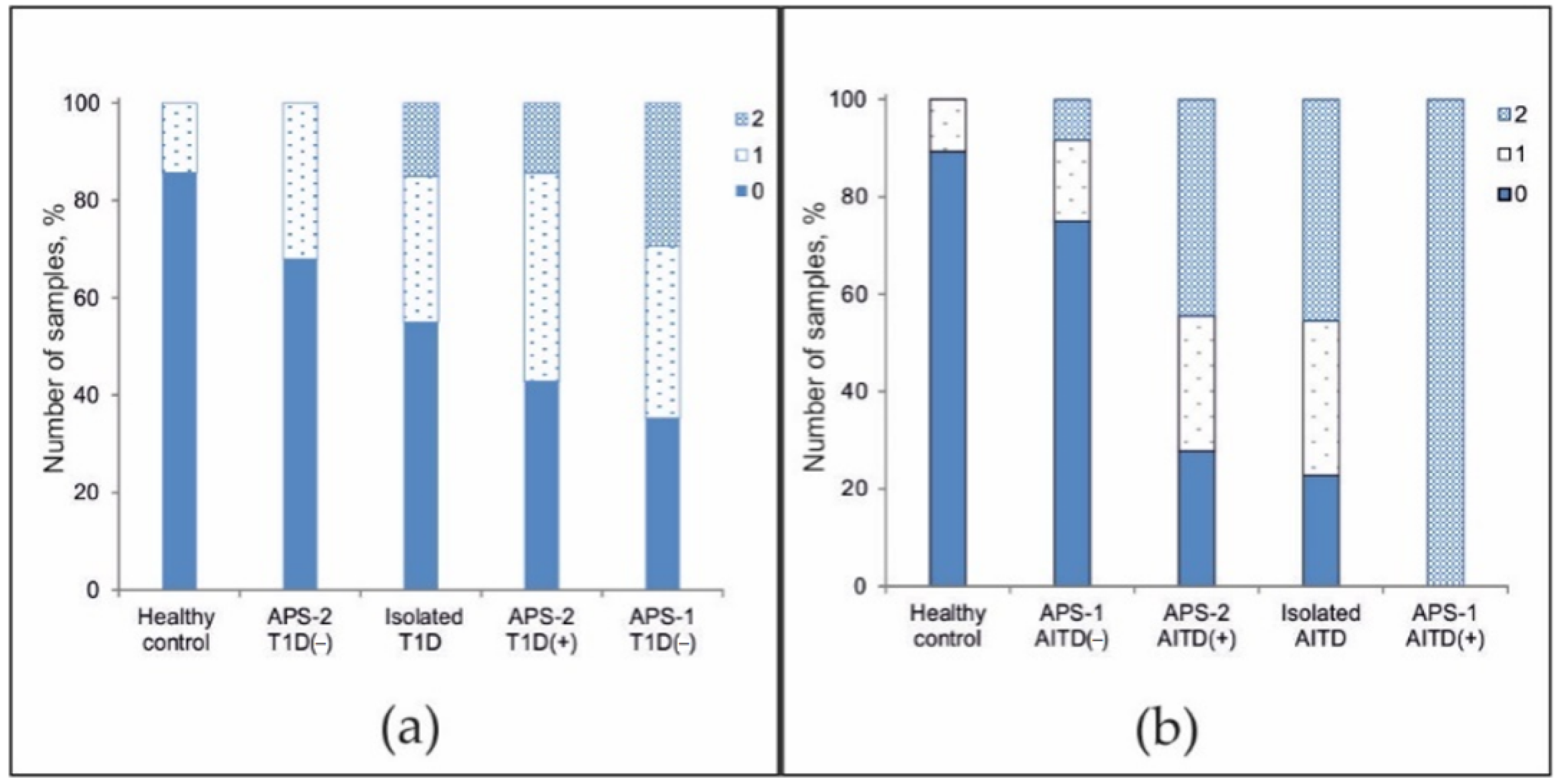
2.4. Frequencies of Positive Autoantibodies in Serum Samples
3. Discussion
4. Materials and Methods
4.1. Clinical Data and Serum Samples
- -
- -
- Hypergonadotropic hypogonadism of autoimmune genesis: the acquired form and combination with any autoimmune disease, antibody carrier and/or signs of autoimmune damage according to ultrasound of the thyroid gland were excluded;
- -
- Primary autoimmune adrenal insufficiency: the acquired form is excluded, antibodies to 21-OH are increased;
- -
- Autoimmune diabetes mellitus: the onset of the disease from a young age, within APS-2 and/or an increased level of antibodies to GAD, ZnT8, IA2, IAA and/or ICA;
- -
- Autoimmune thyroiditis: Elevated levels of antibodies to TPO, TG and/or TSHR; signs of autoimmune lesion on thyroid ultrasound and/or medical history (in the case of Graves’ disease);
- -
- Non-autoimmune hypergonadotropic hypogonadism: intact ovaries, testes; lack of concomitant autoimmune diseases;
- -
- Non-autoimmune adrenal insufficiency: intact adrenal glands, normal level of antibodies to 21-OH; lack of concomitant autoimmune diseases;
- -
- Non-autoimmune thyroid disease: normal level of antibodies to TPO, TG, and/or TSHR; no signs of autoimmune damage according to ultrasound of the thyroid gland; intact thyroid gland; lack of concomitant autoimmune diseases;
- -
- Non-autoimmune diabetes mellitus: normal levels of antibodies to GAD, ZnT8, IA2, IAA, and/or ICA; intact pancreas; lack of concomitant autoimmune diseases;
- -
- Non-autoimmune parathyroid disease: absence of concomitant autoimmune diseases and intact parathyroid gland;
- -
- Healthy persons: absence of endocrine (autoimmune and non-autoimmune) pathology (according to the survey).
4.2. ELISAs for Detection of Autoantibodies
4.3. Microarray Design and Manufacturing
4.4. Fluorescent Antibody Labeling
4.5. Microarray Hybridization and Washing
4.6. Analysis of Fluorescence and Interpretation of Results
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, G.; Jialal, I. Polyglandular Autoimmune Syndrome Type II. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Husebye, E.S.; Anderson, M.S.; Kämpe, O. Autoimmune Polyendocrine Syndromes. N. Engl. J. Med. 2018, 378, 1132–1141. [Google Scholar] [CrossRef]
- Perheentupa, J. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. J. Clin. Endocrinol. Metab. 2006, 91, 2843–2850. [Google Scholar] [CrossRef] [Green Version]
- Bruserud, Ø.; Oftedal, B.E.; Wolff, A.S.B.; Husebye, E.S. AIRE-mutations and autoimmune disease. Curr. Opin. Immunol. 2016, 43, 8–15. [Google Scholar] [CrossRef]
