
Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review

 , , and
, , and 
Abstract
:1. Introduction
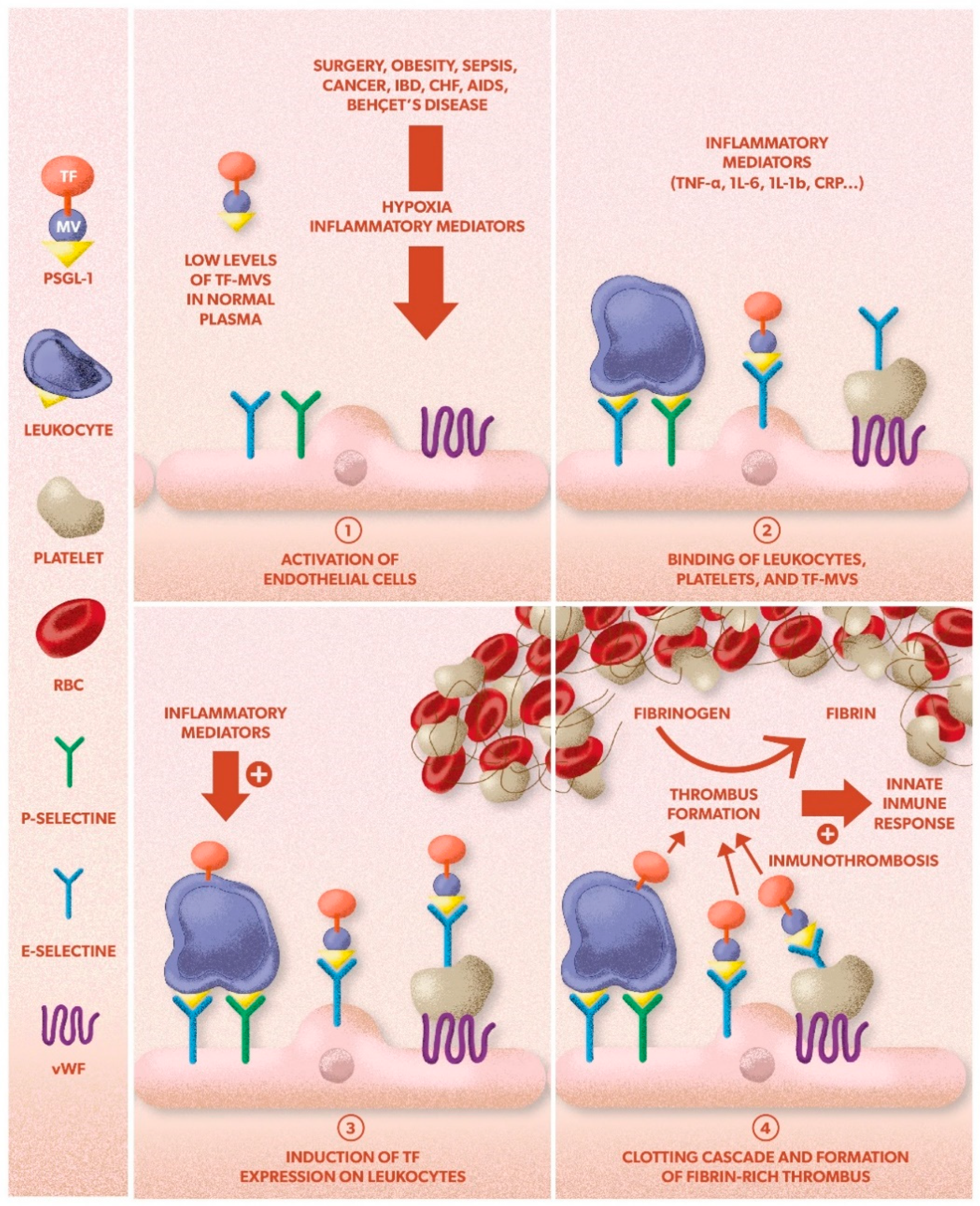
2. Inflammation in VTE
3. Inflammatory Biomarkers in VTE
3.1. C-Reactive Protein (CRP)
3.2. P-Selectin
3.3. Tissue Factor (TF) and Microparticles (MPs)
3.4. Inflammatory Cytokines
3.5. Erythrocyte Sedimentation Rate (ESR)
3.6. Fibrinogen
3.7. Leukocytes

{kind=link}
| C-reactive protein |
| |
| P-selectin | No studies have evaluated the short-term prognosis in VTE | |
| Tissue Factor-Microparticle | ||
| Inflammatory cytokines | ||
| Erythrocyte sedimentation rate | ||
| Fibrinogen |
| |
| Leukocyte count | ||
4. Prognostic Biomarkers for Bleeding Risk during Anticoagulation in VTE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ordieres-Ortega, L.; Demelo-Rodríguez, P.; Galeano-Valle, F.; Kremers, B.; Cate-Hoek, A.T.; Cate, H.T. Predictive value of D-dimer testing for the diagnosis of venous thrombosis in unusual locations: A systematic review. Thromb. Res. 2020, 189, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Bruni-Fitzgerald, K.R. Venous thromboembolism: An overview. J. Vasc. Nurs. 2015, 33, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Beckman, M.G.; Hooper, W.C.; Critchley, S.E.; Ortel, T.L. Venous thromboembolism: A public health concern. Am. J. Prev. Med. 2010, 38 (Suppl. 4), S495–S501. [Google Scholar] [CrossRef]
- Heit, J.A. Epidemiology of venous thromboembolism. Nat. Rev. Cardiol. 2015, 12, 464–474. [Google Scholar] [CrossRef]
- Peñaloza-Martínez, E.; Demelo-Rodríguez, P.; Proietti, M.; Fernández-Llamazares, G.S.; Llamazares-Mendo, C.; Walther, L.Á.-S.; Marra, A.M.; Del Toro-Cervera, J. Update on extended treatment for venous thromboembolism. Ann. Med. 2018, 50, 666–674. [Google Scholar] [CrossRef]
- Heit, J.A.; O’Fallon, W.M.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: A population-based study. Arch. Int. Med. 2002, 162, 1245–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wändell, P.; Forslund, T.; Mankowitz, H.D.; Ugarph-Morawski, A.; Eliasson, S.; Braunschwieg, F.; Holmström, M. Venous thromboembolism 2011–2018 in Stockholm: A demographic study. J. Thromb. Thrombolysis 2019, 48, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Ageno, W.; Cannegieters, S.C.; Cosmi, B.; Geersing, G.J.; Kyrle, P.A. Subcommittees on Control of Anticoagulation, and Predictive and Diagnostic Variables in Thrombotic Disease. The subcommittees on Control of Anticoagulation and Predictive and Di-agnostic Variables in Thrombotic Disease. Categorization of patients as having provoked or unprovoked VTE: Guidance from the SSC of ISTH. J. Thromb Haemost. 2016, 14, 1–4. [Google Scholar]
- Jiménez, D.; de Miguel-Díez, J.; Guijarro, R.; Trujillo-Santos, J.; Otero, R.; Barba, R.; Muriel, A.; Meyer, G.; Yusen, R.D.; RIETE Investigators; et al. Trends in the Management and Out-comes of Acute Pulmonary Embolism: Analysis from the RIETE Registry. J. Am. Coll. Cardiol. 2016, 67, 162–170. [Google Scholar]
- Demelo-Rodriguez, P.; Galeano-Valle, F.; Salzano, A.; Biskup, E.; Vriz, O.; Cittadini, A.; Falsetti, L.; Ranieri, B.; Russo, V.; Stanziola, A.A.; et al. Pulmonary Embolism: A Practical Guide for the Busy Clinician. Heart Fail Clin. 2020, 16, 317–330. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Respir. J. 2019, 54, 543–603. [Google Scholar]
