
A Liquid Biopsy in Bladder Cancer—The Current Landscape in Urinary Biomarkers


Abstract
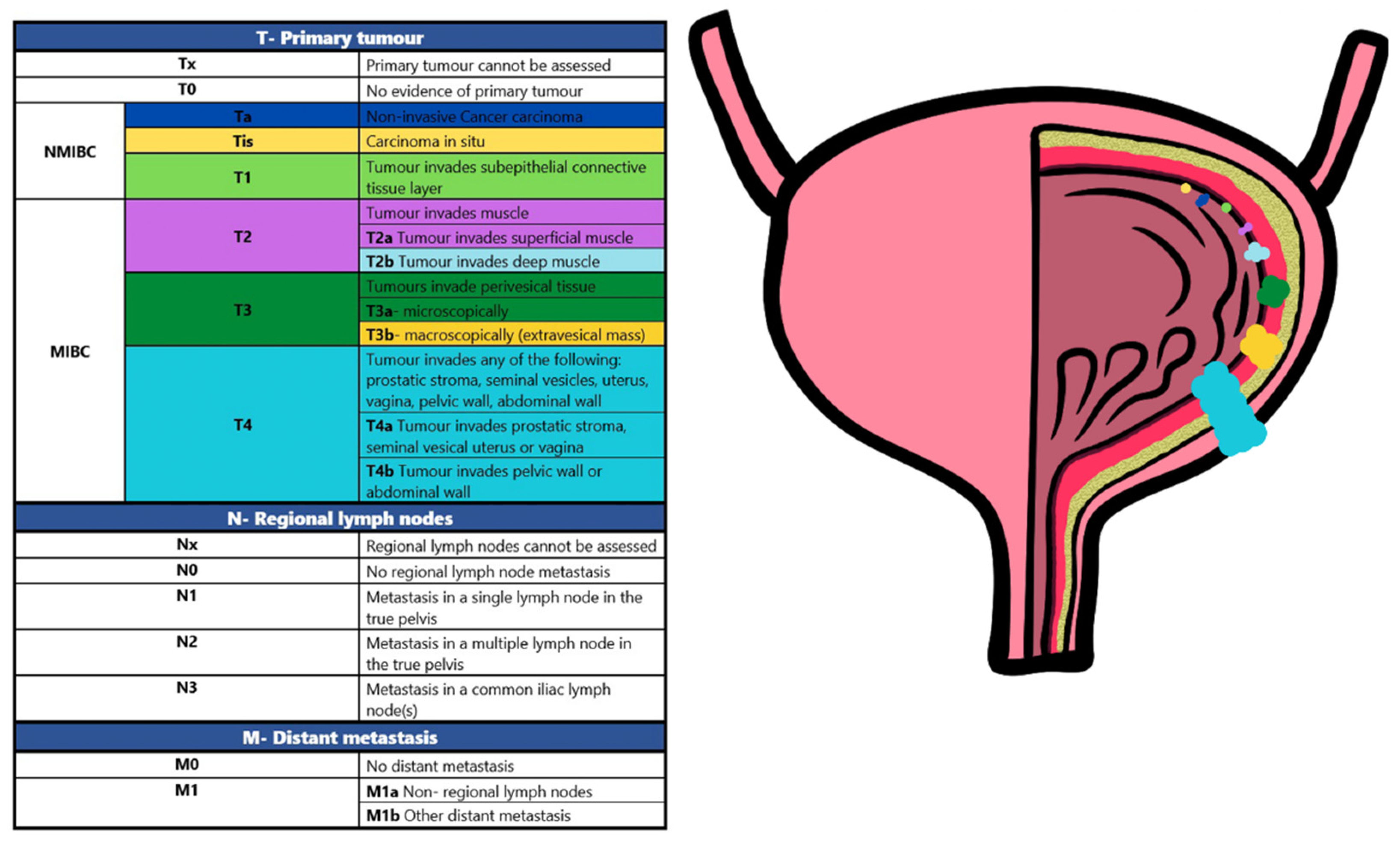
:1. Introduction: Bladder Cancer Issues and Urinary Biomarkers
2. Methods
3. What Is New in the Last Two Years?
3.1. Methylation
3.2. Exosomes
3.3. Proteomics

{kind=link}
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| APOA1 | prognostic | n = 258 (BCa = 108; control group = 150) | Genomic DNA was extracted from the blood and tumour tissues of all patients using the phenol chloroform method and DNA extraction kit (Zymo Research Corporation, Irvine, CA, USA). PCR was conducted using DNTP (Sigma-Aldrich, St. Louis, MO, USA), 10 mMdTTP primers (Sigma-Aldrich, St. Louis, MO, USA) and Taq DNA polymerase (Biotools, Madrid, Spain). PCR-RFLP was performed using a restriction endonuclease enzyme (New England Biolabs, NEB, England). APOA1 concentrations were measured using standard source ELISA kit (Thermo Scientific, Waltham, MA, USA). | n/a | BCa progression | AUC = 0.889 | retrospective | [38] |
| CDHR2 | Prognostic and surveillance | n = 40 (n = 8 no history or evidence of BCa, n = 4 geneal urinary system diseases, n = 16 BCa prior to surgery, n = 12 BCa after surgical removal of the tumour) | Urine samples of 40 patients obtained pre- and postoperatively. iTRAQ reagent kit (8plex, Applied Biosystems, Bedford, MA, USA) was used to quantify proteins in the urine. Q-Exactive mass spectrometry (Thermo Fisher Scientific, Waltham, MA, USA) was used to analyse the samples which then were validated with western blot. | n/a | Postoperative non-recurrence probability | No data | retrospective | [31] |
| HSP27 | n/a | High expression is associated with BCa progression | No data | |||||
| HNRNPA2B1 | n/a | Postoperative non-recurrence probability | No data | |||||
| BTA | Diagnostic and prognostic | n = 157 (BCa = 61, NMIBC: LG = 30, HG = 15; MIBC: hG = 16; UTUC = 44; control group = 52) | Cytology urine of 157 patients was performed and interpreted by pathologists. NMP and BTA-stat were measured by NMP22 (Alere INC., Waltham, MA, USA) and BTA-stat assays (Polymedco CDP, LLC., NY, USA). BTA was measured by chemiluminescence (Pergrande, Beijing, China), and ELISA for survivin (R&D systems, MN, USA). Data analysis performed with SPSS v.19.0 (IBM Corp., Armonk, NY, USA) and GraphPad prism7 (GraphPad Software Inc., Sand Diego, CA, USA). | BCa vs. UTUC differentiation | BCa survival | AUC = 0.84, PPV = 82%, NPV = 72%, Se. = 74%, Sp. = 81% | retrospective | [33] |
| BTA-stat | AUC = 0.67, PPV = 70%, NPV = 64%, Se. = 69%, Sp. = 63% | |||||||
| NMP22 | AUC = 0.69, PPV = 77%, NPV = 62%, Se. = 59%, Sp. = 79% | |||||||
| Survivin | AUC = 0.84, PPV = 84%, NPV = 75%, Se. = 74%, Sp. = 81% | |||||||
| PD-L1 | diagnostic | n = 122 (group 1 = 20, NMIBC: LG = 7, HG = 9; MIBC: HG = 4; group 2 = 63, NMIBC: LG = 10, HG = 21; MIBC: LG = 3, HG = 29; group 3 = 39, NMIBC: LG = 17, HG = 30; MIBC: LG = 3, HG = 33) | Quantikine ELISA for Human/Cynomolgus Monkey PD-L1/B7-H1 Immunoassay from R&D Systems (Catalog Number DB7H10) was used to inspect the urine samples of 122 patients. Data analysis was performed with SAS software v 9.4 (SAS institute Inc., Cary, NC, USA). | BCa detection | AUC = 0.74, PPV = 92%, NPV = 47%, Se. = 53%, Sp. = 90% | retrospective | [34] | |
| ADXBLADDER | prognostic | n = 629 (No recurrent BCa = 550, recurrent BCa = 79) | ADXBLADDER test was performed on urine samples of 629 patients. Data analysis was performed with Stata 12.1 (StataCorp,.College Station, TX, USA) | BCa recurrence prediction | AUC = 0.56, PPV = 17.5%, NPV = 99.15%, Se. = 66.7%, Sp. = 76.0% | prospective | [35] | |
| ANG | prognostic | n = 64 | Urine samples of 64 patients were tested with multiplex bead-based immunoassay (Oncuria™) from R&D Systems Inc (Minneapolis, MN, USA). Data analysis was performed with SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA). | Treatment response, recurrence | AUC = 0.7444, PPV = 41.2%, NPV = 91.5%, Se. = 63.6%, Sp. = 81.1% | prospective | [36] | |
| CA9 | AUC = 0.6878, PPV = 30.4%, NPV = 90.2%, Se. = 63.8%, Sp. = 69.8% | |||||||
| MMP10 | AUC = 0.7238, PPV = 32%, NPV = 92.3%, Se. = 72.7%, Sp. = 67.9% |
3.4. mRNA
3.5. Mutations
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| PIK3CA | diagnostic | n = 70 (LG = 27, HG = 43) | Genomic DNA extracted from fresh frozen tumours and urine cell sediments of 70 patients using phenol/chloroform method. DNA was quantified with a NanoDrop 2000 Spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). DNA amplification was performed on ProFlex PCR system (Applied Biosystems, Foster City, CA, USA). Sequencing was performed with BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA). Data analysis IBM SPSS software version 23. | BCa detection | Se. = 66.7%, Sp. = 100% | prospective | [48] | |
| AKT1 | Se. = 100%, Sp. = 100% | |||||||
| TERT | diagnostic | n = 60 (BCa (NMIBC) = 27, LG = 16, HG = 6; control group = 23; n = 10, tmr) | DNA was isolated from urine samples of 60 patients using QIAamp Circulating Nucleic Acid Kit (Qiagen GmbH, Hilden, Germany). The reference plasmids were created using pUC19 vector (cloning sites KpnI and HindIII). Forward primer and reverse primer were provided by Evrogen RU, AO. DNA isolated from liver cancer cells (originating from the HepG2 cell line; cat no. 85011430; MilliporeSigma) was used for amplification of the mutant C228T fragment. High-Fidelity DNA Polymerase (New England BioLabs Inc., Ipswich, MA, USA) was used to amplify the mutant insert. Quantification of DNA was performed using the QX200 ddPCR System (Bio-Rad Laboratories, Inc., Hercules, CA, USA). Detection of TERT promoter and mutations was achieved using TaqMan Liquid Biopsy dPCR Assays (TERT_C228T, Assay ID Hs000000092_rm and TERT_C250T, Assay ID Hs000000093_rm; Thermo Fisher Scientific Inc.). Data analysis performed with IBM SPSS Statistics 22.0 Software (IBM Corp., Armonk, NY, USA). | BCa detection | AUC = 0.768, Se. = 55.56%, Sp. = 100% | retrospective | [49] | |
| DNA sequencing | diagnostic | Retrospective haematuria clinic cohort = 214 (BCa = 97, non-BCa = 117) | DNA extraction was performed with Quick-DNA urine kits (D3061; Zymo Research, Irvine, CA, USA) on urine samples collected from all patients and quantified using high-sensitivity dsDNA Qubit kits (Thermo Fisher, Waltham, MA, USA). Libraries were prepare using Nonacus Cell3 Target enrichment and sequenced on a NovaSeq (Illumina, San Diego, CA, USA). | BCa detection | Se. = 87.6%, Sp. = 88.9% | retrospective | [50] | |
| Prospective haematuria clinic cohort = 215 (BCa = 68, non-BCa = 147) | Se. = 86.8%, Sp. = 81.0% | prospective | ||||||
| NMIBC surveillance cohort = 293 (BCa = 29, non-BCa = 264) | Se. = 86.2%, Sp. = 62.5% | prospective | ||||||
