

Anti-Inflammatory Drug Therapy in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis of Prospective Randomized, Double-Blind and Placebo-Controlled Trials




Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Types of Studies
2.3. Data Extraction and Quality Evaluation
2.4. Statistics
2.5. Grading of the Evidence
3. Results and Discussion
3.1. Literature Search
3.2. Characteristics of Included Studies
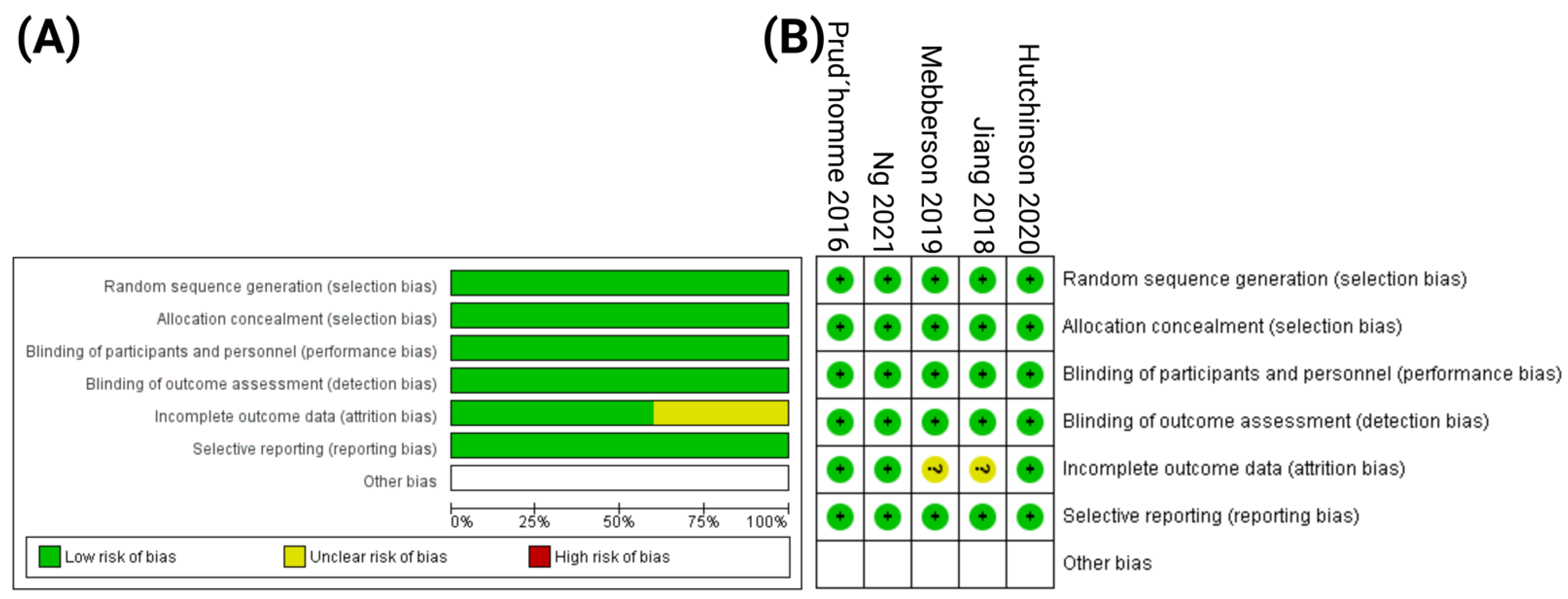
3.3. Risk of Bias Quality Assessment
3.4. Impact of Anti-Inflammatory Therapy on Patients with cSDH
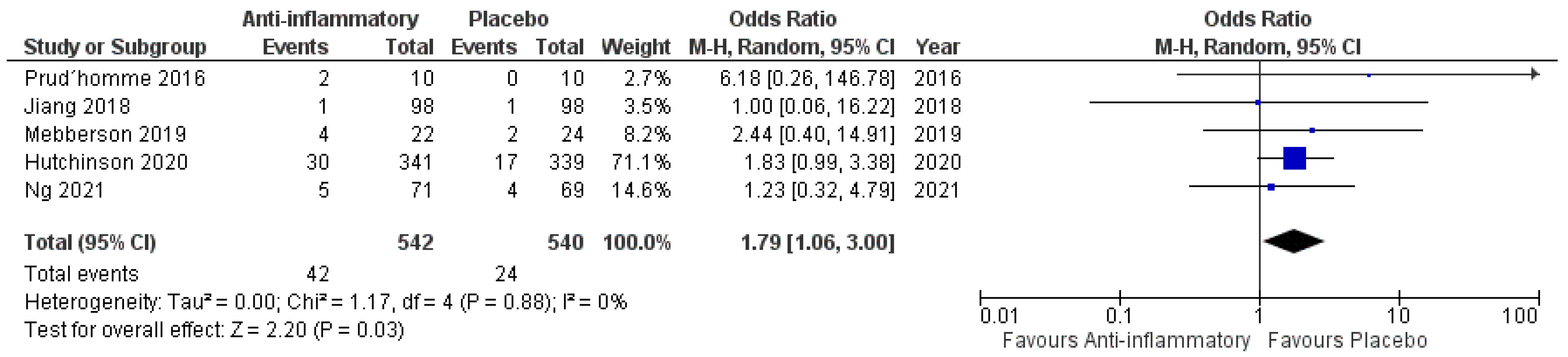
3.4.1. Mortality
3.4.2. Neurological Outcome
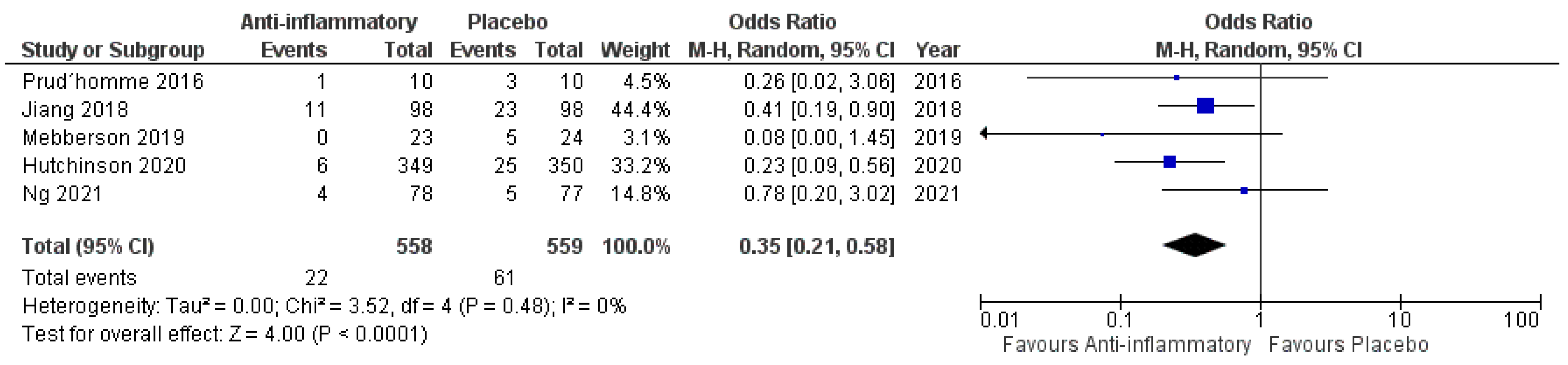
3.4.3. Secondary Surgery for Recurrent cSDH
3.5. Impact of Anti-Inflammatory Therapy on Patients with cSDH Undergoing Primary Surgical Hematoma Evacuation
3.5.1. Mortality
3.5.2. Outcome
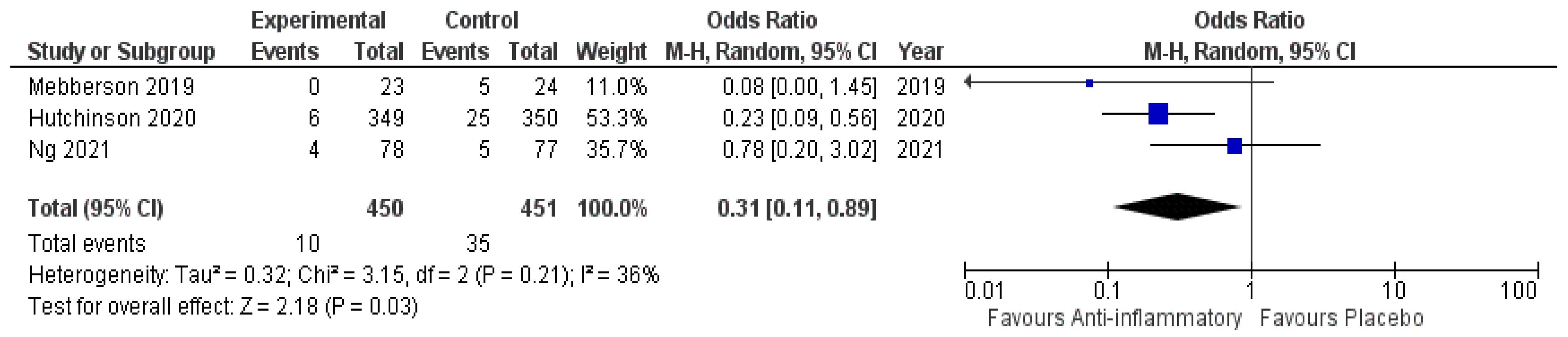
3.5.3. Secondary Surgery for Recurrent cSDH
3.6. Impact of Anti-Inflammatory Therapy on Patients with cSDH and Primary Conservative Treatment
3.6.1. Mortality
3.6.2. Outcome
3.6.3. Secondary Surgery
3.7. Impact of Corticosteroids on Patients with cSDH
3.7.1. Mortality
3.7.2. Secondary Surgery
3.8. High-Dose vs. Low Dose Corticosteroids—Mortality
3.8.1. Low Dose Corticosteroids
3.8.2. High Dose Corticosteroids
3.9. Publication Bias
3.10. Grading of the Evidence
3.11. Discussion
Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stubbs, D.J.; Vivian, M.E.; Davies, B.M.; Ercole, A.; Burnstein, R.; Joannides, A.J. Incidence of chronic subdural haematoma: A single-centre exploration of the effects of an ageing population with a review of the literature. Acta Neurochir. 2021, 163, 2629–2637. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Ebel, H.; Ernestus, R.I.; Klug, N. Various surgical treatments of chronic subdural hematoma and outcome in 172 patients: Is membranectomy necessary? Surg. Neurol. 2004, 61, 523–528. [Google Scholar] [CrossRef]
- Santarius, T.; Kirkpatrick, P.J.; Ganesan, D.; Chia, H.L.; Jalloh, I.; Smielewski, P.; Richards, H.K.; Marcus, H.; Parker, R.A.; Price, S.J.; et al. Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: A randomized controlled trial. Lancet 2009, 374, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Güresir, A.; Coch, C.; Heine, A.; Mass, E.; Lampmann, T.; Vatter, H.; Velten, M.; Schmitz, M.T.; Güresir, E.; Wach, J. Red Blood Cell Distribution Width to Platelet Count Ratio Facilitates Preoperative Prediction of Recurrence in Surgically Treated Chronic Subdural Hematoma. Front. Neurol. 2022, 13, 884231. [Google Scholar] [PubMed]
- Schucht, P.; Fischer, U.; Fung, C.; Bernasconi, C.; Fichtner, J.; Vulcu, S.; Schöni, D.; Nowacki, A.; Wanderer, S.; Eisenring, C.; et al. Follow-up Computed Tomography after Evacuation of Chronic Subdural Hematoma. N. Engl. J. Med. 2019, 380, 1186–1187. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, G.; Caroli, E.; Salvati, M.; Delfini, R. Membranectomy in organized chronic subdural hematomas: Indications and technical notes. Surg. Neurol. 2007, 67, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Markwalder, T.M. Chronic subdural haematoma: A review. J. Neurosurg. 