
Recent Advances in Anticoagulant Treatment of Immune Thrombosis: A Focus on Direct Oral Anticoagulants in Heparin-Induced Thrombocytopenia and Anti-Phospholipid Syndrome


 , ,
, , 
Abstract
:1. Introduction
2. Differences and Similarities between HIT and APS
3. HIT: Diagnosis and Standard of Care
4. HIT: Update on DOACs Use
5. APS: Diagnosis and Standard of Care
6. APS: Update on DOACs’ Use
6.1. DOACs’ Therapeutic Use in APS
6.2. Interferences of DOACs with Lupus Anticoagulant Diagnosis
7. Up-to-Date Data on Vaccine-Induced Thrombotic Thrombocytopenia (VITT): A New Context of Immune Thrombosis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Van Es, N.; Coppens, M.; Schulman, S.; Middeldorp, S.; Büller, H.R. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: Evidence from phase 3 trials. Blood 2014, 124, 1968–1975. [Google Scholar] [CrossRef]
- Gruel, Y.; De Maistre, E.; Pouplard, C.; Mullier, F.; Susen, S.; Roullet, S.; Blais, N.; Le Gal, G.; Vincentelli, A.; Lasne, D.; et al. Diagnosis and management of heparin-induced thrombocytopenia. Anaesth. Crit. Care Pain Med. 2020, 39, 291–310. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derkesen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
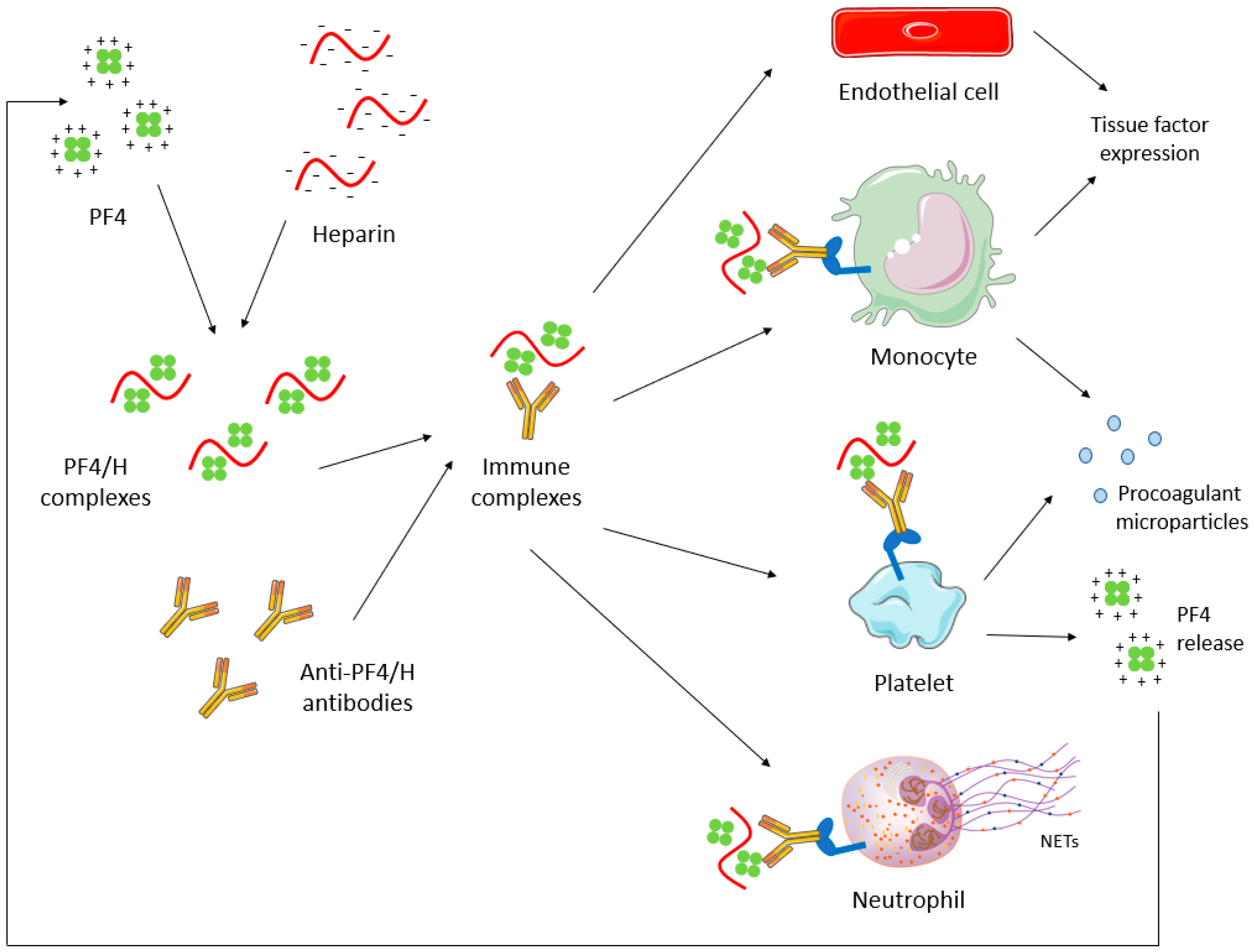
- Arepally, G.M.; Cines, D.B. Pathogenesis of heparin-induced thrombocytopenia. Transl. Res. 2020, 225, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R. Antiphospholipid syndrome. Thromb. Res. 2017, 151, S43–S47. [Google Scholar] [CrossRef]
- Cohen, H.; Hunt, B.J.; Efthymiou, M.; Arachchillage, D.R.J.; Mackie, I.J.; Clawson, S.; Sylvestre, Y.; Machin, S.J.; Bertolaccini, M.L.; Ruiz-Castellano, M.; et al. Rivaroxaban versus warfarin to treat patients with thrombotic antiphospholipid syndrome, with or without systemic lupus erythematosus (RAPS): A randomised, controlled, open-label, phase 2/3, non-inferiority trial. Lancet Haematol. 2016, 3, e426–e436. [Google Scholar] [CrossRef] [Green Version]
- Pengo, V.; Denas, G.; Zoppellaro, G.; Jose, S.P.; Hoxha, A.; Ruffatti, A.; Andreoli, L.; Tincani, A.; Cenci, C.; Prisco, D.; et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood 2018, 132, 1365–1371. [Google Scholar] [CrossRef]