- Lankeit, M.; Jiménez, D.; Kostrubiec, M.; Dellas, C.; Hasenfuss, G.; Pruszczyk, P.; Konstantinides, S. Predictive value of the high-sensitivity troponin T assay and the simplified Pulmonary Embolism Severity Index in hemodynamically stable patients with acute pulmonary embolism: A prospective validation study. Circulation 2011, 124, 2716–2724. [Google Scholar] [CrossRef] [Green Version]
- Poredos, P.; Jezovnik, M.K. The role of inflammation in venous thromboembolism and the link between arterial and venous thrombosis. Int. Angiol. 2007, 26, 306–311. [Google Scholar]
- Saghazadeh, A.; Rezaei, N. Inflammation as a cause of venous thromboembolism. Crit. Rev. Oncol. 2016, 99, 272–285. [Google Scholar] [CrossRef]
- Saghazadeh, A.; Hafizi, S.; Rezaei, N. Inflammation in venous thromboembolism: Cause or consequence? Int. Immunopharmacol. 2015, 28, 655–665. [Google Scholar] [CrossRef]
- Branchford, B.R.; Carpenter, S.L. The Role of Inflammation in Venous Thromboembolism. Front. Pediatr. 2018, 6, 142. [Google Scholar] [CrossRef]
- Vazquez-Garza, E.; Jerjes-Sanchez, C.; Navarrete, A.; Joya-Harrison, J.; Rodriguez, D. Venous thromboembolism: Thrombosis, inflammation, and immunothrombosis for clinicians. J. Thromb Thrombolysis 2017, 44, 377–385. [Google Scholar] [CrossRef]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2012, 13, 34–45. [Google Scholar] [CrossRef]
- Capodanno, D.; Angiolillo, D.J. Antithrombotic Therapy in the Elderly. J. Am. Coll. Cardiol. 2010, 56, 1683–1692. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Sahu, A.; Prabhakar, A.; Chatterjee, T.; Tyagi, T.; Kumari, B.; Khan, N.; Nair, V.; Bajaj, N.; Sharma, M.; et al. Activation of NLRP3 inflammasome complex potentiates venous thrombosis in response to hypoxia. Proc. Natl. Acad. Sci. USA 2017, 114, 4763–4768. [Google Scholar] [CrossRef] [Green Version]
- Piazza, G. Beyond Virchow’s Triad: Does cardiovascular inflammation explain the recurrent nature of venous thromboembolism? Vasc. Med. 2015, 20, 102–104. [Google Scholar] [CrossRef] [Green Version]
- Conde, I.; López, J.A. Classification of venous thromboembolism (VTE). Role of acute inflammatory stress in venous thromboembolism. J. Thromb. Haemost. 2005, 3, 2573–2575. [Google Scholar] [CrossRef]
- Osterud, B.; Olsen, J.O.; Wilsgård, L. Increased lipopolysaccharide-induced tissue factor activity and tumour necrosis factor production in monocytes after intake of aspirin: Possible role of prostaglandin E2. Blood Coagul. Fibrinolysis 1992, 3, 309–313. [Google Scholar] [PubMed]
- Cermak, J.; Key, N.S.; Bach, R.R.; Balla, J.; Jacob, H.S.; Vercellotti, G.M. C-reactive protein induces human peripheral blood monocytes to synthesize tissue factor. Blood 1993, 82, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falati, S.; Liu, Q.; Gross, P.; Merrill-Skoloff, G.; Chou, J.; Vandendries, E.; Celi, A.; Croce, K.; Furie, B.C.; Furie, B. Accumulation of tissue factor into developing thrombi in vivo is dependent upon microparticle P-selectin glycoprotein ligand 1 and platelet P-selectin. J. Exp. Med. 2003, 197, 1585–1598. [Google Scholar] [CrossRef]
- Østerud, B.; Bjørklid, E. Sources of Tissue Factor. Semin. Thromb. Hemost. 2006, 32, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Gross, P.L.; Furie, B.C.; Merrill-Skoloff, G.; Chou, J.; Furie, B. Leukocyte- versus microparticle- mediated tissue factor transfer during arterio-lar thrombus development. J. Leukoc. Biol. 2005, 78, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- López, J.A.; Kearon, C.; Lee, A.Y. Deep Venous Thrombosis. Hematology 2004, 2004, 439–456. [Google Scholar] [CrossRef] [Green Version]