| Control group = 162 (normal samples = 100, confirmatory control samples = 62) | Normal samples Sp. = 89.9% Confirmatory control samples Sp. = 91.2% | retrospective | ||||||
| GWAS (rs9642880, rs710521) | prognostic | n = 200 (BCa = 150, NMIBC = 12, MIBC = 123; control group = 50) | DNA was extracted from urine of 200 patients with Qiagen Kits (Hilden, Germany) and then measured on a Nanodrop ND-2000c (Thermo Scientific, Waltham, MA, USA). PCR was carried out using Bio-RAD T100Thermal cycler. Thermo Scientific FastDigestStyl was used to digest. Data analysis performed with Microsoft Excel 2016 and IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). | BCa progression | No data | retrospective | [51] |
3.6. Metabolites
3.7. Others
4. Discussion
5. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANG | Angiogenin |
| AUC | Area under the curve |
| AS | Active surveillance |
| BC | Bladder cancer |
| BCG | Bacille Calmette–Guérin |
| BE | Bladder EpiCheck |
| BIAS | Bladder Cancer Italian Active Surveillance |
| BTA | Bladder tumour antigen |
| BTG2 | B cell translocation gene 2 |
| cfDNA | Cell-free DNA |
| CIS | Carcinoma in situ |
| CK | Cytokeratin |
| CS | Cystoscopy surveillance |
| CSS | Cancer-specific survival |
| CYFRA 21.1 | Cytokeratin fragment 21.1 |
| DDX17 | DEAD-Box Helicase 17 |
| DFS | Disease-free survival |
| GC-MS | gas chromatography-mass spectrometry |
| GC-TOFMS | gas chromatography coupled to a time-of-flight mass spectrometer |
| EAU | European Association of Urology |
| EMA | European Medicines Agency |
| EV | Extracellular Vesicles |
| FFS | Failure free-survival |
| HG | High grade |
| HPLC | high-performance liquid chromatography |
| IHC | Immunohistochemistry staining |
| iTRAQ | Isobaric tags for relative and absolute quantitation |
| LC-MS | liquid chromatography-mass spectrometry |
| LG | Low grade |
| lncRNA | Long non-coding RNAs |
| MDR | Minimal residual disease |
| MIBC | Muscle-invasive bladder cancer |
| NMIBC | Non-muscle invasive bladder cancer |
| NMP22 | Nuclear matrix protein 22 |
| NMR | nuclear magnetic resonance |
| NPV | Negative predictive value |
| OPLS-DA | Orthogonal Projections to Latent Structures Discriminant Analysis |
| OS | Overall survival |
| pCR | pathologic complete response |
| PD-L1 | Programmed death-ligand 1 |
| PFS | Progression-free survival |
| PPV | Positive predictive value |
| qMSP | quantitative Methylation Specific PCR |
| SERS | surface-enhanced Raman spectroscopy |
| TERC | Telomerase RNA component |
| TURBT | Transurethral resection of bladder tumour |
| UBC | Urothelial bladder cancer |
| UBT | Urinary biomarker test |
| UC | Urothelial carcinoma |
| UPLC-MS | Ultra-performance liquid chromatography coupled to mass spectrometry |
| VOC | volatile organic compounds |
| WLC | White-light cystoscopy |
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M. The global burden of urinary bladder cancer. Scand. J. Urol. Nephrol. 2008, 42 (Suppl. 218), 12–20. [Google Scholar] [CrossRef] [PubMed]
- Clavel, J. Progress in the epidemiological understanding of gene–environment interactions in major diseases: Cancer. Comptes Rendus. Biol. 2007, 330, 306–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Roupret, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)-2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Czerniak, B.; Dinney, C.; McConkey, D. Origins of Bladder Cancer. Annu. Rev. Pathol. Mech. Dis. 2016, 11, 149–174. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.; Campbell, M.; Chapin, A.; Eldrenkamp, E.; Fan, V.Y.; Haakenstad, A.; Kates, J.; Liu, Y.; Matyasz, T.; Micah, A.; et al. Evolution and patterns of global health financing 1995–2014: Development assistance for health, and government, prepaid private, and out-of-pocket health spending in 184 countries. Lancet 2017, 389, 1981–2004. [Google Scholar] [CrossRef] [Green Version]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Grossman, H.B.; Droller, M.; Schmidbauer, J.; Hermann, G.; Drăgoescu, O.; Ray, E.; Fradet, Y.; Karl, A.; Burgués, J.P.; et al. Photodynamic Diagnosis of Non–muscle-invasive Bladder Cancer with Hexaminolevulinate Cystoscopy: A Meta-analysis of Detection and Recurrence Based on Raw Data. Eur. Urol. 2013, 64, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Van Rhijn, B.W.; van der Poel, H.G.; van der Kwast, T.H. Urine Markers for Bladder Cancer Surveillance: A Systematic Review. Eur. Urol. 2005, 47, 736–748. [Google Scholar] [CrossRef]
- Karakiewicz, P.I.; Benayoun, S.; Zippe, C.; Ludecke, G.; Boman, H.; Sanchez-Carbayo, M.; Casella, R.; Mian, C.; Friedrich, M.G.; Eissa, S.; et al. Institutional variability in the accuracy of urinary cytology for predicting recurrence of transitional cell carcinoma of the bladder. BJU Int. 2006, 97, 997–1001. [Google Scholar] [CrossRef]
- Lokeshwar, V.B.; Habuchi, T.; Grossman, H.B.; Murphy, W.M.; Hautmann, S.H.; Hemstreet, G.P.; Bono, A.V.; Getzenberg, R.H.; Goebell, P.; Schmitz-Dräger, B.J.; et al. Bladder tumor markers beyond cytology: International Consensus Panel on bladder tumor markers. Urology 2005, 66, 35–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.J.; Kwon, C.S.; Forsythe, A.; Mamolo, C.M.; Masters, E.T.; Jacobs, I.A. Humanistic and Economic Burden of Non-Muscle Invasive Bladder Cancer: Results of Two Systematic Literature Reviews. Clin. Outcomes Res. 2020, 12, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Matulay, J.T.; Tabayoyong, W.; Duplisea, J.J.; Chang, C.; Daneshmand, S.; Gore, J.L.; Holzbeierlein, J.M.; Karsh, L.I.; Kim, S.P.; Konety, B.R.; et al. Variability in adherence to guidelines based management of nonmuscle invasive bladder cancer among Society of Urologic Oncology (SUO) members. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 796.e1–796.e6. [Google Scholar] [CrossRef]
- Bree, K.K.; Shan, Y.; Hensley, P.J.; Lobo, N.; Hu, C.; Tyler, D.S.; Chamie, K.; Kamat, A.M.; Williams, S.B. Management, Surveillance Patterns, and Costs Associated with Low-Grade Papillary Stage Ta Non–Muscle-Invasive Bladder Cancer Among Older Adults, 2004–2013. JAMA Netw. Open 2022, 5, e223050. [Google Scholar] [CrossRef]
- Matuszczak, M.; Salagierski, M. Diagnostic and Prognostic Potential of Biomarkers CYFRA 21.1, ERCC1, p53, FGFR3 and TATI in Bladder Cancers. Int. J. Mol. Sci. 2020, 21, 3360. [Google Scholar] [CrossRef]
- Oeyen, E.; Hoekx, L.; De Wachter, S.; Baldewijns, M.; Ameye, F.; Mertens, I. Bladder Cancer Diagnosis and Follow-Up: The Current Status and Possible Role of Extracellular Vesicles. Int. J. Mol. Sci. 2019, 20, 821. [Google Scholar] [CrossRef] [Green Version]
- Soria, F.; Droller, M.J.; Lotan, Y.; Gontero, P.; D’Andrea, D.; Gust, K.M.; Rouprêt, M.; Babjuk, M.; Palou, J.; Shariat, S.F. An up-to-date catalog of available urinary biomarkers for the surveillance of non-muscle invasive bladder cancer. World J. Urol. 2018, 36, 1981–1995. [Google Scholar] [CrossRef] [Green Version]
