Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Results
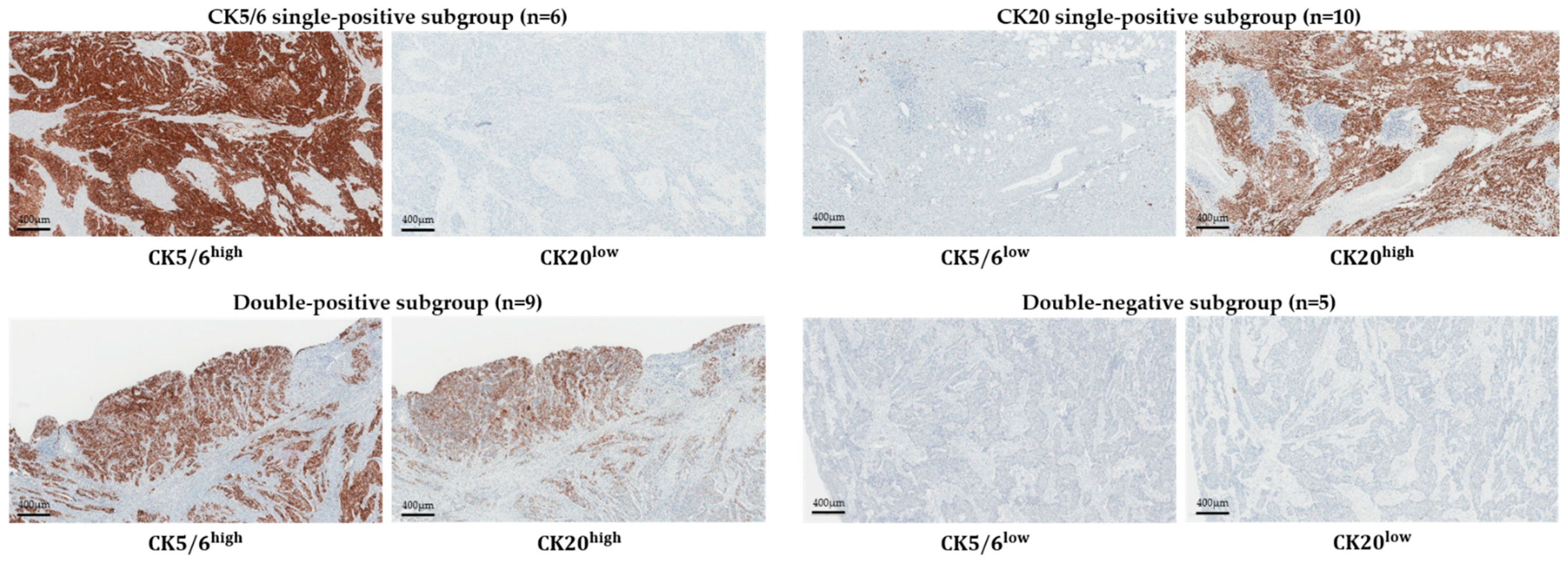
2.1. Subgroup Classification of RNA Sequencing Group
2.2. Differential Expression Genes (DEGs) between Each Subgroups
2.3. Gene Ontology (GO) Analysis
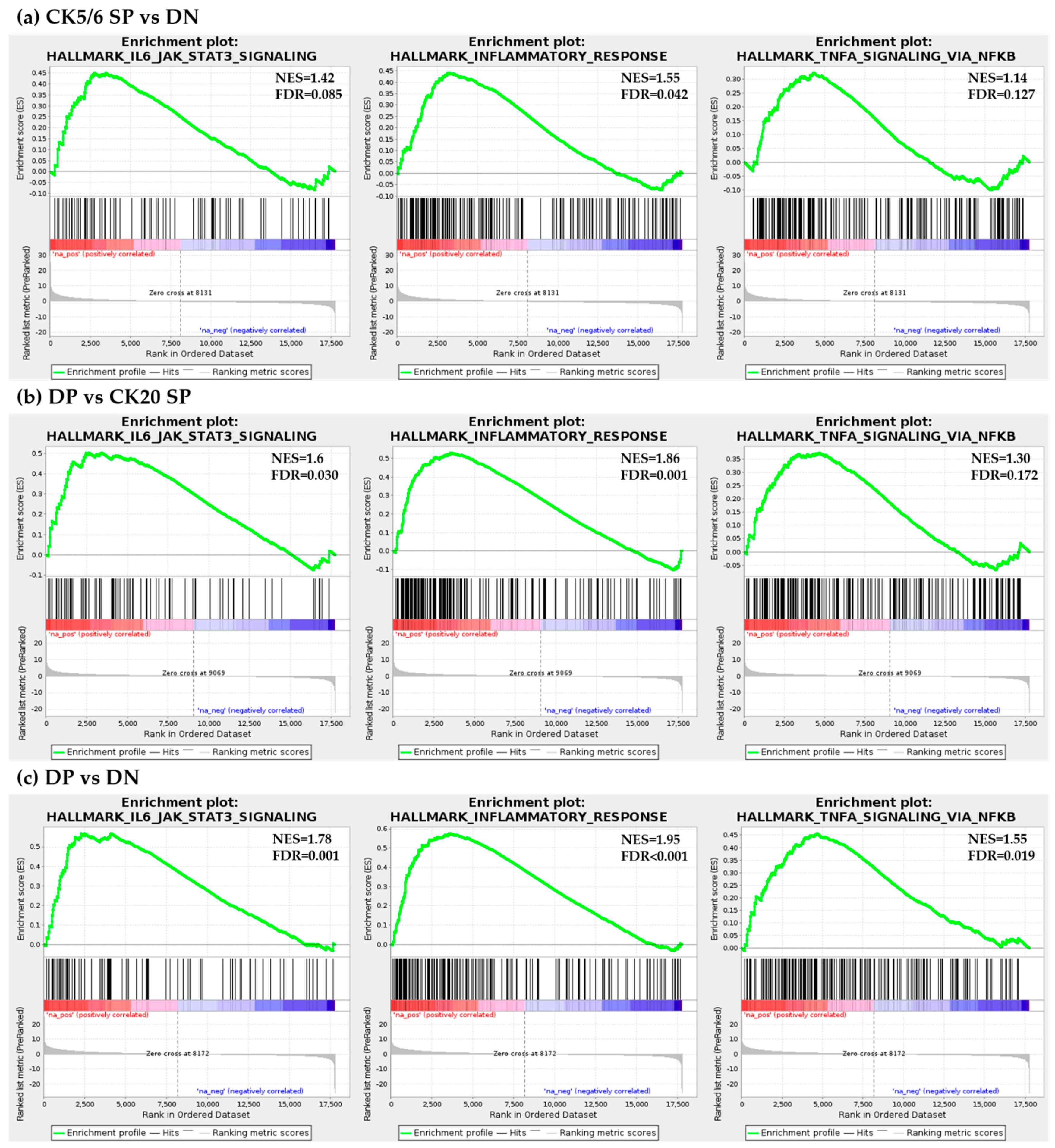
2.4. Ingenuity Pathway Analysis (IPA) and Gene Set Enrichment Analysis (GSEA)
2.5. Expression of Gene Signature Markers
2.6. Clinicopathological Analysis of Immunohistochemistry (IHC)-Based Subgroups
3. Discussion
4. Materials and Methods
4.1. Tissue Samples and Case Selection
4.2. Immunohistochemistry
4.3. RNA Sequencing
4.4. Functional Analysis
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AJCC | American Joint Committee on Cancer |
| BASQ | Basal-squamous-like |
| CK | Cytokeratin |
| DEG | Differential expression gene |
| DN | Double-negative |
| DP | Double-positive |
| EMT | Epithelial-mesenchymal transition |
| FFPE | Formalin-fixed paraffin-embedded |
| GO | Gene ontology |
| GSEA | Gene set enrichment analysis |
| IHC | Immunohistochemistry |
| IL-6 | Interleukin-6 |
| IPA | Ingenuity Pathway Analysis |
| IRB | Institutional Review Board |
| ISUP | International Society of Urologic Pathologists |
| JAK | Janus kinase |
| KEGG | Kyoto Encyclopedia of Genes and Genomes |
| MIBC | Muscle invasive urinary bladder cancer |
| miR | MicroRNA |
| NF-κB | Nuclear factor-κB |
| NGS | Next-generation sequencing |
| OS | Overall survival |
| PD-1 | Programmed cell death-1 |
| PD-L1 | Programmed cell death-ligand 1 |
| PFS | Progression-free survival |
| SP | Single-positive |
| STAT3 | Signal transducer and activator of transcription 3 |
| TMA | Tissue microarray |
| TNF | Tumor necrosis factor |
| UB UC | Urinary bladder urothelial carcinoma |
| WHO | World Health Organization |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Batavia, J.; Yamany, T.; Molotkov, A.; Dan, H.; Mansukhani, M.; Batourina, E.; Schneider, K.; Oyon, D.; Dunlop, M.; Wu, X.R.; et al. Bladder cancers arise from distinct urothelial sub-populations. Nat. Cell Biol. 2014, 16, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.L.; et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Damrauer, J.S.; Hoadley, K.A.; Chism, D.D.; Fan, C.; Tiganelli, C.J.; Wobker, S.E.; Yeh, J.J.; Milowsky, M.I.; Iyer, G.; Parker, J.S.; et al. Intrinsic subtypes of high-grade bladder cancer reflect the hallmarks of breast cancer biology. Proc. Natl. Acad. Sci. USA 2014, 111, 3110–3115. [Google Scholar] [CrossRef] [Green Version]