- Koç¸, Y.; Güllu, I.; Akpek, G.; Akpolat, T.; Kansu, E.; Kiraz, S.; Batman, F.; Kansu, T.; Balkanci, F.; Akkaya, S. Vascular involvement in Behcet’s disease. J. Rheumatol. 1992, 19, 402–410. [Google Scholar]
- Saif, M.W.; Greenberg, B. HIV and Thrombosis: A Review. AIDS Patient Care STDs 2001, 15, 15–24. [Google Scholar] [CrossRef]
- Prandoni, P.; Piccioli, A.; Girolami, A. Cancer and venous thromboembolism: An overview. Haematology 1999, 84, 437–445. [Google Scholar]
- Abgueguen, P.; Delbos, V.; Chennebault, J.M.; Payan, C.; Pichard, E. Vascular thrombosis and acute cytomegalovirus infection in immunocompetent patients: Report of 2 cases and literature review. Clin. Infect. Dis. 2003, 36, E134–E139. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C. Epidemiology of Venous Thromboembolism. Semin. Vasc. Med. 2001, 1, 007–026. [Google Scholar] [CrossRef] [PubMed]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual frame-work. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Strimbu, K.; Tavel, J.A. What are biomarkers? Curr. Opin. HIV AIDS 2010, 5, 463–466. [Google Scholar] [CrossRef]
- Hanna, D.L.; White, R.H.; Wun, T. Biomolecular markers of cancer-associated thromboembolism. Crit. Rev. Oncol. 2013, 88, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Torres-Courchoud, I.; Pérez-Calvo, J.I. Biomarkers and clinical practice. An. Sist. Sanit. Navar. 2016, 39, 5–8. [Google Scholar] [PubMed]
- Clyne, B.; Olshaker, J.S. The C-reactive protein. J. Emerg. Med. 1999, 17, 1019–1025. [Google Scholar] [CrossRef]
- Gotschlich, E.C. C-reactive protein. A historical overview. Ann. N. Y. Acad. Sci. 1989, 557, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Kolb-Bachofen, V. A Review on the Biological Properties of C-Reactive Protein. Immunobiology 1991, 183, 133–145. [Google Scholar] [CrossRef]
- Jupe, D. The acute phase response and laboratory testing. Aust. Fam. Phys. 1996, 25, 324–329. [Google Scholar]
- Wu, Y.; Potempa, L.A.; El Kebir, D.; Filep, J.G. C-reactive protein and inflammation: Conformational changes affect function. Biol. Chem. 2015, 396, 1181–1197. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Seidu, S.; Blom, A.W.; Khunti, K.; Laukkanen, J.A. Serum C-reactive protein increases the risk of venous thromboembolism: A prospective study and meta-analysis of published prospective evidence. Eur. J. Epidemiol. 2017, 32, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.W.; Cushman, M.; Rosamond, W.D.; Heckbert, S.R.; Tracy, R.P.; Aleksic, N.; Folsom, A.R. Coagulation factors, inflammation markers, and venous thromboembolism: The longitudinal investigation of thromboembolism etiology (LITE). Am. J. Med. 2002, 113, 636–642. [Google Scholar] [CrossRef]
- Hald, E.M.; Braekkan, S.K.; Mathiesen, E.B.; Njølstad, I.; Wilsgaard, T.; Brox, J.; Hansen, J.B. High-sensitivity C-reactive protein is not a risk factor for venous thromboem-bolism: The Tromso study. Haematologica 2011, 96, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Vormittag, R.; Funk, M.; Mannhalter, C.; Schönauer, V.; Vukovich, T.; Minar, E.; Bialonczyk, C.; Hirschl, M.; Pabinger, I. C-reactive protein 30 UTR +1444C>T polymorphism in patients with spontaneous venous thromboembolism. Atherosclerosis 2006, 188, 406–411. [Google Scholar] [CrossRef]