- Wolfs, J.R.E.; Hermans, T.J.N.; Koldewijn, E.L.; van de Kerkhof, D. Novel urinary biomarkers ADXBLADDER and bladder EpiCheck for diagnostics of bladder cancer: A review. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 161–170. [Google Scholar] [CrossRef]
- Ruan, W.; Chen, X.; Huang, M.; Wang, H.; Chen, J.; Liang, Z.; Zhang, J.; Yu, Y.; Chen, S.; Xu, S.; et al. A urine-based DNA methylation assay to facilitate early detection and risk stratification of bladder cancer. Clin. Epigenetics 2021, 13, 91. [Google Scholar] [CrossRef]
- Hentschel, A.E.; Beijert, I.J.; Bosschieter, J.; Kauer, P.C.; Vis, A.N.; Lissenberg-Witte, B.I.; van Moorselaar, R.J.A.; Steenbergen, R.D.M.; Nieuwenhuijzen, J.A. Bladder cancer detection in urine using DNA methylation markers: A technical and prospective preclinical validation. Clin. Epigenetics 2022, 14, 19. [Google Scholar] [CrossRef]
- Pierconti, F.; Martini, M.; Cenci, T.; Fiorentino, V.; Di Gianfrancesco, L.; Ragonese, M.; Bientinesi, R.; Rossi, E.; Larocca, L.M.; Racioppi, M.; et al. The bladder epicheck test and cytology in the follow-up of patients with non-muscle-invasive high grade bladder carcinoma. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 108.e19–108.e25. [Google Scholar] [CrossRef] [PubMed]
- Georgopoulos, P.; Papaioannou, M.; Markopoulou, S.; Fragou, A.; Kouvatseas, G.; Apostolidis, A. DNA Hypermethylation af a Panel of Genes as an Urinary Biomarker For Bladder Cancer Diagnosis. Urol. J. 2022, 19, 214–220. [Google Scholar] [CrossRef]
- Fang, Q.; Zhang, X.; Nie, Q.; Hu, J.; Zhou, S.; Wang, C. Improved urine DNA methylation panel for early bladder cancer detection. BMC Cancer 2022, 22, 237. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Cheng, L.; Deng, C.; Huang, L.; Li, J.; Wang, Y.; Li, M.; Yang, Q.; Dong, X.; Su, J.; et al. The genetic source tracking of human urinary exosomes. Proc. Natl. Acad. Sci. USA 2021, 118, e2108876118. [Google Scholar] [CrossRef]
- Huang, H.; Du, J.; Jin, B.; Pang, L.; Duan, N.; Huang, C.; Hou, J.; Yu, W.; Hao, H.; Li, H. Combination of Urine Exosomal mRNAs and lncRNAs as Novel Diagnostic Biomarkers for Bladder Cancer. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.; Han, D.; Ku, J.H.; Kim, H.H.; Kwak, C.; Jeong, C.W. Next-generation Proteomics-Based Discovery, Verification, and Validation of Urine Biomarkers for Bladder Cancer Diagnosis. Cancer Res. Treat. 2022, 54, 882–893. [Google Scholar] [CrossRef]
- El-Shal, A.S.; Shalaby, S.M.; Abouhashem, S.E.; Elbary, E.H.A.; Azazy, S.; Rashad, N.M.; Sarhan, W. Urinary exosomal microRNA-96-5p and microRNA-183-5p expression as potential biomarkers of bladder cancer. Mol. Biol. Rep. 2021, 48, 4361–4371. [Google Scholar] [CrossRef]
- Lin, H.; Shi, X.; Li, H.; Hui, J.; Liu, R.; Chen, Z.; Lu, Y.; Tan, W. Urinary Exosomal miRNAs as biomarkers of bladder Cancer and experimental verification of mechanism of miR-93-5p in bladder Cancer. BMC Cancer 2021, 21, 1293. [Google Scholar] [CrossRef]
- Tomiyama, E.; Matsuzaki, K.; Fujita, K.; Shiromizu, T.; Narumi, R.; Jingushi, K.; Koh, Y.; Matsushita, M.; Nakano, K.; Hayashi, Y.; et al. Proteomic analysis of urinary and tissue-exudative extracellular vesicles to discover novel bladder cancer biomarkers. Cancer Sci. 2021, 112, 2033–2045. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Shang, A.; Sun, Z.; Gao, Y.; Huang, J.; Ping, Y.; Chang, W.; Gu, C.; Sun, J.; Ji, P.; et al. Urinary Exosomal Long Noncoding RNA TERC as a Noninvasive Diagnostic and Prognostic Biomarker for Bladder Urothelial Carcinoma. J. Immunol. Res. 2022, 2022, 1–9. [Google Scholar] [CrossRef]
- Li, X.; Huang, C.; Zhang, X.; Yang, T.; Zuo, S.; Fu, C.; Zhang, Y.; Yang, C.; Chen, L. Discovery of bladder cancer biomarkers in paired pre- and postoperative urine samples. Transl. Androl. Urol. 2021, 10, 3402–3414. [Google Scholar] [CrossRef] [PubMed]
- Islam, K.; Syed, P.; Dhondt, B.; Gidwani, K.; Pettersson, K.; Lamminmäki, U.; Leivo, J. Detection of bladder cancer with aberrantly fucosylated ITGA3. Anal. Biochem. 2021, 628, 114283. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.-W.; Wang, Y.-R.; Fan, G.-R.; Niu, Q.; Zhao, Y.-L.; Wang, H.; Svatek, R.; Rodriguez, R.; Wang, Z.-P. Diagnostic and prognostic role of BTA, NMP22, survivin and cytology in urothelial carcinoma. Transl. Cancer Res. 2021, 10, 3192–3205. [Google Scholar] [CrossRef]
- Tosev, G.; Wahafu, W.; Reimold, P.; Damgov, I.; Schwab, C.; Aksoy, C.; Kaczorowski, A.; Stenzinger, A.; Nyarangi-Dix, J.; Hohenfellner, M.; et al. Detection of PD-L1 in the urine of patients with urothelial carcinoma of the bladder. Sci. Rep. 2021, 11, 14244. [Google Scholar] [CrossRef]
- Rouprêt, M.; Gontero, P.; McCracken, S.R.; Dudderidge, T.; Stockley, J.; Kennedy, A.; Rodriguez, O.; Sieverink, C.; Vanié, F.; Allasia, M.; et al. Reducing the Frequency of Follow-up Cystoscopy in Low-grade pTa Non–muscle-invasive Bladder Cancer Using the ADXBLADDER Biomarker. Eur. Urol. Focus 2022. [Google Scholar] [CrossRef]
- Murakami, K.; Kamat, A.M.; Dai, Y.; Pagano, I.; Chen, R.; Sun, Y.; Gupta, A.; Goodison, S.; Rosser, C.J.; Furuya, H. Application of a multiplex urinalysis test for the prediction of intravesical BCG treatment response: A pilot study. Cancer Biomark. 2022, 33, 151–157. [Google Scholar] [CrossRef]
- Murakami, K.; Pagano, I.; Furuya, H.; Daskivich, T.; Mori, D.; Rosser, C.J. Clinical Utility of OncuriaTM, a Multiplexed Liquid Biopsy for the Non-Invasive Detection of Bladder Cancer—A Pilot Study. Diagnostics 2022, 12, 131. [Google Scholar] [CrossRef]
- Magray, J.; Pandith, A.; Qasim, I.; Khateeb, M.; Hamid, A.; Koul, A.; Shah, Z.; Baba, S.; Mansoor, S.; Charifi, W.; et al. Significant Implications of APOA1 Gene Sequence Variations and Its Protein Expression in Bladder Cancer. Biomedicines 2021, 9, 938. [Google Scholar] [CrossRef]
- Shkolyar, E.; Zhao, Q.; Mach, K.E.; Teslovich, N.C.; Lee, T.J.; Cox, S.; Skinner, E.C.; Lu, Y.; Liao, J.C. Bladder cancer risk stratification using a urinary mRNA biomarker panel–A path towards cystoscopy triaging. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 497.e9–497.e15. [Google Scholar] [CrossRef] [PubMed]
- Dubois, J.; Rueger, J.; Haubold, B.; Far, R.K.-K.; Sczakiel, G. Transcriptome analyses of urine RNA reveal tumor markers for human bladder cancer: Validated amplicons for RT-qPCR-based detection. Oncotarget 2021, 12, 1011–1023. [Google Scholar] [CrossRef] [PubMed]
- Cancel-Tassin, G.; Roupret, M.; Pinar, U.; Gaffory, C.; Vanie, F.; Ondet, V.; Compérat, E.; Cussenot, O. Assessment of Xpert Bladder Cancer Monitor test performance for the detection of recurrence during non-muscle invasive bladder cancer follow-up. World J. Urol. 2021, 39, 3329–3335. [Google Scholar] [CrossRef]