- Ordi-Ros, J.; Sáez-Comet, L.; Pérez-Conesa, M.; Vidal, X.; Riera-Mestre, A.; Castro-Salomó, A.; Cuquet-Pedragosa, J.; Ortiz-Santamaria, V.; Mauri-Plana, M.; Solé, C.; et al. Rivaroxaban versus Vitamin K antagonist in antiphospholipid syndrome a randomized noninferiority trial. Ann. Intern. Med. 2019, 171, 685. [Google Scholar] [CrossRef]
- Woller, S.C.; Stevens, S.M.; Kaplan, D.; Wang, T.-F.; Branch, D.W.; Groat, D.; Wilson, E.L.; Armbruster, B.; Aston, V.T.; Lloyd, J.F.; et al. Apixaban compared with warfarin to prevent thrombosis in thrombotic antiphospholipid syndrome: A randomized trial. Blood Adv. 2021. [Google Scholar] [CrossRef]
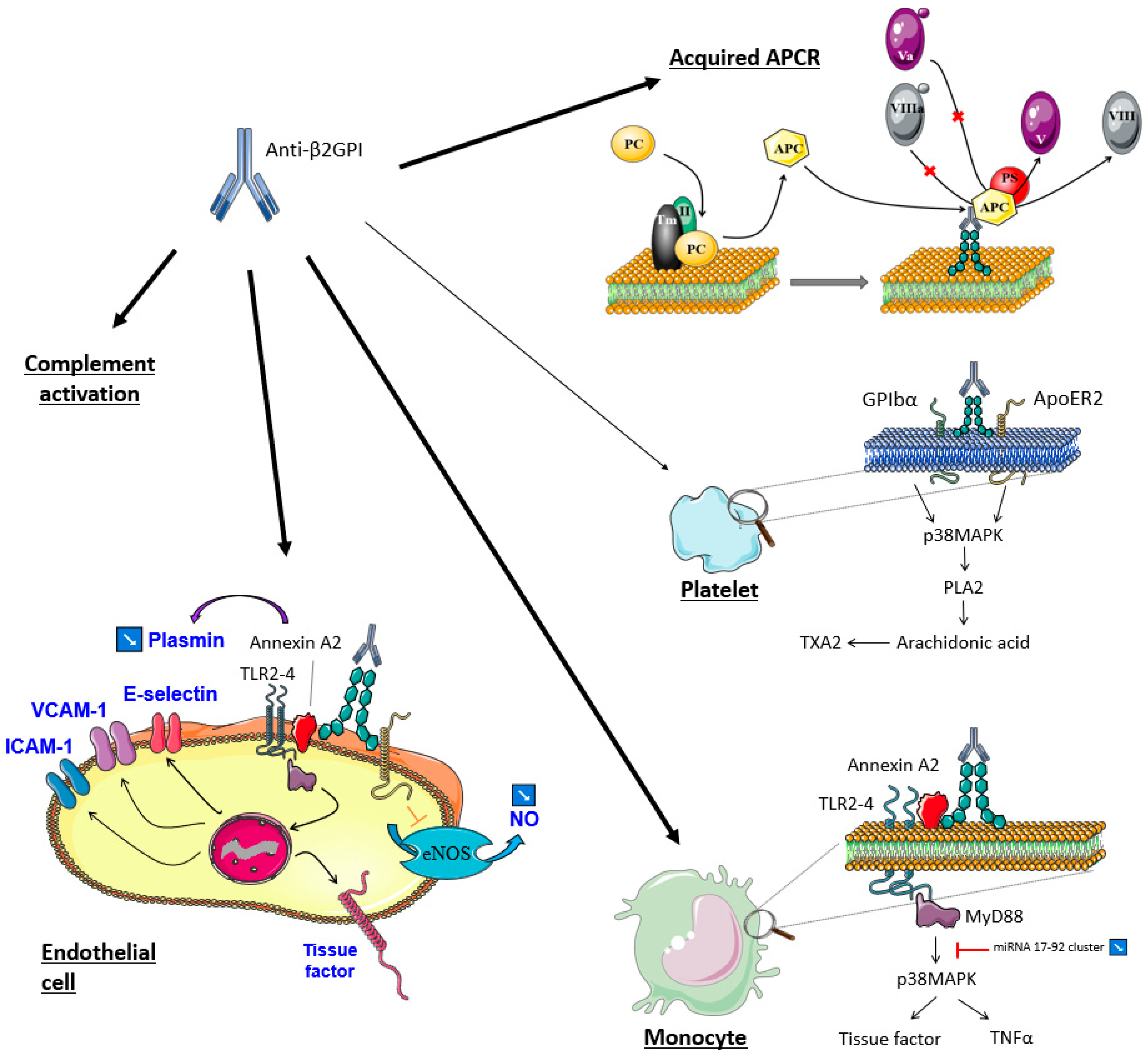
- Aǧar, Ç.; Van Os, G.M.A.; Mörgelin, M.; Sprenger, R.R.; Marquart, J.A.; Urbanus, R.T.; Derksen, R.H.W.M.; Meijers, J.C.M.; De Groot, P.G. β2-Glycoprotein I can exist in 2 conformations: Implications for our understanding of the antiphospholipid syndrome. Blood 2010, 116, 1336–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ZZhang, W.; Gao, F.; Lu, D.; Sun, N.; Yin, X.; Jin, M.; Liu, Y. Anti-β2 glycoprotein I antibodies in complex with β2 glycoprotein I induce platelet activation via two receptors: Apolipoprotein E receptor 2′ and glycoprotein I bα. Front. Med. 2016, 10, 76–84. [Google Scholar] [CrossRef]
- Pennings, M.T.T.; Derksen, R.H.W.M.; Van Lummel, M.; Adelmeijer, J.; Vanhoorelbeke, K.; Urbanus, R.T.; Lisman, T.; De Groot, P.G. Platelet adhesion to dimeric β2-glycoprotein I under conditions of flow is mediated by at least two receptors: Glycoprotein Ib α and apolipoprotein E receptor 2′. J. Thromb. Haemost. 2007, 5, 369–377. [Google Scholar] [CrossRef]
- Lellouche, F.; Martinuzzo, M.; Said, P.; Maclouf, J.; Carreras, L.O. Imbalance of Thromboxane/Prostacyclin Biosynthesis in Patients with Lupus Anticoagulant. Blood 1991, 78, 2894–2899. [Google Scholar] [CrossRef] [Green Version]
- Masliah-Planchon, J.; Darnige, L. Anticorps antiphospholipides et hémostase. La Rev. Médecine Interne 2012, 33, 181–188. [Google Scholar] [CrossRef]
- Greinacher, A. Heparin-Induced Thrombocytopenia. Solomon CG, éditeur. N. Engl. J. Med. 2015, 373, 252–261. [Google Scholar] [CrossRef]
- Tektonidou, M.G.; Andreoli, L.; Limper, M.; Amoura, Z.; Cervera, R.; Costedoat-Chalumeau, N.; Cuadrado, M.J.; Dörner, T.; Ferrer-Oliveras, R.; Hambly, K.; et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann. Rheum. Dis. 2019, 78, 1296–1304. [Google Scholar] [CrossRef]
