
Urinary Levels of the Acrolein Conjugates of Carnosine Are Associated with Cardiovascular Disease Risk

 ,
, 
Abstract
:1. Introduction
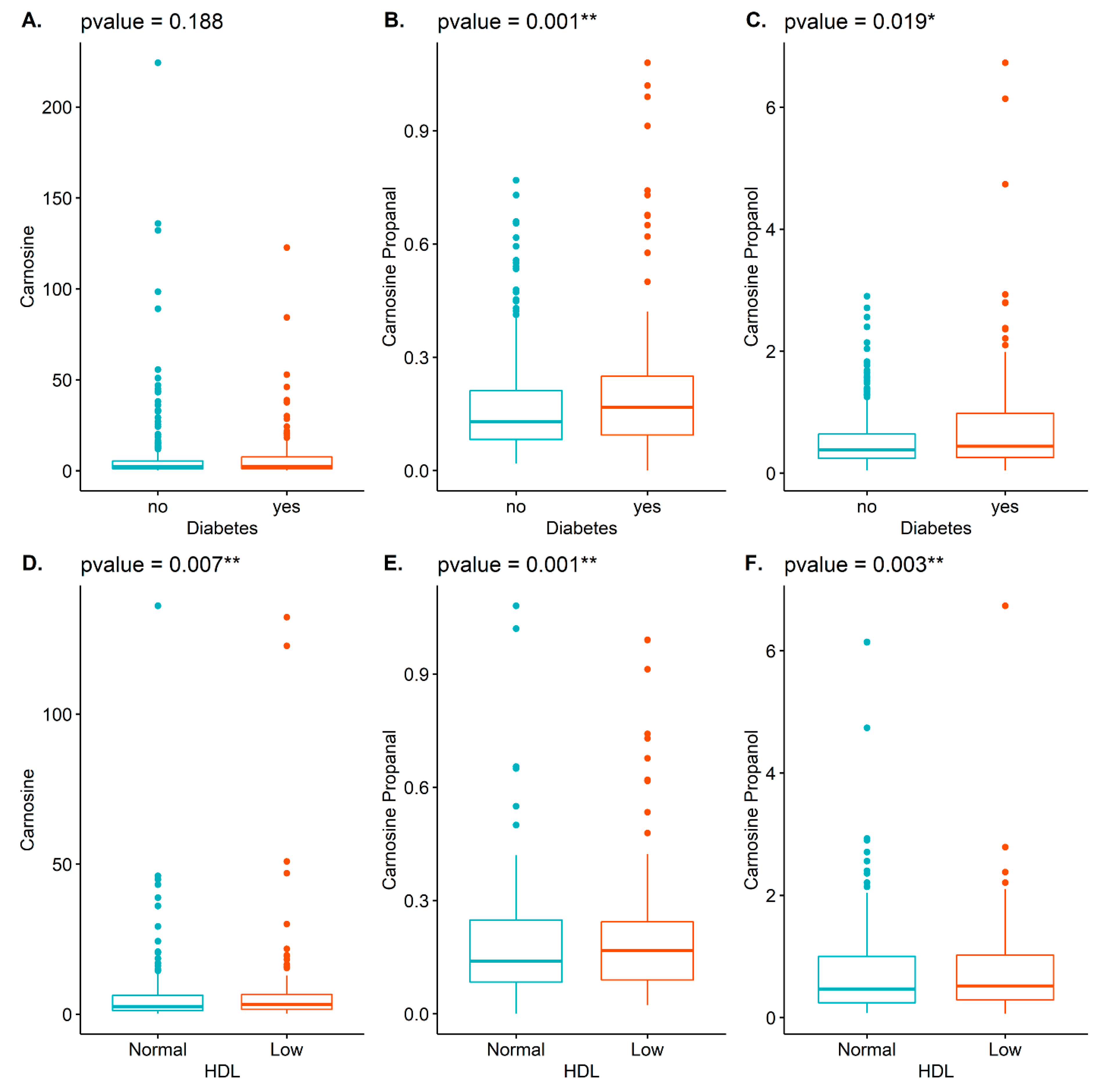
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Cohort, Characteristics, and Sample Collection
4.2. Measurement of Carnosine and Carnosine Conjugates
4.3. Biochemical Measurements
4.4. Statistical Evaluation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boldyrev, A.A.; Aldini, G.; Derave, W. Physiology and pathophysiology of carnosine. Physiol. Rev. 2013, 93, 1803–1845. [Google Scholar] [CrossRef] [PubMed]
- Aldini, G.; Facino, R.M.; Beretta, G.; Carini, M. Carnosine and related dipeptides as quenchers of reactive carbonyl species: From structural studies to therapeutic perspectives. Biofactors 2005, 24, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Aldini, G.; Carini, M.; Beretta, G.; Bradamante, S.; Facino, R.M. Carnosine is a quencher of 4-hydroxy-nonenal: Through what mechanism of reaction? Biochem. Biophys. Res. Commun. 2002, 298, 699–706. [Google Scholar] [CrossRef]
- Carini, M.; Aldini, G.; Beretta, G.; Arlandini, E.; Facino, R.M. Acrolein-sequestering ability of endogenous dipeptides: Characterization of carnosine and homocarnosine/acrolein adducts by electrospray ionization tandem mass spectrometry. J. Mass Spectrom. 2003, 38, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Eaton, P.; Li, J.M.; Hearse, D.J.; Shattock, M.J. Formation of 4-hydroxy-2-nonenal-modified proteins in ischemic rat heart. Am. J. Physiol. 1999, 276 Pt 2, H935–H943. [Google Scholar] [CrossRef] [Green Version]
- Musatov, A.; Carroll, C.A.; Liu, Y.C.; Henderson, G.I.; Weintraub, S.T.; Robinson, N.C. Identification of bovine heart cytochrome c oxidase subunits modified by the lipid peroxidation product 4-hydroxy-2-nonenal. Biochemistry 2002, 41, 8212–8220. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Dixit, B.L.; Cai, J.; Sharma, S.; Hurst, H.E.; Bhatnagar, A.; Srivastava, S.K. Metabolism of lipid peroxidation product, 4-hydroxynonenal (HNE) in rat erythrocytes: Role of aldose reductase. Free Radic. Biol. Med. 2000, 29, 642–651. [Google Scholar] [CrossRef]
- De Courten, B.; Jakubova, M.; de Courten, M.P.; Kukurova, I.J.; Vallova, S.; Krumpolec, P.; Valkovic, L.; Kurdiova, T.; Garzon, D.; Barbaresi, S.; et al. Effects of carnosine supplementation on glucose metabolism: Pilot clinical trial. Obesity 2016, 24, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Regazzoni, L.; de Courten, B.; Garzon, D.; Altomare, A.; Marinello, C.; Jakubova, M.; Vallova, S.; Krumpolec, P.; Carini, M.; Ukropec, J.; et al. A carnosine intervention study in overweight human volunteers: Bioavailability and reactive carbonyl species sequestering effect. Sci. Rep. 2016, 6, 27224. [Google Scholar] [CrossRef]
- Aldini, G.; Orioli, M.; Rossoni, G.; Savi, F.; Braidotti, P.; Vistoli, G.; Yeum, K.J.; Negrisoli, G.; Carini, M. The carbonyl scavenger carnosine ameliorates dyslipidaemia and renal function in Zucker obese rats. J. Cell. Mol. Med. 2011, 15, 1339–1354. [Google Scholar] [CrossRef]
