
Expression of NUCB2/NESF-1 in Breast Cancer Cells

 , and
, and
Abstract
:1. Introduction
2. Results
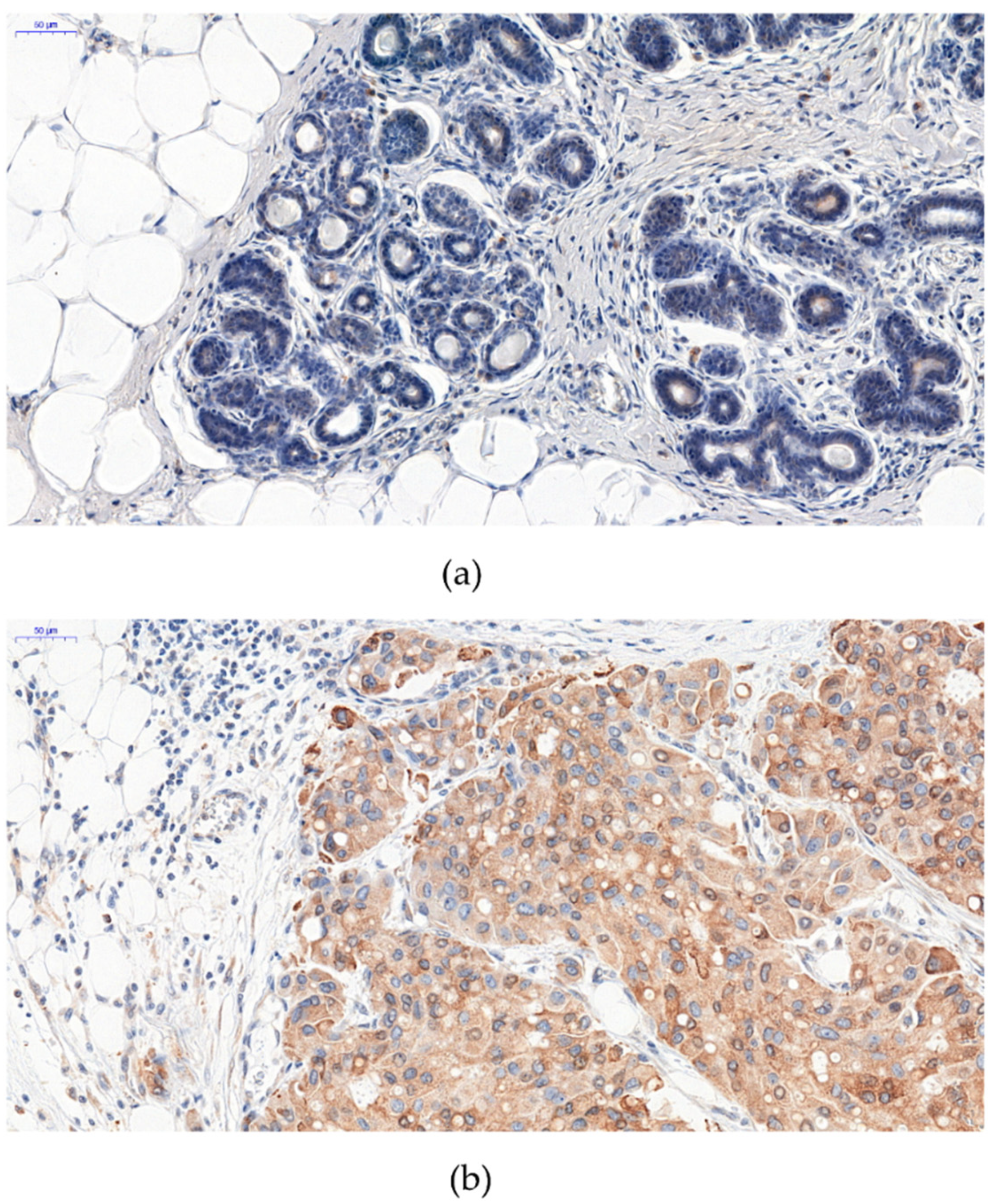
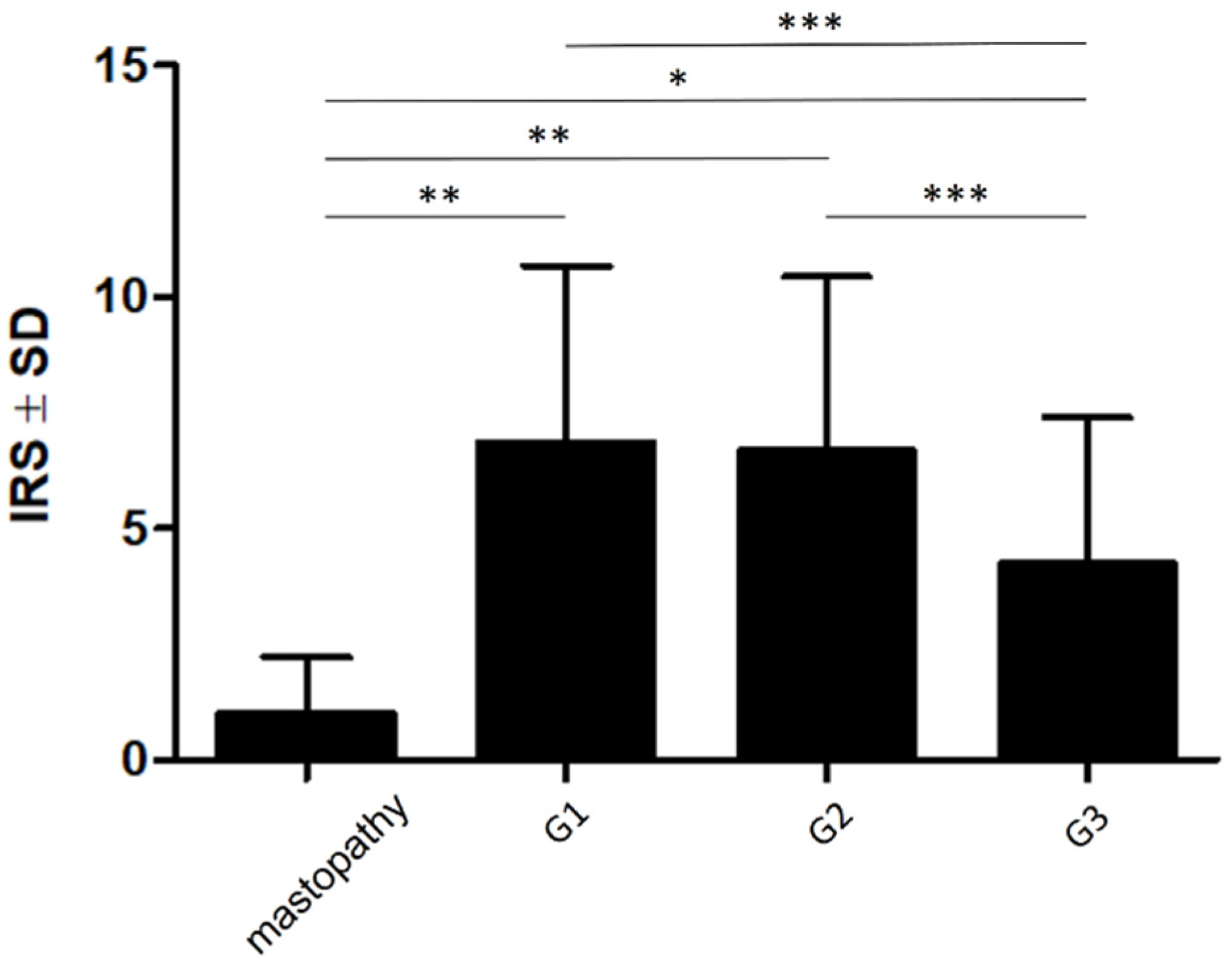
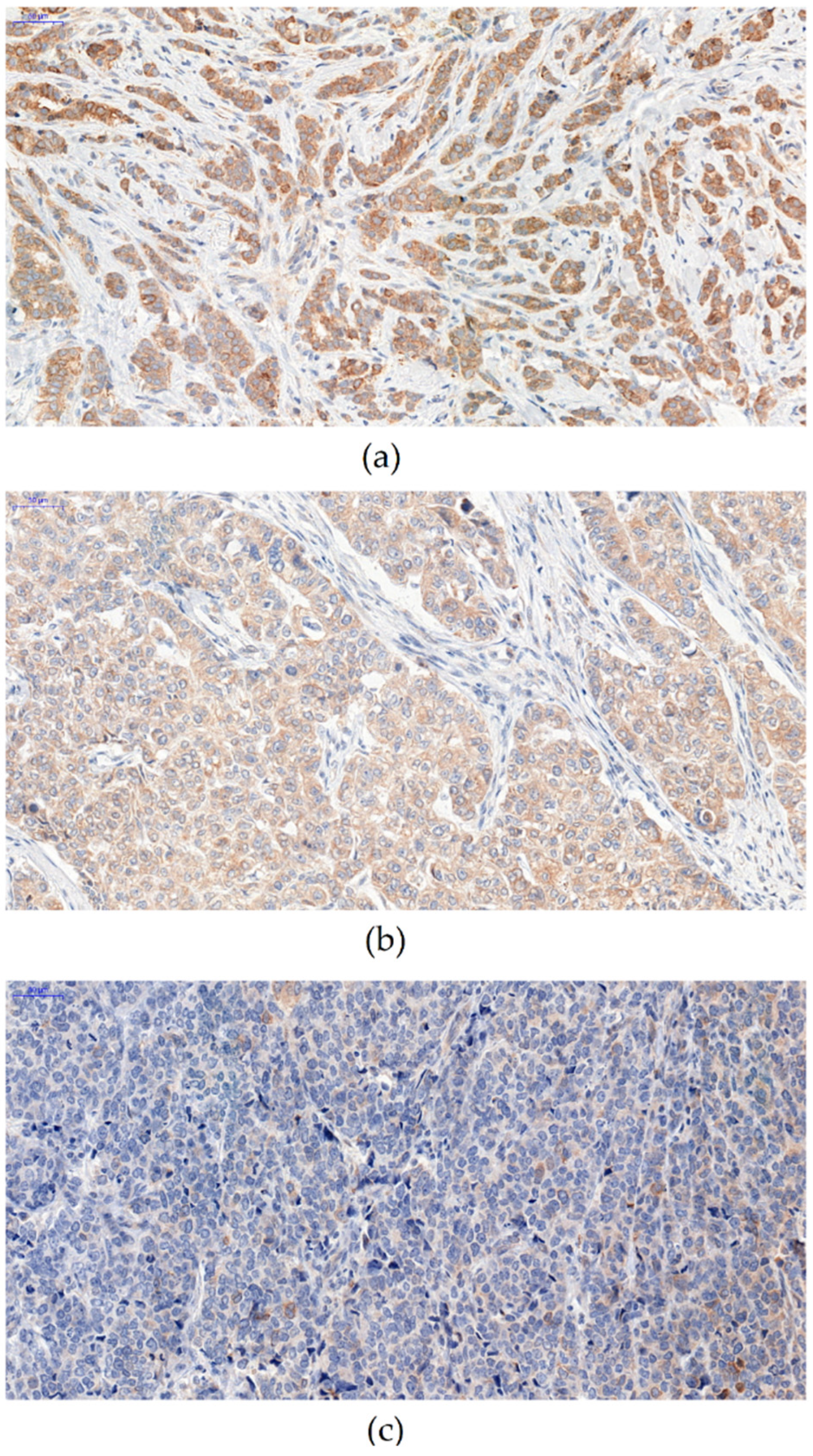
2.1. Immunohistochemical Analysis of NUCB2 Protein Expression in BC and Mastopathy
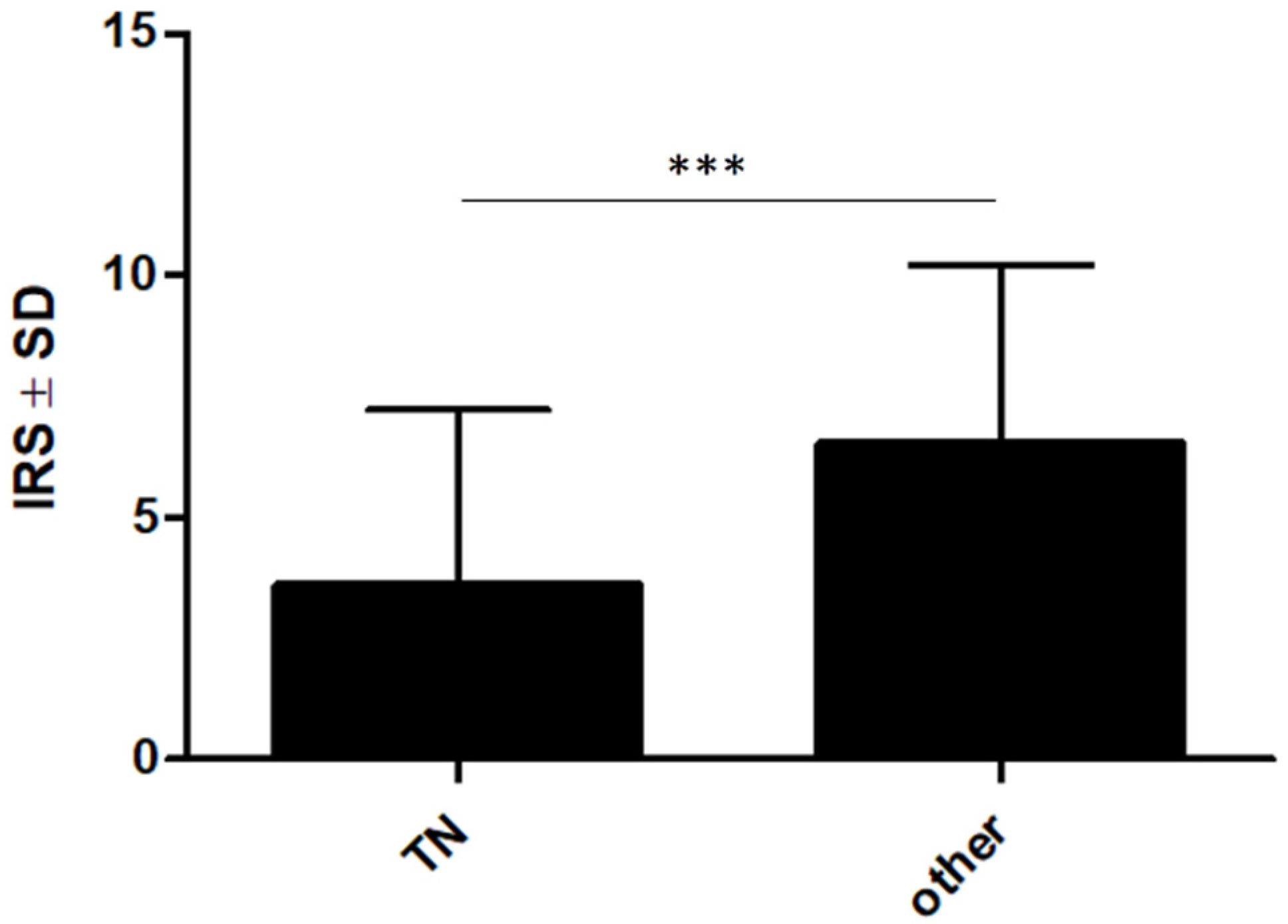
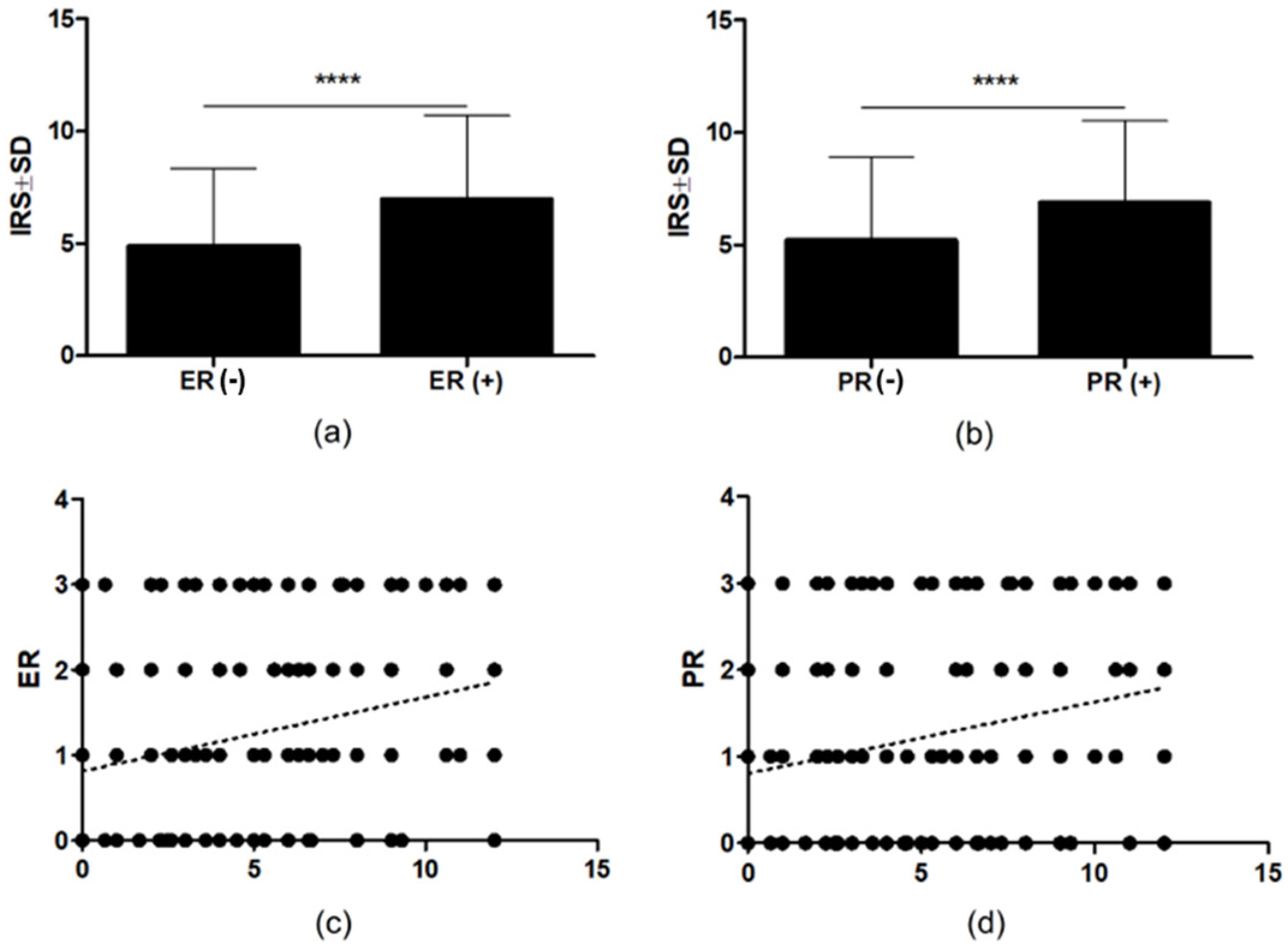
2.2. The Associations between NUCB2 Expression and Clinicopathological Parameters
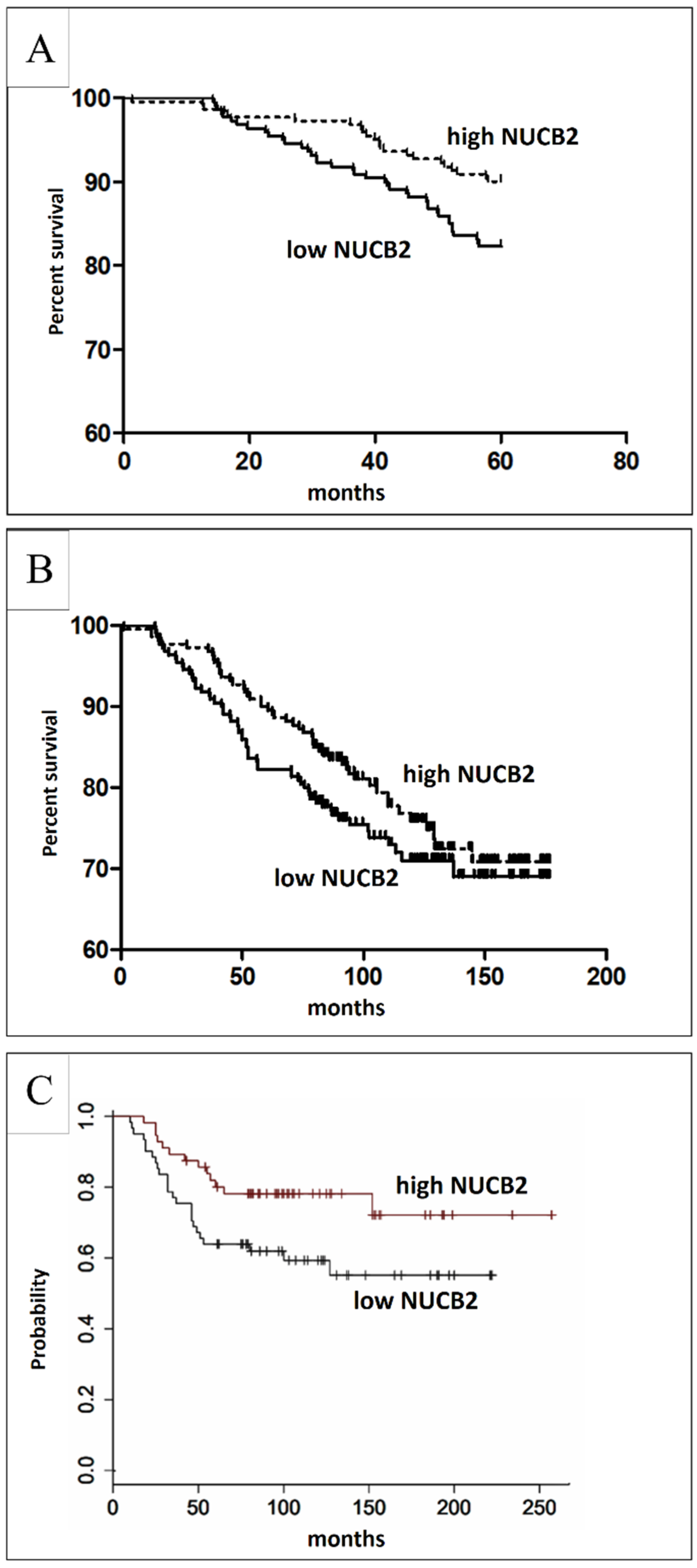
2.3. The Associations between NUCB2 Expression and IDC Patient Survival
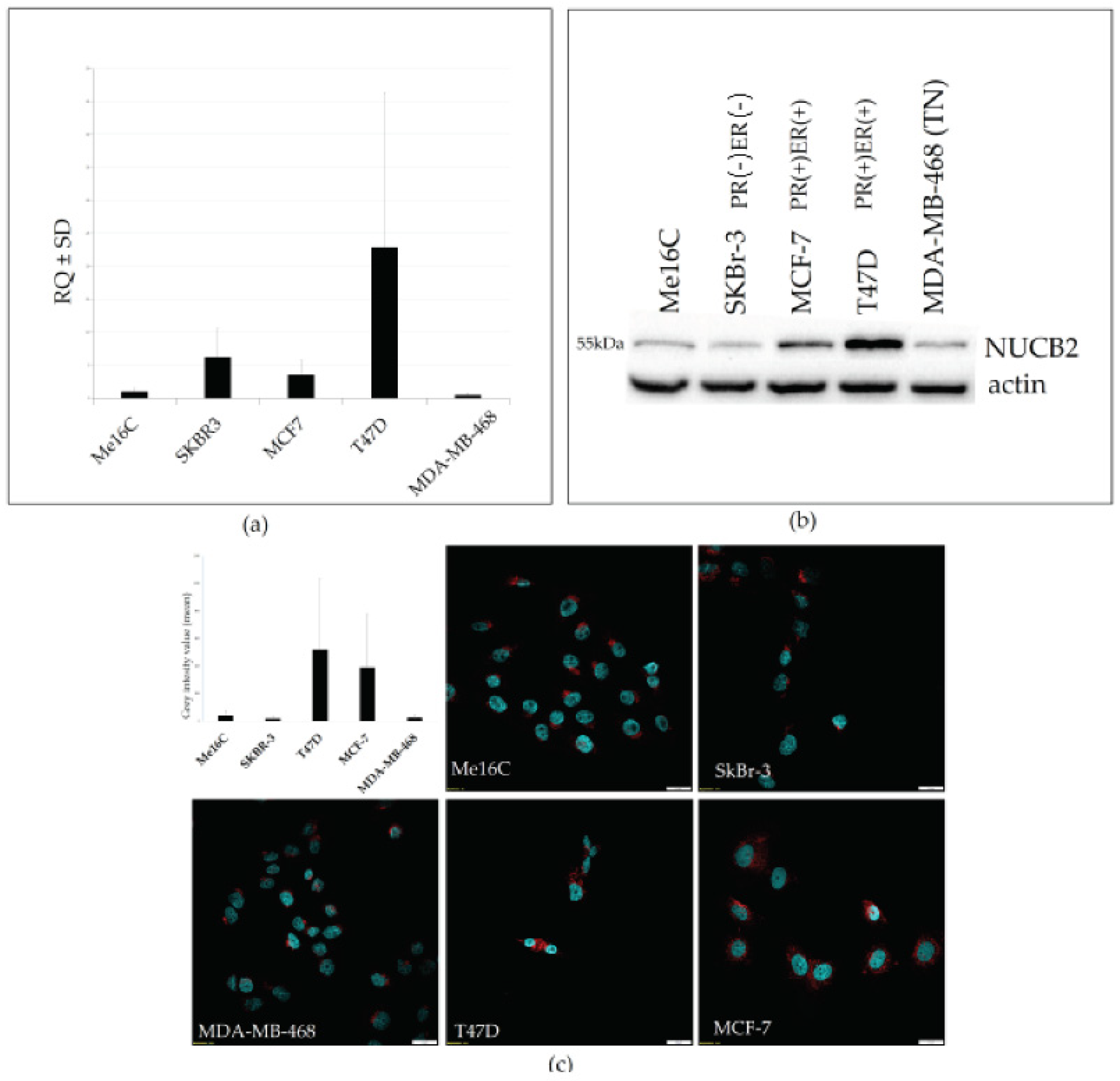
2.4. Expression of NUCB2 in Breast Cancer Cell Lines
3. Discussion
4. Materials and Methods
4.1. Patient Cohort
4.2. Immunohistochemistry (IHC)
4.3. RNA Isolation, cDNA Synthesis and Real-Time PCR
4.4. Confocal Microscopy
4.5. Western Blot (WB) Analysis
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mr, A.; Sharifi, J.M.; Paknahad, P. A Breast Cancer and Associated Factors: A Review. J. Med. Life 2015, 8, 6–11. [Google Scholar]
- Becker, S. A Historic and Scientific Review of Breast Cancer: The next Global Healthcare Challenge. Int. J. Gynecol. Obstet. 2015, 131, S36–S39. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.K.; Zetter, B.R. Cancer Biomarkers: Knowing the Present and Predicting the Future. Future Oncol. 2005, 1, 37–50. [Google Scholar] [CrossRef]
- Kmiecik, A.M.; Dzięgiel, P.; Podhorska-Okołów, M. Nucleobindin-2/Nesfatin-1—A New Cancer Related Molecule? Int. J. Mol. Sci. 2021, 22, 8313. [Google Scholar] [CrossRef]
- Oh-I, S.; Shimizu, H.; Satoh, T.; Okada, S.; Adachi, S.; Inoue, K.; Eguchi, H.; Yamamoto, M.; Imaki, T.; Hashimoto, K.; et al. Identification of Nesfatin-1 as a Satiety Molecule in the Hypothalamus. Nature 2006, 443, 709–712. [Google Scholar] [CrossRef]