- Cervera, R.; Piette, J.C.; Font, J.; Khamashta, M.A.; Shoenfeld, Y.; Camps, M.T.; Jacobsen, S.; Lakos, G.; Tincani, A.; Kontopoulou-Griva, I.; et al. Antiphospholipid syndrome: Clinical and immunologic manifestations and patterns of disease expression in a cohort of 1000 patients. Arthritis Rheum. 2002, 46, 1019–1027. [Google Scholar] [CrossRef]
- Godeau, B.; Piette, J.-C.; Fromont, P.; Intrator, L.; Schaeffer, A.; Bierling, P. Specific anti-platelet glycoprotein autoantibodies are associated with the thrombocytopenia of primary antiphospholipid syndrome. Br. J. Haematol. 1997, 98, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Macchi, L.; Rispal, P.; Clofent-Sanchez, G.; Pellegrin, J.L.; Nurden, P.; Leng, B.; Nurden, A.T. Anti-platelet antibodies in patients with systemic lupus erythematosus and the primary antiphospholipid antibody syndrome: Their relationship with the observed thrombocytopenia. Br. J. Haematol. 1997, 98, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Pardos-Gea, J.; Marques-Soares, J.R.; Buján, S.; Ordi-Ros, J.; Alijotas-Reig, J. Persistent thrombocytopenia predicts poor long-term survival in patients with antiphospholipid syndrome: A 38-year follow-up study. Rheumatology 2021, keab475. [Google Scholar] [CrossRef] [PubMed]
- Chayoua, W.; Nicolson, P.L.R.; Meijers, J.C.M.; Kardeby, C.; Garcia-Quintanilla, L.; Devreese, K.M.J.; de Laat, B.; Watson, S.P.; de Groot, P.G. Antiprothrombin antibodies induce platelet activation: A possible explanation for anti-FXa therapy failure in patients with antiphospholipid syndrome? J. Thromb. Haemost. 2021, 19, 1776–1782. [Google Scholar] [CrossRef]
- Kotyla, P.J.; Islam, M.A. MicroRNA (miRNA): A New Dimension in the Pathogenesis of Antiphospholipid Syndrome (APS). Int. J. Mol. Sci. 2020, 21, 2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, G.K.; Juhl, D.; Warkentin, T.E.; Sigouin, C.S.; Eichler, P.; Greinacher, A. Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings. J. Thromb. Haemost. 2006, 4, 759–765. [Google Scholar] [CrossRef]
- Nagler, M.; Bachmann, L.M.; ten Cate, H.; ten Cate-Hoek, A. Diagnostic value of immunoassays for heparin-induced thrombocytopenia: A systematic review and meta-analysis. Blood 2016, 127, 546–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuker, A.; Arepally, G.M.; Chong, B.H.; Cines, D.B.; Greinacher, A.; Gruel, Y.; Linkins, L.A.; Rodner, S.B.; Selleng, S.; Warkentin, T.E.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Heparin-induced thrombocytopenia. Blood Adv. 2018, 2, 3360–3392. [Google Scholar] [CrossRef] [Green Version]
