
Radiotherapy of High-Grade Gliomas: First Half of 2021 Update with Special Reference to Radiosensitization Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Diagnosis and Prognosis
3. Advances in RT
3.1. Radioresistance
3.1.1. Preclinical Studies
3.1.2. Clinical Studies
3.2. Radiosensitization
3.2.1. Preclinical Studies
3.2.2. Clinical Studies
4. The Other Side of the Coin
5. Concluding Remarks and Future Perspectives
Funding
Conflicts of Interest
Abbreviations
References
- McCutcheon, I.E.; Preul, M.C. Historical Perspective on Surgery and Survival with Glioblastoma: How Far have we Come? World Neurosurg. 2021, 149, 148–168. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.; DeAngelis, L.M. Glioblastoma and Other Malignant Gliomas: A Clinical Review. JAMA 2013, 310, 1842–1850. [Google Scholar] [CrossRef]
- Khan, I.; Mahfooz, S.; Elbasan, E.B.; Karacam, B.; Oztanir, M.N.; Hatiboglu, M.A. Targeting Glioblastoma: The Current State of Different Therapeutic Approaches. Curr. Neuropharmacol. 2021, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy Plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Oronsky, B.; Reid, T.R.; Oronsky, A.; Sandhu, N.; Knox, S.J. A Review of Newly Diagnosed Glioblastoma. Front. Oncol. 2021, 10, 574012. [Google Scholar] [CrossRef]
- Gzell, C.; Back, M.; Wheeler, H.; Bailey, D.; Foote, M. Radiotherapy in Glioblastoma: The Past, the Present and the Future. Clin. Oncol. (R. Coll. Radiol) 2017, 29, 15–25. [Google Scholar] [CrossRef]
- Hau, E.; Shen, H.; Clark, C.; Graham, P.H.; Koh, E.-S.; McDonald, K.L. The Evolving Roles and Controversies of Radiotherapy in the Treatment of Glioblastoma. J. Med. Radiat. Sci. 2016, 63, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Niyazi, M.; Alongi, F.; Navarria, P.; Belka, C. Current Status and Recent Advances in Reirradiation of Glioblastoma. Radiat Oncol. 2021, 16, 36. [Google Scholar] [CrossRef]
- Chelliah, S.S.; Paul, E.A.L.; Kamarudin, M.N.A.; Parhar, I. Challenges and Perspectives of Standard Therapy and Drug Development in High-Grade Gliomas. Molecules 2021, 26, 1169. [Google Scholar] [CrossRef]
- El-Khayat, S.M.; Arafat, W.O. Therapeutic Strategies of Recurrent Glioblastoma and its Molecular Pathways ‘Lock Up the Beast’. Ecancermedicalscience 2021, 15, 1176. [Google Scholar] [CrossRef]
- Bao, Z.; Wang, Y.; Wang, Q.; Fang, S.; Shan, X.; Wang, J.; Jiang, T. Intratumor Heterogeneity, Microenvironment, and Mechanisms of Drug Resistance in Glioma Recurrence and Evolution. Front. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Singh, G.; Manjila, S.; Sakla, N.; True, A.; Wardeh, A.H.; Beig, N.; Vaysberg, A.; Matthews, J.; Prasanna, P.; Spektor, V. Radiomics and Radiogenomics in Gliomas: A Contemporary Update. Br. J. Cancer 2021, 1–17. [Google Scholar] [CrossRef]
- Mair, M.J.; Geurts, M.; van den Bent, M.J.; Berghoff, A.S. A Basic Review on Systemic Treatment Options in WHO Grade II-III Gliomas. Cancer Treat. Rev. 2021, 92, 102124. [Google Scholar] [CrossRef]
- Wang, K.Y.; Chen, M.M.; Malayil Lincoln, C.M. Adult Primary Brain Neoplasm, Including 2016 World Health Organization Classification. Neuroimaging Clin. N. Am. 2021, 31, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Nam, D.H.; Ram, Z.; Poon, W.S.; Wang, J.; Boldbaatar, D.; Mao, Y.; Ma, W.; Mao, Q.; You, Y.; et al. Clinical Practice Guidelines for the Management of Adult Diffuse Gliomas. Cancer Lett. 2021, 499, 60–72. [Google Scholar] [CrossRef]