- Ghodsi, R.; Kheirouri, S. Carnosine and advanced glycation end products: A systematic review. Amino Acids 2018, 50, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Conklin, D.J.; Guo, Y.; Zhang, X.; Obal, D.; Guo, L.; Jagatheesan, G.; Katragadda, K.; He, L.; Yin, X.; et al. Cardiospecific Overexpression of ATPGD1 (Carnosine Synthase) Increases Histidine Dipeptide Levels and Prevents Myocardial Ischemia Reperfusion Injury. J. Am. Heart Assoc. 2020, 9, e015222. [Google Scholar] [CrossRef] [PubMed]
- Barski, O.A.; Xie, Z.; Baba, S.P.; Sithu, S.D.; Agarwal, A.; Cai, J.; Bhatnagar, A.; Srivastava, S. Dietary carnosine prevents early atherosclerotic lesion formation in apolipoprotein E-null mice. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1162–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abplanalp, W.; Haberzettl, P.; Bhatnagar, A.; Conklin, D.J.; O’Toole, T.E. Carnosine Supplementation Mitigates the Deleterious Effects of Particulate Matter Exposure in Mice. J. Am. Heart Assoc. 2019, 8, e013041. [Google Scholar] [CrossRef]
- Damon, B.M.; Hsu, A.C.; Stark, H.J.; Dawson, M.J. The carnosine C-2 proton’s chemical shift reports intracellular pH in oxidative and glycolytic muscle fibers. Magn. Reson. Med. 2003, 49, 233–240. [Google Scholar] [CrossRef]
- Paynter, N.P.; Balasubramanian, R.; Giulianini, F.; Wang, D.D.; Tinker, L.F.; Gopal, S.; Deik, A.A.; Bullock, K.; Pierce, K.A.; Scott, J.; et al. Metabolic Predictors of Incident Coronary Heart Disease in Women. Circulation 2018, 137, 841–853. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Anderson, M.M.; Hazen, S.L.; Hsu, F.F.; Heinecke, J.W. Human neutrophils employ the myeloperoxidase-hydrogen peroxide-chloride system to convert hydroxy-amino acids into glycolaldehyde, 2-hydroxypropanal, and acrolein. A mechanism for the generation of highly reactive alpha-hydroxy and alpha, beta-unsaturated aldehydes by phagocytes at sites of inflammation. J. Clin. Investig. 1997, 99, 424–432. [Google Scholar]
- Uchida, K. Current status of acrolein as a lipid peroxidation product. Trends Cardiovasc. Med. 1999, 9, 109–113. [Google Scholar] [CrossRef]
- Baba, S.P.; Hoetker, J.D.; Merchant, M.; Klein, J.B.; Cai, J.; Barski, O.A.; Conklin, D.J.; Bhatnagar, A. Role of aldose reductase in the metabolism and detoxification of carnosine-acrolein conjugates. J. Biol. Chem. 2013, 288, 28163–28179. [Google Scholar] [CrossRef] [Green Version]
- Baye, E.; Ukropec, J.; de Courten, M.P.J.; Mousa, A.; Kurdiova, T.; Johnson, J.; Wilson, K.; Plebanski, M.; Aldini, G.; Ukropcova, B.; et al. Carnosine Supplementation Improves Serum Resistin Concentrations in Overweight or Obese Otherwise Healthy Adults: A Pilot Randomized Trial. Nutrients 2018, 10, 1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoetker, D.; Chung, W.; Zhang, D.; Zhao, J.; Schmidtke, V.K.; Riggs, D.W.; Derave, W.; Bhatnagar, A.; Bishop, D.J.; Baba, S.P. Exercise alters and beta-alanine combined with exercise augments histidyl dipeptide levels and scavenges lipid peroxidation products in human skeletal muscle. J. Appl. Physiol. 