- Warkentin, T.E.; Arnold, D.M.; Nazi, I.; Kelton, J.G. The platelet serotonin-release assay. Am. J. Hematol. 2015, 90, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Michels, I.; Kiefel, V.; Mueller-Eckhardt, C. A rapid and sensitive test for diagnosing heparin-associated thrombocytopenia. Thromb. Haemost. 1991, 66, 734–736. [Google Scholar] [CrossRef] [PubMed]
- Gonthier, M.-C.; Gendron, N.; Eloy, P.; Bourrienne, M.-C.; Alhenc-Gelas, M.; Pouplard, C.; Tardy, B.; Szymezak, J.; Burdet, C.; Gkalea, V.; et al. Heparin-induced Thrombocytopenia Diagnosis: A Retrospective Study Comparing Heparin-induced Platelet Activation Test to 14C-serotonin Release Assay. TH Open 2021, 5, e507–e512. [Google Scholar] [CrossRef]
- Tardy, B.; Lecompte, T.; Mullier, F.; Vayne, C.; Pouplard, C. Detection of Platelet-Activating Antibodies Associated with Heparin-Induced Thrombocytopenia. J. Clin. Med. 2020, 9, 1226. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Ashoorion, V.; Cuker, A.; Begum, H.; Ross, S.; Martinez, N.; Chong, B.H.; Linkins, L.A.; Warkentin, T.E.; Wiercioch, W.; et al. Management of heparin-induced thrombocytopenia: Systematic reviews and meta-analyses. Blood Adv. 2020, 4, 5184–5193. [Google Scholar] [CrossRef]
- Linkins, L.-A.; Dans, A.L.; Moores, L.K.; Bona, R.; Davidson, B.L.; Schulman, S.; Crowther, M. Treatment and Prevention of Heparin-Induced Thrombocytopenia. Chest 2012, 141 (Suppl. 2), e495S–e530S. [Google Scholar] [CrossRef] [Green Version]
- Watson, H.; Davidson, S.; Keeling, D. Guidelines on the diagnosis and management of heparin-induced thrombocytopenia: Second edition. Br. J. Haematol. 2012, 159, 528–540. [Google Scholar] [CrossRef]
- Krauel, K.; Hackbarth, C.; Fürll, B.; Greinacher, A. Heparin-induced thrombocytopenia: In vitro studies on the interaction of dabigatran, rivaroxaban, and low-sulfated heparin, with platelet factor 4 and anti-PF4/heparin antibodies. Blood 2012, 119, 1248–1255. [Google Scholar] [CrossRef] [Green Version]
