
Argon Attenuates Multiorgan Failure in Relation with HMGB1 Inhibition

 , , ,
, , ,  and
and 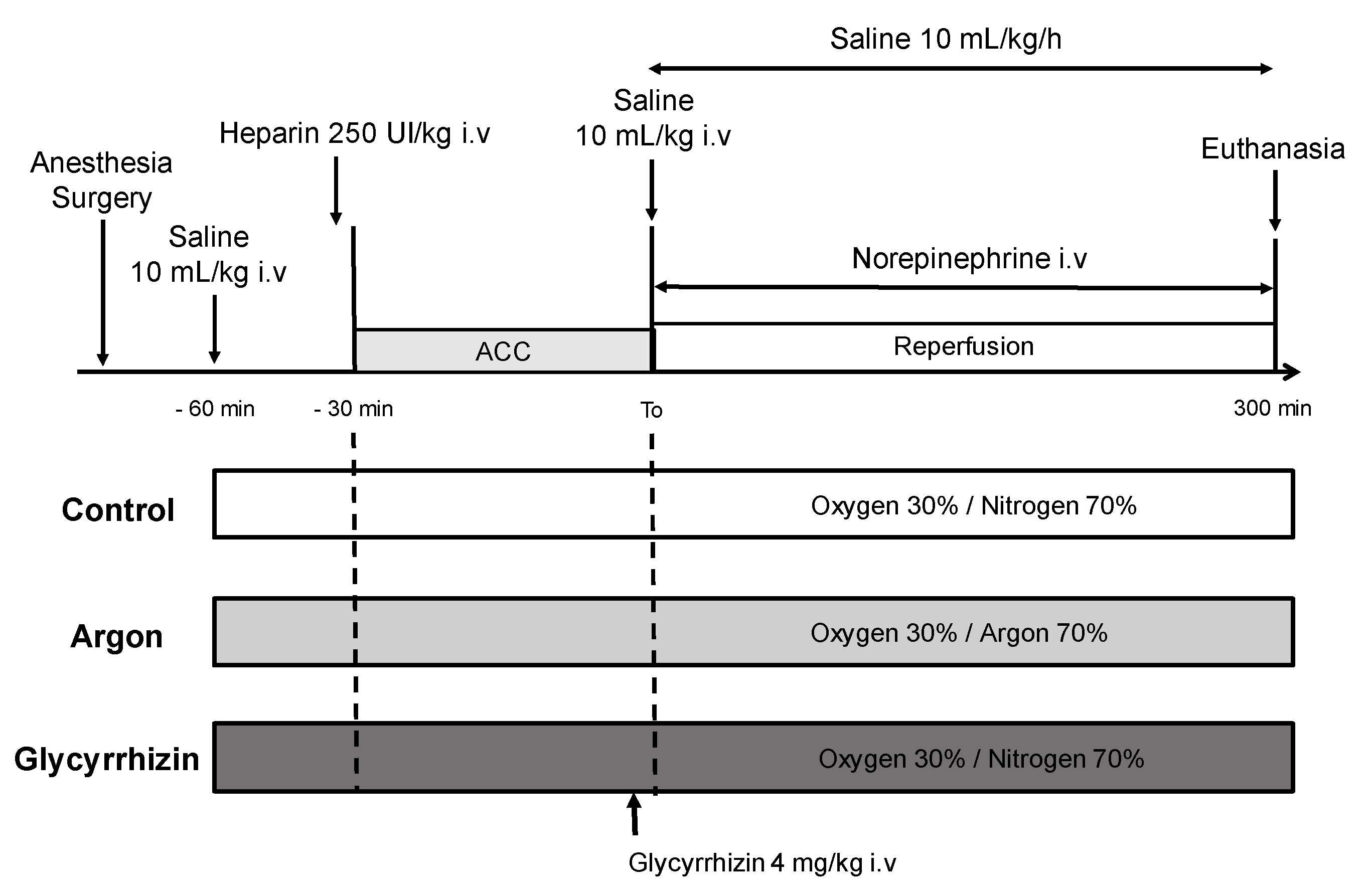{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
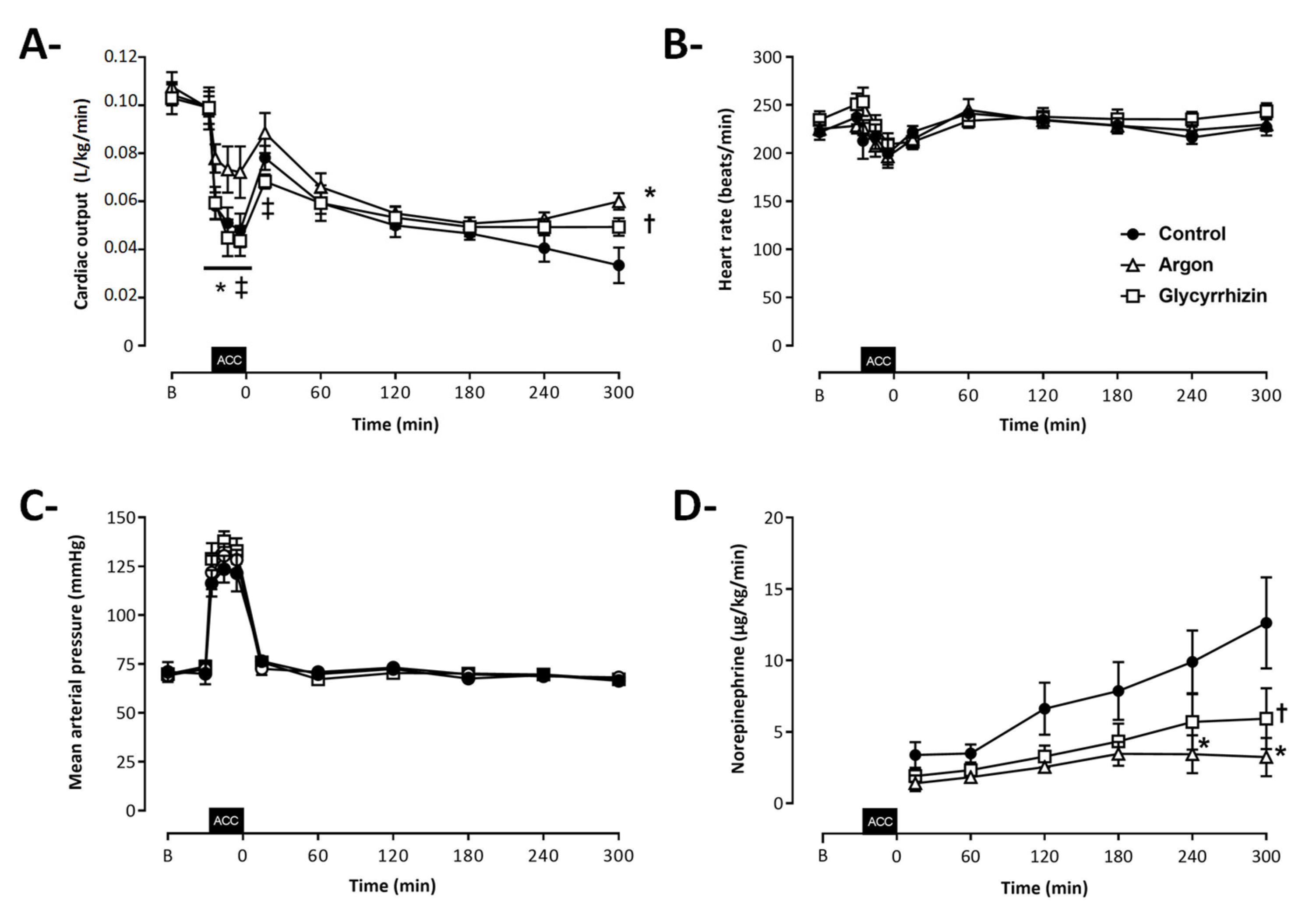
2.1. Hemodynamic Parameters
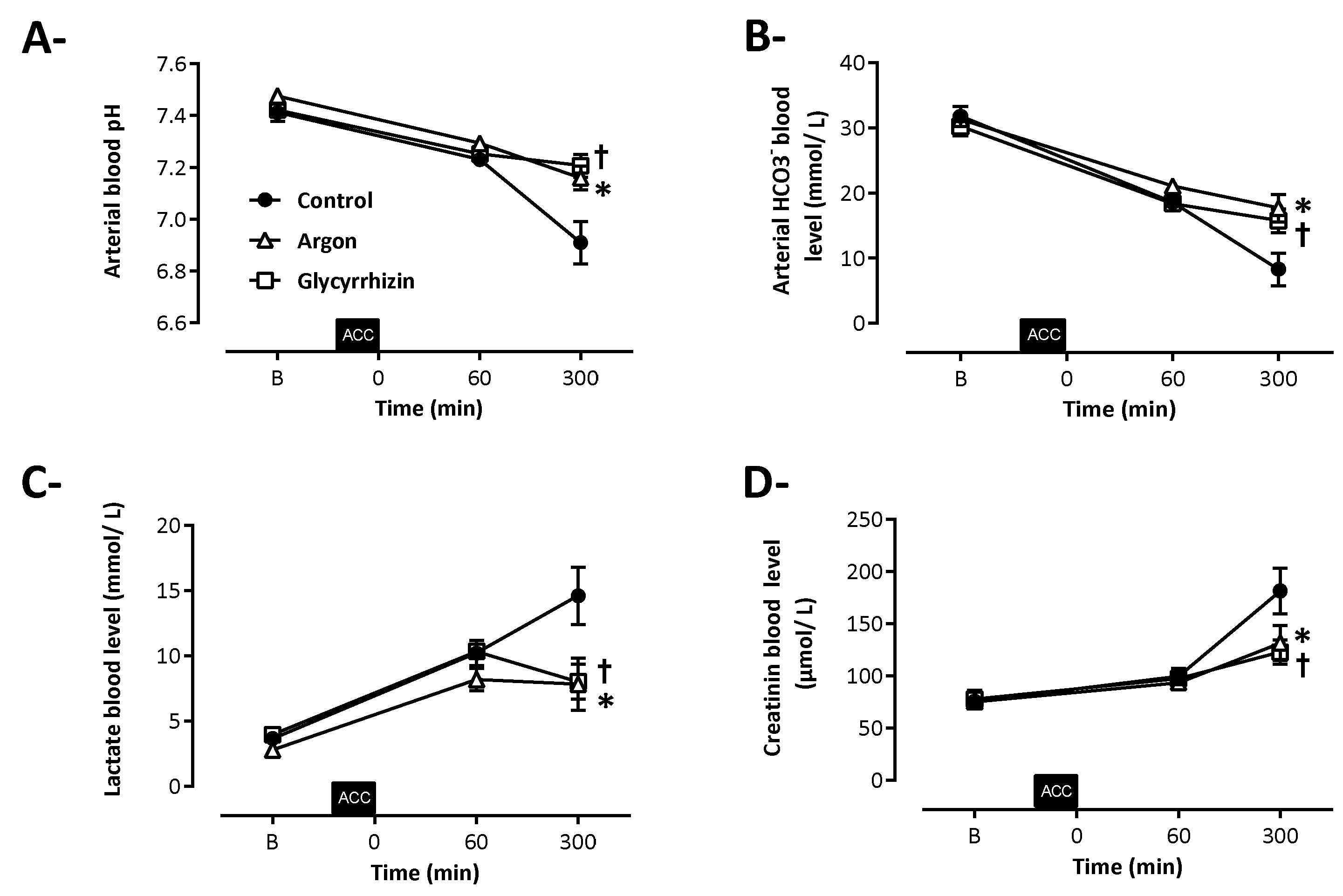
2.2. Biochemical Alterations of Shock
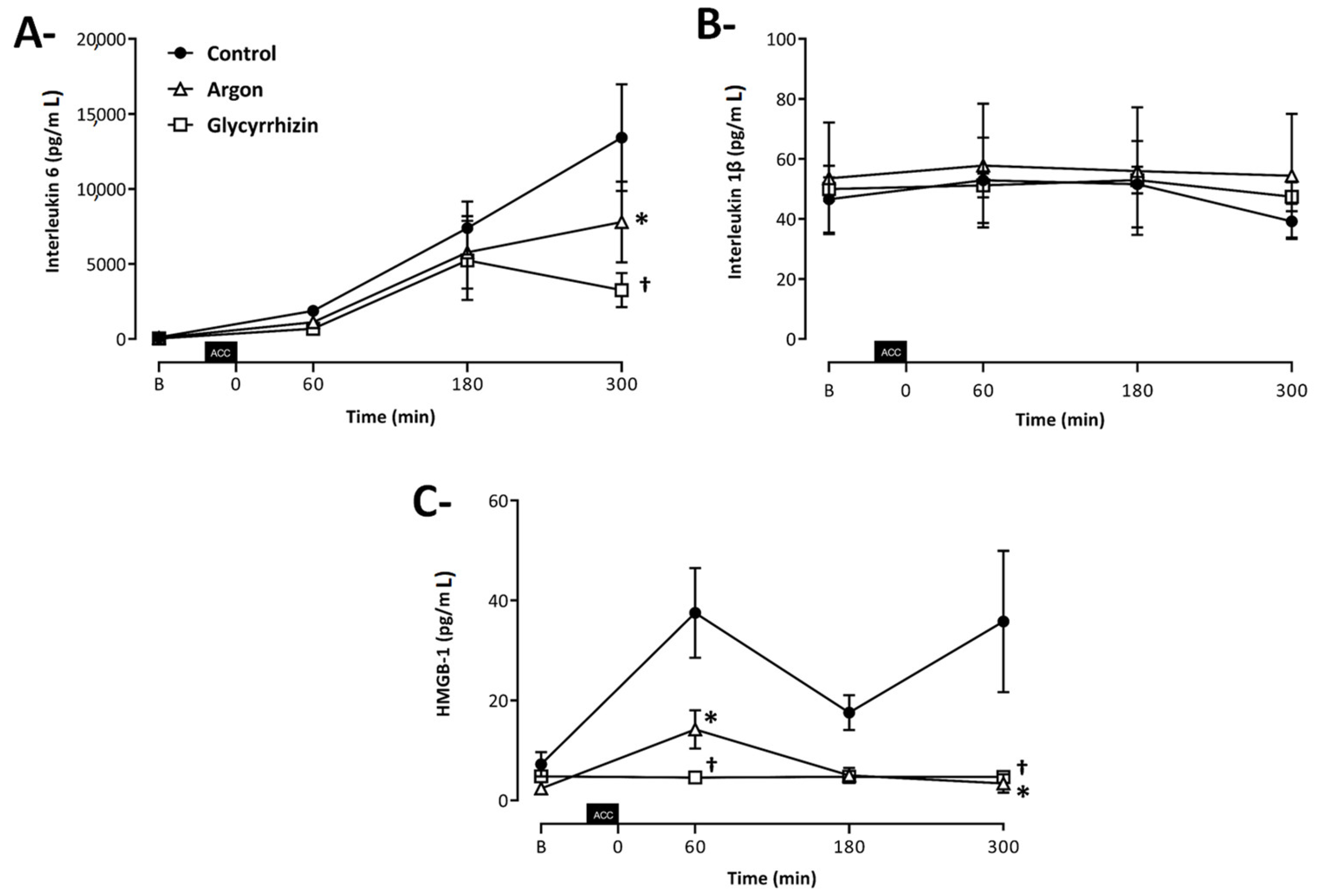
2.3. Cytokine Blood Levels
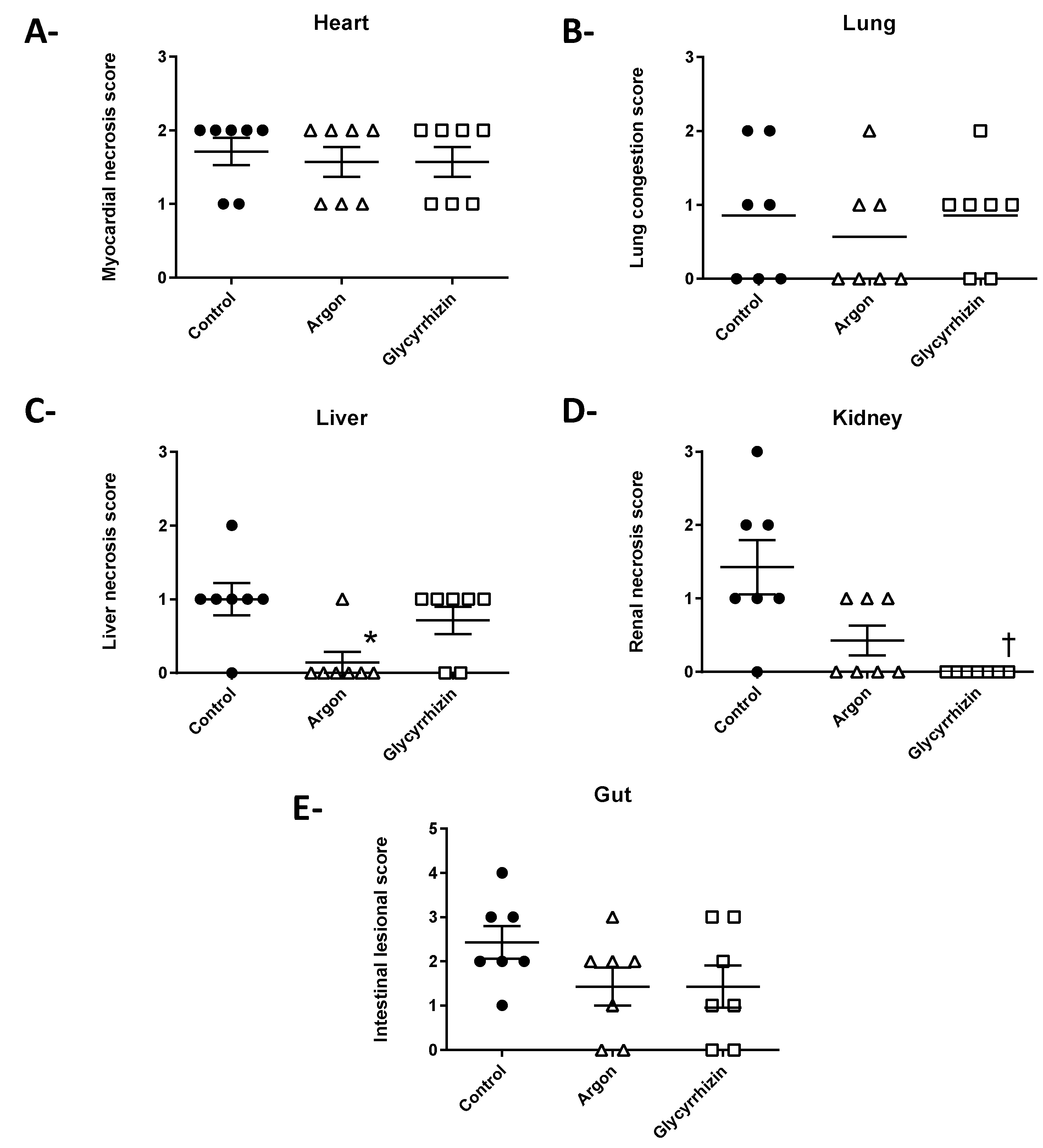
2.4. Histopathological Evaluation
2.5. Immunohistochemistry
3. Discussion
4. Materials and Methods
4.1. Animal Preparation
4.2. Protocol of Aortic Cross-Clamping
4.3. Experimental Protocol
4.4. Immuno–Assay and Histology
4.5. Statistical Analysis
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mongardon, N.; Dyson, A.; Singer, M. Is MOF an Outcome Parameter or a Transient, Adaptive State in Critical Illness? Curr. Opin. Crit. Care 2009, 15, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Savary, G.; Lidouren, F.; Rambaud, J.; Kohlhauer, M.; Hauet, T.; Bruneval, P.; Costes, B.; Cariou, A.; Ghaleh, B.; Mongardon, N.; et al. Argon Attenuates Multiorgan Failure Following Experimental Aortic Cross–Clamping. Br. J. Clin. Pharmacol. 2018, 84, 1170–1179. [Google Scholar] [CrossRef] [Green Version]