- Lerner, S.P.; McConkey, D.J.; Hoadley, K.A.; Chan, K.S.; Kim, W.Y.; Radvanyi, F.; Hoglund, M.; Real, F.X. Bladder Cancer Molecular Taxonomy: Summary from a Consensus Meeting. Bladder Cancer 2016, 2, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Lee, C.; Kim, Y.A.; Moon, K.C. PD-L1 Expression in Muscle-Invasive Urinary Bladder Urothelial Carcinoma According to Basal/Squamous-Like Phenotype. Front. Oncol. 2020, 10, 527385. [Google Scholar] [CrossRef]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e525. [Google Scholar] [CrossRef] [Green Version]
- McConkey, D.J.; Choi, W.; Dinney, C.P. Genetic subtypes of invasive bladder cancer. Curr. Opin. Urol. 2015, 25, 449–458. [Google Scholar] [CrossRef]
- McConkey, D.J.; Choi, W.; Ochoa, A.; Siefker-Radtke, A.; Czerniak, B.; Dinney, C.P. Therapeutic opportunities in the intrinsic subtypes of muscle-invasive bladder cancer. Hematol. Oncol. Clin. N. Am. 2015, 29, 377–394. [Google Scholar] [CrossRef]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.G.; Winters, B.; Douglas, J.; Van Kessel, K.E.; Fransen van de Putte, E.E.; Sommerlad, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kwiatkowski, D.; McConkey, D.J.; Meeks, J.J.; Freeman, S.S.; Bellmunt, J.; Getz, G.; Lerner, S.P. The Cancer Genome Atlas Expression Subtypes Stratify Response to Checkpoint Inhibition in Advanced Urothelial Cancer and Identify a Subset of Patients with High Survival Probability. Eur. Urol. 2019, 75, 961–964. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [Green Version]
- Tan, T.Z.; Rouanne, M.; Tan, K.T.; Huang, R.Y.; Thiery, J.P. Molecular Subtypes of Urothelial Bladder Cancer: Results from a Meta-cohort Analysis of 2411 Tumors. Eur. Urol. 2019, 75, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Retz, M.; Siefker-Radtke, A.; Baron, A.; Necchi, A.; Bedke, J.; Plimack, E.R.; Vaena, D.; Grimm, M.O.; Bracarda, S.; et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017, 18, 312–322. [Google Scholar] [CrossRef]
- Sjodahl, G.; Lauss, M.; Lovgren, K.; Chebil, G.; Gudjonsson, S.; Veerla, S.; Patschan, O.; Aine, M.; Ferno, M.; Ringner, M.; et al. A molecular taxonomy for urothelial carcinoma. Clin. Cancer Res. 2012, 18, 3377–3386. [Google Scholar] [CrossRef] [Green Version]
- Sjodahl, G.; Lovgren, K.; Lauss, M.; Patschan, O.; Gudjonsson, S.; Chebil, G.; Aine, M.; Eriksson, P.; Mansson, W.; Lindgren, D.; et al. Toward a molecular pathologic classification of urothelial carcinoma. Am. J. Pathol. 2013, 183, 681–691. [Google Scholar] [CrossRef] [Green Version]