- Carré, J.; Guérineau, H.; Le Beller, C.; Mauge, L.; Huynh, B.; Nili, R.; Planquette, B.; Clauser, S.; Smadja, D.M.; Helley, D.; et al. Direct Oral Anticoagulants as Successful Treatment of Heparin-Induced Thrombocytopenia: A Parisian Retrospective Case Series. Front. Med. 2021, 8, 1239. [Google Scholar] [CrossRef]
- Davis, K.A.; Davis, D.O. Direct acting oral anticoagulants for the treatment of suspected heparin-induced thrombocytopenia. Eur. J. Haematol. 2017, 99, 332–335. [Google Scholar] [CrossRef]
- Ong, S.Y.; Chin, Y.A.; Than, H.; Tan, C.W.; Yap, E.S.; Wong, W.H.; Ng, H.J. Rivaroxaban for heparin-induced thrombocytopenia: Adding to the evidence. Ann. Hematol. 2017, 96, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Nilius, H.; Kaufmann, J.; Cuker, A.; Nagler, M. Comparative effectiveness and safety of anticoagulants for the treatment of heparin-induced thrombocytopenia. Am. J. Hematol. 2021, 96, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Barlow, A.; Barlow, B.; Reinaker, T.; Harris, J. Potential Role of Direct Oral Anticoagulants in the Management of Heparin-induced Thrombocytopenia. Pharmacotherapy 2019, 39, 837–853. [Google Scholar] [CrossRef]
- Linkins, L.A.; Warkentin, T.E.; Pai, M.; Shivakumar, S.; Manji, R.A.; Wells, P.S.; Wu, C.; Nazi, I.; Crowther, M.A. Rivaroxaban for treatment of suspected or confirmed heparin-induced thrombocytopenia study. J. Thromb. Haemost. 2016, 14, 1206–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warkentin, T.E.; Pai, M.; Linkins, L.-A. Direct oral anticoagulants for treatment of HIT: Update of Hamilton experience and literature review. Blood 2017, 130, 1104–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauzner, R.; Greinacher, A.; Selleng, K.; Althaus, K.; Shenkman, B.; Seligsohn, U. False-positive tests for heparin-induced thrombocytopenia in patients with antiphospholipid syndrome and systemic lupus erythematosus. J. Thromb. Haemost. 2009, 7, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Gruel, Y.; Rupin, A.; Watier, H.; Vigier, S.; Bardos, P.; Leroy, J. Anticardiolipin antibodies in heparin-associated thrombocytopenia. Thromb. Res. 1992, 67, 601–606. [Google Scholar] [CrossRef]