- Nespoli, F.; Redaelli, S.; Ruggeri, L.; Fumagalli, F.; Olivari, D.; Ristagno, G. A Complete Review of Preclinical and Clinical Uses of the Noble Gas Argon: Evidence of Safety and Protection. Ann. Card. Anaesth. 2019, 22, 122. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, D.; Robertson, N.J.; Bainbridge, A.; Cady, E.; Charles–Edwards, G.; Deierl, A.; Fagiolo, G.; Franks, N.P.; Griffiths, J.; Hajnal, J.; et al. Moderate Hypothermia within 6 h of Birth plus Inhaled Xenon versus Moderate Hypothermia Alone after Birth Asphyxia (TOBY–Xe): A Proof–of–Concept, Open–Label, Randomised Controlled Trial. Lancet Neurol. 2016, 15, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Ryang, Y.–M.; Fahlenkamp, A.V.; Rossaint, R.; Wesp, D.; Loetscher, P.D.; Beyer, C.; Coburn, M. Neuroprotective Effects of Argon in an in Vivo Model of Transient Middle Cerebral Artery Occlusion in Rats. Crit. Care Med. 2011, 39, 1448–1453. [Google Scholar] [CrossRef]
- Lemoine, S.; Blanchart, K.; Souplis, M.; Lemaitre, A.; Legallois, D.; Coulbault, L.; Simard, C.; Allouche, S.; Abraini, J.H.; Hanouz, J.–L.; et al. Argon Exposure Induces Postconditioning in Myocardial Ischemia–Reperfusion. J. Cardiovasc. Pharmacol. Ther. 2017, 22, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Chu, D.; Li, L.; Creed, J.A.; Ryang, Y.