- AJCC Cancer Staging Manual, 8th ed; Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) Springer: New York, NY, USA, 2017; pp. 739–748. [Google Scholar]
- Eble, J.N.; Sauter, G.; Epstein, J.I.; Sesterhenn, I.A. World Health Organization Classification of Tumors: Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs; IARC Press: Lyon, France, 2016. [Google Scholar]
- Choi, W.; Czerniak, B.; Ochoa, A.; Su, X.; Siefker-Radtke, A.; Dinney, C.; McConkey, D.J. Intrinsic basal and luminal subtypes of muscle-invasive bladder cancer. Nat. Rev. Urol. 2014, 11, 400–410. [Google Scholar] [CrossRef]
- de la Rosette, J.; Smedts, F.; Schoots, C.; Hoek, H.; Laguna, P. Changing patterns of keratin expression could be associated with functional maturation of the developing human bladder. J. Urol. 2002, 168, 709–717. [Google Scholar] [CrossRef]
- Volkmer, J.P.; Sahoo, D.; Chin, R.K.; Ho, P.L.; Tang, C.; Kurtova, A.V.; Willingham, S.B.; Pazhanisamy, S.K.; Contreras-Trujillo, H.; Storm, T.A.; et al. Three differentiation states risk-stratify bladder cancer into distinct subtypes. Proc. Natl. Acad. Sci. USA 2012, 109, 2078–2083. [Google Scholar] [CrossRef] [Green Version]
- Kardos, J.; Chai, S.; Mose, L.E.; Selitsky, S.R.; Krishnan, B.; Saito, R.; Iglesia, M.D.; Milowsky, M.I.; Parker, J.S.; Kim, W.Y.; et al. Claudin-low bladder tumors are immune infiltrated and actively immune suppressed. JCI Insight 2016, 1, e85902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeisberg, M.; Neilson, E.G. Biomarkers for epithelial-mesenchymal transitions. J. Clin. Investig. 2009, 119, 1429–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hugo, H.; Ackland, M.L.; Blick, T.; Lawrence, M.G.; Clements, J.A.; Williams, E.D.; Thompson, E.W. Epithelial—Mesenchymal and mesenchymal—Epithelial transitions in carcinoma progression. J. Cell Physiol. 2007, 213, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development and disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.A.; Kraut, N.; Beug, H. Molecular requirements for epithelial-mesenchymal transition during tumor progression. Curr. Opin. Cell Biol. 2005, 17, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Byers, L.A.; Diao, L.; Wang, J.; Saintigny, P.; Girard, L.; Peyton, M.; Shen, L.; Fan, Y.; Giri, U.; Tumula, P.K.; et al. An epithelial-mesenchymal transition gene signature predicts resistance to EGFR and PI3K inhibitors and identifies Axl as a therapeutic target for overcoming