- Arnaud, L.; Mathian, A.; Ruffatti, A.; Erkan, D.; Tektonidou, M.; Cervera, R.; Forastiero, R.; Pengo, V.; Lambert, M.; Martinez-Zamora, M.A.; et al. Efficacy of aspirin for the primary prevention of thrombosis in patients with antiphospholipid antibodies: An international and collaborative meta-analysis. Autoimmun. Rev. 2014, 13, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Crowther, M.A.; Ginsberg, J.S.; Julian, J.; Denburg, J.; Hirsh, J.; Douketis, J.; Laskin, C.; Fortin, P.; Anderson, D.; Kearon, C.; et al. A Comparison of Two Intensities of Warfarin for the Prevention of Recurrent Thrombosis in Patients with the Antiphospholipid Antibody Syndrome. N. Engl. J. Med. 2003, 349, 1133–1138. [Google Scholar] [CrossRef]
- Tripodi, A.; de Laat, B.; Wahl, D.; Ageno, W.; Cosmi, B.; Crowther, M. Monitoring patients with the lupus anticoagulant while treated with vitamin K antagonists: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2016, 14, 2304–2307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Irastorza, G.; Hunt, B.J.; Khamashta, M.A. A systematic review of secondary thromboprophylaxis in patients with antiphospholipid antibodies. Arthritis Care Res. 2007, 57, 1487–1495. [Google Scholar] [CrossRef]
- Pengo, V.; Hoxha, A.; Andreoli, L.; Tincani, A.; Silvestri, E.; Prisco, D.; Fierro, T.; Gresele, P.; Cafolla, A.; De Micheli, V.; et al. Trial of Rivaroxaban in AntiPhospholipid Syndrome (TRAPS): Two-year outcomes after the study closure. J. Thromb. Haemost. 2021, 19, 531–535. [Google Scholar] [CrossRef]
- Zuily, S.; Cohen, H.; Isenberg, D.; Woller, S.C.; Crowther, M.; Dufrost, V.; Wahl, D.; Doré, C.J.; Cuker, A.; Carrier, M.; et al. Use of direct oral anticoagulants in patients with thrombotic antiphospholipid syndrome: Guidance from the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. J. Thromb. Haemost. 2020, 18, 2126–2137. [Google Scholar] [CrossRef]
- Dufrost, V.; Wahl, D.; Zuily, S. Direct oral anticoagulants in antiphospholipid syndrome: Meta-analysis of randomized controlled trials. Autoimmun. Rev. 2021, 20, 102711. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Bueno, H.; Galié, N.; Gibbs, J.S.R.; Ageno, W.; Agewall, S.; Almeida, A.G.; Andreotti, F.; Barbato, E.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Pharmacovigilance Risk Assessment Committee (PRAC). EMA/ PRAC/219985/2019. Available online: https://www.ema.europa.eu/en/documents/prac-recommendation/prac-recommendations-signals-adopted-8-11-april-2019-prac-meeting_en.pdf (accessed on 15 September 2021).