–M.; Sheng, H.; Yang, W.; Warner, D.S.; Turner, D.A.; Hoffmann, U. Argon Inhalation for 24 Hours After Onset of Permanent Focal Cerebral Ischemia in Rats Provides Neuroprotection and Improves Neurologic Outcome. Crit. Care Med. 2019, 47, e693–e699. [Google Scholar] [CrossRef] [PubMed]
- Goebel, U.; Scheid, S.; Spassov, S.; Schallner, N.; Wollborn, J.; Buerkle, H.; Ulbrich, F. Argon Reduces Microglial Activation and Inflammatory Cytokine Expression in Retinal Ischemia/Reperfusion Injury. Neural. Regen. Res. 2021, 16, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, F.; Olivari, D.; Boccardo, A.; De Giorgio, D.; Affatato, R.; Ceriani, S.; Bariselli, S.; Sala, G.; Cucino, A.; Zani, D.; et al. Ventilation with Argon Improves Survival With Good Neurological Recovery After Prolonged Untreated Cardiac Arrest in Pigs. J. Am. Heart. Assoc. 2020, 9, e016494. [Google Scholar] [CrossRef] [PubMed]
- Brücken, A.; Kurnaz, P.; Bleilevens, C.; Derwall, M.; Weis, J.; Nolte, K.; Rossaint, R.; Fries, M. Delayed Argon Administration Provides Robust Protection against Cardiac Arrest–Induced Neurological Damage. Neurocrit. Care 2015, 22, 112–120. [Google Scholar] [CrossRef]
- Ulbrich, F.; Goebel, U. The Molecular Pathway of Argon–Mediated Neuroprotection. Int. J. Mol. Sci. 2016, 17, 1816. [Google Scholar] [CrossRef] [Green Version]
