
In Vitro Cartilage Regeneration with a Three-Dimensional Polyglycolic Acid (PGA) Implant in a Bovine Cartilage Punch Model


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Cell-Free PGA
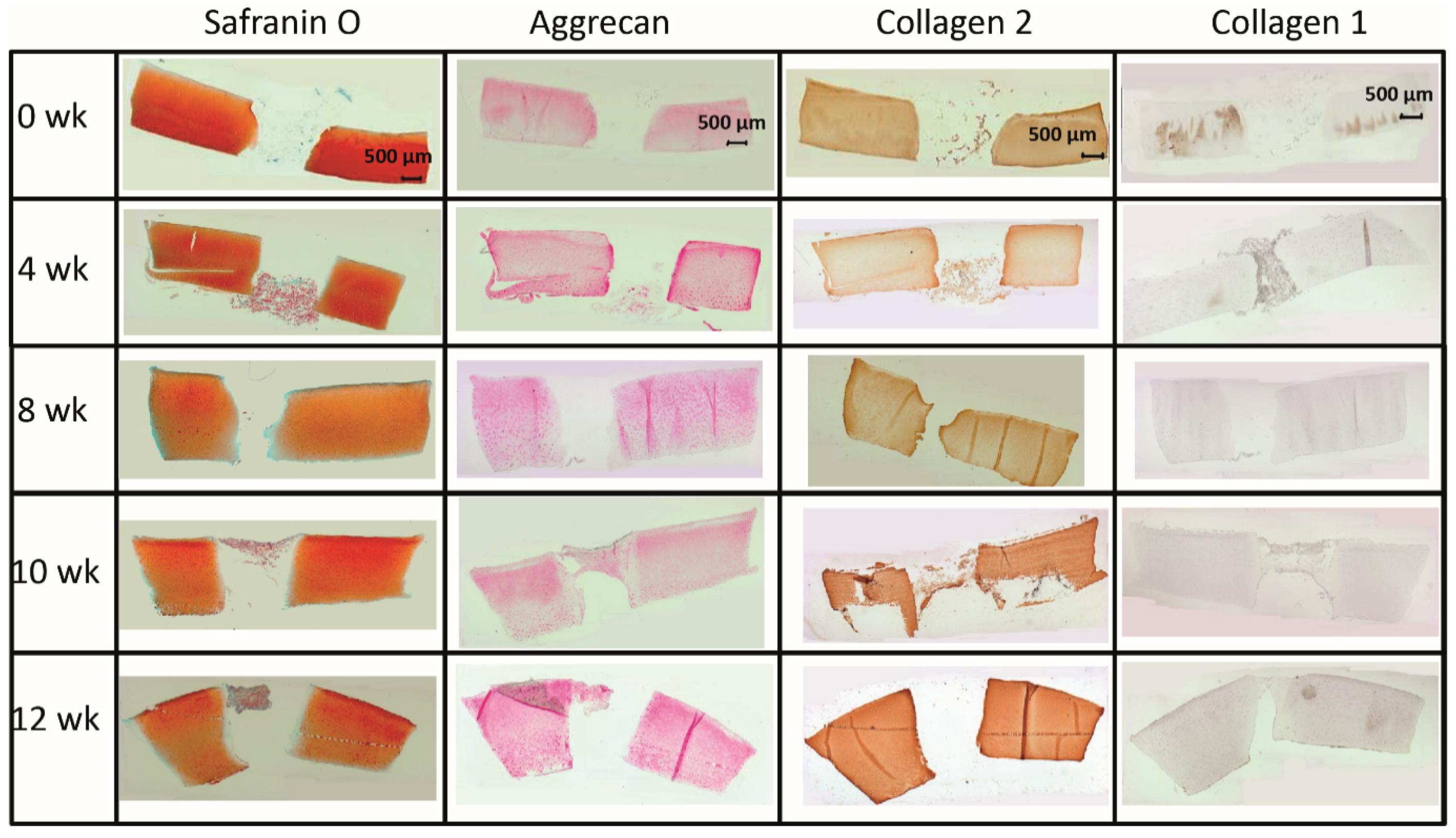
2.1.1. Morphological Features
2.1.2. Content of Cartilage Matrix Proteins (Tissue)
2.1.3. Concentration of Proteoglycans in Tissue and Supernatant (Dimethylmethylene Blue, DMB-Test)
2.1.4. Collagen 2 and 1 Content of Supernatant (ELISA)
2.1.5. mRNA Levels for Cartilage Matrix Proteins (Quantitative Real-Time Polymerase Chain Reaction, qRT-PCR)
2.2. Cell-Loaded PGA
2.2.1. Morphological Features
2.2.2. Content of Cartilage Matrix Proteins (Tissue)
2.2.3. Proteoglycan Content in Tissue Extracts and Culture Supernatant (DMB-Test)
2.2.4. Collagen 2 and 1 Content of Culture Supernatant (ELISA)
2.2.5. mRNA Levels for Cartilage Matrix Proteins (RT-PCR)
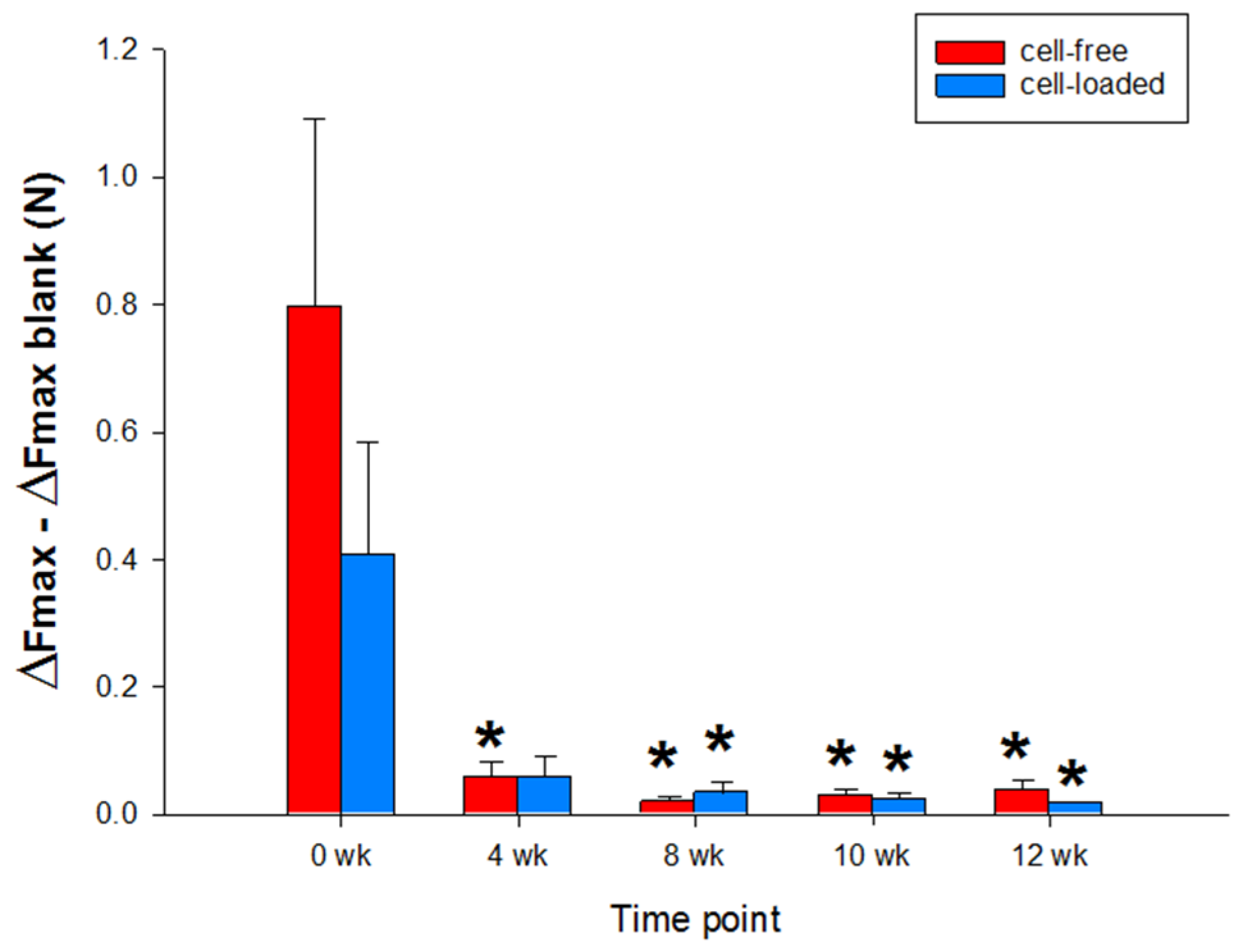
2.2.6. Push-Out Forces of Cultivated Cartilage/PGA Hybrids (Biomechanical Analyses)
3. Discussion
3.1. “Host” Cartilage Ring Performance
3.2. Cartilage Regeneration in the PGA Implants
3.2.1. Cell Colonization of the Implant
3.2.2. Local Production of Cartilage Matrix Molecules
3.2.3. De-Differentiation/Re-Differentiation of CHONDROCYTES
3.2.4. Lateral Attachment (Decreased Push-Out Forces)
4. Materials and Methods
4.1. Preparation/Culture of Bovine Cartilage with PGA
4.2. Histology and Immunohistochemistry
4.3. Cell Migration Score
4.4. Safranin O, Collagen 1, Collagen 2, and Aggrecan Score
4.5. Quantitative Real-Time Polymerase Chain Reaction
4.6. Protein Preparation
4.7. Quantification of Glycosaminoglycans
4.8. Enzyme-Linked Immunosorbent Assay
4.9. Testing of Push-Out Forces
4.10. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nii, T.; Katayama, Y. Biomaterial-Assisted Regenerative Medicine. Int. J. Mol. Sci. 2021, 22, 8657. [Google Scholar] [CrossRef]
- Qu, H.; Fu, H.; Han, Z.; Sun, Y. Biomaterials for bone tissue engineering scaffolds: A review. RSC Adv. 2019, 9, 26252–26262. [Google Scholar] [CrossRef] [Green Version]
- Nesic, D.; Whiteside, R.; Brittberg, M.; Wendt, D.; Martin, I.; Mainil-Varlet, P. Cartilage tissue engineering for degenerative joint disease. Adv. Drug. Deliv. Rev. 2006, 58, 300–322. [Google Scholar] [CrossRef]
- Kwee, B.J.; Mooney, D.J. Biomaterials for skeletal muscle tissue engineering. Curr. Opin. Biotechnol. 2017, 47, 16–22. [Google Scholar] [CrossRef]
- Nii, T.; Makino, K.; Tabata, Y. Three-Dimensional Culture System of Cancer Cells Combined with Biomaterials for Drug Screening. Cancers 2020, 12, 2754. [Google Scholar] [CrossRef] [PubMed]