2018, 125, 1767–1778. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, T.E.; Li, X.; Riggs, D.W.; Hoetker, D.J.; Yeager, R.; Lorkiewicz, P.; Baba, S.P.; Cooper, N.G.F.; Bhatnagar, A. Urinary levels of the acrolein conjugates of carnosine are associated with inhaled toxicants. Inhal. Toxicol. 2020, 32, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Esterbauer, H.; Schaur, R.J.; Zollner, H. Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med 1991, 11, 81–128. [Google Scholar] [CrossRef]
- Bhatnagar, A. Cardiovascular pathophysiology of environmental pollutants. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H479–H485. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Chandra, A.; Wang, L.F.; Seifert, W.E., Jr.; DaGue, B.B.; Ansari, N.H.; Srivastava, S.K.; Bhatnagar, A. Metabolism of the lipid peroxidation product, 4-hydroxy-trans-2-nonenal, in isolated perfused rat heart. J. Biol. Chem. 1998, 273, 10893–10900. [Google Scholar] [CrossRef] [Green Version]
- Conklin, D.J.; Guo, Y.; Jagatheesan, G.; Kilfoil, P.J.; Haberzettl, P.; Hill, B.G.; Baba, S.P.; Guo, L.; Wetzelberger, K.; Obal, D.; et al. Genetic Deficiency of Glutathione S-Transferase P Increases Myocardial Sensitivity to Ischemia-Reperfusion Injury. Circ. Res. 2015, 117, 437–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barski, O.A.; Tipparaju, S.M.; Bhatnagar, A. The aldo-keto reductase superfamily and its role in drug metabolism and detoxification. Drug Metab. Rev. 2008, 40, 553–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeJarnett, N.; Conklin, D.J.; Riggs, D.W.; Myers, J.A.; O’Toole, T.E.; Hamzeh, I.; Wagner, S.; Chugh, A.; Ramos, K.S.; Srivastava, S.; et al. Acrolein exposure is associated with increased cardiovascular disease risk. J. Am. Heart Assoc. 2014, 3, e000934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiper, H.C.; Bruno, R.S.; Traber, M.G.; Stevens, J.F. Vitamin C supplementation lowers urinary levels of 4-hydroperoxy-2-nonenal metabolites in humans. Free Radic. Biol. Med. 2011, 50, 848–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Courten, B.; Kurdiova, T.; de Courten, M.P.; Belan, V.; Everaert, I.; Vician, M.; Teede, H.; Gasperikova, D.; Aldini, G.; Derave, W.; et al. Muscle Carnosine Is Associated with Cardiometabolic Risk Factors in Humans. PLoS ONE 2015, 10, e0138707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abplanalp, W.; DeJarnett, N.; Riggs, D.W.; Conklin, D.J.; McCracken, J.P.; Srivastava, S.; Xie, Z.; Rai, S.; Bhatnagar, A.; O’Toole, T.E. Benzene exposure is associated with cardiovascular disease risk. PLoS ONE 2017, 12, e0183602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Framingham Heart Study. Cardiovascular Disease (10 Year Risk). 2018. Available online: https://framinghamheartstudy.org/fhs-risk-functions/cardiovascular-disease-10-year-risk/ (accessed on 26 January 2021).