- Fahlenkamp, A.V.; Rossaint, R.; Haase, H.; Al Kassam, H.; Ryang, Y.–M.; Beyer, C.; Coburn, M. The Noble Gas Argon Modifies Extracellular Signal–Regulated Kinase 1/2 Signaling in Neurons and Glial Cells. Eur. J. Pharmacol. 2012, 674, 104–111. [Google Scholar] [CrossRef]
- Zhuang, L.; Yang, T.; Zhao, H.; Fidalgo, A.R.; Vizcaychipi, M.P.; Sanders, R.D.; Yu, B.; Takata, M.; Johnson, M.R.; Ma, D. The Protective Profile of Argon, Helium, and Xenon in a Model of Neonatal Asphyxia in Rats. Crit. Care Med. 2012, 40, 1724. [Google Scholar] [CrossRef] [Green Version]
- Ulbrich, F.; Kaufmann, K.; Roesslein, M.; Wellner, F.; Auwärter, V.; Kempf, J.; Loop, T.; Buerkle, H.; Goebel, U. Argon Mediates Anti–Apoptotic Signaling and Neuroprotection via Inhibition of Toll–Like Receptor 2 and 4. PLoS ONE 2015, 10, e0143887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaffidi, P.; Misteli, T.; Bianchi, M.E. Release of Chromatin Protein HMGB1 by Necrotic Cells Triggers Inflammation. Nature 2002, 418, 191–195. [Google Scholar] [CrossRef]
- Kiss, A.; Shu, H.; Hamza, O.; Santer, D.; Tretter, E.V.; Yao, S.; Markstaller, K.; Hallström, S.; Podesser, B.K.; Klein, K.U. Argon Preconditioning Enhances Postischaemic Cardiac Functional Recovery Following Cardioplegic Arrest and Global Cold Ischaemia. Eur. J. Cardiothorac. Surg. 2018, 54, 539–546. [Google Scholar] [CrossRef]