- Nordenholz, K.E.; Mitchell, A.M.; Kline, J.A. Direct comparison of the diagnostic accuracy of fifty protein biological markers of pulmonary embolism for use in the emergency department. Acad. Emerg. Med. 2008, 15, 795–799. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.M.; Nordenholz, K.E.; Kline, J.A. Tandem Measurement of D-dimer and Myeloperoxidase or C-reactive Protein to Effectively Screen for Pulmonary Embolism in the Emergency Department. Acad. Emerg. Med. 2008, 15, 800–805. [Google Scholar] [CrossRef]
- Shen, Q.; Dong, X.; Tang, X.; Zhou, J. Risk factors and prognosis value of venous thromboembolism in patients with advanced non-small cell lung cancer: A case-control study. J. Thorac. Dis. 2017, 9, 5068–5074. [Google Scholar] [CrossRef] [Green Version]
- Horvei, L.D.; Grimnes, G.; Hindberg, K.; Mathiesen, E.B.; Njølstad, I.; Wilsgaard, T.; Brox, J.; Braekkan, S.K.; Hansen, J. C-reactive protein, obesity, and the risk of arterial and venous thrombosis. J. Thromb. Haemost. 2016, 14, 1561–1571. [Google Scholar] [CrossRef]
- Grimnes, G.; Isaksen, T.; Tichelaar, Y.I.; Brox, J.; Brækkan, S.K.; Hansen, J.B. C-reactive protein and risk of venous thromboembolism: Results from a popu-lation-based case-crossover study. Haematologica 2018, 103, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M.; O’Meara, E.S.; Heckbert, S.R.; Zakai, N.A.; Rosamond, W.; Folsom, A.R. Body size measures, hemostatic and inflammatory markers and risk of venous thrombosis: The Longitudinal Investigation of Thromboembolism Etiology. Thromb. Res. 2016, 144, 127–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchena-Yglesias, P.J.; Nieto-Rodríguez, J.A.; Serrano-Martínez, S.; Moya, O.B.; Carmona, A.C.; de Tuesta, A.D.; Alijarde, M.J.B.; Ribó, M.D.R. Acute-phase reactants and markers of inflammation in venous thromboembolic disease: Correlation with clinical and evolution parameters. An. Med. Int. 2006, 23, 105–110. [Google Scholar]
- Chung, T.; Connor, D.; Joseph, J.; Emmett, L.; Mansberg, R.; Peters, M.; Ma, D.; Kritharides, L. Platelet activation in acute pulmonary embolism. J. Thromb. Haemost. 2007, 5, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.A.; Zeitouni, R.; Marchick, M.R.; Hernandez-Nino, J.; Rose, G.A. Comparison of 8 biomarkers for prediction of right ventricular hypokinesis 6 months after submassive pulmonary embolism. Am. Heart J. 2008, 156, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Abul, Y.; Karakurt, S.; Ozben, B.; Toprak, A.; Celikel, T. C-Reactive Protein in Acute Pulmonary Embolism. J. Investig. Med. 2011, 59, 8–14. [Google Scholar] [CrossRef]
- Hogg, K.; Hinchliffe, E.; Haslam, S.; Sethi, B.; Carrier, M.; Lecky, F. Predicting short term mortality after investigation for venous thromboembolism. Thromb. Res. 2013, 131, e141–e146. [Google Scholar] [CrossRef]
- Demelo-Rodríguez, P.; Galeano-Valle, F.; Marcelo-Ayala, A.; Fernández-Carracedo, E.; Cuenca-Zarzuela, A.; Gómez-Morales, M.; Alvarez-Sala-Walther, L.A.; Bellón-Cano, J.M.; del-Toro-Cervera, J. C-reactive protein level predicts 30-day mortality and bleeding in patients with venous thromboembolism: A prospective single-center study. Med. Clin. 2020, 155, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Kanz, R.; Vukovich, T.; Vormittag, R.; Dunkler, D.; Ay, C.; Thaler, J.; Haselböck, J.; Scheithauer, W.; Zielinski, C.; Pabinger, I. Thrombosis risk and survival in cancer patients with elevated C-reactive protein. J. Thromb. Haemost. 2011, 9, 57–63. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kamphuisen, P.W.; Meyer, G.; Bauersachs, R.; Janas, M.S.; Jarner, M.F.; Lee, A.Y. Tissue factor as a predictor of recurrent venous thromboembolism in ma-lignancy: Biomarker analyses of the CATCH trial. J. Clin. Oncol. 2017, 35, 1078–1085. [Google Scholar] [CrossRef]