- Angelone, T.; Filice, E.; Pasqua, T.; Amodio, N.; Galluccio, M.; Montesanti, G.; Quintieri, A.M.; Cerra, M.C. Nesfatin-1 as a Novel Cardiac Peptide: Identification, Functional Characterization, and Protection against Ischemia/Reperfusion Injury. Cell. Mol. Life Sci. 2013, 70, 495–509. [Google Scholar] [CrossRef]
- Foo, K.S.; Brauner, H.; Östenson, C.G.; Broberger, C. Nucleobindin-2/Nesfatin in the Endocrine Pancreas: Distribution and Relationship to Glycaemic State. J. Endocrinol. 2010, 204, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Ramanjaneya, M.; Chen, J.; Brown, J.E.; Tripathi, G.; Hallschmid, M.; Patel, S.; Kern, W.; Hillhouse, E.W.; Lehnert, H.; Tan, B.K.; et al. Identification of Nesfatin-1 in Human and Murine Adipose Tissue: A Novel Depot-Specific Adipokine with Increased Levels in Obesity. Endocrinology 2010, 151, 3169–3180. [Google Scholar] [CrossRef] [PubMed]
- Stengel, A.; Hofmann, T.; Goebel-Stengel, M.; Lembke, V.; Ahnis, A.; Elbelt, U.; Lambrecht, N.W.G.; Ordemann, J.; Klapp, B.F.; Kobelt, P. Ghrelin and NUCB2/Nesfatin-1 Are Expressed in the Same Gastric Cell and Differentially Correlated with Body Mass Index in Obese Subjects. Histochem. Cell Biol. 2013, 139, 909–918. [Google Scholar] [CrossRef]
- Miura, K.; Titani, K.; Kurosawa, Y.; Kanai, Y. Molecular Cloning of Nucleobindin, a Novel DNA-Binding Protein That Contains Both a Signal Peptide and a Leucine Zipper Structure. Biochem. Biophys. Res. Commun. 1992, 187, 375–380. [Google Scholar] [CrossRef]
- Taniguchi, N.; Taniura, H.; Niinobe, M.; Takayama, C.; Tominaga-Yoshino, K.; Ogura, A.; Yoshikawa, K. The Postmitotic Growth Suppressor Necdin Interacts with a Calcium-Binding Protein (NEFA) in Neuronal Cytoplasm. J. Biol. Chem. 2000, 275, 31674–31681. [Google Scholar] [CrossRef] [PubMed]