- Ogiku, M.; Kono, H.; Hara, M.; Tsuchiya, M.; Fujii, H. Glycyrrhizin Prevents Liver Injury by Inhibition of High–Mobility Group Box 1 Production by Kupffer Cells after Ischemia–Reperfusion in Rats. J. Pharmacol. Exp. Ther. 2011, 339, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Wang, X.; Li, J.; Chen, S. Protective Effect of Glycyrrhizin on Myocardial Ischemia/Reperfusion Injury–Induced Oxidative Stress, Inducible Nitric Oxide Synthase and Inflammatory Reactions through High–Mobility Group Box 1 and Mitogen–Activated Protein Kinase Expression. Exp. Ther. Med. 2017, 14, 1219–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, S.; Ma, M.; Fei, X.; Zhang, Y.; Gong, F.; Fang, M. Glycyrrhizin Attenuates Hepatic Ischemia–Reperfusion Injury by Suppressing HMGB1–Dependent GSDMD–Mediated Kupffer Cells Pyroptosis. Int. Immunopharmac. 2019, 68, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Suleiman, S.; Klassen, S.; Katz, I.; Balakirski, G.; Krabbe, J.; von Stillfried, S.; Kintsler, S.; Braunschweig, T.; Babendreyer, A.; Spillner, J.; et al. Argon Reduces the Pulmonary Vascular Tone in Rats and Humans by GABA–Receptor Activation. Sci. Rep. 2019, 9, 1902. [Google Scholar] [CrossRef] [PubMed]