- Lee, D.; Riestenberg, R.A.; Haskell-Mendoza, A.; Bloch, O. Diffuse Astrocytic Glioma, IDH-Wildtype, with Molecular Features of Glioblastoma, WHO Grade IV: A Single-Institution Case Series and Review. J. Neurooncol. 2021, 152, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Huo, J.; Li, B.; Cui, Y.; Zhang, H.; Zhang, L.; Ma, L. Predicting Isocitrate Dehydrogenase (IDH) Mutation Status in Gliomas using Multiparameter MRI Radiomics Features. J. Magn. Reson. Imaging 2021, 53, 1399–1407. [Google Scholar] [CrossRef]
- Kawai, T.; Brender, J.R.; Lee, J.A.; Kramp, T.; Kishimoto, S.; Krishna, M.C.; Tofilon, P.; Camphausen, K.A. Detection of Metabolic Change in Glioblastoma Cells After Radiotherapy using Hyperpolarized (13) C-MRI. NMR Biomed. 2021, 34, e4514. [Google Scholar] [CrossRef] [PubMed]
- Sui, Z.; Zhang, X.; Li, H.; Xu, D.; Li, G. Magnetic Resonance Imaging Evaluation of Brain Glioma before Postoperative Radiotherapy. Clin. Transl. Oncol. 2021, 23, 820–826. [Google Scholar] [CrossRef]
- Viswanath, P.; Batsios, G.; Mukherjee, J.; Gillespie, A.M.; Larson, P.E.Z.; Luchman, H.A.; Phillips, J.J.; Costello, J.F.; Pieper, R.O.; Ronen, S.M. Non-Invasive Assessment of Telomere Maintenance Mechanisms in Brain Tumors. Nat. Commun. 2021, 12, 92. [Google Scholar] [CrossRef]
- Park, I.; Kim, S.; Pucciarelli, D.; Song, J.; Choi, J.M.; Lee, K.H.; Kim, Y.H.; Jung, S.; Yoon, W.; Nakamura, J.L. Differentiating Radiation Necrosis from Brain Tumor using Hyperpolarized Carbon-13 MR Metabolic Imaging. Mol. Imaging Biol. 2021, 23, 417–426. [Google Scholar] [CrossRef]
- Anami, S.; Fukai, J.; Hama, M.; Awaya, A.; Inagaki, T.; Chiba, T.; Noda, Y.; Kanemura, Y.; Nakao, N.; Sonomura, T. Brainstem Infiltration Predicts Survival in Patients with High-Grade Gliomas Treated with Chemoradiotherapy. Anticancer Res. 2021, 41, 2583–2589. [Google Scholar] [CrossRef] [PubMed]
- Panciani, P.P.; Giordana, M.T.; Gallone, S.; Muratori, A.; Rotunno, R.; Migliorati, K.; Spena, G.; Ducati, A.; Fontanella, M. Blood-Tissue Analysis of TP53 Polymorphisms and Survival of Patients with Glioma. J. Neurosurg. Sci. 2021, 65, 8–13. [Google Scholar] [CrossRef]
- Massey, S.C.; Whitmire, P.; Doyle, T.E.; Ippolito, J.E.; Mrugala, M.M.; Hu, L.S.; Canoll, P.; Anderson, A.R.A.; Wilson, M.A.; Fitzpatrick, S.M.; et al. Sex Differences in Health and Disease: A Review of Biological Sex Differences Relevant to Cancer with a Spotlight on Glioma. Cancer Lett. 2021, 498, 178–187. [Google Scholar] [CrossRef]
- Zhang, Q.Q.; Xiong, J.; Lu, D.L.; Wang, Z.X.; Sun, S.Y.; Liu, W.W. Expression and Clinical Significance of CXC Chemokine Ligand 10 in Glioma. Zhonghua Yi Xue Za Zhi 2021, 101, 1031–1035. [Google Scholar]
- Kocakavuk, E.; Anderson, K.J.; Varn, F.S.; Johnson, K.C.; Amin, S.B.; Sulman, E.P.; Lolkema, M.P.; Barthel, F.P.; Verhaak, R.G.W. Radiotherapy is Associated with a Deletion Signature that Contributes to Poor Outcomes in Patients with Cancer. Nat. Genet. 2021, 53, 1088–1096. [Google Scholar] [CrossRef]
- Liu, J.; Hormuth, D.A.; Davis, T.; Yang, J.; McKenna, M.T.; Jarrett, A.M.; Enderling, H.; Brock, A.; Yankeelov, T.E. A Time-Resolved Experimental-Mathematical Model for Predicting the Response of Glioma Cells to Single-Dose Radiation Therapy. Integr. Biol. 2021, 13, 167–183. [Google Scholar]
- Daniel, A.G.S.; Park, K.Y.; Roland, J.L.; Dierker, D.; Gross, J.; Humphries, J.B.; Hacker, C.D.; Snyder, A.Z.; Shimony, J.S.; Leuthardt, E.C. Functional Connectivity within Glioblastoma Impacts overall Survival. Neuro Oncol. 2021, 23, 412–421. [Google Scholar] [CrossRef]
- Lang, F.; Liu, Y.; Chou, F.J.; Yang, C. Genotoxic Therapy and Resistance Mechanism in Gliomas. Pharmacol. Ther. 2021, 228, 107922. [Google Scholar] [CrossRef]