- Feijóo-Bandín, S.; Rodríguez-Penas, D.; García-Rúa, V.; Mosquera-Leal, A.; Otero, M.F.; Pereira, E.; Rubio, J.; Martínez, I.; Seoane, L.M.; Gualillo, O.; et al. Nesfatin-1 in Human and Murine Cardiomyocytes: Synthesis, Secretion, and Mobilization of GLUT-4. Endocrinology 2013, 154, 4757–4767. [Google Scholar] [CrossRef] [PubMed]
- Navarro, V.M.; Gaytan, F.; Tena-sempere, M. Expanding Roles of NUCB2/Nesfatin-1 in Neuroendocrine Regulation. J. Mol. Endocrinol. 1992, 45, 281–290. [Google Scholar] [CrossRef]
- Khalili, S.; Shekari Khaniani, M.; Afkhami, F.; Mansoori Derakhshan, S. NUCB2/Nesfatin-1: A Potent Meal Regulatory Hormone and Its Role in Diabetes. Egypt. J. Med. Hum. Genet. 2017, 18, 105–109. [Google Scholar] [CrossRef]
- Lago, F.; Scotece, M.; Conde, J.; Abella, V.; Lo, V. NUCB2/Nesfatin-1: A New Adipokine Expressed in Human and Murine Chondrocytes with Pro-Inflammatory Properties, An In Vitro Study. J. Orthop. Res. 2014, 32, 653–660. [Google Scholar] [CrossRef]
- Altan, B.; Kaira, K.; Okada, S.; Saito, T.; Yamada, E.; Bao, H.; Bao, P.; Takahashi, K.; Yokobori, T.; Tetsunari, O.; et al. High Expression of Nucleobindin 2 Is Associated with Poor Prognosis in Gastric Cancer. Tumor Biol. 2017, 39, 1–7. [Google Scholar] [CrossRef]
- Cho, J.M.; Moon, K.T.; Lee, H.J.; Shin, S.C.; Choi, J.D.; Kang, J.Y.; Yoo, T.K. Nucleobindin 2 Expression Is an Independent Prognostic Factor for Bladder Cancer. Medicine 2020, 13, e19597. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Zhu, Y.; Wang, Y.; Liu, Z.; Zhang, J. High NUCB2 Expression Level Represents an Independent Negative Prognostic Factor in Chinese Cohorts of Non-Metastatic Clear Cell Renal Cell Carcinoma Patients. Oncotarget 2017, 8, 35244–35254. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Miki, Y.; Tanaka, S.; Hashimoto, C.; Watanabe, M.; Sasano, H.; Ito, K.; Suzuki, T. Nucleobindin 2 (NUCB2) in Human Endometrial Carcinoma: A Potent Prognostic Factor Associated with Cell Proliferation and Migration. Endocr. J. 2016, 63, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Chen, L.; Chen, W. High NUCB2 Expression Level Is Associated with Metastasis and May Promote Tumor Progression in Colorectal Cancer. Oncol. Lett. 2018, 15, 9188–9194. [Google Scholar] [CrossRef]
- Liu, G.-M.; Xu, Z.-Q.; Ma, H.-S. Nesfatin-1/Nucleobindin-2 Is a Potent Prognostic Marker and Enhances Cell Proliferation, Migration, and Invasion in Bladder Cancer. Dis. Markers 2018, 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.J.; Lv, J.X.; Liu, J.; Zhang, X.B.; Wang, L.B. Nucleobindin-2 Promotes the Growth and Invasion of Glioblastoma. Cancer Biother. Radiopharm. 2019, 34, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Takagi, K.; Miki, Y.; Onodera, Y.; Akahira, J.I.; Ebata, A.; Ishida, T.; Watanabe, M.; Sasano, H.; Suzuki, T. Nucleobindin 2 in Human Breast Carcinoma as a Potent Prognostic Factor. Cancer Sci. 2012, 103, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Xu, H.; Shi, Q.; Li, L.; Zhou, J.; Yu, G.; Xu, B.; Liu, Y.; Wang, Z. Nucleobindin 2 (NUCB2) in Renal Cell Carcinoma: A Novel Factor Associated with Tumor Development. Int. J. Clin. Exp. Med. 2019, 12, 8686–8693. [Google Scholar]
- Press, D. High Expression of NUCB2 Promotes Papillary Thyroid Cancer Cells Proliferation and Invasion. OncoTargets Ther. 2019, 12, 1309–1318. [Google Scholar]