- Elsawy, A.A.; Awadalla, A.; Abdullateef, M.; Ahmed, A.E.; Abol-Enein, H. Can repeat biopsy be skipped after initial complete resection of T1 bladder cancer? The role of a novel urinary mRNA biomarker. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 437.e11–437.e19. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Y.; Cao, C.; Xi, H.; Chen, W.; Zheng, W.; Dong, X.; Zheng, S.; Li, L.; Ma, J.; et al. CYR61 as a potential biomarker for the preoperative identification of muscle-invasive bladder cancers. Ann. Transl. Med. 2021, 9, 761. [Google Scholar] [CrossRef]
- Singer, G.; Ramakrishnan, V.M.; Rogel, U.; Schötzau, A.; Disteldorf, D.; Maletzki, P.; Adank, J.-P.; Hofmann, M.; Niemann, T.; Stadlmann, S.; et al. The Role of New Technologies in the Diagnosis and Surveillance of Non-Muscle Invasive Bladder Carcinoma: A Prospective, Double-Blinded, Monocentric Study of the XPERT© Bladder Cancer Monitor and Narrow Band Imaging© Cystoscopy. Cancers 2022, 14, 618. [Google Scholar] [CrossRef]
- Fasulo, V.; Paciotti, M.; Lazzeri, M.; Contieri, R.; Casale, P.; Saita, A.; Lughezzani, G.; Diana, P.; Frego, N.; Avolio, P.P.; et al. Xpert Bladder Cancer Monitor Avoid Cystoscopies in Patients Under ‘Active Surveillance’ for Recurrent Bladder Cancer (BIAS Project): Longitudinal Cohort Study. Front. Oncol. 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Chai, C.A.; Yeoh, W.S.; Rajandram, R.; Aung, K.P.; Ong, T.A.; Kuppusamy, S.; Nazran, A.; Kumaran, K.; Razack, A.H.A.; Teoh, J.Y. Comparing CxBladder to Urine Cytology as Adjunct to Cystoscopy in Surveillance of Non-muscle Invasive Bladder Cancer—A Pilot Study. Front. Surg. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Raman, J.D.; Kavalieris, L.; Konety, B.; Porten, S.; Daneshmand, S.; Lotan, Y.; Loo, R. The Diagnostic Performance of Cxbladder Resolve, Alone and in Combination with Other Cxbladder Tests, in the Identification and Priority Evaluation of Patients at Risk for Urothelial Carcinoma. J. Urol. 2021, 206, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- El Ahanidi, H.; El Azzouzi, M.; Arrouchi, H.; Alaoui, C.H.; Tetou, M.; Bensaid, M.; Oukabli, M.; Ameur, A.; Al Bouzidi, A.; El Mzibri, M.; et al. AKT1 and PIK3CA activating mutations in Moroccan bladder cancer patients’ biopsies and matched urine. Pan Afr. Med. J. 2022, 41, 59. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Kamalov, D.; Tivtikyan, A.; Balatsky, A.; Samokhodskaya, L.; Okhobotov, D.; Kozlova, P.; Pisarev, E.; Zvereva, M.; Kamalov, A. Urine TERT promoter mutations-based tumor DNA detection in patients with bladder cancer: A pilot study. Mol. Clin. Oncol. 2021, 15, 253. [Google Scholar] [CrossRef]
- Ward, D.G.; Baxter, L.; Ott, S.; Gordon, N.S.; Wang, J.; Patel, P.; Piechocki, K.; Silcock, L.; Sale, C.; Zeegers, M.P.; et al. Highly Sensitive and Specific Detection of Bladder Cancer via Targeted Ultra-deep Sequencing of Urinary DNA. Eur. Urol. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Mamdouh, S.; Khorshed, F.; Hammad, G.; Elesaily, K.; Safwat, G.; Hammam, O.; Aboushousha, T. Molecular Detection of Genetic Susceptibility to Bladder Cancer in Egyptian Patients. Asian Pac. J. Cancer Prev. 2022, 23, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Y.; Juo, B.-R.; Yeh, Y.-H.; Fu, S.-H.; Chen, Y.-T.; Chen, C.-L.; Wu, K.-P. Putative markers for the detection of early-stage bladder cancer selected by urine metabolomics. BMC Bioinform. 2021, 22, 305. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Kang, H.; Zhang, X.; Nie, Q.; Wang, H.; Wang, C.; Zhou, S. Urinary metabolomics for discovering metabolic biomarkers of bladder cancer by UPLC-MS. BMC Cancer 2022, 22, 214. [Google Scholar] [CrossRef] [PubMed]
- Nerli, R.; Ghagane, S.; Rangrez, S.; Chandra, S.; Thakur, M.; Gomella, L. Detection of bladder cancer using voided urine sample and by targeting genomic VPAC receptors. Indian J. Urol. 2021, 37, 345. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, P.S.; Chen, K.; Babbra, R.K.; Feng, W.; Pejovic, N.; Nallicheri, A.; Harris, P.K.; Dienstbach, K.; Atkocius, A.; Maguire, L.; et al. Urine tumor DNA detection of minimal residual disease in muscle-invasive bladder cancer treated with curative-intent radical cystectomy: A cohort study. PLoS Med. 2021, 18, e1003732. [Google Scholar] [CrossRef]
- Mukae, Y.; Ito, H.; Miyata, Y.; Araki, K.; Matsuda, T.; Aibara, N.; Nakamura, Y.; Matsuo, T.; Sakai, H.; Ohyama, K. Ceruloplasmin Levels in Cancer Tissues and Urine Are Significant Biomarkers of Pathological Features and Outcome in Bladder Cancer. Anticancer Res. 2021, 41, 3815–3823. [Google Scholar] [CrossRef]
- Muto, S.; Lu, Y.; Ide, H.; Yamaguchi, R.; Saito, K.; Kitamura, K.; Noma, Y.; Koyasu, H.; Hirano, H.; Ashizawa, T.; et al. The Use of Urine Mycobacterium tuberculosis Complex Polymerase Chain Reaction as a Predictive Factor for Recurrence and Progression After Intravesical Bacillus Calmette-Guérin Therapy in Patients with Non–muscle-invasive Bladder Cancer. Eur. Urol. Open Sci. 2021, 27, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Aalami, A.H.; Abdeahad, H.; Mesgari, M.; Sathyapalan, T.; Sahebkar, A. Urinary Angiogenin as a Marker for Bladder Cancer: A Meta-Analysis. BioMed Res. Int. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Džubinská, D.; Zvarík, M.; Kollárik, B.; Šikurová, L. Multiple Chromatographic Analysis of Urine in the Detection of Bladder Cancer. Diagnostics 2021, 11, 1793. [Google Scholar] [CrossRef]
- Moisoiu, T.; Dragomir, M.P.; Iancu, S.D.; Schallenberg, S.; Birolo, G.; Ferrero, G.; Burghelea, D.; Stefancu, A.; Cozan, R.G.; Licarete, E.; et al. Combined miRNA and SERS urine liquid biopsy for the point-of-care diagnosis and molecular stratification of bladder cancer. Mol. Med. 2022, 28, 39. [Google Scholar] [CrossRef]
- Lett, L.; George, M.; Slater, R.; Costello, B.D.L.; Ratcliffe, N.; García-Fiñana, M.; Lazarowicz, H.; Probert, C. Investigation of urinary volatile organic compounds as novel diagnostic and surveillance biomarkers of bladder cancer. Br. J. Cancer 2022, 127, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Beukers, W.; van der Keur, K.A.; Kandimalla, R.; Vergouwe, Y.; Steyerberg, E.W.; Boormans, J.L.; Jensen, J.B.; Lorente, J.A.; Real, F.X.; Segersten, U.; et al. FGFR3, TERT and OTX1 as a Urinary Biomarker Combination for Surveillance of Patients with Bladder Cancer in a Large Prospective Multicenter Study. J. Urol. 2017, 197, 1410–1418. [Google Scholar] [CrossRef]
- Köhler, C.U.; Bonberg, N.; Ahrens, M.; Behrens, T.; Hovanec, J.; Eisenacher, M.; Noldus, J.; Deix, T.; Braun, K.; Gohlke, H.; et al. Noninvasive diagnosis of urothelial cancer in urine using DNA hypermethylation signatures—Gender matters. Int. J. Cancer 2019, 145, 2861–2872. [Google Scholar] [CrossRef] [PubMed]