EGFR inhibitor resistance. Clin. Cancer Res. 2013, 19, 279–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, M.P.; Tong, P.; Diao, L.; Cardnell, R.J.; Gibbons, D.L.; William, W.N.; Skoulidis, F.; Parra, E.R.; Rodriguez-Canales, J.; Wistuba, I.I.; et al. A Patient-Derived, Pan-Cancer EMT Signature Identifies Global Molecular Alterations and Immune Target Enrichment Following Epithelial-to-Mesenchymal Transition. Clin. Cancer Res. 2016, 22, 609–620. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Gibbons, D.L.; Goswami, S.; Cortez, M.A.; Ahn, Y.H.; Byers, L.A.; Zhang, X.; Yi, X.; Dwyer, D.; Lin, W.; et al. Metastasis is regulated via microRNA-200/ZEB1 axis control of tumour cell PD-L1 expression and intratumoral immunosuppression. Nat. Commun. 2014, 5, 5241. [Google Scholar] [CrossRef]
- Gregory, P.A.; Bert, A.G.; Paterson, E.L.; Barry, S.C.; Tsykin, A.; Farshid, G.; Vadas, M.A.; Khew-Goodall, Y.; Goodall, G.J. The miR-200 family and miR-205 regulate epithelial to mesenchymal transition by targeting ZEB1 and SIP1. Nat. Cell Biol. 2008, 10, 593–601. [Google Scholar] [CrossRef]
- Kusaba, T.; Nakayama, T.; Yamazumi, K.; Yakata, Y.; Yoshizaki, A.; Inoue, K.; Nagayasu, T.; Sekine, I. Activation of STAT3 is a marker of poor prognosis in human colorectal cancer. Oncol. Rep. 2006, 15, 1445–1451. [Google Scholar] [CrossRef] [Green Version]
- Macha, M.A.; Matta, A.; Kaur, J.; Chauhan, S.S.; Thakar, A.; Shukla, N.K.; Gupta, S.D.; Ralhan, R. Prognostic significance of nuclear pSTAT3 in oral cancer. Head Neck 2011, 33, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; O’Keefe, R.A.; Grandis, J.R. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat. Rev. Clin. Oncol. 2018, 15, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhou, B.P. TNF-alpha/NF-kappaB/Snail pathway in cancer cell migration and invasion. Br. J. Cancer 2010, 102, 639–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Y.; Shen, S.; Verma, I.M. NF-kappaB, an active player in human cancers. Cancer Immunol. Res. 2014, 2, 823–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuelten, C.H.; Parent, C.A.; Montell, D.J. Cell motility in cancer invasion and metastasis: Insights from simple model organisms. Nat. Rev. Cancer 2018, 18, 296–312. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Condeelis, J. Regulation of the actin cytoskeleton in cancer cell migration and invasion. Biochim. Biophys. Acta 2007, 1773, 642–652. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, M.; Christofori, G. Mechanisms of motility in metastasizing cells. Mol. Cancer Res. 2010, 8, 629–642. [Google Scholar] [CrossRef] [Green Version]