- Peña, B.; Laughter, M.; Jett, S.; Rowland, T.J.; Taylor, M.R.G.; Mestroni, L.; Park, D. Injectable Hydrogels for Cardiac Tissue Engineering. Macromol. Biosci. 2018, 18, e1800079. [Google Scholar] [CrossRef]
- Reddy, M.S.B.; Ponnamma, D.; Choudhary, R.; Sadasivuni, K.K. A Comparative Review of Natural and Synthetic Biopolymer Composite Scaffolds. Polymers 2021, 13, 1105. [Google Scholar] [CrossRef] [PubMed]
- Hunziker, E.B. Articular cartilage repair: Basic science and clinical progress. A review of the current status and prospects. Osteoarthr. Cartil. 2002, 10, 432–463. [Google Scholar] [CrossRef] [Green Version]
- Musumeci, G.; Castrogiovanni, P.; Leonardi, R.; Trovato, F.M.; Szychlinska, M.A.; Di Giunta, A.; Loreto, C.; Castorina, S. New perspectives for articular cartilage repair treatment through tissue engineering: A contemporary review. World J. Orthop. 2014, 5, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Dell’Accio, F.; De Bari, C.; El Tawil, N.M.; Barone, F.; Mitsiadis, T.A.; O’Dowd, J.; Pitzalis, C. Activation of WNT and BMP signaling in adult human articular cartilage following mechanical injury. Arthritis Res. 2006, 8, R139. [Google Scholar] [CrossRef] [Green Version]
- Ye, K.; Di Bella, C.; Myers, D.E.; Choong, P.F. The osteochondral dilemma: Review of current management and future trends. ANZ J. Surg. 2014, 84, 211–217. [Google Scholar] [CrossRef]
- Bachmann, G.; Basad, E.; Lommel, D.; Steinmeyer, J. MRI in the follow-up of matrix-supported autologous chondrocyte transplantation (MACI) and microfracture. Radiologe 2004, 44, 773–782. [Google Scholar]
- Dewan, A.K.; Gibson, M.A.; Elisseeff, J.H.; Trice, M.E. Evolution of autologous chondrocyte repair and comparison to other cartilage repair techniques. BioMed Res. Int. 2014, 2014, 272481. [Google Scholar] [CrossRef]
- Gobbi, A.; Chaurasia, S.; Karnatzikos, G.; Nakamura, N. Matrix-Induced Autologous Chondrocyte Implantation versus Multipotent Stem Cells for the Treatment of Large Patellofemoral Chondral Lesions: A Nonrandomized Prospective Trial. Cartilage 2015, 6, 82–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kon, E.; Verdonk, P.; Condello, V.; Delcogliano, M.; Dhollander, A.; Filardo, G.; Pignotti, E.; Marcacci, M. Matrix-assisted autologous chondrocyte transplantation for the repair of cartilage defects of the knee: Systematic clinical data review and study quality analysis. Am. J. Sports Med. 2009, 37 (Suppl. S1), 156S–166S. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.P.; Bartlett, W.; Skinner, J.A.; Carrington, R.W.J.; Briggs, T.W.R.; Bentley, G. Collagen-covered versus matrix-induced autologous chondrocyte implantation for osteochondral defects of the knee: A comparison of tourniquet times. Eur. J. Orthop. Surg. Traumatol. 2006, 16, 315–317. [Google Scholar]