- Spaggiari, S.; Kepp, O.; Rello–Varona, S.; Chaba, K.; Adjemian, S.; Pype, J.; Galluzzi, L.; Lemaire, M.; Kroemer, G. Antiapoptotic Activity of Argon and Xenon. Cell Cycle 2013, 12, 2636–2642. [Google Scholar] [CrossRef] [Green Version]
- Mollica, L.; De Marchis, F.; Spitaleri, A.; Dallacosta, C.; Pennacchini, D.; Zamai, M.; Agresti, A.; Trisciuoglio, L.; Musco, G.; Bianchi, M.E. Glycyrrhizin Binds to High–Mobility Group Box 1 Protein and Inhibits Its Cytokine Activities. Chem. Biol. 2007, 14, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Ni, B.; Cao, Z.; Liu, Y. Glycyrrhizin Protects Spinal Cord and Reduces Inflammation in Spinal Cord Ischemia–Reperfusion Injury. Int. J. Neurosci. 2013, 123, 745–751. [Google Scholar] [CrossRef]
- Musumeci, D.; Roviello, G.N.; Montesarchio, D. An Overview on HMGB1 Inhibitors as Potential Therapeutic Agents in HMGB1–Related Pathologies. Pharmacol. Ther. 2014, 141, 347–357. [Google Scholar] [CrossRef]
- Kageyama, Y.; Suzuki, H.; Saruta, T. Glycyrrhizin Induces Mineralocorticoid Activity through Alterations in Cortisol Metabolism in the Human Kidney. J. Endocrinol. 1992, 135, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Chen, Z.; Chen, J.–Z.; Pei, L.–G.; Xie, J.; Wei, Z.–H.; Kang, L.–N.; Wang, L.; Xu, B. High Mobility Group B–1 (HMGB–1) Promotes Apoptosis of Macrophage–Derived Foam Cells by Inducing Endoplasmic Reticulum Stress. Cell Physiol. Biochem. 2018, 48, 1019–1029. [Google Scholar] [CrossRef]