- Ramanjaneya, M.; Tan, B.K.; Rucinski, M.; Kawan, M.; Hu, J.; Kaur, J.; Patel, V.H.; Malendowicz, L.K.; Komarowska, H.; Lehnert, H.; et al. Nesfatin-1 Inhibits Proliferation and Enhances Apoptosis of Human Adrenocortical H295R Cells. J. Endocrinol. 2015, 226, 1–11. [Google Scholar] [CrossRef]
- Xu, Y.; Pang, X.; Dong, M.; Wen, F.; Zhang, Y. Nesfatin-1 Inhibits Ovarian Epithelial Carcinoma Cell Proliferation in Vitro. Biochem. Biophys. Res. Commun. 2013, 440, 467–472. [Google Scholar] [CrossRef]
- Islam, A.; Adamik, B.; Hawari, F.I.; Ma, G.; Rouhani, F.N.; Zhang, J.; Levine, S.J. Extracellular TNFR1 Release Requires the Calcium-Dependent Formation of a Nucleobindin 2-ARTS-1 Complex. J. Biol. Chem. 2006, 281, 6860–6873. [Google Scholar] [CrossRef]
- Ham, B.; Fernandez, M.C.; D’Costa, Z.; Brodt, P. The Diverse Roles of the TNF Axis in Cancer Progression and Metastasis. Trends Cancer Res. 2016, 11, 1–27. [Google Scholar]
- Locksley, R.M.; Killeen, N.; Lenardo, M.J. The TNF and TNF Receptor Superfamilies: Integrating Mammalian Biology. Cell 2001, 104, 487–501. [Google Scholar] [CrossRef]
- Györffy, B.; Lanczky, A.; Eklund, A.C.; Denkert, C.; Budczies, J.; Li, Q.; Szallasi, Z. An Online Survival Analysis Tool to Rapidly Assess the Effect of 22,277 Genes on Breast Cancer Prognosis Using Microarray Data of 1,809 Patients. Breast Cancer Res. Treat. 2010, 123, 725–731. [Google Scholar] [CrossRef]
- Bystranowska, D.; Skorupska, A.; Sołtys, K.; Padjasek, M.; Krężel, A.; Żak, A.; Kaus-Drobek, M.; Taube, M.; Kozak, M.; Ożyhar, A. Nucleobindin-2 Consists of Two Structural Components: The Zn2+-Sensitive N-Terminal Half, Consisting of Nesfatin-1 and -2, and the Ca2+-Sensitive C-Terminal Half, Consisting of Nesfatin-3. Comput. Struct. Biotechnol. J. 2021, 19, 4300–4318. [Google Scholar] [CrossRef] [PubMed]