- Gillogly, S.D.; Wheeler, K.S. Autologous Chondrocyte Implantation with Collagen Membrane. Sports Med. Arthrosc. 2015, 23, 118–124. [Google Scholar] [CrossRef]
- Steinwachs, M.; Kreuz, P.C. Autologous chondrocyte implantation in chondral defects of the knee with a type I/III collagen membrane: A prospective study with a 3-year follow-up. Arthroscopy 2007, 23, 381–387. [Google Scholar] [CrossRef]
- Enea, D.; Cecconi, S.; Calcagno, S.; Busilacchi, A.; Manzotti, S.; Kaps, C.; Gigante, A. Single-stage cartilage repair in the knee with microfracture covered with a resorbable polymer-based matrix and autologous bone marrow concentrate. Knee 2013, 20, 562–569. [Google Scholar] [CrossRef]
- Erggelet, C.; Kreuz, P.C.; Mrosek, E.H.; Schagemann, J.C.; Lahm, A.; Ducommun, P.P.; Ossendorf, C. Autologous chondrocyte implantation versus ACI using 3D-bioresorbable graft for the treatment of large full-thickness cartilage lesions of the knee. Arch. Orthop. Trauma Surg. 2010, 130, 957–964. [Google Scholar] [CrossRef] [Green Version]
- Erggelet, C.; Sittinger, M.; Lahm, A. The arthroscopic implantation of autologous chondrocytes for the treatment of full-thickness cartilage defects of the knee joint. Arthroscopy 2003, 19, 108–110. [Google Scholar] [CrossRef] [Green Version]
- Kreuz, P.C.; Muller, S.; Freymann, U.; Erggelet, C.; Niemeyer, P.; Kaps, C.; Hirschmuller, A. Repair of focal cartilage defects with scaffold-assisted autologous chondrocyte grafts: Clinical and biomechanical results 48 months after transplantation. Am. J. Sports Med. 2011, 39, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Kreuz, P.C.; Muller, S.; Ossendorf, C.; Kaps, C.; Erggelet, C. Treatment of focal degenerative cartilage defects with polymer-based autologous chondrocyte grafts: Four-year clinical results. Arthritis Res. 2009, 11, R33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erggelet, C.; Endres, M.; Neumann, K.; Morawietz, L.; Ringe, J.; Haberstroh, K.; Sittinger, M.; Kaps, C. Formation of cartilage repair tissue in articular cartilage defects pretreated with microfracture and covered with cell-free polymer-based implants. J. Orthop. Res. 2009, 27, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Siclari, A.; Mascaro, G.; Gentili, C.; Kaps, C.; Cancedda, R.; Boux, E. Cartilage repair in the knee with subchondral drilling augmented with a platelet-rich plasma-immersed polymer-based implant. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1225–1234. [Google Scholar] [CrossRef]