- Jara-Palomares, L.; Solier-Lopez, A.; Elias-Hernandez, T.; Asensio-Cruz, M.I.; Blasco-Esquivias, I.; Sanchez-Lopez, V.; De La Borbolla, M.R.; Arellano-Orden, E.; Suarez-Valdivia, L.; Marin-Romero, S.; et al. D-dimer and high-sensitivity C-reactive protein levels to predict venous thromboembolism recurrence after discontinuation of anticoagulation for cancer-associated thrombosis. Br. J. Cancer 2018, 119, 915–921. [Google Scholar] [CrossRef] [Green Version]
- Ogita, M.; Miyauchi, K.; Tsuboi, S.; Shitara, J.; Endo, H.; Wada, H.; Doi, S.; Naito, R.; Konishi, H.; Dohi, T.; et al. Impact of Combined C-Reactive Protein and High-Density Lipoprotein Cholesterol Levels on Long-Term Outcomes in Patients with Coronary Artery Disease After a First Percutaneous Coronary Intervention. Am. J. Cardiol. 2015, 116, 999–1002. [Google Scholar] [CrossRef]
- Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Porro, E.; Fanelli, G.; Maggio, M.; Meschi, T. C-reactive protein (CRP) measurement in geriatric patients hospitalized for acute infection. Eur. J. Intern. Med. 2017, 37, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Gremmel, T.; Ay, C.; Seidinger, D.; Pabinger, I.; Panzer, S.; Koppensteiner, R. Soluble p-selectin, D-dimer, and high-sensitivity C-reactive protein after acute deep vein thrombosis of the lower limb. J. Vasc. Surg. 2011, 54, 48S–55S. [Google Scholar] [CrossRef] [Green Version]
- Mrozinska, S.; Cieslik, J.; Broniatowska, E.; Malinowski, K.P.; Undas, A. Prothrombotic fibrin clot properties associated with increased endogenous thrombin potential and soluble P-selectin predict occult cancer after unprovoked venous thromboembolism. J. Thromb. Haemost. 2019, 17, 1912–1922. [Google Scholar] [CrossRef] [PubMed]
- Mosevoll, K.A.; Lindas, R.; Tvedt, T.H.; Bruserud, Ø.; Reikvam, H. Altered plasma levels of cytokines, soluble adhesion molecules and matrix metal-loproteases in venous thrombosis. Thromb. Res. 2015, 136, 30–39. [Google Scholar] [CrossRef]
- Antonopoulos, C.N.; Sfyroeras, G.S.; Kakisis, J.D.; Moulakakis, K.G.; Liapis, C.D. The role of soluble P selectin in the diagnosis of venous thromboembolism. Thromb. Res. 2014, 133, 17–24. [Google Scholar] [CrossRef]
- Schaefer, J.K.; Jacobs, B.; Wakefield, T.W.; Sood, S.L. New biomarkers and imaging approaches for the diagnosis of deep venous thrombosis. Curr. Opin. Hematol. 2017, 24, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Ramacciotti, E.; Blackburn, S.; Hawley, A.E.; Vandy, F.; Ballard-Lipka, N.; Stabler, C.; Baker, N.; Guire, K.E.; Rectenwald, J.E.; Henke, P.K.; et al. Evaluation of Soluble P-Selectin as a Marker for the Diagnosis of Deep Venous Thrombosis. Clin. Appl. Thromb. 2010, 17, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Vandy, F.C.; Stabler, C.; Eliassen, A.M.; Hawley, A.E.; Guire, K.E.; Myers, D.D.; Henke, P.K.; Wakefield, T.W. Soluble P-selectin for the diagnosis of lower extremity deep venous thrombosis. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 117–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmoamly, S.; Mattar, M.; Yacoub, M.F.; Afif, A. Can Biomarkers of Coagulation, Platelet Activation, and Inflammation Predict Venous Thromboembolism in Patients with Haematological Malignancies? Acta Haematol. 2019, 141, 245–253. [Google Scholar] [CrossRef]