- Dore, R.; Levata, L.; Lehnert, H.; Schulz, C. Nesfatin-1: Functions and Physiology of a Novel Regulatory Peptide. J. Endocrinol. 2006, 232, R45–R65. [Google Scholar] [CrossRef] [PubMed]
- Tymicki, G.; Puzio, I.; Pawłowska-olszewska, M. Nesfatyna-1–Hormon o Działaniu Plejotropowym. Med. Weter 2019, 76, 1–9. [Google Scholar]
- Zeng, L.; Zhong, J.; He, G.; Li, F.; Li, J.; Zhou, W.; Liu, W.; Zhang, Y.; Huang, S.; Liu, Z.; et al. Identification of Nucleobindin-2 as a Potential Biomarker for Breast Cancer Metastasis Using ITRAQ-Based Quantitative Proteomic Analysis. J. Cancer 2017, 8, 3062–3069. [Google Scholar] [CrossRef] [PubMed]
- Carriaga, M.T.; Henson, D.E. The Histologic Grading of Cancer. Cancer 1995, 75, 406–421. [Google Scholar] [CrossRef]
- Koh, J.; Kim, M.J. Introduction of a New Staging System of Breast Cancer for Radiologists: An Emphasis on the Prognostic Stage. Korean J. Radiol. 2019, 20, 69–82. [Google Scholar] [CrossRef]
- Zhang, H.; Qi, C.; Li, L.; Luo, F.; Xu, Y. Clinical Significance of NUCB2 MRNA Expression in Prostate Cancer. J. Exp. Clin. Cancer Res. 2013, 32, 1–6. [Google Scholar] [CrossRef]
- Markowska, A.; Szarszewska, M.; Knapp, P.; Grybos, A.; Grybos, M.; Marszalek, A.; Filas, V.; Wojcik-krowiranda, K.; Swornik, M. The Role of Nesfatin and Selected Molecular Factors in Various Types of Endometrial Cancer. Ginekol. Polska 2019, 90, 571–576. [Google Scholar] [CrossRef]
- Lumachi, F.; Brunello, A.; Maruzzo, M.; Basso, U.; Basso, S. Treatment of Estrogen Receptor-Positive Breast Cancer. Curr. Med. Chem. 2013, 20, 596–604. [Google Scholar] [CrossRef]