- Puel, A.; Döffinger, R.; Natividad, A.; Chrabieh, M.; Barcenas-Morales, G.; Picard, C.; Cobat, A.; Ouachée-Chardin, M.; Toulon, A.; Bustamante, J.; et al. Autoantibodies against IL-17A, IL-17F, and IL-22 in patients with chronic mucocutaneous candidiasis and autoimmune polyendocrine syndrome type I. J. Exp. Med. 2010, 207, 291–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisand, K.; Wolff, A.S.B.; Podkrajšek, K.T.; Tserel, L.; Link, M.; Kisand, K.V.; Ersvaer, E.; Perheentupa, J.; Erichsen, M.M.; Bratanic, N.; et al. Chronic mucocutaneous candidiasis in APECED or thymoma patients correlates with autoimmunity to Th17-associated cytokines. J. Exp. Med. 2010, 207, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Meager, A.; Visvalingam, K.; Peterson, P.; Möll, K.; Murumägi, A.; Krohn, K.; Eskelin, P.; Perheentupa, J.; Husebye, E.; Kadota, Y.; et al. Anti-interferon autoantibodies in autoimmune polyendocrinopathy syndrome type 1. PLoS Med. 2006, 3, 1152–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Barker, J.M.; Babu, S.; Su, M.; Stenerson, M.; Cheng, M.; Shum, A.; Zamir, E.; Badolato, R.; Law, A.; et al. A robust immunoassay for anti-interferon autoantibodies that is highly specific for patients with autoimmune polyglandular syndrome type 1. Clin. Immunol. 2007, 125, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larosa, M.D.P.; Mackenzie, R.; Burne, P.; Garelli, S.; Barollo, S.; Masiero, S.; Rubin, B.; Chen, S.; Furmaniak, J.; Betterle, C.; et al. Assessment of autoantibodies to interferon-ω in patients with autoimmune polyendocrine syndrome type 1: Using a new immunoprecipitation assay. Clin. Chem. Lab. Med. 2017, 55, 1003–1012. [Google Scholar] [CrossRef]
- Eriksson, D.; Dalin, F.; Eriksson, G.N.; Landegren, N.; Bianchi, M.; Hallgren, Å.; Dahlqvist, P.; Wahlberg, J.; Ekwall, O.; Winqvist, O.; et al. Cytokine autoantibody screening in the Swedish Addison Registry identifies patients with undiagnosed APS1. J. Clin. Endocrinol. Metab. 2018, 103, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.S.B.; Erichsen, M.M.; Meager, A.; Magitta, N.F.; Myhre, A.G.; Bollerslev, J.; Fougner, K.J.; Lima, K.; Knappskog, P.M.; Husebye, E.S. Autoimmune polyendocrine syndrome type 1 in Norway: Phenotypic variation, autoantibodies, and novel mutations in the autoimmune regulator gene. J. Clin. Endocrinol. Metab. 2007, 92, 595–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meloni, A.; Furcas, M.; Cetani, F.; Marcocci, C.; Falorni, A.; Perniola, R.; Pura, M.; Wolff, A.S.B.; Husebye, E.S.; Lilic, D.; et al. Autoantibodies against type I interferons as an additional diagnostic criterion for autoimmune polyendocrine syndrome type I. J. Clin. Endocrinol. Metab. 2008, 93, 4389–4397. [Google Scholar] [CrossRef] [Green Version]
- Magitta, N.F.; Pura, M.; Wolff, A.S.B.; Vanuga, P.; Meager, A.; Knappskog, P.M.; Husebye, E.S. Autoimmune polyendocrine syndrome type I in Slovakia: Relevance of screening patients with autoimmune Addison’s disease. Eur. J. Endocrinol. 2008, 158, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Orlova, E.M.; Sozaeva, L.S.; Kareva, M.A.; Oftedal, B.E.; Wolff, A.S.B.; Breivik, L.; Zakharova, E.Y.; Ivanova, O.N.; Kämpe, O.; Dedov, I.I.; et al. Expanding the phenotypic and genotypic landscape of autoimmune polyendocrine syndrome type 1. J. Clin. Endocrinol. Metab. 2017, 102, 3546–3556. [Google Scholar] [CrossRef]