- Siclari, A.; Mascaro, G.; Kaps, C.; Boux, E. A 5-year follow-up after cartilage repair in the knee using a platelet-rich plasma-immersed polymer-based implant. Open Orthop. J. 2014, 8, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Erggelet, C.; Neumann, K.; Endres, M.; Haberstroh, K.; Sittinger, M.; Kaps, C. Regeneration of ovine articular cartilage defects by cell-free polymer-based implants. Biomaterials 2007, 28, 5570–5580. [Google Scholar] [CrossRef]
- Peltoniemi, H.; Ashammakhi, N.; Kontio, R.; Waris, T.; Salo, A.; Lindqvist, C.; Grätz, K.; Seppänen-Kaijansinkko, R. The use of bioabsorbable osteofixation devices in craniomaxillofacial surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Horbert, V.; Foehr, P.; Kramer, F.; Udhardt, U.; Bungartz, M.; Brinkmann, O.; Burgkart, R.H.; Klemm, D.O.; Kinne, R.W. In vitro analysis of the potential cartilage implant bacterial nanocellulose using the bovine cartilage punch model. Cellulose 2019, 26, 631–645. [Google Scholar] [CrossRef]
- Horbert, V.; Boettcher, J.; Foehr, P.; Kramer, F.; Udhardt, U.; Bungartz, M.; Brinkmann, O.; Burgkart, R.H.; Klemm, D.O.; Kinne, R.W. Laser perforation and cell seeding improve bacterial nanocellulose as a potential cartilage implant in the in vitro cartilage punch model. Cellulose 2019, 26, 647–664. [Google Scholar] [CrossRef]
- Horbert, V.; Xin, L.; Foehr, P.; Brinkmann, O.; Bungartz, M.; Burgkart, R.H.; Graeve, T.; Kinne, R.W. In Vitro Analysis of Cartilage Regeneration Using a Collagen Type I Hydrogel (CaReS) in the Bovine Cartilage Punch Model. Cartilage 2019, 10, 346–363. [Google Scholar] [CrossRef] [PubMed]
- Dunzel, A.; Rudiger, T.; Pretzel, D.; Kopsch, V.; Endres, M.; Kaps, C.; Fohr, P.; Burgkart, R.H.; Linss, S.; Kinne, R.W. The bovine cartilage punch model: A tool for the in vitro analysis of biomaterials and cartilage regeneration. Orthopade 2013, 42, 254–261. [Google Scholar] [CrossRef]
- Enders, J.T.; Otto, T.J.; Peters, H.C.; Wu, J.; Hardouin, S.; Moed, B.R.; Zhang, Z. A model for studying human articular cartilage integration in vitro. J. Biomed. Mater. Res. A 2009, 94, 509–514. [Google Scholar]
- Hunter, C.J.; Levenston, M.E. Maturation and integration of tissue-engineered cartilages within an in vitro defect repair model. Tissue Eng. 2004, 10, 736–746. [Google Scholar] [CrossRef]