- Arachchillage, D.R.J.; Gomez, K.; Alikhan, R.; Anderson, J.A.M.; Lester, W.; Laffan, M. Addendum to British Society for Haematology Guidelines on Investigation and Management of Antiphospholipid syndrome, 2012 (Br. J. Haematol. 2012; 157: 47–58): Use of direct acting oral anticoagulants. Br. J. Haematol. 2020, 189, 212–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lameijer, H.; Aalberts, J.J.J.; van Veldhuisen, D.J.; Meijer, K.; Pieper, P.G. Efficacy and safety of direct oral anticoagulants during pregnancy; a systematic literature review. Thromb. Res. 2018, 169, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Joste, V.; Dragon-Durey, M.-A.; Darnige, L. Diagnostic biologique du syndrome des antiphospholipides: Des critères à la pratique. La Rev. Médecine Interne 2018, 39, 34–41. [Google Scholar] [CrossRef]
- Ratzinger, F.; Lang, M.; Belik, S.; Jilma-Stohlawetz, P.; Schmetterer, K.G.; Haslacher, H.; Perkmann, T.; Quehenberger, P. Lupus-anticoagulant testing at NOAC trough levels. Thromb. Haemost. 2016, 116, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Hoxha, A.; Banzato, A.; Ruffatti, A.; Pengo, V. Detection of lupus anticoagulant in the era of direct oral anticoagulants. Autoimmun. Rev. 2017, 16, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Jourdi, G.; Delrue, M.; Stepanian, A.; Valaize, J.; Foulon-Pinto, G.; Demagny, J.; Duchemin, J.; Nedelec-Gac, F.; Darnige, L.; Curis, E.; et al. Potential usefulness of activated charcoal (DOAC remove®) for dRVVT testing in patients receiving Direct Oral AntiCoagulants. Thromb. Res. 2019, 184, 86–91. [Google Scholar] [CrossRef]
- Favresse, J.; Lardinois, B.; Sabor, L.; Devalet, B.; Vandepapeliere, J.; Braibant, M.; Lessire, S.; Chatelain, B.; Jacqmin, H.; Douxfils, J.; et al. Evaluation of the DOAC-Stop® Procedure to Overcome the Effect of DOACs on Several Thrombophilia Screening Tests. TH Open 2018, 2, e202–e209. [Google Scholar] [CrossRef] [Green Version]
- Farkh, C.; Ellouze, S.; Gounelle, L.; Sad Houari, M.; Duchemin, J.; Proulle, V.; Fontenay, M.; Delavenne, X.; Jourdi, G. A Diagnostic Solution for Lupus Anticoagulant Testing in Patients Taking Direct Oral FXa Inhibitors Using DOAC Filter. Front. Med. 2021, 8, 683357. [Google Scholar] [CrossRef]
- Devreese, K.M.J.; de Groot, P.G.; de Laat, B.; Erkan, D.; Favaloro, E.J.; Mackie, I.; Martinuzzo, M.; Ortel, T.L.; Pengo, V.; Rand, J.H.; et al. Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis: Update of the guidelines for lupus anticoagulant detection and interpretation. J. Thromb. Haemost. 2020, 18, 2828–2839. [Google Scholar] [CrossRef]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef]
- Platton, S.; Bartlett, A.; MacCallum, P.; Makris, M.; McDonald, V.; Singh, D.; Scully, M.; Pavord, S. Evaluation of laboratory assays for anti-platelet factor 4 antibodies after ChAdOx1 nCOV-19 vaccination. J. Thromb. Haemost. 2021, 19, 2007–2013. [Google Scholar] [CrossRef] [PubMed]
- Nazy, I.; Sachs, U.J.; Arnold, D.M.; McKenzie, S.E.; Choi, P.; Althaus, K.; Ahlen, M.T.; Sharma, R.; Grace, R.F.; Bakchoul, T. Recommendations for the clinical and laboratory diagnosis of VITT against COVID-19: Communication from the ISTH SSC Subcommittee on Platelet Immunology. J. Thromb. Haemost. 2021, 19, 1585–1588. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Langer, F.; Makris, M.; Pai, M.; Pavord, S.; Tran, H.; Warkentin, T.E. Vaccine-induced immune thrombotic thrombocytopenia (VITT): Update on diagnosis and management considering different resources. J. Thromb. Haemost. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HIT | APS | |
|---|---|---|
| Clinical expression | Thrombosis Thrombocytopenia +++ | Thrombosis and/or obstetrical events Thrombocytopenia |
| Main immunoglobulin isotype | IgG1 and IgG3 (IgM) | IgG2 IgM |
| Antibody targets | PF4/H complexes | β2GPI-CL PS/PT |