- Rosenberg, J.M.; Price, J.V.; Barcenas-Morales, G.; Ceron-Gutierrez, L.; Davies, S.; Kumararatne, D.S.; Döffinger, R.; Utz, P.J. Protein microarrays identify disease-specific anti-cytokine autoantibody profiles in the landscape of immunodeficiency. J. Allergy Clin. Immunol. 2016, 137, 204–213.e3. [Google Scholar] [CrossRef] [Green Version]
- Vazquez, S.E.; Ferré, E.M.N.; Scheel, D.W.; Sunshine, S.; Miao, B.; Mandel-Brehm, C.; Quandt, Z.; Chan, A.Y.; Cheng, M.; German, M.; et al. Identification of novel, clinically correlated autoantigens in the monogenic autoimmune syndrome APS1 by proteome-wide phip-seq. eLife 2020, 9, 1–25. [Google Scholar] [CrossRef]
- Zhan, F.; Cao, L. Late-onset autoimmune polyendocrine syndrome type 1: A case report and literature review. Immunol. Res. 2021, 69, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Karamifar, H.; Dalili, S.; Karamizadeh, Z.; Amirhakimi, G.; Hosein, D. Autoimmune polyglandular syndrome type 2: An unusual presentation. Acta Med. Iran. 2010, 48, 196–197. [Google Scholar] [PubMed]
- Abruzzo, A.; Giovale, M.C.; Damiano, G.; Palumbo, V.D.; Buscemi, S.; Monte, G.L.; Gulotta, L.; Buscemi, G.; Monte, A.I.L. Reoperation for persistent or recurrent secondary hyperparathyroidism. Surgical treatment of renal hyperparathyroidism. Acta BioMed. 2017, 88, 271–275. [Google Scholar] [CrossRef]
- Oftedal, B.E.; Hellesen, A.; Erichsen, M.M.; Bratland, E.; Vardi, A.; Perheentupa, J.; Kemp, E.H.; Fiskerstrand, T.; Viken, M.K.; Weetman, A.P.; et al. Dominant Mutations in the Autoimmune Regulator AIRE Are Associated with Common Organ-Specific Autoimmune Diseases. Immunity 2015, 42, 1185–1196. [Google Scholar] [CrossRef] [Green Version]
- Söderbergh, A.; Myhre, A.G.; Ekwall, O.; Gebre-Medhin, G.; Hedstrand, H.; Landgren, E.; Miettinen, A.; Eskelin, P.; Halonen, M.; Tuomi, T.; et al. Prevalence and Clinical Associations of 10 Defined Autoantibodies in Autoimmune Polyendocrine Syndrome Type I. J. Clin. Endocrinol. Metab. 2004, 89, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landegren, N.; Sharon, D.; Freyhult, E.; Hallgren, Å.; Eriksson, D.; Edqvist, P.H.; Bensing, S.; Wahlberg, J.; Nelson, L.M.; Gustafsson, J.; et al. Proteome-wide survey of the autoimmune target repertoire in autoimmune polyendocrine syndrome type 1. Sci. Rep. 2016, 6, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham-Dobor, G.; Hanák, L.; Hegyi, P.; Márta, K.; Párniczky, A.; Gergics, M.; Sarlós, P.; Erőss, B.; Mezősi, E. Prevalence of other autoimmune diseases in polyglandular autoimmune syndromes type II and III. J. Endocrinol. Invest. 2020, 43, 1327–1335. [Google Scholar] [CrossRef] [Green Version]