- Madry, H.; Zurakowski, D.; Trippel, S.B. Overexpression of human insulin-like growth factor-I promotes new tissue formation in an ex vivo model of articular chondrocyte transplantation. Gene 2001, 8, 1443–1449. [Google Scholar] [CrossRef] [Green Version]
- Obradovic, B.; Martin, I.; Padera, R.F.; Treppo, S.; Freed, L.E.; Vunjak-Novakovic, G. Integration of engineered cartilage. J. Orthop. Res. 2001, 19, 1089–1097. [Google Scholar] [CrossRef]
- Pretzel, D.; Linss, S.; Ahrem, H.; Endres, M.; Kaps, C.; Klemm, D.; Kinne, R.W. A novel in vitro bovine cartilage punch model for assessing the regeneration of focal cartilage defects with biocompatible bacterial nanocellulose. Arthritis Res. 2013, 15, R59. [Google Scholar] [CrossRef] [Green Version]
- Pretzel, D.; Pohlers, D.; Weinert, S.; Kinne, R.W. In vitro model for the analysis of synovial fibroblast-mediated degradation of intact cartilage. Arthritis Res. 2009, 11, R25. [Google Scholar] [CrossRef] [Green Version]
- Secretan, C.; Bagnall, K.M.; Jomha, N.M. Effects of introducing cultured human chondrocytes into a human articular cartilage explant model. Cell Tissue Res. 2010, 339, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Vinardell, T.; Thorpe, S.D.; Buckley, C.T.; Kelly, D.J. Chondrogenesis and integration of mesenchymal stem cells within an in vitro cartilage defect repair model. Ann. Biomed. Eng. 2009, 37, 2556–2565. [Google Scholar] [CrossRef] [PubMed]
- Endres, M.; Neumann, K.; Schroder, S.E.; Vetterlein, S.; Morawietz, L.; Ringe, J.; Sittinger, M.; Kaps, C. Human polymer-based cartilage grafts for the regeneration of articular cartilage defects. Tissue Cell 2007, 39, 293–301. [Google Scholar] [CrossRef]
- Endres, M.; Neumann, K.; Zhou, B.; Freymann, U.; Pretzel, D.; Stoffel, M.; Kinne, R.W.; Kaps, C. An ovine in vitro model for chondrocyte-based scaffold-assisted cartilage grafts. J. Orthop. Surg. Res. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrascu, J.M.; Kruger, J.P.; Boss, H.G.; Ketzmar, A.K.; Freymann, U.; Sittinger, M.; Notter, M.; Endres, M.; Kaps, C. Polyglycolic acid-hyaluronan scaffolds loaded with bone marrow-derived mesenchymal stem cells show chondrogenic differentiation in vitro and cartilage repair in the rabbit model. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1310–1320. [Google Scholar] [CrossRef] [PubMed]
- Kaps, C.; Fuchs, S.; Endres, M.; Vetterlein, S.; Krenn, V.; Perka, C.; Sittinger, M. Molecular characterization of tissue-engineered articular chondrocyte transplants based on resorbable polymer fleece. Orthopade 2004, 33, 76–85. [Google Scholar] [PubMed]