- Osuka, S.; Zhu, D.; Zhang, Z.; Li, C.; Stackhouse, C.T.; Sampetrean, O.; Olson, J.J.; Gillespie, G.Y.; Saya, H.; Willey, C.D.; et al. N-Cadherin Upregulation Mediates Adaptive Radioresistance in Glioblastoma. J. Clin. Investig. 2021, 131, 136098. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, H.J.; Jung, C.W.; Choi, B.I.; Lee, D.H.; Park, M.J. PARK7 Maintains the Stemness of Glioblastoma Stem Cells by Stabilizing Epidermal Growth Factor Receptor Variant III. Oncogene 2021, 40, 508–521. [Google Scholar] [CrossRef]
- Nimbalkar, V.P.; Kruthika, B.S.; Sravya, P.; Rao, S.; Sugur, H.S.; Verma, B.K.; Chickabasaviah, Y.T.; Arivazhagan, A.; Kondaiah, P.; Santosh, V. Differential Gene Expression in Peritumoral Brain Zone of Glioblastoma: Role of SERPINA3 in Promoting Invasion, Stemness and Radioresistance of Glioma Cells and Association with Poor Patient Prognosis and Recurrence. J. Neurooncol. 2021, 152, 55–65. [Google Scholar] [CrossRef]
- Jung, E.; Osswald, M.; Ratliff, M.; Dogan, H.; Xie, R.; Weil, S.; Hoffmann, D.C.; Kurz, F.T.; Kessler, T.; Heiland, S.; et al. Tumor Cell Plasticity, Heterogeneity, and Resistance in Crucial Microenvironmental Niches in Glioma. Nat. Commun. 2021, 12, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Zhang, S.; Li, Y.; Liu, Z.; Mi, L.; Cai, Y.; Wang, X.; Chen, L.; Ran, H.; Xiao, D.; et al. Suppression of Mitochondrial ROS by Prohibitin Drives Glioblastoma Progression and Therapeutic Resistance. Nat. Commun. 2021, 12, 3720. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Cao, F.; Xiong, Y.; Zhou, H. SP1 Transcriptionally Activates NLRP6 Inflammasome and Induces Immune Evasion and Radioresistance in Glioma Cells. Int. Immunopharmacol. 2021, 98, 107858. [Google Scholar] [CrossRef]
- Allen, M.; Bjerke, M.; Edlund, H.; Nelander, S.; Westermark, B. Origin of the U87MG Glioma Cell Line: Good News and Bad News. Sci. Transl. Med. 2016, 8, 354re3. [Google Scholar] [CrossRef]
- Berg, T.J.; Marques, C.; Pantazopoulou, V.; Johansson, E.; von Stedingk, K.; Lindgren, D.; Jeannot, P.; Pietras, E.J.; Bergström, T.; Swartling, F.J.; et al. The Irradiated Brain Microenvironment Supports Glioma Stemness and Survival Via Astrocyte-Derived Transglutaminase 2. Cancer Res. 2021, 81, 2101–2115. [Google Scholar] [CrossRef]
- Riva, M.; Wouters, R.; Sterpin, E.; Giovannoni, R.; Boon, L.; Himmelreich, U.; Gsell, W.; Van Ranst, M.; Coosemans, A. Radiotherapy, Temozolomide, and Antiprogrammed Cell Death Protein 1 Treatments Modulate the Immune Microenvironment in Experimental High-Grade Glioma. Neurosurgery 2021, 88, E205–E215. [Google Scholar]
- Chédeville, A.L.; Madureira, P.A. The Role of Hypoxia in Glioblastoma Radiotherapy Resistance. Cancers 2021, 13, 542. [Google Scholar] [CrossRef]
- Hettie, K.S.; Klockow, J.L.; Moon, E.J.; Giaccia, A.J.; Chin, F.T. A NIR Fluorescent Smart Probe for Imaging Tumor Hypoxia. Cancer. Rep. 2021, e1384. [Google Scholar] [CrossRef]
- Zamora, P.L.; Miller, S.R.; Kovoor, J.J. Single Institution Experience in Re-Irradiation of Biopsy-Proven Diffuse Intrinsic Pontine Gliomas. Childs Nerv. Syst. 2021, 37, 2539–2543. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhao, Q.; Shi, W.; Zheng, Z.; Liu, Z.; Meng, L.; Dong, L.; Jiang, X. Advances in Radiotherapy and Comprehensive Treatment of High-Grade Glioma: Immunotherapy and Tumor-Treating Fields. J. Cancer 2021, 12, 1094–1104. [Google Scholar] [CrossRef]
- Gupta, T.; Maitre, M.; Maitre, P.; Goda, J.S.; Krishnatry, R.; Chatterjee, A.; Moiyadi, A.; Shetty, P.; Epari, S.; Sahay, A.; et al. High-Dose Salvage Re-Irradiation for Recurrent/Progressive Adult Diffuse Glioma: Healing Or Hurting? Clin. Transl. Oncol. 2021, 23, 1358–1367. [Google Scholar] [CrossRef]