1981, 54, 637–645. [Google Scholar] [CrossRef]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural hematoma: Inflammation. angiogenesis and implications for pharmacotherapy. J. Neuroinflam. 2017, 14, 108. [Google Scholar] [CrossRef] [Green Version]
- Shono, T.; Inamura, T.; Morioka, T. Vascular endothelial growth factor in chronic subdural haematomas. J. Clin. Neurosci. 2001, 8, 411–415. [Google Scholar] [CrossRef]
- Nanko, N.; Tanikawa, M.; Mase, M.; Fujita, M.; Tateyama, H.; Miyati, T.; Yamada, K. Involvement of hypoxia-inducible factor-1alpha and vascular endothelial growth factor in the mechanism of development of chronic subdural hematoma. Neurol. Med. Chir. 2009, 49, 379–385. [Google Scholar] [CrossRef]
- Hohenstein, A.; Erber, R.; Schilling, L.; Weigel, R. Increased mRNA expression of VEGF within the hematoma and imbalance of angiopoietin-1 and-2 mRNA within the neomembranes of chronic subdural hematoma. J. Neurotrauma 2005, 22, 518–528. [Google Scholar] [CrossRef]
- Hong, H.J.; Kim, Y.J.; Yi, H.J.; Ko, Y.; Oh, S.J.; Kim, J.M. Role of angiogenetic growth factors and inflammatory cytokine on recurrence of chronic subdural hematoma. Surg. Neurol. 2009, 71, 161–165. [Google Scholar] [CrossRef]
- Dietrich, J.; Rao, K.; Pastorino, S.; Kesari, S. Corticosteroids in brain cancer patients: Benefits and pitfalls. Expert. Rev. Clin. Pharmacol. 