- Ossendorf, C.; Kaps, C.; Kreuz, P.C.; Burmester, G.R.; Sittinger, M.; Erggelet, C. Treatment of posttraumatic and focal osteoarthritic cartilage defects of the knee with autologous polymer-based three-dimensional chondrocyte grafts: 2-year clinical results. Arthritis Res. 2007, 9, R41. [Google Scholar] [CrossRef] [Green Version]
- Bartz, C.; Meixner, M.; Giesemann, P.; Roel, G.; Bulwin, G.C.; Smink, J.J. An ex vivo human cartilage repair model to evaluate the potency of a cartilage cell transplant. J. Transl. Med. 2016, 14, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zscharnack, M.; Krause, C.; Aust, G.; Thummler, C.; Peinemann, F.; Keller, T.; Smink, J.J.; Holland, H.; Somerson, J.S.; Knauer, J.; et al. Preclinical good laboratory practice-compliant safety study to evaluate biodistribution and tumorigenicity of a cartilage advanced therapy medicinal product (ATMP). J. Transl. Med. 2015, 13, 160. [Google Scholar] [CrossRef] [Green Version]
- Schneevoigt, J.; Fabian, C.; Leovsky, C.; Seeger, J.; Bahramsoltani, M. In Vitro Expression of the Extracellular Matrix Components Aggrecan, Collagen Types I and II by Articular Cartilage-Derived Chondrocytes. Anat. Histol. Embryol. 2017, 46, 43–50. [Google Scholar] [CrossRef]
- Zhang, M.; Meng, Q.C.; Yang, X.F.; Mu, W.D. TGF-β1/WISP1/Integrin-α interaction mediates human chondrocytes dedifferentiation. Eur. Rev. Med. Pharm. Sci. 2020, 24, 8675–8684. [Google Scholar]
- Pasold, J.; Zander, K.; Heskamp, B.; Grüttner, C.; Lüthen, F.; Tischer, T.; Jonitz-Heincke, A.; Bader, R. Positive impact of IGF-1-coupled nanoparticles on the differentiation potential of human chondrocytes cultured on collagen scaffolds. Int. J. Nanomed. 2015, 10, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Efe, T.; Theisen, C.; Fuchs-Winkelmann, S.; Stein, T.; Getgood, A.; Rominger, M.B.; Paletta, J.R.; Schofer, M.D. Cell-free collagen type I matrix for repair of cartilage defects-clinical and magnetic resonance imaging results. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1915–1922. [Google Scholar] [CrossRef] [PubMed]
- Schneider, U.; Rackwitz, L.; Andereya, S.; Siebenlist, S.; Fensky, F.; Reichert, J.; Loer, I.; Barthel, T.; Rudert, M.; Noth, U. A prospective multicenter study on the outcome of type I collagen hydrogel-based autologous chondrocyte implantation (CaReS) for the repair of articular cartilage defects in the knee. Am. J. Sports Med. 2011, 39, 2558–2565. [Google Scholar] [CrossRef] [PubMed]