- Guan, Y.; Xiong, J.; Pan, M.; Shi, W.; Li, J.; Zhu, H.; Gong, X.; Li, C.; Mei, G.; Liu, X.; et al. Safety and Efficacy of Hypofractionated Stereotactic Radiosurgery for High-Grade Gliomas at First Recurrence: A Single-Center Experience. BMC Cancer 2021, 21, 123. [Google Scholar] [CrossRef]
- Zhao, M.; Fu, X.; Zhang, Z.; Ma, L.; Wang, X.; Li, X. Gamma Knife Radiosurgery for High-Grade Gliomas: Single-Center Experience of Six Years in China. Stereotact. Funct. Neurosurg. 2021, 99, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Dono, A.; Mitra, S.; Shah, M.; Takayasu, T.; Zhu, J.J.; Tandon, N.; Patel, C.B.; Esquenazi, Y.; Ballester, L.Y. PTEN Mutations Predict Benefit from Tumor Treating Fields (TTFields) Therapy in Patients with Recurrent Glioblastoma. J. Neurooncol. 2021, 153, 153–160. [Google Scholar] [CrossRef]
- Sanvito, F.; Castellano, A.; Falini, A. Advancements in Neuroimaging to Unravel Biological and Molecular Features of Brain Tumors. Cancers 2021, 13, 424. [Google Scholar] [CrossRef]
- Galldiks, N.; Niyazi, M.; Grosu, A.L.; Kocher, M.; Langen, K.J.; Law, I.; Minniti, G.; Kim, M.M.; Tsien, C.; Dhermain, F.; et al. Contribution of PET Imaging to Radiotherapy Planning and Monitoring in Glioma Patients—A Report of the PET/RANO Group. Neuro Oncol. 2021, 23, 881–893. [Google Scholar] [CrossRef]
- Galldiks, N.; Niyazi, M.; Tonn, J.C.; Langen, K.J. Reply to the Letter regarding”Contribution of PET Imaging to Radiotherapy Planning and Monitoring in Glioma Patients-a Report of the PET/RANO Group”: 18F-Fluciclovine and Target Volume Delineation. Neuro Oncol. 2021. [Google Scholar] [CrossRef]
- Prost, D.M.; Merenzon, M.A.; Gómez-Escalante, J.I.; Primavera, A.; Vargas Benítez, M.; Gil, A.S.; Marenco, P.M.; Califano, M.M.; Moughty Cueto, C.; Zaloff Dakoff, J.M.; et al. Effects of Time to Chemoradiation on High-Grade Gliomas from the Buenos Aires Metropolitan Area. PLoS ONE 2021, 16, e0249486. [Google Scholar] [CrossRef]
- Toor, H.; Savla, P.; Podkovik, S.; Patchana, T.; Ghanchi, H.; Kashyap, S.; Tashjian, V.; Miulli, D. Timing of Chemoradiation in Newly Diagnosed Glioblastoma: Comparative Analysis between County and Managed Care Health Care Models. World Neurosurg. 2021, 149, e1038–e1042. [Google Scholar] [CrossRef]
- Yan, D.; Ziaja, E.; Jaffray, D.; Wong, J.; Brabbins, D.; Vicini, F.; Martinez, A. The use of Adaptive Radiation Therapy to Reduce Setup Error: A Prospective Clinical Study. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 715–720. [Google Scholar] [CrossRef]
- Cao, Y.; Tang, D.; Xiang, Y.; Men, L.; Liu, C.; Zhou, Q.; Wu, J.; Huo, L.; Song, T.; Wang, Y.; et al. Study on the Appropriate Timing of Postoperative Adaptive Radiotherapy for High-Grade Glioma. Cancer. Manag. Res. 2021, 13, 3561–3572. [Google Scholar]
- Tsien, C.I.; Brown, D.; Normolle, D.; Schipper, M.; Piert, M.; Junck, L.; Heth, J.; Gomez-Hassan, D.; Ten Haken, R.K.; Chenevert, T.; et al. Concurrent Temozolomide and Dose-Escalated Intensity-Modulated Radiation Therapy in Newly Diagnosed Glioblastoma. Clin. Cancer Res. 2012, 18, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Frosina, G.; Fontana, V.; Verzola, D.; Rosa, A.; Gaggero, G.; Garibotto, G.; Vagge, S.; Pigozzi, S.; Daga, A. Ultra-Hyper-Fractionated Radiotherapy for High Grade Gliomas. J. Neurosci. Res. 2021, in press. [Google Scholar]