- Bouman, A.; Cheung, Y.; Spronk, H.; Schalkwijk, C.; Cate, H.T.; Wolde, M.T.; Cate-Hoek, A.T. Biomarkers for post thrombotic syndrome: A case-control study. Thromb. Res. 2014, 134, 369–375. [Google Scholar] [CrossRef]
- Hoffman, M.; Monroe, D.M. Coagulation 2006: A Modern View of Hemostasis. Hematol. Clin. N. Am. 2007, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Husted, S.; Wallentin, L.; Andreotti, F.; Arnesen, H.; Bachmann, F.; Baigent, C.; Huber, K.; Jespersen, J.; Kristensen, S.D.; et al. General mechanisms of coagulation and targets of anticoagulants (Section I). Position Paper of the ESC Working Group on Thrombosis–Task Force on Anticoagulants in Heart Disease. Thromb. Haemost. 2013, 109, 569–579. [Google Scholar] [PubMed] [Green Version]
- Pabinger, I.; Thaler, J.; Ay, C. Biomarkers for prediction of venous thromboembolism in cancer. Blood 2013, 122, 2011–2018. [Google Scholar] [CrossRef] [Green Version]
- Gezelius, E.; Kristensen, A.F.; Bendahl, P.O.; Hisada, Y.; Kristensen, S.R.; Ek, L.; Bergman, B.; Wallberg, M.; Falkmer, U.; Mackman, N.; et al. Coagulation biomarkers and prediction of venous thromboembolism and survival in small cell lung cancer: A sub-study of RASTEN—A randomized trial with low molecular weight heparin. PLoS ONE 2018, 13, e0207387. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.J.; Wang, G.J.; Yang, S.; Huang, S.K.; Qiao, R.; Cui, W. Tissue Factor-bearing MPs and the risk of venous thrombosis in cancer patients: A meta-analysis. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anghel, L.; Sascău, R.; Radu, R.; Stătescu, C. From Classical Laboratory Parameters to Novel Biomarkers for the Diagnosis of Venous Thrombosis. Int. J. Mol. Sci. 2020, 21, 1920. [Google Scholar] [CrossRef] [Green Version]
- Steppich, B.A.; Hassenpflug, M.; Braun, S.L.; Schömig, K.; Beckerath, V. Ott Circulating tissue factor and microparticles are not increased in patients with deep vein thrombosis. Vasa 2011, 40, 117–122. [Google Scholar] [CrossRef]
- Ruf, W.; Mueller, B. Thrombin Generation and the Pathogenesis of Cancer. Semin. Thromb. Hemost. 2006, 32, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Beckers, M.M.; Ruven, H.J.; Haas, F.J.; Doevendans, P.A.; Ten Cate, H.; Prins, M.H.; Biesma, D.H. Single nucleotide polymorphisms in inflammation-related genesare associated with venous thromboembolism. Eur. J. Int. Med. 2010, 21, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Kerr, R.; Stirling, D.; Ludlam, C.A. Interleukin 6 and Haemostasis. Br. J. Haematol. 2001, 115, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Van Aken, B.; Reitsma, P.; Rosendaal, F. Interleukin 8 and venous trombosis evidence for a role of inflamation in trombosis. Br. J. Haematol. 2002, 116, 173–177. [Google Scholar] [CrossRef]
- Vormittag, R.; Hsieh, K.; Kaider, A.; Minar, E.; Bialonczyk, C.; Hirschl, M.; Mannhalter, C. Interleukin-6 and interleukin-6 promoter polymorphism (−174) GNC in patients with spontaneous venous thromboembolism. Thromb. Haemost. 2006, 95, 802–806. [Google Scholar] [CrossRef]
- Downing, L.J.; Strieter, R.M.; Kadell, A.M.; Wilke, C.A.; Austin, J.C.; Hare, B.D.; Burdick, M.D.; Greenfield, L.J.; Wakefield, T.W. IL-10 regulates thrombus-induced vein wall inflammation and thrombosis. J. Immunol. 1998, 161, 1471–1476. [Google Scholar] [PubMed]