- De Strooper, L.M.A.; van Zummeren, M.; Steenbergen, R.D.M.; Bleeker, M.C.G.; Hesselink, A.T.; Wisman, G.B.A.; Snijders, P.J.F.; Heideman, D.A.M.; Meijer, C.J.L.M. CADM1, MAL and miR124-2 methylation analysis in cervical scrapes to detect cervical and endometrial cancer. J. Clin. Pathol. 2014, 67, 1067–1071. [Google Scholar] [CrossRef]
- Vorsters, A.; Bergh, J.V.D.; Micalessi, I.; Biesmans, S.; Bogers, J.-P.; Henß, A.; De Coster, I.; Ieven, M.; Van Damme, P. Optimization of HPV DNA detection in urine by improving collection, storage, and extraction. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 2005–2014. [Google Scholar] [CrossRef] [PubMed]
- Winnike, J.H.; Wei, X.; Knagge, K.J.; Colman, S.D.; Gregory, S.G.; Zhang, X. Comparison of GC-MS and GC×GC-MS in the Analysis of Human Serum Samples for Biomarker Discovery. J. Proteome Res. 2015, 14, 1810–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittmann, B.M.; Stirdivant, S.M.; Mitchell, M.W.; Wulff, J.E.; McDunn, J.E.; Li, Z.; Dennis-Barrie, A.; Neri, B.P.; Milburn, M.V.; Lotan, Y.; et al. Bladder Cancer Biomarker Discovery Using Global Metabolomic Profiling of Urine. PLoS ONE 2014, 9, e115870. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| VIM, OSTM1, SLC4A10, AC092805.1, ONECUT2 | Prognostic | Cohort 1 = 192 (116 BCa, MIBC = 47, NMIBC = 68; 76 non-BCa) | Urine samples collected from 464 patients before cystoscopy or surgery. Genomic DNA was extracted using the QIAamp DNA blood Mini Kit (Qiagen, Germany, Catalog No. 51106) and quantified by the Qubit Assay (Thermo Fisher Scientific, USA, Catalog No. Q32851). Bisulfite treatment was performed on genomic DNA with the EZ-96-DNA Methylation-Direct MagPrep Kit (Zymo Research, USA, Catalog No. D5044). The methylation of bisulfite-treated DNA was analyzed by a 22-marker BCA DNA (AnchorDX, China, Catalog No. UME043) on the QuantStudio 3 Real-Time PCR System (Thermo Fisher, Waltham, Ma, USA). EpiTect PCR Control DNA Set (Qiagen, Germany, Catalog No. 59695) was used as positive and negative controls. DNA quantified by the Meth-Quant Master Mix (AnchorDx, China, Catalog No. UME043-01 ) and the 22-marker BCA Detect Panel (AnchorDx, China, Catalog No. UME043-02). | Preoperative risk stratification of BCa | Non-BCa AUC = 0.78, PPV = 88.6%, NPV = 81.8%, Se. = 87.8%, Sp. = 82.9% | Retrospective | [19] | |
| LMR-NMIBC AUC = 0.78, PPV = 54.5%, NPV = 91.7%, Se. = 46.2%, Sp. = 93.9% | ||||||||
| NMIBC+MIBC AUC = 0.78, PPV = 80.4%, NPV = 84.8%, Se. = 83.1%, Sp. = 82.4% | ||||||||
| Cohort 2 = 98 (59 BCa, MIBC = 22, NMIBC = 35; 39 non-BCa) | Non-BCa AUC = 0.821, PPV = 81.1%, NPV = 87.2%, Se. = 91.1% Sp. = 87.2% | |||||||
| LMR-NMIBC AUC = 0.821, PPV = 54.5%, NPV = 90.5%, Se. = 42.9%, Sp. = 93.8% | ||||||||
| NMIBC+MIBC AUC = 0.821, PPV = 84.4%, NPV = 92.0%, Se. = 90.5%, Sp. = 86.8% | ||||||||
| ONECUT2, VIM | Diagnostic and prognostic | Cohort 1 = 192 (116 BCa, MIBC = 47, NMIBC = 68; 76 non-BCa) | BCa detection | AUC = 0.898, PPV = 88.6%, NPV = 80.8%, Se. = 87.1%, Sp. = 82.9% | Retrospective | |||
| Cohort 2 = 98 (59 BCA, MIBC = 22, NMIBC = 35; 39 non-BCa) | AUC = 0.921, PPV = 92.9%, NPV = 83.3%, Se. = 88.1%, Sp. = 89.7% | |||||||
| Cohort 3 = 174 (35 BCa, MIBC = 5, NMIBC = 29; 147 non-BCa) | AUC = 0.935, PPV = 60.8%, NPV = 97.6%, Se. = 91.2%, Sp. = 85.7% | Prospective | ||||||
| FAM19A4 | diagnostic | n = 208 (BCa = 108; LG = 45, HG = 63; Control group = 100, haematuria = 34, benign urological conditions = 43, healthy = 23) | Urine samples of 208 patients were collected before cystoscopy or TURBT. DNA was isolated from urine using QIAamp DNA Mini Kit (Qiagen GmbH, Hilden, Germany). DNA concentrations were measured with NanoDrop 1000 (ThermoFisher Scientific, Waltham, MA, USA). EZ DNA Methylation™ Kit (Zymo Research, Orange, CA, USA) was used for bisulphite conversion. qMSP was performed to identify methylation values of targeted biomarkers. Data analysis were performed with R Statistical Software (v.3.6.1, R Foundation for Statistical Computing, Vienna, Austria). | BCa detection | AUC = 0.72 | Retrospective | [20] | |
| GHSR | GHSR AUC = 0.89, MAL AUC = 0.85, GHSR/MAL AUC = 0.89, Se. = 80%, Sp. = 93% | |||||||
| MAL | ||||||||
| miR-129 | AUC = 0.83 | |||||||
| miR-935 | AUC = 0.79 | |||||||
| PHACTR3 | AUC = 0.69 | |||||||
| PRDM14 | AUC = 0.88 | |||||||
| SST | AUC = 0.84 | |||||||
| ZIC1 | AUC = 0.88 | |||||||
| Altogether | Se. = 81%, Sp. = 95% | |||||||
| Bladder epicheck | diagnostic | n = 205 (HG NMIBC = 135, T1G3 = 86, T1G2 = 49, CIS = 70) | Urine samples collected from 205 patients were centrifuged twice. DNA was extracted using Bladder EpiCheck DNA extraction kit and prepared for the PCR assay using the Bladder EpiCheck test kit. Data analysis performed with GraphPad-Prism 5 software (Graphpad Software-Prism 5 software, San Diego, CA, USA) and MedCalc version 10.2.0.0 (MedCalc Software, Mariakerke, Belgium). | BCa detection | AUC = 0.94, PPV = 60%, NPV = 97.7%, Se. = 94.3%, Sp. = 79.6% | Prospective | [21] | |
| DNA hypermethylation (RASSF1, RARB, DAPK, TERT, APC) | diagnostic | n = 85 (BCa = 50, NMIBC = 37, MIBC = 5; control group = 35) | Urine samples were collected form 85 patients before cystoscopy. DNA was extracted from urine using the Cells and Tissue DNA Isolation Kit (Norgen Biotek Corp., Thorold, Canada). Sodium bisulfite modification of DNA was performed with the EZ DNA Methylation-GoldKit (Zymo Research, Orange, CA). Quantification of the percentage of methylation of DNA was performed with Luna Universal Probe qPCR Master Mix (New England Biolabs, Ipswich, MA, USA) and on Applied Biosystems StepOnePlus Real Time PCR System (Thermo Fisher Scientific, Inc., Waltham, MA, USA). | BCa detection | AUC = 0.76, PPV = 90%, NPV = 53%, Se. = 61.4%, Sp. = 86.4% | Prospective | [22] | |
| PCDH17, POU4F2, PENK | diagnostic | n = 252 (panel design: BCa = 18, control group = 15; validation: BCa = 107, control group = 100) | DNA from the urinary cell pellets was extracted using QIAamp DNA Mini Kit (Qiagen). DNA quality and quantity were assessed using a NanoDrop2000 (Thermo Scientific, Wilmington, DE, USA). Bisulfite conversion was performed with a ZYMO EZ DNA Methylation-Gold Kit (ZYMO, Irvine, CA, USA). Sequencing was performed on an Illumina Hiseq platform. The bisulfite modification reaction was executed by 96-Well GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA, USA). DNA amplification was performed on 7500 Real-Time PCR System (Applied Biosystems, Foster City, CA, USA). | BCa detection | AUC = 0.96, Se. = 87%, Sp. = 97% | Retrospective | [23] |
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference | |
|---|---|---|---|---|---|---|---|---|---|