- Soh, S.-B.; Aw, T.-C. Laboratory Testing in Thyroid Conditions—Pitfalls and Clinical Utility. Ann. Lab. Med. 2019, 39, 3. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.P. Type 1 diabetes and polyglandular autoimmune syndrome: A review. World J. Diabetes 2015, 6, 67. [Google Scholar] [CrossRef] [PubMed]
- Betterle, C.; Morlin, L. Autoimmune Addison’s Disease. In Pediatric Adrenal Diseases; Karger: Basel, Switzerland, 2011; Volume 20, pp. 161–172. [Google Scholar]
- Devendra, D.; Yu, L.; Eisenbarth, G.S. Endocrine autoantibodies. Clin. Lab. Med. 2004, 24, 275–303. [Google Scholar] [CrossRef]
- Falorni, A.; Laureti, S.; Santeusanio, F. Autoantibodies in autoimmune polyendocrine syndrome type II. Endocrinol. Metab. Clin. 2002, 31, 369–389. [Google Scholar] [CrossRef]
- Meager, A.; Wadhwa, M.; Dilger, P.; Bird, C.; Thorpe, R.; Newsom-Davis, J.; Willcox, N. Anti-cytokine autoantibodies in autoimmunity: Preponderance of neutralizing autoantibodies against interferon-alpha, interferon-omega and interleukin-12 in patients with thymoma and/or myasthenia gravis. Clin. Exp. Immunol. 2003, 132, 128–136. [Google Scholar] [CrossRef]
- Gupta, S.; Tatouli, I.P.; Rosen, L.B.; Hasni, S.; Alevizos, I.; Manna, Z.G.; Rivera, J.; Jiang, C.; Siegel, R.M.; Holland, S.M.; et al. Distinct Functions of Autoantibodies Against Interferon in Systemic Lupus Erythematosus: A Comprehensive Analysis of Anticytokine Autoantibodies in Common Rheumatic Diseases. Arthritis Rheumatol. 2016, 68, 1677–1687. [Google Scholar] [CrossRef] [Green Version]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370. [Google Scholar] [CrossRef]
- Kemp, E.H.; Kahaly, G.J.; Porter, J.A.; Frommer, L.; Weetman, A.P. Autoantibodies against the calcium-sensing receptor and cytokines in autoimmune polyglandular syndromes types 2, 3 and 4. Clin. Endocrinol. 2018, 88, 139–145. [Google Scholar] [CrossRef]
- Antonelli, G.; Currenti, M.; Turriziani, O.; Dianzani, F. Neutralizing antibodies to interferon-α: Relative frequency in patients treated with different interferon preparations. J. Infect. Dis. 1991, 163, 882–885. [Google Scholar] [CrossRef]
- Antonelli, G.; Simeoni, E.; Currenti, M.; De Pisa, F.; Colizzi, V.; Pistello, M.; Dianzani, F. Interferon antibodies in patients with infectious diseases. Biotherapy 1997, 10, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.S.B.; Sarkadi, A.K.; Maródi, L.; Kärner, J.; Orlova, E.; Oftedal, B.E.V.; Kisand, K.; Oláh, É.; Meloni, A.; Myhre, A.G.; et al. Anti-cytokine autoantibodies preceding onset of autoimmune polyendocrine syndrome type i features in early childhood. J. Clin. Immunol. 2013, 33, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.J.; Leung, P.S.C.; Zhang, W.; Ma, X.; Gershwin, M.E. The immunobiology and clinical features of type 1 autoimmune polyglandular syndrome (APS-1). Autoimmun. Rev. 2018, 17, 78–85. [Google Scholar] [CrossRef]