- O’Toole, T.E.; Hellmann, J.; Wheat, L.; Haberzettl, P.; Lee, J.; Conklin, D.J.; Bhatnagar, A.; Pope, C.A., 3rd. Episodic exposure to fine particulate air pollution decreases circulating levels of endothelial progenitor cells. Circ. Res. 2010, 107, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chesher, D. Evaluating assay precision. Clin. Biochem. Rev. 2008, 29 (Suppl. 1), S23–S26. [Google Scholar]


{kind=link}
| Total n = 605 | Low (0.04:0.29) n = 202 | Middle (0.30:0.58) n = 202 | High (0.59:6.73) n = 201 | p Value | |
|---|---|---|---|---|---|
| Gender ** | 0.002 | ||||
| Female | 322 (53.5) | 126 (62.7) | 106 (53.0) | 90 (44.8) | |
| Male | 280 (46.5) | 75 (37.3) | 94 (47.0) | 111 (55.2) | |
| CVD Risk Factors | |||||
| Hypertension * | 389 (69.3) | 141 (77.5) | 120 (63.5) | 128 (67.4) | 0.011 |
| High CVD risk *** | 376 (65.6) | 143 (75.3) | 103 (54.8) | 130 (66.7) | <0.001 |
| Not significant: hyperlipidemia, diabetes, obesity | |||||
| Medical History | |||||
| Heart failure * | 92 (15.5) | 43 (21.5) | 23 (11.8) | 26 (13.1) | 0.015 |
| Not significant: myocardial infarction, stroke, CBAG/PCI/stents, angina | |||||
| Medication | |||||
| ACE inhibitor * | 250 (42.4) | 92 (46.9) | 69 (35.2) | 89 (45.2) | 0.040 |
| Beta blockers * | 269 (46.1) | 106 (54.1) | 80 (41.0) | 83 (43.2) | 0.022 |
| Aspirin * | 258 (46.7) | 99 (54.7) | 74 (40.0) | 85 (46.0) | 0.014 |
| Calcium channel blockers * | 112 (19.2) | 47 (24.0) | 25 (12.9) | 40 (20.7) | 0.017 |
| Diuretics *** | 203 (34.8) | 94 (48.0) | 48 (24.7) | 61 (31.6) | < 0.001 |
| Statins * | 249 (45.2) | 89 (49.2) | 70 (37.6) | 90 (48.9) | 0.039 |
| Not significant: vasodilators | |||||
| FRS *** | 22.0 (11.1) | 24.3 (9.6) | 19.5 (11.7) | 22.2 (11.3) | < 0.001 |
| BMI ** | 32.2 (7.8) | 33.3 (8.7) | 30.7 (6.8) | 32.5 (7.8) | 0.007 |
| hsCRP (mg/L) * | 4.4 (4.6) | 5.3 (5.0) | 4.0 (4.4) | 3.9 (4.4) | 0.026 |
| HDL(mg/dL) ** | 45.3 (14.6) | 48.1 (14.7) | 47.0 (16.3) | 42.0 (12.2) | 0.007 |
| Not significant: systolic and diastolic BP, glucose, fibrinogen, platelet aggregates, cholesterol, LDL, triglycerides | |||||
| Total n = 561 | Low (0.0:0.14) n = 281 | High (0.15:1.01) n = 280 | p Value | |
|---|---|---|---|---|
| Gender *** | < 0.001 | |||
| Female | 294 (52.7) | 191(69.0) | 103 (37.2) | |
| Male | 264 (47.3) | 90 (32.0) | 174 (61.9) | |
| CVD risk factors | ||||
| Hyperlipidemia ** | 305 (55.3) | 135 (48.6) | 170 (62.0) | 0.002 |
| Diabetes ** | 158 (28.4) | 62 (22.1) | 96 (34.9) | 0.001 |
| Not significant: hypertension, obesity, high CVD risk | ||||
| Medical history | ||||
| Heart failure * | 90 (16.4) | 55 (19.6) | 35 (13.0) | 0.045 |
| Not significant: myocardial infarction, stroke, CBAG/PCI/stents, angina | ||||
| Medication | ||||