| Exosome 2 (CD248, MT-ATP) | Diagnostic | n = 116 | Urine samples were collected from 116 patients and then expression of genes and functionality of exosomal RNAs were investigates by using single-cell mapper (scMappR). Data analysis performed with R package (version 3.0.2, R-project). | BCa detection | AUC = 0.898 | Retrospective | [24] | ||
| KLHDC7B | Diagnostic and prognostic | n = 180 (group 1 = 10 BCa, LG = 4, HG = 6; 10 HCs, group 2 = 80 BCa, LG = 35, HG = 45; 80 HCs) | Urine samples collected from 90 patients. Extraction of exosomes was conducted using a commercial kit (Norgen Biotek Corp., Thorold, Canada). Nanoparticle Tracking Analysis (NTA) was used to examine the size distribution and concentration of exosomes (ZetaView particle tracker, ZetaVIEW S/N 17-310, Particle Metrix, Germany). Extracted exosomes were imaged using a JEM-1400 transmission electron microscope (JEOL Inc., Peabody, MA, USA). Western Blot was performed using Western Chemiluminescent HRP Substrate (WBKLS0100). Urine Exosome RNA Isolation Kit (Norgen Biotek Corp, Product No. 47200, Thorold, Canada) was used to extract total exosome RNA, and then evaluated by a NanoDrop spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). RT-qPCR was performed using SYBR Premix Ex-Taq II (RR820A, Takara, Dalian, China). Data analysis performed using SPSS 24.0 software (IBM Corp., Armonk, NY, USA). | BCa detection | BCa progression | AUC = 0.842, PPV = 68.5%, NPV = 86.7%, Se. = 68.5%, Sp. = 88.3% | Retrospective | [25] | |
| CASP14 | AUC = 0.765, PPV = 80.3%, NPV = 64.7%, Se. = 77.5%, Sp. = 70.6% | ||||||||
| PRSS1 | AUC = 0.823, PPV = 60.3%, NPV = 87.5%, Se. = 78.1%, Sp. = 75.0% | ||||||||
| MIR205HG | AUC = 0.843, PPV = 56%, NPV = 88.7%, Se. = 77.3%, Sp. = 83.1% | ||||||||
| GAS5 | AUC = 0.729, PPV = 74.7%, NPV = 64.1%, Se. = 78.7%, Sp. = 60.3% | ||||||||
| A2M | Diagnostic and surveillance | n = 156 (discovery = 12; n = 24, LG = 3, HG = 3; verification = 24, LG = 0, HG = 18; validation = 120, LG = 20, HG = 75) | Urine protein and exosome was extracted from 156 participants urine. Prepared urinary peptides were analyzed using liquid chromatography-tandem mass spectrometry LC-MS/MS. MS raw files were processed in MaxQuant (v.1.5.3.1). Data-dependent acquisition (DDA) and data-independent acquisition (DIA) methods were conducted with an Ultimate 3000 UHPLC system (Dionex, Sunnyvale, CA, USA) coupled to a Q-Exactive Plus mass spectrometer (Thermo Fisher Scientific Inc., Waltham, MA, USA). | BCa detection | n/a | A2M AUC = 0.658 CFL1 AUC = 0.629 ITIH2 AUC = 0.759 Model 1(3 biomarkers) AUC = 0.845, PPV = 48.5%, NPV = 94.9%, Se. = 88.0%, Sp. = 81.3% | Model 2 (All biomarkers) AUC = 0.842, PPV = 42.5%, NPV = 95.8%, Se. = 85.0%, Sp. = 74.7% | Retrospective | [26] |
| CFL1 | |||||||||
| ITIH2 | |||||||||
| APOA1 | AUC = 0.702 | ||||||||
| AFM | AUC = 0.687 | ||||||||
| FGA | AUC = 0.612 | ||||||||
| CDC5L | AUC = 0.659 | ||||||||
| CD5L | AUC = 0.658 | ||||||||
| miRNA-96 | Diagnostic | n = 100 (study group = 72, NMIBC = 22, MIBC = 29; control group = 28) | Exosomes were isolated from urine of 100 patients before treatment using miRCURY Exosome Isolation Kit (Qiagen, Hilden, Germany). Extraction of total miRNA was performed with miRcute miRNA isolation kits (Tiangen biotech, Beijing, China). miScript Reverse Transcription Kit (Qiagen GmbH, Hilden, Germany) was used for reverse transcription and polyadenylation of the miRNA to complementary DNA (cDNA). Quantification of exosomal miRNA was performed with a Stratagene Mx3005P. Statistical analysis was performed using SPSS software (IBM Corp., Armonk, NY, USA). | BCa detection | AUC = 0.85, PPV = 91.1%, NPV = 81.8%, Se. = 80.4%, Sp. = 91.8% | Prospective | [27] | ||
| miRNA-183 | AUC = 0.83, PPV = 81.6%, NPV = 78.4%, Se. = 78.4%, Sp. = 81.6% | ||||||||
| miR-93-5p | Diagnostic | n = 120 (BCa = 12, NMIBC = 6, MIBC = 6; control group = 4; validation = 104, BCa = 53, control group = 51) | Exosomes were isolated from urine collected from 120 patients before treatment in an ultracentrifuge (Beckman Coulter, Miami, FL, USA). Exosomes were processed for nanoparticle tracking analysis (NTA) with NanoSight NS300 instrument (Malvern, UK). Total protein was extracted in RIPA lysis buffer (89,900, Thermo Fisher Scientific, Waltham, MA, USA). Total RNA was extracted with the Trizol Reagent (15,596,026, Invitrogen, Carlsbad, CA, USA). RNA was quantified and assessed by NanoDrop ND-2000 (Thermo Fisher Scientific, Waltham, MA, USA). miRNA expression was quantified using TaqMan single® microRNA assays (442,975, Applied Biosystems®, Foster City, CA, USA). qRT-PCR was performed with ABI 7300 Real-Time PCR System (Applied Biosystems, Foster City, CA, USA). Data analysis was peformed using R 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). | BCa detection | AUC = 0.838, Se. = 74.1%, Sp. = 90.2% | retrospective | [28] | ||
| miR-516a-5p | AUC = 0.790, Se. = 72.9%, Sp. = 89.9% | ||||||||
| HSP90 | diagnostic | n = 81 (discovery phase: BCa = 7, NMIBC = 3, MIBC = 4; control group= 4; validation phase: BCa = 40, NMIBC = 20, MIBC = 20, control group = 30) | Urine samples were collected from 77 and BCa tissue samples from 47 patients. Proteis concentration of Te-EVs was measured using a Micro BCa protein assay kit (Thermo Fisher Scientific, Waltham, MA, USA). Proteins in urinary and tissue samples were separated using SDS-PAGE and transferred on to a polyvinylidene difluoride (Thermo Fisher Scientific, Waltham, MA, USA). The size and concentration of EVs were analyzed using NTA system (NanoSight). TEM was used to inspect the samples with JEM-1400Plus transmission electron microscope (JEOL Ltd., Tokyo, Japan). EVs were lysed using a MPEX PTS reagent kit (GL Science). TMT 10-plex system (Thermo Fisher Scientific, Waltham, MA, USA) was used for TMT-labeling. TMT-labeled peptides were alanyzed using a Q-Exactive Plus mass spectrometer (Thermo Fisher Scientific, Waltham, MA, USA) with an UltiMate 3000 Nano-flow high-performance LC system (Dionex, Sunnyvale, CA, USA) and an HTC-PAL autosampler (CTC Analytics, Zwingen, Switzerland). Data analysis was performed using JMP Pro software (v.14.0.0, SAS Institute, CARY, N.C, USA), and visualization quantification was performed using GraphPad Prism software (v.7.05; GraphPad Software, San Diego, CA, USA). | BCa detection | AUC = 0.813, Se. = 82.5%, Sp. = 70.0% | retrospective | [29] | ||
| SDC1 | AUC = 0.785, Se. = 82.5%, Sp. = 63.3% | ||||||||
| MARCKS | AUC = 0.772, Se. = 65%, Sp. = 80% | ||||||||
| MARCKSL | AUC = 0.757, | ||||||||
| TJP2 | AUC = 0.748 | ||||||||
| CD55 | AUC = 0.706 | ||||||||