- Clark, A.G.; Vignjevic, D.M. Modes of cancer cell invasion and the role of the microenvironment. Curr. Opin. Cell Biol. 2015, 36, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Dadhania, V.; Zhang, M.; Zhang, L.; Bondaruk, J.; Majewski, T.; Siefker-Radtke, A.; Guo, C.C.; Dinney, C.; Cogdell, D.E.; Zhang, S.; et al. Meta-Analysis of the Luminal and Basal Subtypes of Bladder Cancer and the Identification of Signature Immunohistochemical Markers for Clinical Use. EBioMedicine 2016, 12, 105–117. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, A.; Liu, S.K.; Vesprini, D.; Xu, B.; Downes, M.R. Basal-subtype bladder tumours show a ‘hot’ immunophenotype. Histopathology 2018, 73, 748–757. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CK5/6 single-positive (CK5/6 SP) vs. double-positive (DP) |
| None related to major cellular function |
| CK5/6 SP vs. CK20 single-positive (CK20 SP) |
| Immune response (leukocyte aggregation) |
| CK5/6 SP vs. double-negative (DN) |
| Immune response (positive regulation of lymphocyte proliferation, positive regulation of T cell activation, positive regulation of T cell proliferation, regulation of B cell receptor signaling pathway, neutrophil activation involved in immune response, and positive regulation of leukocyte cell-cell adhesion) |
| Tumor necrosis factor (TNF) signaling pathway (MyD88-dependent toll-like receptor signaling pathway and positive regulation of NF-κB transcription factor activity) |
| DP vs. CK20 SP |
| Immune response (regulation of T cell proliferation and positive regulation of inflammatory response) |
| DP vs. DN |
| Cell proliferation (positive regulation of cell proliferation) |
| Immune response (T cell proliferation, regulation of T cell activation, regulation of immune response, regulation of inflammatory response, regulation of B cell proliferation, positive regulation of lymphocyte proliferation, positive regulation of T cell activation, and positive regulation of T cell proliferation) |
| TNF signaling pathway (positive regulation of tumor necrosis factor biosynthetic process, positive regulation of tumor necrosis factor production, regulation of tumor necrosis factor biosynthetic process, MyD88-dependent toll-like receptor signaling pathway, positive regulation of I-κB kinase/NF-κB signaling, regulation of I-κB kinase/NF-κB signaling, regulation of interleukin-6 production, and regulation of interleukin-8 secretion) |