- Detti, B.; Scoccianti, S.; Teriaca, M.A.; Maragna, V.; Lorenzetti, V.; Lucidi, S.; Bellini, C.; Greto, D.; Desideri, I.; Livi, L. Bevacizumab in Recurrent High-Grade Glioma: A Single Institution Retrospective Analysis on 92 Patients. Radiol. Med. 2021, 1–6. [Google Scholar] [CrossRef]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab Plus Radiotherapy-Temozolomide for Newly Diagnosed Glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.; Won, M.; et al. A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Voss, M.; Wenger, K.J.; Fokas, E.; Forster, M.T.; Steinbach, J.P.; Ronellenfitsch, M.W. Single-Shot Bevacizumab for Cerebral Radiation Injury. BMC Neurol. 2021, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Kulinich, D.P.; Sheppard, J.P.; Nguyen, T.; Kondajji, A.M.; Unterberger, A.; Duong, C.; Enomoto, A.; Patel, K.; Yang, I. Radiotherapy Versus Combination Radiotherapy-Bevacizumab for the Treatment of Recurrent High-Grade Glioma: A Systematic Review. Acta Neurochir. 2021, 163, 1921–1934. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Bailleul, Q.; Rakotomalala, A.; Ferry, I.; Leblond, P.; Meignan, S.; Furlan, A. The Art of War as Applied to Pediatric Gliomas: Know Your Enemy. Med. Sci. 2021, 37, 159–166. [Google Scholar]
- Friedman, G.K.; Johnston, J.M.; Bag, A.K.; Bernstock, J.D.; Li, R.; Aban, I.; Kachurak, K.; Nan, L.; Kang, K.D.; Totsch, S.; et al. Oncolytic HSV-1 G207 Immunovirotherapy for Pediatric High-Grade Gliomas. N. Engl. J. Med. 2021, 384, 1613–1622. [Google Scholar] [CrossRef]
- Shi, S.; Lu, S.; Jing, X.; Liao, J.; Li, Q. The Prognostic Impact of Radiotherapy in Conjunction with Temozolomide in Diffuse Intrinsic Pontine Glioma: A Systematic Review and Meta-Analysis. World Neurosurg. 2021, 148, e565–e571. [Google Scholar] [CrossRef]
- Krishnatry, R.; Manjali, J.J.; Chinnaswamy, G.; Chatterjee, A.; Goda, J.S.; Janu, A.; Sahu, A.; Jalali, R.; Gupta, T. Clinical Approach to Re-Irradiation for Recurrent Diffuse Intrinsic Pontine Glioma. Jpn. J. Clin. Oncol. 2021, 51, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Nunna, R.S.; Khalid, S.; Behbahani, M.; Mehta, A.I. Pediatric Primary High-Grade Spinal Glioma: A National Cancer Database Analysis of Current Patterns in Treatment and Outcomes. Childs Nerv. Syst. 2021, 37, 185–193. [Google Scholar] [CrossRef]
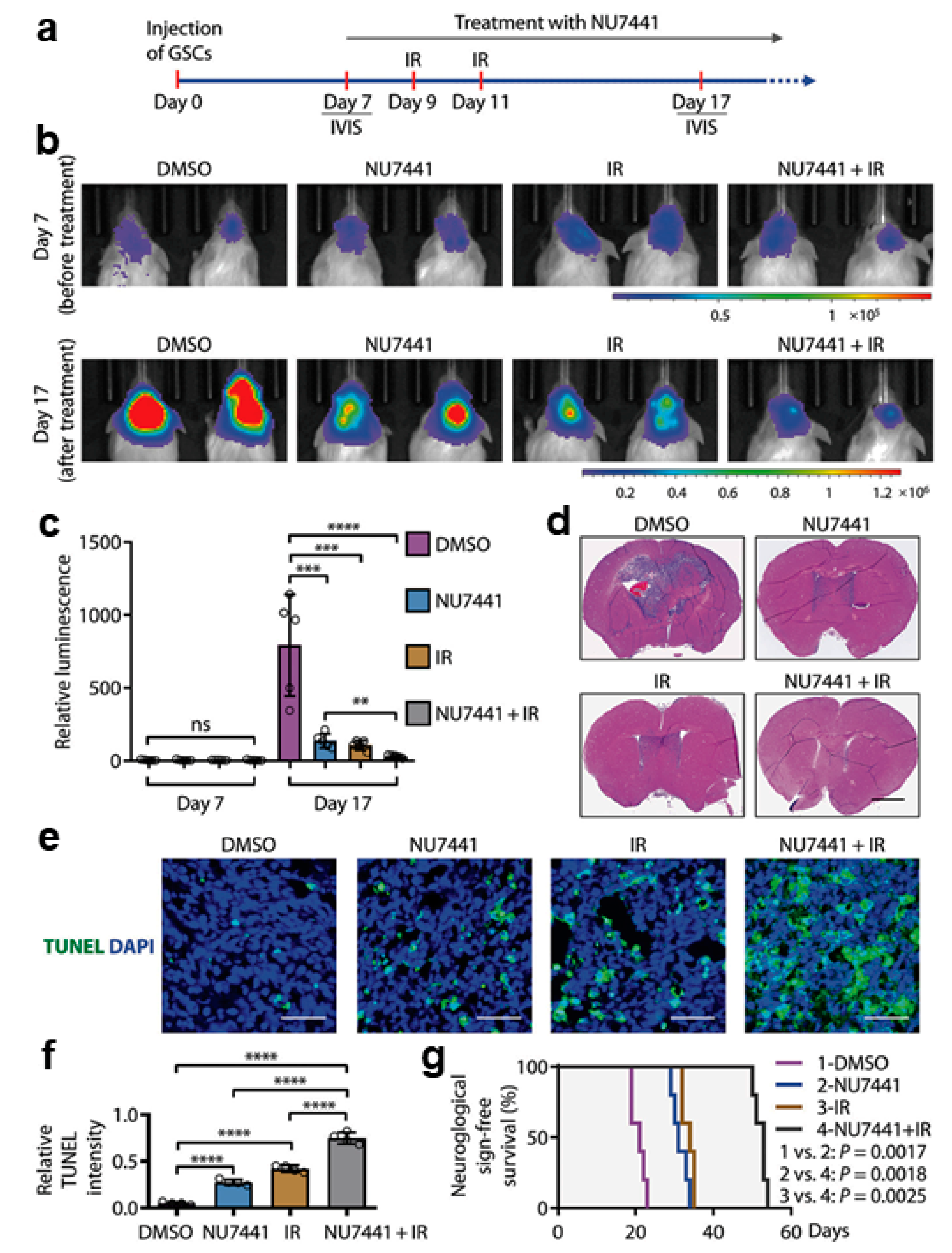
- Fang, X.; Huang, Z.; Zhai, K.; Huang, Q.; Tao, W.; Kim, L.; Wu, Q.; Almasan, A.; Yu, J.S.; Li, X.; et al. Inhibiting DNA-PK Induces Glioma Stem Cell Differentiation and Sensitizes Glioblastoma to Radiation in Mice. Sci. Transl. Med. 2021, 13, eabc7275. [Google Scholar] [CrossRef] [PubMed]
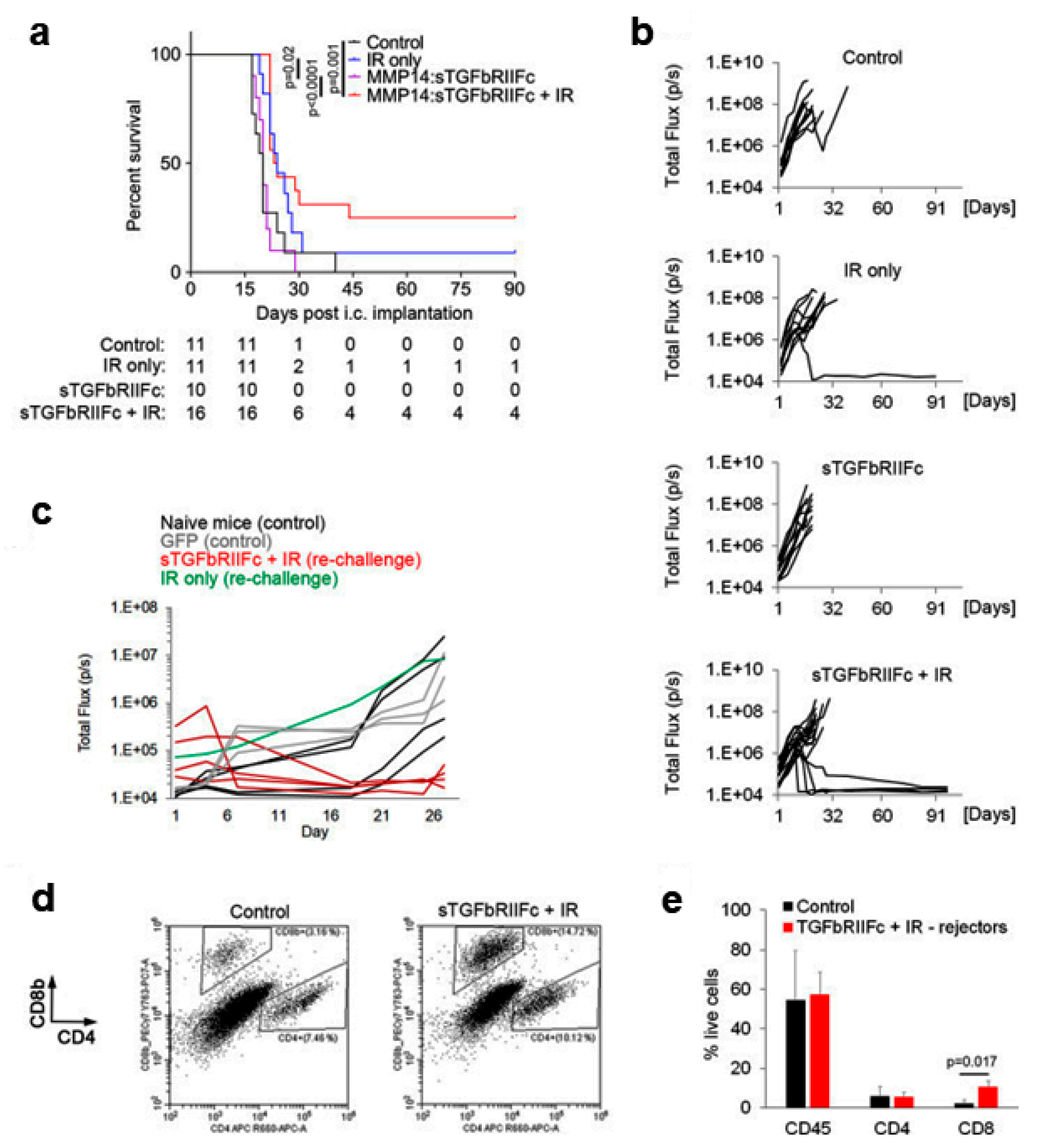
- Andreou, T.; Williams, J.; Brownlie, R.J.; Salmond, R.J.; Watson, E.; Shaw, G.; Melcher, A.; Wurdak, H.; Short, S.C.; Lorger, M. Hematopoietic Stem Cell Gene Therapy Targeting TGFβ Enhances the Efficacy of Irradiation Therapy in a Preclinical Glioblastoma Model. J. Immunother. Cancer 2021, 9, e001143. [Google Scholar] [CrossRef]
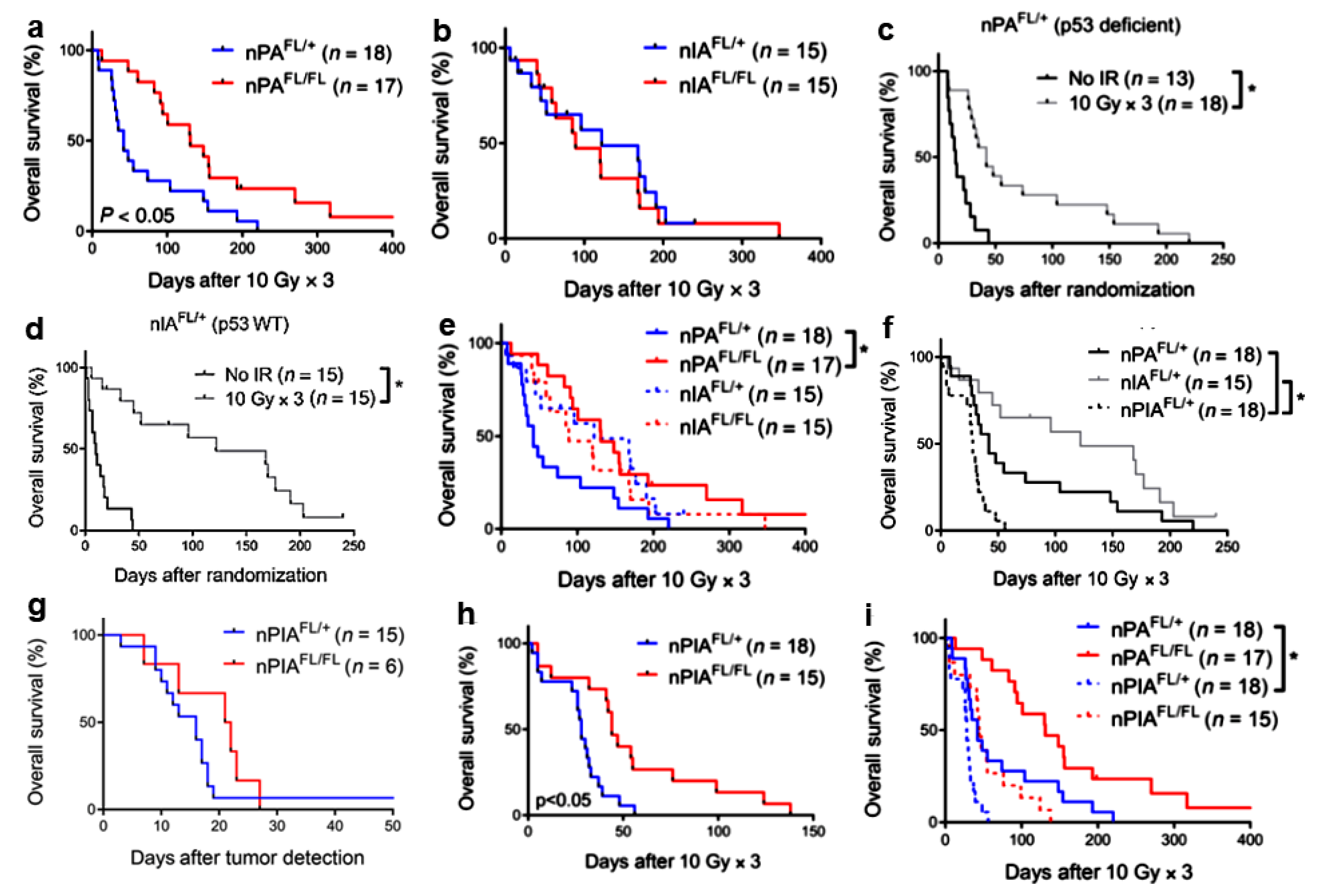
- Deland, K.; Starr, B.F.; Mercer, J.S.; Byemerwa, J.; Crabtree, D.M.; Williams, N.T.; Luo, L.; Ma, Y.; Chen, M.; Becher, O.J.; et al. Tumor Genotype Dictates Radiosensitization After Atm Deletion in Primary Brainstem Glioma Models. J. Clin. Investig. 2021, 131, e142158. [Google Scholar] [CrossRef]
- Barton, K.L.; Misuraca, K.; Cordero, F.; Dobrikova, E.; Min, H.D.; Gromeier, M.; Kirsch, D.G.; Becher, O.J. PD-0332991, a CDK4/6 Inhibitor, significantly Prolongs Survival in a Genetically Engineered Mouse Model of Brainstem Glioma. PLoS ONE 2013, 8, e77639. [Google Scholar] [CrossRef] [Green Version]
- Frosina, G.; Marubbi, D.; Marcello, D.; Vecchio, D.; Daga, A. The Efficacy and Toxicity of ATM Inhibition in Glioblastoma Initiating Cells-Driven Tumor Models. Crit. Rev. Oncol. Hematol. 2019, 138, 214–222. [Google Scholar] [CrossRef] [PubMed]
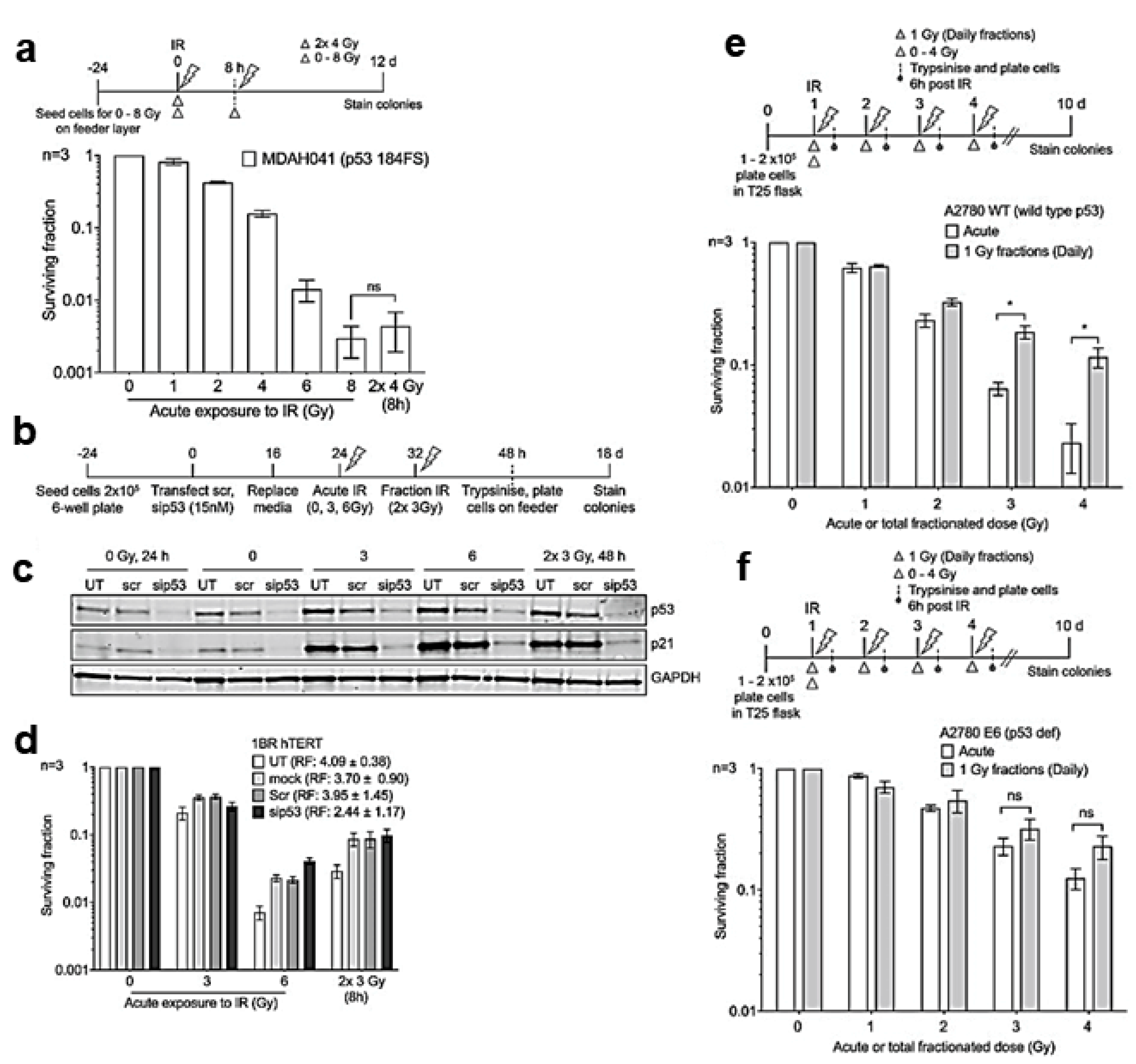