2011, 4, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P.J. Anti-inflammatory actions of glucocorticoids: Molecular mechanisms. Clin. Sci. 1998, 94, 557–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinarello, C.A. Anti-inflammatory agents: Present and future. Cell 2010, 140, 935–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistics insights. Mol. Cell Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef]
- Quan, W.; Zhang, Z.; Li, P.; Tian, Q.; Huang, J.; Qian, Y.; Gao, C.; Su, W.; Wang, Z.; Zhang, J.; et al. Role of regulatroy T cells in atorvastatin induced absorption of chronic subdural hematoma in rats. Aging Dis. 2019, 10, 992–1002. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022): Cochrane. 2022. Available online: https://training.cochrane.org/handbook/current (accessed on 31 August 2022).
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Lampmann, T.; Hadjiathanasiou, A.; Asoglu, H.; Wach, J.; Kern, T.; Vatter, H.; Güresir, E. Early Serum Creatinine Levels after Aneurysmal Subarachnoid Hemorrhage Predict Functional Neurological Outcome after 6 Months. J. Clin. Med. 2022, 11, 4753. [Google Scholar] [CrossRef]
- Kim, H.C.; Ko, J.H.; Yoo, D.S.; Lee, S.K. Spontaneous Resolution of Chronic Subdural Hematoma: Close Observation as a Treatment Strategy. J. Korean Neurosurg. Soc. 2016, 59, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Schünemann, H.; Brozek, J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations (Updated October 2013): The GRADE Working Group. 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 31 August 2022).
- Wells, G.A.; Shea, B.; O´Connell, D.; Petersen, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000; Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 September 2022).