- Bjork, E.; Velloso, L.A.; Kampe, O.; Karlsson, F.A. GAD autoantibodies in IDDM, stiff-man syndrome, and autoimmune polyendocrine syndrome type I recognize different epitopes. Diabetes 1994, 43, 161–165. [Google Scholar] [CrossRef]
- Wilmot-Roussel, H.; Lévy, D.J.; Carette, C.; Caillat-Zucman, S.; Boitard, C.; Timsit, J.; Dubois-Laforgue, D. Factors associated with the presence of glutamic acid decarboxylase and islet antigen-2 autoantibodies in patients with long-standing type 1 diabetes. Diabetes Metab. 2013, 39, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Prummel, M.F.; Wiersinga, W.M. Thyroid peroxidase autoantibodies in euthyroid subjects. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 1–15. [Google Scholar] [CrossRef]
- Wiberg, A.; Granstam, A.; Ingvast, S.; Härkönen, T.; Knip, M.; Korsgren, O.; Skog, O. Characterization of human organ donors testing positive for type 1 diabetes-associated autoantibodies. Clin. Exp. Immunol. 2015, 182, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Yukina, M.; Erofeeva, T.; Nuralieva, N.; Andreeva, T.; Savvateeva, E.; Dudko, N.; Troshina, E.; Rogaev, E.; Melnichenko, G. Novel gene mutations regulating immune responses in autoimmune polyglandular syndrome with an atypical course. J. Endocr. Soc. 2021, 1–14. [Google Scholar] [CrossRef]
- Gryadunov, D.A.; Shaskolskiy, B.L.; Nasedkina, T.V.; Rubina, A.Y.; Zasedatelev, A.S. The EIMB Hydrogel Microarray Technology: Thirty Years Later. Acta Nat. 2018, 10, 4–18. [Google Scholar] [CrossRef]
- Rubina, A.Y.; Filippova, M.A.; Feizkhanova, G.U.; Shepeliakovskaya, A.O.; Sidina, E.I.; Boziev, K.M.; Laman, A.G.; Brovko, F.A.; Vertiev, Y.V.; Zasedatelev, A.S.; et al. Simultaneous detection of seven staphylococcal enterotoxins: Development of hydrogel biochips for analytical and practical application. Anal. Chem. 2010, 82, 8881–8889. [Google Scholar] [CrossRef] [PubMed]
- Lysov, Y.; Barsky, V.; Urasov, D.; Urasov, R.; Cherepanov, A.; Mamaev, D.; Yegorov, Y.; Chudinov, A.; Surzhikov, S.; Rubina, A.; et al. Microarray analyzer based on wide field fluorescent microscopy with laser illumination and a device for speckle suppression. Biomed. Opt. Express 2017, 8, 4798. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Age | Sex | CMC | CHP | AD | Comorbidity | AIRE Mutations |
|---|---|---|---|---|---|---|---|
| 3 | 49 | m | + | + | + | - | R257X/R257X |
| 49 | 20 | f | + | + | + | HH, AIT, VIT, DA, malabsorption syndrome, enamel hypoplasia | R257X/not found |
| 51 | 18 | f | + | + | + | HH | R257X/R257X |
| 64 | 29 | f | + | + | + | HH, atrophic gastritis, cataract | p.R257*/p.W78R |
| 103 | 18 | f | + | + | + | HH | R257X/R257X |
| 115 | 30 | f | + | + | + | AIT, T1D, DA, atrophic gastritis | R257X/R257X |
| 124 | 18 | m | + | - | + | Megaloblastic anemia, malabsorption syndrome, enamel hypoplasia, splenic hypoplasia | R257X/A58 V |