- Budnik, I.; Brill, A. Immune Factors in Deep Vein Thrombosis Initiation. Trends Immunol. 2018, 39, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Reitter, E.M.; Ay, C.; Kaider, A.; Pirker, R.; Zielinski, C.; Zlabinger, G.; Pabinger, I. Interleukin levels and their potential association with venous thromboembolism and survival in cancer patients. Clin. Exp. Immunol. 2014, 177, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Shbaklo, H.; Holcroft, C.A.; Kahn, S.R. Levels of inflammatory markers and the development of the post-thrombotic syndrome. Thromb. Haemost. 2009, 101, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Maruna, P.; Kunstyr, J.; Plocova, K.M.; Mlejnsky, F.; Hubacek, J.; Klein, A.A.; Lindner, J. Predictors of infection after pulmonary endarterectomy for chronic throm-bo-embolic pulmonary hypertension. Eur. J. Cardiothorac. Surg. 2011, 39, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Van Aken, B.E.; den Heijer, M.; Bos, G.M.; van Deventer, S.J.; Reitsma, P.H. Recurrent venous thrombosis and markers of inflammation. Thromb. Haemost. 2000, 83, 536–539. [Google Scholar] [CrossRef]
- Deodar, S. C-reactive protein: The best laboratory indicator available for monitoring disease activity. Cleve. Clin. J. Med. 1989, 56, 126–130. [Google Scholar]
- Krieger, E.; van Der Loo, B.; Amann-Vesti, B.R.; Rousson, V.; Koppensteiner, R. C-reactive protein and red cell aggregation correlate with late venous function after acute deep venous thrombosis. J. Vasc. Surg. 2004, 40, 644–649. [Google Scholar] [CrossRef] [Green Version]
- Luxembourg, B.; Schmitt, J.; Humpich, M.; Glowatzki, M.; Dressler, D.; Seifried, E.; Lindhoff-Last, E. Cardiovascular risk factors in idiopathic compared to risk-associated venous thromboembolism: A focus on fibrinogen, factor VIII, and high-sensitivity C-reactive protein (hs-CRP). Thromb. Haemost. 2009, 102, 668–675. [Google Scholar] [PubMed]
- Lin, C.; Chen, Y.; Chen, B.; Zheng, K.; Luo, X.; Lin, F. D-Dimer Combined with Fibrinogen Predicts the Risk of Venous Thrombosis in Fracture Patients. Emerg. Med. Int. 2020, 2020, 1930405. [Google Scholar] [CrossRef]
- Wang, T.-F.; Wong, C.A.; Milligan, P.E.; Thoelke, M.S.; Woeltje, K.F.; Gage, B.F. Risk factors for inpatient venous thromboembolism despite thromboprophylaxis. Thromb. Res. 2014, 133, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blix, K.; Jensvoll, H.; Brækkan, S.K.; Hansen, J.-B. White Blood Cell Count Measured Prior to Cancer Development Is Associated with Future Risk of Venous Thromboembolism—The Tromsø Study. PLoS ONE 2013, 8, e73447. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Meng, X.; Feng, J.; Zhou, X.; Zhu, H. Hypereosinophilia with Concurrent Venous Thromboembolism: Clinical Features, Potential Risk Factors, and Short-term Outcomes in a Chinese Cohort. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Wypasek, E.; Padjas, A.; Szymańska, M.; Plens, K.; Siedlar, M.; Undas, A. Non-classical and intermediate monocytes in patients following venous throm-boembolism: Links with inflammation. Adv. Clin. Exp. Med. 2019, 28, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Kushnir, M.; Cohen, H.W.; Billett, H.H. Persistent neutrophilia is a marker for an increased risk of venous thrombosis. J. Thromb. Thrombolysis 2016, 42, 545–551. [Google Scholar] [CrossRef]