| Not significant: ACE inhibitor, beta blockers, aspirin, calcium channel blockers, diuretics, statins, vasodilators | ||||
| BMI ** | 32.2 (8.0) | 31.4 (8.2) | 33.0 (7.7) | 0.005 |
| Glucose (mg/dL) ** | 116.3 (58.4) | 112 (58.2) | 121 (58.6) | 0.003 |
| HDL (mg/dL) ** | 45.3 (14.6) | 48.1 (14.3) | 42.9 (14.5) | 0.001 |
| Not significant: FRS, systolic and diastolic BP, fibrinogen, platelet aggregates, hsCRP, cholesterol, LDL, triglycerides | ||||
| Total n = 561 | Low (0.04:0.29) n = 187 | Middle (0.30:0.58) n = 187 | High (0.59:6.73) n = 187 | p Value | |
|---|---|---|---|---|---|
| Gender *** | <0.001 | ||||
| Female | 294 (52.7) | 140 (74.9) | 84 (45.2) | 70 (37.8) | |
| Male | 264 (47.3) | 47 (25.1) | 102 (54.8) | 115 (62.2) | |
| CVD risk factors | |||||
| Diabetes * | 158 (28.4) | 49 (26.2) | 43 (23.2) | 66 (35.9) | 0.019 |
| Not significant: hypertension, hyperlipidemia, obesity, high CVD risk | |||||
| Medical history | |||||
| Not significant: myocardial infarction, stroke, CABG/PCI/stents, heart failure, angina | |||||
| Medication | |||||
| Calcium-channel blockers * | 109 (20.1) | 45 (24.9) | 26 (14.4) | 38 (20.9) | 0.045 |
| Diuretics ** | 196 (36.1) | 82 (45.3) | 54 (30.0) | 60 (33.0) | 0.006 |
| Not significant: ACE inhibitor, beta-blockers, aspirin, statins, vasodilators | |||||
| BMI * | 32.2 (8.0) | 32.0 (8.7) | 31.4 (7.5) | 33.3 (7.5) | 0.035 |
| Glucose (mg/dL) * | 116.3 (58.4) | 114 (56.3) | 117 (69.3) | 117 (45.7) | 0.030 |
| HDL (mg/dL) ** | 45.3 (14.6) | 49.6 (14.2) | 44.3 (14.4) | 43.2 (14.4) | 0.003 |
| Not significant: FRS, systolic and diastolic BP, fibrinogen, platelet aggregates, hsCRP, cholesterol, LDL, triglycerides | |||||
| Carnosine † | Carnosine-Propanal ‡ | Carnosine-Propanol † | ||||
|---|---|---|---|---|---|---|
| Independent Variables | Exponential (Coefficient) | p Value | Coefficient | p Value | Exponential (Coefficient) | p Value |
| Diabetes | 1.310 | 0.047 * | 0.057 | <0.001 *** | 1.362 | <0.001 *** |
| Age | 0.986 | 0.015 * | <−0.001 | 0.675 | 0.991 | 0.017 * |
| Female | 0.717 | 0.007 * | −0.096 | <0.001 *** | 0.624 | <0.001 *** |
| Race-Caucasian | 1.189 | 0.169 | 0.007 | 0.658 | 1.202 | 0.019 * |
| Beta Blocker | 0.752 | 0.033 * | −0.011 | 0.504 | 0.792 | 0.005 ** |
| Aspirin | 0.888 | 0.377 | −0.021 | 0.181 | 0.852 | 0.055 |
| Diuretics | 0.719 | 0.012 * | −0.003 | 0.822 | 0.884 | 0.126 |
| Current smoking | 0.848 | 0.202 | −0.011 | 0.479 | 0.838 | 0.027 * |
| Carnosine † | Carnosine-Propanal ‡ | Carnosine-Propanol † | ||||
|---|---|---|---|---|---|---|
| Independent Variables | Exponential (Coefficient) | p Value | Coefficient | p Value | Exponential (Coefficient) | p Value |
| HDL | 1.293 | 0.104 | 0.043 | 0.041 * | 1.274 | 0.026 * |