| 125 | 45 | f | + | + | + | HH, AIT, VIT, atrophic gastroduodenitis, cataract, corneal dystrophy | No genetic study was performed |
| 129 | 45 | m | + | + | + | AA | No genetic study was performed |
| 133 | 27 | m | + | - | + | AIT, DA, autoimmune fibrosing alveolitis | No genetic study was performed |
| 135 | 30 | f | + | + | + | HH, VIT, malabsorption syndrome, corneal dystrophy, ptosis, asplenia, atrophic gastroduodenitis, autoimmune hepatitis | R257X/R257X |
| 136 | 28 | f | + | + | + | HH, corneal dystrophy, atrophic gastritis | R257X/c.931delT |
| 152 | 27 | f | + | + | + | HH, AA, DA, enamel hypoplasia, tubulointerstitial nephritis | R257X/not found |
| 156 | 36 | m | + | + | + | - | No genetic study was performed |
| 168 | 32 | f | + | + | + | HH, AIT, DA, VIT | R257X/R257X |
| 189 | 31 | f | + | + | + | HH, atrophic gastroduodenitis malabsorption syndrome, enamel hypoplasia, retinitis pigmentosa, cataract, heterotropia | R257X/R257X |
| 191 | 44 | f | + | + | + | HH | R257X/R257X |
| 194 | 25 | f | + | + | + | HH, AIT, atrophic gastritis | R257X/c.821delG |
| AuAbs to: | ELISA Positive/Microarray Positive | ELISA Negative/Microarray Negative | ELISA Negative/Microarray Positive | ELISA Positive/Microarray Negative | Accuracy, % | Precision | Recall |
|---|---|---|---|---|---|---|---|
| 21-OH | 154 | 30 | 9 | 13 | 89.3 | 0.94 | 0.92 |
| GAD-65 | 184 | 16 | 2 | 4 | 97.1 | 0.99 | 0.98 |
| IA2 | 184 | 17 | 0 | 5 | 97.6 | 1.00 | 0.97 |
| ICA | 178 | 18 | 8 | 2 | 95.1 | 0.96 | 0.99 |
| TG | 160 | 35 | 8 | 3 | 94.7 | 0.95 | 0.98 |
| TPO | 126 | 57 | 14 | 9 | 88.8 | 0.90 | 0.93 |
| Total | 986 | 173 | 41 | 36 | 93.8 | 0.96 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savvateeva, E.N.; Yukina, M.Y.; Nuralieva, N.F.; Filippova, M.A.; Gryadunov, D.A.; Troshina, E.A. Multiplex Autoantibody Detection in Patients with Autoimmune Polyglandular Syndromes. Int. J. Mol. Sci. 2021, 22, 5502. https://doi.org/10.3390/ijms22115502
Savvateeva EN, Yukina MY, Nuralieva NF, Filippova MA, Gryadunov DA, Troshina EA. Multiplex Autoantibody Detection in Patients with Autoimmune Polyglandular Syndromes. International Journal of Molecular Sciences. 2021; 22(11):5502. https://doi.org/10.3390/ijms22115502
Chicago/Turabian StyleSavvateeva, Elena N., Marina Yu. Yukina, Nurana F. Nuralieva, Marina A. Filippova, Dmitry A. Gryadunov, and Ekaterina A. Troshina. 2021. "Multiplex Autoantibody Detection in Patients with Autoimmune Polyglandular Syndromes" International Journal of Molecular Sciences 22, no. 11: 5502. https://doi.org/10.3390/ijms22115502
APA StyleSavvateeva, E. N., Yukina, M. Y., Nuralieva, N. F., Filippova, M. A., Gryadunov, D. A., & Troshina, E. A. (2021). Multiplex Autoantibody Detection in Patients with Autoimmune Polyglandular Syndromes. International Journal of Molecular Sciences, 22(11), 5502. https://doi.org/10.3390/ijms22115502