| Cellular activation | Multicellular activation via FcγRII (on platelets +++, endothelial cells, monocytes, neutrophils) | Multicellular activation via activation cascades of intracellular kinases |
| TF expression and secretion of procoagulant microparticles | ||
| Mechanism of platelet activation and thrombocytopenia | Strong platelet activation FcγRII +++ | Weak platelet activation F(ab’)2 ++ (FcγRII) |
| Recommended laboratory tests | Detection of anti-PF4/H antibodies Platelet functional assays | Detection of anti-CL, anti-β2GPI, or LAC activity; twice, 12 weeks apart. |
| Standard care | Non-heparin treatment (argatroban, danaparoid, bivalirudin, fondaparinux) Contraindication of VKA until platelet count ≥150 G/L | VKA +/− low-dose aspirin LMWH |
| DOAC use | Recommended in stable patients Rivaroxaban +++ | Still debated Contraindicated in triple-positive patients Not recommended in patients with arterial thrombosis |
| DOAC RCT | None | Cohen H. et al., 2016 [6] Pengo et al., 2018 [7] Ordi-Ros J. et al., 2019 [8] Woller S. et al., 2021 [9] |
| 2 Points | 1 Point | 0 Point | |
|---|---|---|---|
| Thrombocytopenia | Platelet count fall > 50% and platelet nadir ≥ 20 G/L | Platelet count fall 30%–50% or platelet nadir 10–19 G/L | Platelet count fall < 30% or platelet nadir < 10 G/L |
| Timing of platelet count fall | Clear onset between days 5–10; or platelet fall ≤ 1 day with prior heparin exposure within 30 days | Consistent with days 5–10 fall, but not clear; onset after day 10; or fall ≤ 1 day with prior heparin exposure between 30–100 days ago | Platelet count fall < 4 days without recent exposure |
| Thrombosis or other sequelae | New thrombosis (confirmed); skin necrosis; acute systemic reaction post IV UFH bolus | Progressive or recurrent thrombosis; non-necrotizing (erythematous) skin lesions; suspected thrombosis | None |
| oTher causes for thrombocytopenia | None apparent | Possible | Definite |
| Mechanism of Action | Administration | Half-Life | Clearance | |
|---|---|---|---|---|
| Recommended molecules | ||||
| Argatroban | Direct thrombin inhibitor | IV | ≈50 min | Hepatic +++ |
| Danaparoid | Factor Xa inhibitor | IV/SC | ≈25 h | Renal +++ |
| Bivalirudin | Direct thrombin inhibitor | IV | ≈25 min | Renal +++ |
| Fondaparinux | Factor Xa inhibitor | SC | ≈17 h | Renal +++ |
| Rivaroxaban | Direct factor Xa inhibitor | PO | 5–13 h | 2/3 hepatic1/3 renal |
| Other potential treatments | ||||
| Apixaban | Direct factor Xa inhibitor | PO | ≈12 h | 1/3 renal |
| Dabigatran | Direct thrombin inhibitor | PO | ≈13 h | Renal +++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carré, J.; Jourdi, G.; Gendron, N.; Helley, D.; Gaussem, P.; Darnige, L. Recent Advances in Anticoagulant Treatment of Immune Thrombosis: A Focus on Direct Oral Anticoagulants in Heparin-Induced Thrombocytopenia and Anti-Phospholipid Syndrome. Int. J. Mol. Sci. 2022, 23, 93. https://doi.org/10.3390/ijms23010093
Carré J, Jourdi G, Gendron N, Helley D, Gaussem P, Darnige L. Recent Advances in Anticoagulant Treatment of Immune Thrombosis: A Focus on Direct Oral Anticoagulants in Heparin-Induced Thrombocytopenia and Anti-Phospholipid Syndrome. International Journal of Molecular Sciences. 2022; 23(1):93. https://doi.org/10.3390/ijms23010093
Chicago/Turabian StyleCarré, Julie, Georges Jourdi, Nicolas Gendron, Dominique Helley, Pascale Gaussem, and Luc Darnige. 2022. "Recent Advances in Anticoagulant Treatment of Immune Thrombosis: A Focus on Direct Oral Anticoagulants in Heparin-Induced Thrombocytopenia and Anti-Phospholipid Syndrome" International Journal of Molecular Sciences 23, no. 1: 93. https://doi.org/10.3390/ijms23010093
APA StyleCarré, J., Jourdi, G., Gendron, N., Helley, D., Gaussem, P., & Darnige, L. (2022). Recent Advances in Anticoagulant Treatment of Immune Thrombosis: A Focus on Direct Oral Anticoagulants in Heparin-Induced Thrombocytopenia and Anti-Phospholipid Syndrome. International Journal of Molecular Sciences, 23(1), 93. https://doi.org/10.3390/ijms23010093