- Anbalagan, S.; Ström, C.; Downs, J.A.; Jeggo, P.A.; McBay, D.; Wilkins, A.; Rothkamm, K.; Harrington, K.J.; Yarnold, J.R.; Somaiah, N. TP53 Modulates Radiotherapy Fraction Size Sensitivity in Normal and Malignant Cells. Sci. Rep. 2021, 11, 7119. [Google Scholar] [CrossRef] [PubMed]
- Biddlestone-Thorpe, L.; Sajjad, M.; Rosenberg, E.; Beckta, J.M.; Valerie, N.C.; Tokarz, M.; Adams, B.R.; Wagner, A.F.; Khalil, A.; Gilfor, D.; et al. ATM Kinase Inhibition Preferentially Sensitizes p53-Mutant Glioma to Ionizing Radiation. Clin. Cancer Res. 2013, 19, 3189–3200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchio, D.; Daga, A.; Carra, E.; Marubbi, D.; Raso, A.; Mascelli, S.; Nozza, P.; Garre, M.L.; Pitto, F.; Ravetti, J.L.; et al. Pharmacokinetics, Pharmacodynamics and Efficacy on Pediatric Tumors of the Glioma Radiosensitizer KU60019. Int. J. Cancer 2015, 136, 1445–1457. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Sun, Y.; Sun, X.; Li, J.; Shi, X.; Liang, Z.; Ma, Y.; Zhang, X. AEG-1 Knockdown Sensitizes Glioma Cells to Radiation through Impairing Homologous Recombination Via Targeting RFC5. DNA Cell Biol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nile, D.L.; Rae, C.; Walker, D.J.; Waddington, J.C.; Vincent, I.; Burgess, K.; Gaze, M.N.; Mairs, R.J.; Chalmers, A.J. Inhibition of Glycolysis and Mitochondrial Respiration Promotes Radiosensitisation of Neuroblastoma and Glioma Cells. Cancer. Metab. 2021, 9, 24. [Google Scholar] [CrossRef]
- Allahgholipour, S.Z.; Farzipour, S.; Ghasemi, A.; Asgarian-Omran, H.; Hosseinimehr, S.J. The Radiosensitizing Effect of Olanzapine as an Antipsychotic Medication in Glioblastoma Cell. Curr. Radiopharm. 2021, 14, 1. [Google Scholar] [CrossRef]
- Nordmann, N.J.; Michael, A.P. 5-Aminolevulinic Acid Radiodynamic Therapy for Treatment of High-Grade Gliomas: A Systematic Review. Clin. Neurol. Neurosurg. 2021, 201, 106430. [Google Scholar] [CrossRef]
- Chen, M.H.; Liu, T.Y.; Chen, Y.C.; Chen, M.H. Combining Augmented Radiotherapy and Immunotherapy through a Nano-Gold and Bacterial Outer-Membrane Vesicle Complex for the Treatment of Glioblastoma. Nanomaterials 2021, 11, 1661. [Google Scholar] [CrossRef]
- Sotiropoulos, M.; Brisebard, E.; Le Dudal, M.; Jouvion, G.; Juchaux, M.; Crépin, D.; Sebrie, C.; Jourdain, L.; Labiod, D.; Lamirault, C.; et al. X-rays Minibeam Radiation Therapy at a Conventional Irradiator: Pilot Evaluation in F98-Glioma Bearing Rats and Dose Calculations in a Human Phantom. Clin. Transl. Radiat. Oncol. 2021, 27, 44–49. [Google Scholar] [CrossRef]
- Sminia, P.; van den Berg, J.; van Kootwijk, A.; Hageman, E.; Slotman, B.J.; Verbakel, W.F.A.R. Experimental and Clinical Studies on Radiation and Curcumin in Human Glioma. J. Cancer Res. Clin. Oncol. 2021, 147, 403–409. [Google Scholar] [CrossRef]
- Sapienza, L.G.; Nasra, K.; Berry, R.; Danesh, L.; Little, T.; Abu-Isa, E. Clinical Effects of Morning and Afternoon Radiotherapy on High-Grade Gliomas. Chronobiol. Int. 2021, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sahebjam, S.; Forsyth, P.A.; Tran, N.D.; Arrington, J.A.; Macaulay, R.; Etame, A.B.; Walko, C.M.; Boyle, T.; Peguero, E.N.; Jaglal, M.; et al. Hypofractionated Stereotactic Re-Irradiation with Pembrolizumab and Bevacizumab in Patients with Recurrent High-Grade Gliomas: Results from a Phase I Study. Neuro Oncol. 2021, 23, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Shirvalilou, S.; Khoei, S.; Esfahani, A.J.; Kamali, M.; Shirvaliloo, M.; Sheervalilou, R.; Mirzaghavami, P. Magnetic Hyperthermia as an Adjuvant Cancer Therapy in Combination with Radiotherapy Versus Radiotherapy Alone for Recurrent/Progressive Glioblastoma: A Systematic Review. J. Neurooncol. 2021, 152, 419–428. [Google Scholar] [CrossRef]