- Ng, S.; Boetto, J.; Huguet, H.; Roche, P.H.; Fuentes, S.; Lonjon, M.; Litrico, S.; Barbanel, A.M.; Sabatier, P.; Bauchet, L.; et al. HEMACORT Study Group. Corticosteroids as an Adjuvant Treatment to Surgery in Chronic Subdural Hematomas: A Multi-Center Double-Blind Randomized Placebo-Controlled Trial. J. Neurotrauma 2021, 38, 1484–1494. [Google Scholar] [CrossRef]
- Hutchinson, P.J.; Edlmann, E.; Bulters, D.; Zolnourian, A.; Holton, P.; Suttner, N.; Agyemang, K.; Thomson, S.; Anderson, I.A.; Al-Tamimi, Y.Z.; et al. British Neurosurgical Trainee Research Collaborative; Dex-CSDH Trial Collaborators. Trial of Dexamethasone for Chronic Subdural Hematoma. N. Engl. J. Med. 2020, 383, 2616–2627. [Google Scholar] [CrossRef]
- Mebberson, K.; Colditz, M.; Marshman, L.A.G.; Thomas, P.A.W.; Mitchell, P.S.; Robertson, K. Prospective randomized placebo-controlled double-blind clinical study of adjuvant dexamethasone with surgery for chronic subdural haematoma with post-operative subdural drainage: Interim analysis. J. Clin. Neurosci. 2020, 71, 153–157. [Google Scholar] [CrossRef]
- Jiang, R.; Zhao, S.; Wang, R.; Feng, H.; Zhang, J.; Li, X.; Mao, Y.; Yuan, X.; Fei, Z.; Zhao, Y.; et al. Safety and Efficacy of Atorvastatin for Chronic Subdural Hematoma in Chinese Patients: A Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1338–1346. [Google Scholar] [CrossRef] [Green Version]
- Prud’homme, M.; Mathieu, F.; Marcotte, N.; Cottin, S. A Pilot Placebo Controlled Randomized Trial of Dexamethasone for Chronic Subdural Hematoma. Can. J. Neurol. Sci. 2016, 43, 284–290. [Google Scholar] [CrossRef]
- Tariq, J.; Bhatti, S.N. Adjunctive postoperative course of dexamethasone in chronic subdural hematoma: Effect on surgical outcome. Pak. J. Med. Sci. 2021, 37, 1877–1882. [Google Scholar] [CrossRef]
- Fujisawa, N.; Oya, S.; Yoshida, S.; Tsuchiya, T.; Nakamura, T.; Indo, M.; Matsui, T. A Prospective Randomized Study on the Preventive Effect of Japanese Herbal Kampo Medicine Goreisan for Recurrence of Chronic Subdural Hematoma. Neurol. Med. Chir. 2021, 61, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Katayama, K.; Matsuda, N.; Kakuta, K.; Naraoka, M.; Takemura, A.; Hasegawa, S.; Akasaka, K.; Shimamura, N.; Itoh, K.; Asano, K.; et al. The Effect of Goreisan on the Prevention of Chronic Subdural Hematoma Recurrence: Multi-Center Randomized Controlled Study. J. Neurotrauma 2018, 35, 1537–1542. [Google Scholar] [CrossRef] [PubMed]
- Workewych, A.; Callum, J.; Saarela, O.; Montanera, W. Tranexamic acid in the treatment of residual chronic subdural hematoma: A single-centre, randomized controlled trial (TRACE). J. Neurotrauma 2018, 35, A244–A245. [Google Scholar]
- Yamada, T.; Natori, Y. Prospective Study on the Efficacy of Orally Administered Tranexamic Acid and Goreisan for the Prevention of Recurrence After Chronic Subdural Hematoma Burr Hole Surgery. World Neurosurg. 2020, 134, e549–e553. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.Y.C.; Sun, T.F.D.; Poon, W.S. Steroid for chronic subdural hematoma? A prospective phase IIB pilot randomized controlled trial on the use of dexamethasone with surgical drainage for the reduction of recurrence with reoperation. Chin. Neurosurg. J. 2015, 1. [Google Scholar] [CrossRef] [Green Version]