| Age | 0.987 | 0.091 | <0.001 | 0.813 | 0.997 | 0.546 |
| Female | 0.715 | 0.032 * | −0.115 | <0.001 *** | 0.615 | <0.001 *** |
| Race-Caucasian | 1.029 | 0.855 | <−0.001 | 0.997 | 1.139 | 0.221 |
| Beta Blocker | 0.766 | 0.110 | −0.011 | 0.622 | 0.815 | 0.075 |
| Aspirin | 0.867 | 0.417 | −0.023 | 0.326 | 0.736 | 0.012 * |
| Diuretics | 0.987 | 0.933 | 0.030 | 0.152 | 1.028 | 0.798 |
| Current smoking | 0.859 | 0.341 | −0.014 | 0.500 | 0.808 | 0.052 |
| Carnosine † | Carnosine-Propanal ‡ | Carnosine-Propanol † | ||||
|---|---|---|---|---|---|---|
| Independent Variables | Exponential (Coefficient) | p Value | Coefficient | p Value | Exponential (Coefficient) | p Value |
| Heart Failure | 0.794 | 0.182 | −0.029 | 0.159 | 0.803 | 0.041 * |
| Age | 0.986 | 0.017 * | <0.001 | 0.953 | 0.995 | 0.156 |
| Female | 0.727 | 0.011 * | −0.097 | <0.001 *** | 0.613 | <0.001 *** |
| Race-Caucasian | 1.170 | 0.224 | 0.009 | 0.542 | 1.246 | 0.006 ** |
| Beta Blocker | 0.792 | 0.091 | −0.003 | 0.876 | 0.834 | 0.034 ** |
| Aspirin | 0.924 | 0.563 | −0.016 | 0.313 | 0.862 | 0.080 |
| Diuretics | 0.768 | 0.064 | −0.009 | 0.586 | 0.834 | 0.041 * |
| 18 years or older; patients of University of Louisville Hospital or associated clinics |
| unwilling to sign consent; chronic lung, liver, or kidney disease; hematological disease; cancer; neurological or psychiatric illness; HIV; hepatitis; drug or substance abuse; chronic cachexia; severe coagulopathies; pregnancy; prisoners or other vulnerable populations |
| age, gender, race, medication use, current smoking |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Toole, T.E.; Li, X.; Riggs, D.W.; Hoetker, D.J.; Baba, S.P.; Bhatnagar, A. Urinary Levels of the Acrolein Conjugates of Carnosine Are Associated with Cardiovascular Disease Risk. Int. J. Mol. Sci. 2021, 22, 1383. https://doi.org/10.3390/ijms22031383
O’Toole TE, Li X, Riggs DW, Hoetker DJ, Baba SP, Bhatnagar A. Urinary Levels of the Acrolein Conjugates of Carnosine Are Associated with Cardiovascular Disease Risk. International Journal of Molecular Sciences. 2021; 22(3):1383. https://doi.org/10.3390/ijms22031383
Chicago/Turabian StyleO’Toole, Timothy E., Xiaohong Li, Daniel W. Riggs, David J. Hoetker, Shahid P. Baba, and Aruni Bhatnagar. 2021. "Urinary Levels of the Acrolein Conjugates of Carnosine Are Associated with Cardiovascular Disease Risk" International Journal of Molecular Sciences 22, no. 3: 1383. https://doi.org/10.3390/ijms22031383
APA StyleO’Toole, T. E., Li, X., Riggs, D. W., Hoetker, D. J., Baba, S. P., & Bhatnagar, A. (2021). Urinary Levels of the Acrolein Conjugates of Carnosine Are Associated with Cardiovascular Disease Risk. International Journal of Molecular Sciences, 22(3), 1383. https://doi.org/10.3390/ijms22031383