- Fernández, E.; Morillo, V.; Salvador, M.; Santafé, A.; Beato, I.; Rodríguez, M.; Ferrer, C. Hyperbaric Oxygen and Radiation Therapy: A Review. Clin. Transl. Oncol. 2021, 23, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Porper, K.; Shpatz, Y.; Plotkin, L.; Pechthold, R.G.; Talianski, A.; Champ, C.E.; Furman, O.; Shimoni-Sebag, A.; Symon, Z.; Amit, U.; et al. A Phase I Clinical Trial of Dose-Escalated Metabolic Therapy Combined with Concomitant Radiation Therapy in High-Grade Glioma. J. Neurooncol. 2021, 1–10. [Google Scholar] [CrossRef]
- Saeed, H.; Tseng, Y.D.; Lo, S.S. Narrative Review of Palliative Hypofractionated Radiotherapy for High Grade Glioma. Ann. Palliat. Med. 2021, 10, 846–862. [Google Scholar] [CrossRef] [PubMed]
- Carr, C.M.; Benson, J.C.; DeLone, D.R.; Diehn, F.E.; Kim, D.K.; Merrell, K.W.; Nagelschneider, A.A.; Madhavan, A.A.; Johnson, D.R. Intracranial Long-Term Complications of Radiation Therapy: An Image-Based Review. Neuroradiology 2021, 63, 471–482. [Google Scholar] [CrossRef]
- Torres, V.A.; Ashford, J.M.; Wright, E.; Xu, J.; Zhang, H.; Merchant, T.E.; Conklin, H.M. The Impact of Socioeconomic Status (SES) on Cognitive Outcomes Following Radiotherapy for Pediatric Brain Tumors: A Prospective, Longitudinal Trial. Neuro Oncol. 2021, 23, 1173–1182. [Google Scholar] [CrossRef]
- Terziev, R.; Psimaras, D.; Marie, Y.; Feuvret, L.; Berzero, G.; Jacob, J.; Dehais, C.; Bompaire, F.; Mueller, W.; Kinnersley, B.; et al. Cumulative Incidence and Risk Factors for Radiation Induced Leukoencephalopathy in High Grade Glioma Long Term Survivors. Sci. Rep. 2021, 11, 10176. [Google Scholar] [CrossRef]
- Hadi, I.; Reitz, D.; Bodensohn, R.; Roengvoraphoj, O.; Lietke, S.; Niyazi, M.; Tonn, J.C.; Belka, C.; Thon, N.; Nachbichler, S.B. Radiation Necrosis After a Combination of External Beam Radiotherapy and Iodine-125 Brachytherapy in Gliomas. Radiat Oncol. 2021, 16, 40. [Google Scholar] [CrossRef]
- Sager, O.; Dincoglan, F.; Demiral, S.; Uysal, B.; Gamsiz, H.; Colak, O.; Ozcan, F.; Gundem, E.; Elcim, Y.; Dirican, B.; et al. Concise Review of Stereotactic Irradiation for Pediatric Glial Neoplasms: Current Concepts and Future Directions. World J. Methodol. 2021, 11, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Grimm, J.; Niemierko, A.; Soltys, S.G.; Moiseenko, V.; Redmond, K.J.; Yorke, E.; Sahgal, A.; Xue, J.; Mahadevan, A.; et al. Single- and Multifraction Stereotactic Radiosurgery Dose/Volume Tolerances of the Brain. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 68–86. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Grimm, J.; Soltys, S.G.; Yorke, E.; Moiseenko, V.; Tomé, W.A.; Sahgal, A.; Xue, J.; Ma, L.; Solberg, T.D.; et al. Single- and Multi-Fraction Stereotactic Radiosurgery Dose Tolerances of the Optic Pathways. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.; Drijver, A.J.; van den Bent, M.J.; Bromberg, J.C.; Hoang-Xuan, K.; Taphoorn, M.J.B.; Reijneveld, J.C.; Ben Hassel, M.; Vauleon, E.; Eekers, D.B.P.; et al. Memory in Low-Grade Glioma Patients Treated with Radiotherapy Or Temozolomide: A Correlative Analysis of EORTC Study 22033–26033. Neuro Oncol. 2021, 23, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Ma, L.; Ye, Z.; Shi, W.; Zhang, L.; Wang, J.; Yang, H. Radiation-Induced Bystander Effects may Contribute to Radiation-Induced Cognitive Impairment. Int. J. Radiat. Biol. 2021, 97, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Mendonca, M.S. News FLASH-RT: To Treat GBM and Spare Cognition, Fraction Size and Total Dose Matter. Clin. Cancer Res. 2021, 27, 662–664. [Google Scholar] [CrossRef] [PubMed]