- Moasser, M.M. The Oncogene HER2: Its Signaling and Transforming Functions and Its Role in Human Cancer Pathogenesis. Oncogene 2007, 26, 6469–6487. [Google Scholar] [CrossRef] [PubMed]
- Hilton, H.N.; Clarke, C.L.; Graham, J.D. Estrogen and Progesterone Signalling in the Normal Breast and Its Implications for Cancer Development. Mol. Cell. Endocrinol. 2018, 466, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-Negative Breast Cancer Molecular Subtyping and Treatment Progress. Breast Cancer Res. 2020, 22, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.; Yen, M.; Wang, J.; Wu, D. Nesfatin-1/Nucleobindin-2 Enhances Cell Migration, Invasion, and Epithelial-Mesenchymal Transition via LKB1/AMPK/TORC1/ZEB1 Pathways in Colon Cancer. Oncotarget 2016, 7, 31336. [Google Scholar] [CrossRef]
- Ranjan, A.; Choubey, M.; Yada, T.; Krishna, A. Immunohistochemical Localization and Possible Functions of Nesfatin-1 in the Testis of Mice during Pubertal Development and Sexual Maturation. J. Mol. Histol. 2019, 50, 533–549. [Google Scholar] [CrossRef]
- Ranjan, A.; Choubey, M.; Yada, T.; Krishna, A. Nesfatin-1 Ameliorates Type-2 Diabetes-Associated Reproductive Dysfunction in Male Mice. J. Endocrinol. Investig. 2020, 43, 515–528. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Parameters | Breast Cancer | |
|---|---|---|
| Univariate Analysis HR (95% CI) p | Multivariate Analysis HR (95% CI) p | |
| Grade (G1 vs. G2-G3) | 1.02 (0.9–1.0) 0.079196 | |
| pT (1–2 vs. 3–4) | 2.07 (1.5–2.7) <0.0001 | 1.68 (1.21–2.33) <0.01 |
| pN (0 vs. 1–3) | 1.41 (0.9–2.1) 0.109256 | |
| Stage (1–2 vs. 3–4) | 4.23 (2.3–7.5) <0.0001 | 2.15 (1.04–4.45) <0.05 |
| ER (0 vs. 1–3) | 0.77 (0.5–1.1) 0.123913 | |
| PR (0 vs. 1–3) | 0.72 (0.5–1.0) 0.05778937 | |
| HER-2 (0–2 vs. 3) | 1.49 (0.7–2.9) 0.238655 | |
| NUCB2 (median) | 0.78 (0.5–1.1) 0.2096233 | |