- Boissady, E.; Kohlhauer, M.; Lidouren, F.; Hocini, H.; Lefebvre, C.; Chateau–Jouber, S.; Mongardon, N.; Deye, N.; Cariou, A.; Micheau, P.; et al. Ultrafast Hypothermia Selectively Mitigates the Early Humoral Response After Cardiac Arrest. J. Am. Heart Assoc. 2020, 9, e017413. [Google Scholar] [CrossRef] [PubMed]
- Katseni, K.; Chalkias, A.; Kaparos, G.; Iacovidou, N.; Logothetis, E.; Dafnios, N.; Kotsis, T.; Karvouni, E.; Arapoglou, V. The effects of n–acetylcysteine and desferoxamine on IL–6, TNF–a, and oxLDL after infrarenal aortic clamping. Hellenic J. Surg. 2015, 87, 407–414. [Google Scholar] [CrossRef]
- Mongardon, N.; Kohlhauer, M.; Lidouren, F.; Hauet, T.; Giraud, S.; Hutin, A.; Costes, B.; Barau, C.; Bruneval, P.; Micheau, P.; et al. A Brief Period of Hypothermia Induced by Total Liquid Ventilation Decreases End–Organ Damage and Multiorgan Failure Induced by Aortic Cross–Clamping. Anesth. Analg. 2016, 123, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Gong, G.; Xiang, L.; Yuan, L.; Hu, L.; Wu, W.; Cai, L.; Yin, L.; Dong, H. Protective Effect of Glycyrrhizin, a Direct HMGB1 Inhibitor, on Focal Cerebral Ischemia/Reperfusion–Induced Inflammation, Oxidative Stress, and Apoptosis in Rats. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Roux, Q.; Lidouren, F.; Kudela, A.; Slassi, L.; Kohlhauer, M.; Boissady, E.; Chalopin, M.; Farjot, G.; Billoet, C.; Bruneval, P.; et al. Argon Attenuates Multiorgan Failure in Relation with HMGB1 Inhibition. Int. J. Mol. Sci. 2021, 22, 3257. https://doi.org/10.3390/ijms22063257
de Roux Q, Lidouren F, Kudela A, Slassi L, Kohlhauer M, Boissady E, Chalopin M, Farjot G, Billoet C, Bruneval P, et al. Argon Attenuates Multiorgan Failure in Relation with HMGB1 Inhibition. International Journal of Molecular Sciences. 2021; 22(6):3257. https://doi.org/10.3390/ijms22063257
Chicago/Turabian Stylede Roux, Quentin, Fanny Lidouren, Agathe Kudela, Lina Slassi, Matthias Kohlhauer, Emilie Boissady, Matthieu Chalopin, Géraldine Farjot, Catherine Billoet, Patrick Bruneval, and et al. 2021. "Argon Attenuates Multiorgan Failure in Relation with HMGB1 Inhibition" International Journal of Molecular Sciences 22, no. 6: 3257. https://doi.org/10.3390/ijms22063257
APA Stylede Roux, Q., Lidouren, F., Kudela, A., Slassi, L., Kohlhauer, M., Boissady, E., Chalopin, M., Farjot, G., Billoet, C., Bruneval, P., Ghaleh, B., Mongardon, N., & Tissier, R. (2021). Argon Attenuates Multiorgan Failure in Relation with HMGB1 Inhibition. International Journal of Molecular Sciences, 22(6), 3257. https://doi.org/10.3390/ijms22063257