- Sun, T.F.; Boet, R.; Poon, W.S. Non-surgical Primary Treatment of Chronic Subdural Haematoma: Preliminary Results of Using Dexamethasone. Br. J. Neurosurg. 2005, 19, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hirashima, Y.; Kurimoto, M.; Nagai, S.; Hori, E.; Origasa, H.; Endo, S. Effect of platelet-activating factor receptor antagonist, etizolam, on resolution of chronic subdural hematoma--a prospective study to investigate use as conservative therapy. Neurol. Med. Chir. 2005, 45, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Hirashima, Y.; Kuwayama, N.; Hamada, H.; Hayashi, N.; Endo, S. Etizolam, an anti-anxiety agent, attenuates recurrence of chronic subdural hematoma--evaluation by computed tomography. Neurol. Med. Chir. 2002, 42, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Schaumann, A.; Klene, W.; Rosenstengel, C.; Ringel, F.; Tüttenberg, J.; Vajkoczy, P. COXIBRAIN: Results of the prospective, randomized, phase II/III study for the selective COX-2 inhibition in chronic subdural haematoma patients. Acta Neurochir. 2016, 158, 2039–2044. [Google Scholar] [CrossRef]
- Kolias, A.G.; Chari, A.; Santarius, T.; Hutchinson, P.J. Chronic subdural haematoma: Modern management and emerging therapies. Nat. Rev. Neurol. 2014, 10, 570–578. [Google Scholar] [CrossRef]
- Almenawer, S.A.; Farrokhyar, F.; Hong, C.; Alhazzani, W.; Manoranjan, B.; Yarascavitch, B.; Arjmand, P.; Baronia, B.; Reddy, K.; Murty, N.; et al. Chronic subdural hematoma management: A systematic review and meta-analysis of 34,829 patients. Ann. Surg. 2014, 259, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Torihashi, K.; Sadamasa, N.; Yoshida, K.; Narumi, O.; Chin, M.; Yamagata, S. Independent predictors for recurrence of chronic subdural hematoma: A review of 343 consecutive surgical cases. Neurosurgery 2008, 63, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Li, T.; Tian, Y.; Wang, S.; Jin, C.; Wei, H.; Quan, W.; Wang, J.; Chen, J.; Dong, J.; et al. Effects of Atorvastatin on Chronic Subdural Hematoma: A Preliminary Report from Three Medical Centers. J. Neurol. Sci. 2014, 336, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zacharek, A.; Li, A.; Cui, X.; Roberts, C.; Lu, M.; Chopp, M. Atorvastatin promotes presenilin-1 expression and Notch1 activity and increases neural progenitor cell proliferation after stroke. Stroke 2008, 39, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Chen, Z.; Zou, Y.; Ge, J. Atorvastatin represses the angiotensin 2-induced oxidative stress and inflammatory response in dendritic cells via the PI3K/Akt/Nrf 2 pathway. Oxid. Med. Cell. Longev. 2014, 2014, 148798. [Google Scholar] [CrossRef] [Green Version]
- He, C.; Xia, P.; Xu, J.; Chen, L.; Zhang, Q. Evaluation of the efficacy of atorvastatin in the treatment for chronic subdural hematoma: A meta-analysis. Neurosurg. Rev. 2021, 44, 479–484. [Google Scholar] [CrossRef]
- Song, Y.; Wang, Z.; Liu, L.; Wang, D.; Zhang, J. The level of circulating endothelial progenitor cells may be associated with the occurrence and recurrence of chronic subdural hematoma. Clinics 2013, 68, 1084–1088. [Google Scholar] [CrossRef]
- Liu, H.F.; Qi, X.W.; Ma, L.L.; Yao, D.K.; Wang, L. Atorvastatin improves endothelial progenitor cell function and reduces pulmonary hypertension in patients with chronic pulmonary heart disease. Exp. Clin. Cardiol. 2013, 18, e40–e43. [Google Scholar]
- Araujo, F.; Rocha, M.A.; Mendes, J.B.; Andrade, S.P. Atorvastatin Inhibits Inflammatory Angiogenesis in Mice through Down Regulation of VEGF, TNF-Alpha and TGF-Beta1. Biomed. Pharmacother. 2010, 64, 29–34. [Google Scholar] [CrossRef]