| NUCB2 (0 vs. 1–12) | 0.74 (0.4–1.4) 0.3487976 | |
| Parameters | No. | % |
|---|---|---|
| Age (years) | ||
| ≤66 | 239 | 54 |
| >66 | 207 | 46 |
| Tumor size | ||
| T1 | 259 | 62 |
| T2 | 145 | 35 |
| T3 | 2 | 0 |
| T4 | 9 | 2 |
| Grade | ||
| G1 | 66 | 15 |
| G2 | 291 | 68 |
| G3 | 70 | 16 |
| Lymph nodes | ||
| N0 | 255 | 63 |
| N1, N2, N3 | 153 | 38 |
| ER | ||
| Positive | 302 | 68 |
| Negative | 142 | 100 |
| PR | ||
| Positive | 294 | 66 |
| Negative | 150 | 34 |
| TNM | ||
| I | 179 | 44 |
| II | 213 | 52 |
| III | 17 | 4 |
| HER2 | ||
| Positive | 31 | 11 |
| Negative | 245 | 89 |
| Triple negative | ||
| Yes | 30 | 7 |
| No | 401 | 93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kmiecik, A.; Ratajczak-Wielgomas, K.; Grzegrzółka, J.; Romanowicz, H.; Smolarz, B.; Dziegiel, P. Expression of NUCB2/NESF-1 in Breast Cancer Cells. Int. J. Mol. Sci. 2022, 23, 9177. https://doi.org/10.3390/ijms23169177
Kmiecik A, Ratajczak-Wielgomas K, Grzegrzółka J, Romanowicz H, Smolarz B, Dziegiel P. Expression of NUCB2/NESF-1 in Breast Cancer Cells. International Journal of Molecular Sciences. 2022; 23(16):9177. https://doi.org/10.3390/ijms23169177
Chicago/Turabian StyleKmiecik, Alicja, Katarzyna Ratajczak-Wielgomas, Jędrzej Grzegrzółka, Hanna Romanowicz, Beata Smolarz, and Piotr Dziegiel. 2022. "Expression of NUCB2/NESF-1 in Breast Cancer Cells" International Journal of Molecular Sciences 23, no. 16: 9177. https://doi.org/10.3390/ijms23169177
APA StyleKmiecik, A., Ratajczak-Wielgomas, K., Grzegrzółka, J., Romanowicz, H., Smolarz, B., & Dziegiel, P. (2022). Expression of NUCB2/NESF-1 in Breast Cancer Cells. International Journal of Molecular Sciences, 23(16), 9177. https://doi.org/10.3390/ijms23169177