- Artoni, A.; Abbattista, M.; Bucciarelli, P.; Gianniello, F.; Scalambrino, E.; Pappalardo, E.; Peyvandi, F.; Martinelli, I. Platelet to Lymphocyte Ratio and Neutrophil to Lymphocyte Ratio as Risk Fac-tors for Venous Thrombosis. Clin. Appl. Thromb. Hemost. 2018, 24, 808–814. [Google Scholar] [CrossRef] [Green Version]
- Morillo, R.; Jiménez, D.; Aibar, M.Á.; Mastroiacovo, D.; Wells, P.S.; Sampériz, Á.; Saraiva de Sousa, M.; Muriel, A.; Yusen, R.D.; Monreal, M.; et al. DVT Management and Outcome Trends, 2001 to 2014. Chest 2016, 150, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Huisman, M.V. How I assess and manage the risk of bleeding in patients treated for venous thromboembolism. Blood 2020, 135, 724–734. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Akl, E.A.; Comerota, A.J.; Prandoni, P.; Bounameaux, H.; Goldhaber, S.Z.; Nelson, M.E.; Wells, P.S.; Gould, M.K.; Dentali, F.; et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. 2), e419S–e496S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]

| Biomarkers | Role in the Pathophysiology of VTE |
|---|---|
| C-reactive protein | Its production is stimulated by cytokines. It modulates innate immunity. |
| P-selectin | Cell adhesion molecule present in platelets and endothelial cells. It mediates the binding of platelets and endothelial cells with leukocytes and the transfer of TF to platelets and triggers the formation of leukocyte-derived microparticles. |
| Microparticles | Small membranous vesicles, released from the plasma membranes of platelets, leukocytes, red cells, and endothelial cells. They play an important role in the initiation and propagation of VTE through the development of their own procoagulant properties, enhancing intercellular communication and promoting inflammation. |
| Interleukins | Released by leukocytes, endothelial cells, and other cell types that promote inflammation, they influence endothelial function and the expression of TF. |
| Fibrinogen | Induces thrombus formation through platelet activation. |
| Leukocytes | They can keep the thrombi attached to the vessel wall. Leukocyte-derived particles were found to be related to increased thrombus formation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galeano-Valle, F.; Ordieres-Ortega, L.; Oblitas, C.M.; del-Toro-Cervera, J.; Alvarez-Sala-Walther, L.; Demelo-Rodríguez, P. Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review. Int. J. Mol. Sci. 2021, 22, 2627. https://doi.org/10.3390/ijms22052627
Galeano-Valle F, Ordieres-Ortega L, Oblitas CM, del-Toro-Cervera J, Alvarez-Sala-Walther L, Demelo-Rodríguez P. Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review. International Journal of Molecular Sciences. 2021; 22(5):2627. https://doi.org/10.3390/ijms22052627
Chicago/Turabian StyleGaleano-Valle, Francisco, Lucía Ordieres-Ortega, Crhistian Mario Oblitas, Jorge del-Toro-Cervera, Luis Alvarez-Sala-Walther, and Pablo Demelo-Rodríguez. 2021. "Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review" International Journal of Molecular Sciences 22, no. 5: 2627. https://doi.org/10.3390/ijms22052627
APA StyleGaleano-Valle, F., Ordieres-Ortega, L., Oblitas, C. M., del-Toro-Cervera, J., Alvarez-Sala-Walther, L., & Demelo-Rodríguez, P. (2021). Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review. International Journal of Molecular Sciences, 22(5), 2627. https://doi.org/10.3390/ijms22052627