- Schuttler, K.F.; Schenker, H.; Theisen, C.; Schofer, M.D.; Getgood, A.; Roessler, P.P.; Struewer, J.; Rominger, M.B.; Efe, T. Use of cell-free collagen type I matrix implants for the treatment of small cartilage defects in the knee: Clinical and magnetic resonance imaging evaluation. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1270–1276. [Google Scholar] [CrossRef]
- Chandrasekhar, S.; Esterman, M.A.; Hoffman, H.A. Microdetermination of proteoglycans and glycosaminoglycans in the presence of guanidine hydrochloride. Anal. Biochem. 1987, 161, 103–108. [Google Scholar] [CrossRef]
- Farndale, R.W.; Buttle, D.J.; Barrett, A.J. Improved quantitation and discrimination of sulphated glycosaminoglycans by use of dimethylmethylene blue. Biochim. Biophys. Acta 1986, 883, 173–177. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Upstream Primer (5′ 3′) | Downstream Primer (3′ 5′) | Product Length | Annealing Temp. | Melting Temp. |
|---|---|---|---|---|---|
| Aggrecan | CAGAGTTCAGTGGGACAGCA | AGACACCCAGCTCTCCTGAA | 193 | 60 | 84 |
| Collagen 2 | CATCTGGTTTGGAGAAACCATC | GCCCAGTTCAGGTCTCTTAG | 600 | 61 | 83 |
| Collagen 1 | AGCCAGCAGATCGAGAACAT | ACACAGGTCTCACCGGTTTC | 185 | 60 | 86 |
| Aldolase | CACCGGATTGTGGCTCCGGG | CGCCCCCGATGCAGGGATTC | 170 | 58 | 88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horbert, V.; Xin, L.; Föhr, P.; Huber, R.; Burgkart, R.H.; Kinne, R.W. In Vitro Cartilage Regeneration with a Three-Dimensional Polyglycolic Acid (PGA) Implant in a Bovine Cartilage Punch Model. Int. J. Mol. Sci. 2021, 22, 11769. https://doi.org/10.3390/ijms222111769
Horbert V, Xin L, Föhr P, Huber R, Burgkart RH, Kinne RW. In Vitro Cartilage Regeneration with a Three-Dimensional Polyglycolic Acid (PGA) Implant in a Bovine Cartilage Punch Model. International Journal of Molecular Sciences. 2021; 22(21):11769. https://doi.org/10.3390/ijms222111769
Chicago/Turabian StyleHorbert, Victoria, Long Xin, Peter Föhr, René Huber, Rainer H. Burgkart, and Raimund W. Kinne. 2021. "In Vitro Cartilage Regeneration with a Three-Dimensional Polyglycolic Acid (PGA) Implant in a Bovine Cartilage Punch Model" International Journal of Molecular Sciences 22, no. 21: 11769. https://doi.org/10.3390/ijms222111769
APA StyleHorbert, V., Xin, L., Föhr, P., Huber, R., Burgkart, R. H., & Kinne, R. W. (2021). In Vitro Cartilage Regeneration with a Three-Dimensional Polyglycolic Acid (PGA) Implant in a Bovine Cartilage Punch Model. International Journal of Molecular Sciences, 22(21), 11769. https://doi.org/10.3390/ijms222111769