| MAPK signaling pathway (activation of MAPK activity, regulation of MAP kinase activity, positive regulation of MAP kinase activity, positive regulation of MAPK cascade, positive regulation of phosphatidylinositol 3-kinase signaling, positive regulation of ERK1 and ERK2 cascade, regulation of ERK1 and ERK2 cascade, and positive regulation of JNK cascade) |
| CK20 SP vs. DN |
| None related to major cellular function |
| CK5/6-Positive vs. CK5/6-Negative |
| Cell migration (positive regulation of cell migration, positive regulation of cell motility, and regulation of cell migration) |
| Immune response (positive regulation of immune response, positive regulation of inflammatory response, positive regulation of lymphocyte proliferation, regulation of immune response, regulation of immune response, B cell activation, regulation of B cell proliferation, positive regulation of T cell activation, regulation of T cell proliferation, and T cell activation) |
| TNF signaling pathway (positive regulation of NF-κB transcription factor activity and MyD88-dependent toll-like receptor signaling pathway) |
| MAPK signaling pathway (positive regulation of MAP kinase activity, positive regulation of MAPK cascade, regulation of MAP kinase activity, regulation of ERK1 and ERK2 cascade, and positive regulation of JNK cascade) |
| CK5/6 SP vs. DP | |
| None related to major cellular function | |
| CK5/6 SP vs. CK20 SP | |
| upregulated in CK5/6 SP | Cancer and invasion of tumor cell lines |
| Adhesion of immune cells | |
| CK5/6 SP vs. DN | |
| upregulated in CK5/6 SP | Cancer, neoplasia of cells, cell movement of cancer cells, cell movement of tumor cell lines, cell movement, and migration of cells |
| Lymphocyte migration, cell movement of T lymphocytes, leukocyte migration, cell movement of mononuclear leukocytes, activation of lymphocytes, proliferation of immune cells, and proliferation of lymphocytes | |
| DP vs. CK20 SP | |
| upregulated in DP | Activation of leukocytes, activation of mononuclear leukocytes, and leukocyte migration |
| Chemotaxis | |
| DP vs. DN | |
| upregulated in DP | Cancer and activation of cells |
| Cell movement, migration of cells, and binding of tumor cell lines | |
| Activation of lymphocytes, lymphocyte migration, cell movement of lymphocytes, immune response of cells, and inflammatory response | |
| I-κB kinase/NF-κB cascade | |
| CK20 SP vs. DN | |
| upregulated in CK20 SP | Activation of cells |