- Montay-Gruel, P.; Acharya, M.M.; Gonçalves Jorge, P.; Petit, B.; Petridis, I.G.; Fuchs, P.; Leavitt, R.; Petersson, K.; Gondré, M.; Ollivier, J.; et al. Hypofractionated FLASH-RT as an Effective Treatment Against Glioblastoma that Reduces Neurocognitive Side Effects in Mice. Clin. Cancer Res. 2021, 27, 775–784. [Google Scholar] [CrossRef]
- Brown, P.D.; Chung, C.; Liu, D.D.; McAvoy, S.; Grosshans, D.; Al Feghali, K.; Mahajan, A.; Li, J.; McGovern, S.L.; McAleer, M.F.; et al. A Prospective Phase II Randomized Trial of Proton Radiotherapy Vs. Intensity Modulated Radiotherapy for Patients with Newly Diagnosed Glioblastoma. Neuro Oncol. 2021. [Google Scholar] [CrossRef]
- Journy, N.M.Y.; Zrafi, W.S.; Bolle, S.; Fresneau, B.; Alapetite, C.; Allodji, R.S.; Berchery, D.; Haddy, N.; Kobayashi, I.; Labbé, M.; et al. Risk Factors of Subsequent Central Nervous System Tumors After Childhood and Adolescent Cancers: Findings from the French Childhood Cancer Survivor Study. Cancer Epidemiol. Biomark. Prev. 2021, 30, 133–141. [Google Scholar] [CrossRef]
- Rodrigues, A.J.; Jin, M.C.; Wu, A.; Bhambhvani, H.P.; Li, G.; Grant, G.A. Risk of Secondary Neoplasms After External-Beam Radiation Therapy Treatment of Pediatric Low-Grade Gliomas: A SEER Analysis, 1973-2015. J. Neurosurg. Pediatr. 2021, 1–9. [Google Scholar] [CrossRef]
- Pan, S.P.; Zheng, X.L.; Zhang, N.; Lin, X.M.; Li, K.J.; Xia, X.F.; Zou, C.L.; Zhang, W.Y. A Novel Nomogram for Predicting the Risk of Epilepsy Occurrence After Operative in Gliomas Patients without Preoperative Epilepsy History. Epilepsy Res. 2021, 174, 106641. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.Y.; Oliva, C.R.; Noman, A.S.M.; Allen, B.G.; Goswami, P.C.; Zakharia, Y.; Monga, V.; Spitz, D.R.; Buatti, J.M.; Griguer, C.E. Radioresistance in Glioblastoma and the Development of Radiosensitizers. Cancers 2020, 12, 2511. [Google Scholar] [CrossRef] [PubMed]
- Rossmeisl, J.H.; Herpai, D.; Quigley, M.; Cecere, T.E.; Robertson, J.L.; D’Agostino, R.B.; Hinckley, J.; Tatter, S.B.; Dickinson, P.J.; Debinski, W. Phase I Trial of Convection-Enhanced Delivery of IL13RA2 and EPHA2 Receptor Targeted Cytotoxins in Dogs with Spontaneous Intracranial Gliomas. Neuro Oncol. 2021, 23, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Szychot, E.; Walker, D.; Collins, P.; Hyare, H.; Shankar, A.; Bienemann, A.; Hollingworth, M.; Gill, S. Clinical Experience of Convection-Enhanced Delivery (CED) of Carboplatin and Sodium Valproate into the Pons for the Treatment of Diffuse Intrinsic Pontine Glioma (DIPG) in Children and Young Adults After Radiotherapy. Int. J. Clin. Oncol. 2021, 26, 647–658. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosina, G. Radiotherapy of High-Grade Gliomas: First Half of 2021 Update with Special Reference to Radiosensitization Studies. Int. J. Mol. Sci. 2021, 22, 8942. https://doi.org/10.3390/ijms22168942
Frosina G. Radiotherapy of High-Grade Gliomas: First Half of 2021 Update with Special Reference to Radiosensitization Studies. International Journal of Molecular Sciences. 2021; 22(16):8942. https://doi.org/10.3390/ijms22168942
Chicago/Turabian StyleFrosina, Guido. 2021. "Radiotherapy of High-Grade Gliomas: First Half of 2021 Update with Special Reference to Radiosensitization Studies" International Journal of Molecular Sciences 22, no. 16: 8942. https://doi.org/10.3390/ijms22168942
APA StyleFrosina, G. (2021). Radiotherapy of High-Grade Gliomas: First Half of 2021 Update with Special Reference to Radiosensitization Studies. International Journal of Molecular Sciences, 22(16), 8942. https://doi.org/10.3390/ijms22168942