| TERC | Diagnostic and prognostic | n = 128 (LG = 20, HG = 108) | Exosomes used for sequencing were isolated from urine using differential centrifugation. Exosomes used for validation were isolated from urine using exosome extraction kit (BestBio, Shanghai, China). TEM was performed to view and capture images (Thermo Fisher Scientific, Waltham, MA, USA). NanoSight LM10 system (Malvern Instruments LTD., Malvern, UK) was used to detect the concetration and size distribution of particles. Western blot was performed using anti-TSG101 (Abcam, Cambridge, UK), anti-HSP70, antiAnnexin V, and anti-CD9 (Cell Signaling Technology, Danvers, MA, USA). Second antibody antirabbiy IgG (Millipore, Burlington, MA, USA). RNA sequencing was performed using an Illumina Novaseq 6000 system (San Diego, CA, USA). qPCR was performed using TB Green Premix Ex Taq II (Tli RNaseH Plus, Takara, Dalian, Japan) on an Applied Biosystems 7300 real-time PCR system (Waltham, MA, USA). Data analysis perfomed with Graphpad Prism 8 (GraphPad Software Inc., Sand Diego, CA, USA) and MedCalc v.15.2.2 (MedCalc software Ltd., Ostend, Belgium). | BCa detection | AUC = 0.836, Se. = 78.65%, Sp. = 77.78% | retrospective | [30] | ||
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| ROBO1, CRH, IGF2 | diagnostic | n = 177 (screening = 95; surveillance = 76; both = 6) | Urine collected from 177 patients and then evaluated d for ROBO1, WNT5A, CDC42BPB, ABL1, CRH, IGF2, ANXA10, and UPK1B expression using GeneXpert Dx (Cepheid, Sunnyvale, CA, USA) automated multiplex RT-PCR platform. Statistical analysis was performed using statistical software R 3.5 (R Foundation for Statistical Computing). | BCa screening and surveillance (detection) | Risk stratification | AUC = 0.923, PPV = 47.1%, NPV = 97.4%, Se. = 92.5%, Sp. = 73.5% | retrospective | [39] |
| S100A6, TRAM1 | diagnostic | n = 113 (HR patients = 66; control group = 47) | RNeasy Midi Kit (QIAGEN, Hilden, Germany) was used to isolate RNA from urine samples of 113 patients which then were quantified using a NanoDrop ND-1000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). Measuring of concentration and integrity of pooled urinary RNA was done with Agilent 2100 Bioanalyzer and Agilent RNA 6000 Pico Kit (Agilent Technologies, Santa Clara, CA, USA). cDNA synthesis was done with SMARTer Stranded Total RNA-Seq Kit—Pico Input Mammalian (TaKaRa Bio INC., Kusatsu, prefecture Shiga, Japan) and then purified with Agencourt AMPure XP PCR purification system (Beckman Coulter, Brea, CA, USA). The double-stranded cDNA libraries were quantified with Qubit dsDNA HS Assay Kit and the Qubit Fluorometer (Thermo Fisher Scientific, Waltham, MA, USA). DNA was sequenced by GATC Biotech AG (GATC Biotech AG, Konstanz, Germany). qPCR was performed using SYBR green and TaqMan Systems. Data analysis was performed with SDS 2.1 software (Applied Biosystems, Foster City, CA, USA). | BCa detection | No data | retrospective | [40] | |
| Xpert BCa Monitor (ABL1, ANXA10, CRH, IGF2, UPK1B) | diagnostic | n = 500 (LG = 287, HG = 194) | Cepheid GeneXpert Instrument System was used for sample processing, nucleic acid amplification, and detection of the target sequences. XLSTAT version 2020.2.2 (Addinsoft) was used for data analysis. | BCa recurrence detection | AUC = 0.73, PPV = 21.3%, NPV = 96.5%, Se. = 72.7%, Sp. = 73.7% | retrospective | [41] | |
| Xpert analysis | Diagnostic and prognostic | n = 254 (LG = 60, HG = 194) | GeneXpert system (Cepheid, Synnyvale, CA, USA) was used to detect target mRNA sequences (ABL1, ANXA, UPK1B, CRH, IGF2) in urine samples of 254 patients using RT-PCR. Data analysis performed with IBM statistica software v.20. | BCa detection | PPV = 66.4%, NPV = 88.9%, Se. = 85.9%, Sp. = 72.3% | prospective | [42] | |
| CYR61 | Prognostic and diagnostic | n = 303 (screening set = 30, LG = 12, HG = 18; validation set = 54, LG = 20, HG = 34; FFPE set = 115, LG43, HG = 32; Urine set = 104, LG = 57, HG = 47) | Total RNA was extracted from frozen tissue using TRIzol (Invitrogen, Carlsbad, CA, USA). RNA concentration was determined using a NanoDrop ND-1000 Spectrophotometer (NanoDrop Technologies, Wilmington, DE, USA). RNA’s integrity was determined using a 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA). qRT-PCR was performed with SYBR PREMIX ex Taq (TaKaRa, Dalian, China) and Mx3005p thermal cycler (Stratagene, La Jolla, CA, USA). Mouse monoclonal antibodies against CYR61 (ab80112; dilution 1:400, Abcam, Cambridge, UK) were used to stain CYR61. Urine samples of 303 patients were tested for CYR61 levels using commercial ELISA test (DY4055, R&D Systems, MN, USA). Data analysis performed with SPSS statistical package, v 17.0 (SPSS Inc., Chicago, IL, USA). | MIBC vs. NMIBC differentiation | BCa progression | AUC = 0.883, Se. = 72.7%, Sp. = 86.0% | retrospective | [43] |
| Xpert BCa monitor (ABL1, CRH, IGF2, UPK1B, ANXA10) | diagnostic | n = 139 (LG = 62, HG = 63) | Urine samples collected from 139 patients were tested with the XBCM. Data analysis peformed with Excel (Microsoft Corp., Redmond, WA, USA). | BCa detection | AUC = 0.79, PPV = 51%, NPV = 92%, Se. = 58%, Sp. = 89% | retrospective | [44] | |
| Diagnostic and surveillance | n = 139 (LG = 139) | Urine samples of 139 patients were tested with Xpert BCa Monitor (Cepheid, Sunnyvale, CA, USA). Data analysis performed with STATA® (IC 16.1; StataCorp LLC, College Station, TX, USA). | BCa detection | No data | prospective | [45] | ||
| CxBladder (MDK, HOXA13, CDC2, IGFBP5, CXCR2) | diagnostic | n = 28 (LG = 10, HG = 18) | Urine samples collected from 28 patients were sent for urine cytology and CxBladder test. Statistical analysis performed with Microsoft Excel. | BCa detection | PPV = 62%, NPV = 100%, Se. = 100%, Sp. = 75% | prospective | [46] | |
| diagnostic | n = 1411 (Development data set = 863, LG = 43, HG = 46, haematuria = 774; Independent data = 548, LG = 5, HG = 9, haematuria 534) | Quantitative reverse transcription polymerase chain reaction was used on urine of to measure the expression of 5 genotypic biomarkers (MDK, CDK1, IGFBP5, HOXA13, CXCR2). Data analysis was performed with R 3.5.1 software (R Foundation for Statistical Computing, Vienna, Austria). | Stratification of patients at low and high probability of BCa | NPV = 99.4%, Se. = 92.4%, Sp. = 93.8% | prospective | [47] |
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| Putative markers | diagnostic | n = 124 (BCa = 63, control group = 61) | Urine samples were collected from 124 patients and then derivatizated. GC-MS analysis was performed with Pegasus® 4D GC × GC-TOFMS (LECO, St. Joseph, MI, USA). Data analysis performed with ChromaTOFF® Software (LECO, St. Joseph, MI, USA). | BCa vs. hernia differentiation | AUC = 0.976 | retrospective | [52] | |