| CK5/6 SP | DP | CK20 SP | DN | Total | p-Value | |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n | ||
| Age (years) | ||||||
| ≤68 | 27 (44.3%) | 7 (53.8%) | 29 (41.4%) | 21 (46.7%) | 84 | 0.846 |
| >68 | 34 (55.7%) | 6 (46.2%) | 41 (58.6%) | 24 (53.3%) | 105 | |
| Gender | ||||||
| Male | 48 (78.7%) | 13 (100.0%) | 58 (82.9%) | 39 (86.7%) | 158 | 0.266 |
| Female | 13 (21.3%) | 0 (0.0%) | 12 (17.1%) | 6 (13.3%) | 31 | |
| Nuclear grade | ||||||
| Low | 1 (1.6%) | 0 (0.0%) | 3 (4.3%) | 3 (6.7%) | 7 | 0.493 |
| High | 60 (98.4%) | 13 (100.0%) | 67 (95.7%) | 42 (93.3%) | 182 | |
| T category | ||||||
| T2 | 55 (90.2%) | 12 (92.3%) | 63 (90.0%) | 42 (93.3%) | 172 | 0.927 |
| T3~4 | 6 (9.8%) | 1 (7.7%) | 7 (10.0%) | 3 (6.7%) | 17 | |
| CK5/6 SP | DP | CK20 SP | DN | Total | p-Value | |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n | ||
| CK14 | ||||||
| Low | 28 (45.9%) | 12 (92.3%) | 69 (98.6%) | 45 (100%) | 154 | <0.001 |
| High | 33 (54.1%) | 1 (7.7%) | 1 (1.4%) | 0 (0.0%) | 35 | |
| CD44 | ||||||
| Low | 2 (3.3%) | 2 (15.4%) | 64 (91.4%) | 34 (75.6%) | 102 | <0.001 |
| High | 59 (96.7%) | 11 (84.6%) | 6 (8.6%) | 11 (24.4%) | 87 | |
| GATA3 | ||||||
| Low | 55 (90.2%) | 3 (23.1%) | 11 (15.7%) | 20 (44.4%) | 89 | <0.001 |
| High | 6 (9.8%) | 10 (76.9%) | 59 (84.3%) | 25 (55.6%) | 100 | |
| FOXA1 | ||||||
| Low | 56 (91.8%) | 9 (69.2%) | 25 (35.7%) | 30 (66.7%) | 120 | <0.001 |
| High | 5 (8.2%) | 4 (30.8%) | 45 (64.3%) | 15 (33.3%) | 69 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.; Jang, I.; Kim, K.; Jung, M.; Lee, C.; Park, J.H.; Kim, Y.A.; Moon, K.C. Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma. Int. J. Mol. Sci. 2021, 22, 628. https://doi.org/10.3390/ijms22020628
Kim B, Jang I, Kim K, Jung M, Lee C, Park JH, Kim YA, Moon KC. Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma. International Journal of Molecular Sciences. 2021; 22(2):628. https://doi.org/10.3390/ijms22020628
Chicago/Turabian StyleKim, Bohyun, Insoon Jang, Kwangsoo Kim, Minsun Jung, Cheol Lee, Jeong Hwan Park, Young A. Kim, and Kyung Chul Moon. 2021. "Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma" International Journal of Molecular Sciences 22, no. 2: 628. https://doi.org/10.3390/ijms22020628
APA StyleKim, B., Jang, I., Kim, K., Jung, M., Lee, C., Park, J. H., Kim, Y. A., & Moon, K. C. (2021). Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma. International Journal of Molecular Sciences, 22(2), 628. https://doi.org/10.3390/ijms22020628