| Urinary metabolomics | diagnostic | n = 44 (BCa = 29, LG = 10, HG = 19; control group = 15) | Metabolomics analysis on urine samples of 44 paitents was conducted with the Q300 Metabolite Assay Kit (Human Metabolomics Institute, Inc., Shenzen, Guangdong, China). Ultra-performance liquid chromatography coupled to tandem mass spectrometry (ACQUITY UPLC-Xevo TQ-S, Waters Corp., Milford, MA, USA) with an electrospray ionization (ESI) source was operated under positive and negative ion modes for the quantitation of metabolites. Data analysis performed with Targeted Metabolome Batch Quantification software (v1.0, Human Metabolomics Institute, Shenzen, Guangdong, China). | BCa detection | AUC = 0.983, Se. = 95.3%, Sp. = 100% | retrospective | [53] |
| Biomarker | Purpose | Number of Patients | Method | Diagnostic Value | Prognostic Value | Predictive Capacity | Type of Study | Reference |
|---|---|---|---|---|---|---|---|---|
| VPAC | diagnostic | n = 103 (group 1 = 65, LG = 30, HG = 35; group 2 = 38, NMIBC) | Urine samples collected from 103 patients were treated with 5-aimnolevulinic acid and then tested for protoporhyrin IX using Nikon ECLIPSE NI fluorescent microscope (Nikon Corporation, Tokyo, Japan). TP4303 solution was used to identify VPAC receptors under fluorescent microscope. All patients underwent cystoscopy/biopsy/TURBT and surgical samples were examined by a pathologist and then compared to the results of conventional cytology, 5-ALA-induced fluorescent cytology, and fluorescent microscopic VPAC receptors examination. Data analysis was performed using Microsoft Excel 2019. | Detection of BCa | n/a | Se. = 89.23%, Sp. = 100% | prospective | [54] |
| utDNA | Prognostic and diagnostic | n = 57 (BCa = 42, MIBC = 32, NMIBC = 10, control group = 15) | Urine and blood sample of 57 patients acquired on the day of RT. cfDNA was isolated from urine and purified by AMPure XP (Beckman Coulter Life Sciences, Indianapolis, IN, USA) and then analyzed by Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA). utDNA detection using urine Cancer Personalized Profiling by Deep Sequencing (uCAPP-Seq). Data analysis performed with RStudio v1.1.463 environment (RStudio, Boston, MA, USA) and Prism 8 (GraphPad Software, San Diego, CA, USA). | MRD detection | Predicting FPS and OS | AUC = 0.78, PPV = 88%, NPV = 72%, Se. = 81%, Sp. = 81% | Retrospective | [55] |
| CP | diagnostic | n = 273 (cohort 1 = 97; cohort 2 = 176) | Urine collected from 273 patients was measured for CP levels using commercial ELISA kit (R&D systems, Minneapolis, MN, USA). Data analysis was performed using StatView (v 5.0, Abacus Concepts, Berkeley, CA, USA) | BCa progression | No data | retrospective | [56] | |
| MTC-PCR | prognostic | n = 123 (LG = 37, HG = 86) | Urine samples of 123 patients collected after TURBT and before initiation of BCG instillation, and every year after the last BCG instillation, including induction and maintenance for up to 10 yr. DNA was purified from the pellet using a QIAamp DNA kit (Qiagen, Hilden, Germany). MTC-PCR was used to detect the presence of mycobacterial DNA in urine samples. Statistical analysis performed with R software v.3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). | BCa progression and recurrence | Progression AUC = 0.875 Se. = 83.3%, Sp. = 91.5% Recurrence AUC = 0.868, Se. = 75%, Sp. = 100% | [57] | ||
| Multiple Chromatographic Analysis (Fluorescent peak F) | diagnostic | n = 47 (BCa = 23, LG = 19, HG = 4; NMHU = 24) | Urine collected from 47 patients was filtered using a 0.22um nylon membrane filter-LLG Syringe Filter PTFE (AZ chrome, Bratislava, Slovak Republic). Urines samples were analyzed using RP-HPLC system Prominence 20A (Shimadzu Co., Kyoto, Japan). Data analysis was performed using Software LC solution (Shimadzu Co., Kyoto, Japan). | BCa vs. NMHU differentiation | AUC = 0.824, PPV = 78%, NPV = 88%, Se. = 90%, Sp. = 74% | retrospective | [59] | |
| miR-34a-5p, miR-205-3p, miR-210-3p | diagnostic | n = 147 (prospective: BCa = 15, NMIBC = 12, MIBC = 3, LG = 8, HG = 7; control group = 16; retrospective: BCa = 66, NMIBC = 56, MIBC = 10, LG = 25, HG = 41; control group = 50) | BenchMark XT immunostainer (Ventana Medycal Sysems, Tucson, AZ, USA) was used for immunohistochemical staining of tissue samples. The stains were inspected using an Olympus BX50 and Olympus BX46 mucroscopes (Olympus Europe) by two pathologists. Total RNA was extracted from urine supernatant samples of 116 patients using the Urine microRNA Purification kit (Norgen Biotek, Thorold, Canada). RNA concentration was quantified by Invitrogen Qubit® 4 Fluorometer with Qubit® microRNA Assay Kit (Invitrogen, Milan, Italy). Small RNA transcripts were converted into barcoded cDNA libraries with the NEBNext Multiplex Small RNA Library Prep Set for Illumina (New England Biolabs, Ipswich, MA, USA) and run on Illumina NextSeq 500 platform (Illumina, San Diego, CA, USA). Differential expression analysis was performed with DESeq2 Bioconductor’s package (version 1.22.2). miRNA biomarkers were replicated using miRCURY LNA miRNA PCR Assays (Qiagen, Milan, Italy). Reverse transcription was performed using the miRCURY LNA RT kit (Qiagen, Milan, Italy). Functional enrichment analysis of miRNA target genes was performed using RBiomirGS v0.2.12. Data analysis was performed using Graphpad Prism 8 sofware (Graphpad Software, San Diego, CA, USA) and Quasar-Orange software (Bioinformatics Laboratory of the University of Ljubljana). | BCa detection | AUC = 0.92 | Prospective and retrospective | [60] | |
| Urinary VOC analysis | Diagnostic and surveillance | n = 305 (BCa = 96, Control group = 209) | Urine samples of 305 patients were collected before cystoscopy. Sulphuric acid solution (Fisher Scientific, Waltham, MA, USA) was added to urine. A PerkinElmer Clarus 500 GC-MS single quadrupole system (PerkinElmer, Waltham, MA, USA) and PAL COMBI-xt autosampler (CTC Analytics, Zwingen, Switzerland) were used to analyse samples. Data analysis performed with Metaboanalyst. | BCa detection | Eight-Voc diagnostic biomarker AUC = 0.77, Se. = 71%, Sp. = 72% Six-VOC surveillace biomarker AUC = 0.80, Se. = 71%, Sp. = 80% | retrospective | [61] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matuszczak, M.; Kiljańczyk, A.; Salagierski, M. A Liquid Biopsy in Bladder Cancer—The Current Landscape in Urinary Biomarkers. Int. J. Mol. Sci. 2022, 23, 8597. https://doi.org/10.3390/ijms23158597
Matuszczak M, Kiljańczyk A, Salagierski M. A Liquid Biopsy in Bladder Cancer—The Current Landscape in Urinary Biomarkers. International Journal of Molecular Sciences. 2022; 23(15):8597. https://doi.org/10.3390/ijms23158597
Chicago/Turabian StyleMatuszczak, Milena, Adam Kiljańczyk, and Maciej Salagierski. 2022. "A Liquid Biopsy in Bladder Cancer—The Current Landscape in Urinary Biomarkers" International Journal of Molecular Sciences 23, no. 15: 8597. https://doi.org/10.3390/ijms23158597
APA StyleMatuszczak, M., Kiljańczyk, A., & Salagierski, M. (2022). A Liquid Biopsy in Bladder Cancer—The Current Landscape in Urinary Biomarkers. International Journal of Molecular Sciences, 23(15), 8597. https://doi.org/10.3390/ijms23158597