- Li, T.; Wang, D.; Tian, Y.; Yu, H.; Wang, Y.; Quan, W.; Cui, W.; Zhou, L.; Chen, J.; Jiang, R.; et al. Effects of atorvastatin on the inflammation regulation and elimination of subdural hematoma in rats. J. Neruol. Sci. 2014, 341, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Shofty, B.; Grossman, R. Treatment Options for Chronic Subdural Hematoma. World Neurosurg. 2016, 87, 529–530. [Google Scholar] [CrossRef]
- Soleman, J.; Nocera, F.; Mariani, L. The Conservative and Pharmacological Management of Chronic Subdural Haematoma. Swiss Med. Wkly. 2017, 147, w14398. [Google Scholar] [PubMed]
- Yu, W.; Chen, Q.; Jiang, Y.; Ma, M.; Zhang, W.; Zhang, X.; Cheng, Y. Effectiveness Comparisons of Drug Therapy on Chronic Subdural Hematoma Recurrence: A Bayesian Network Meta-Analysis and Systematic Review. Front. Pharmacol. 2022, 13, 845386. [Google Scholar] [CrossRef] [PubMed]
- Glover, D.; Labadie, E.L. Physiopathogenesis of Subdural Hematomas. Part 2: Inhibition of Growth of Experimental Hematomas with Dexamethasone. J. Neurosurg. 1976, 45, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Holl, D.C.; Volovici, V.; Dirven, C.M.F.; van Kooten, F.; Miah, I.P.; Jellema, K.; Peul, W.C.; van der Gaag, N.A.; Kho, K.H.; Hertog, H.M.D.; et al. Corticosteroid Treatment Compared with Surgery in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis. Acta Neurochir. 2019, 161, 1231–1242. [Google Scholar] [CrossRef] [PubMed]
- Shhrestha, D.B.; Budhathoki, P.; Sedhai, Y.R.; Jain, S.; Karki, P.; Jha, P.; Mainali, G.; Ghimire, P. Steroid in Chronic Subdural Hematoma: An Updated Systematic Review and Meta-Analysis Post DEX-CSDH Trial. World Neurosurg. 2021, 158, 84–99. [Google Scholar] [CrossRef]
- Wang, X.; Song, J.; He, Q.; You, C. Pharmacological Treatment in the Management of Chronic Subdural Hematoma. Front. Aging. Neurosci. 2021, 13, 684501. [Google Scholar] [CrossRef]
- Wang, D.; Gao, C.; Xu, X.; Chen, T.; Tian, Y.; Wie, H.; Zhang, S.; Quan, W.; Wang, Y.; Yue, S.; et al. Treatment of chronic subdural hematoma with atorvastatin combined with low-dose dexamethasone: Phase II randomized proof-of-concept clinical trial. J. Neurosurg. 2020, 31, 1–9. [Google Scholar] [CrossRef]
- Gong, Z.; Zhan, D.; Nie, M.; Li, X.; Gao, C.; Liu, X.; Xiang, T.; Yuan, J.; Jiang, W.; Huang, J.; et al. Dexamethasone enhances the efficacy of atorvastatin in inhibiting excessively inflammation-induced abnormal angiogenesis by regulating macrophages. J. Neuroninflamm. 2021, 18, 203. [Google Scholar] [CrossRef]
- Won, S.Y.; Dubinski, D.; Sautter, L.; Hattingen, E.; Seifert, V.; Rosenow, F.; Freiman, T.; Strzelczyk, A.; Konczalla, J. Seizure and status epilepticus in chronic subdural hematoma. Acta Neurol. Scand. 2019, 140, 194–203. [Google Scholar] [CrossRef]
- Stippler, M.; Ramirez, P.; Berti, A.; Macindoe, C.; Villalobos, N.; Murray-Krezan, C. Chronic subdural hematoma patients aged 90 years and older. Neurol. Res. 2013, 35, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Vychopen, M.; Hamed, M.; Bahna, M.; Racz, A.; Ilic, I.; Salemdawod, A.; Schneider, M.; Lehmann, F.; Eichhorn, L.; Bode, C.; et al. A Validation Study for SHE Score for Acute Subdural Hematoma in the Elderly. Brain Sci. 2022, 12, 981. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Year | Treatments and Dosage | Sample Size (n) | Intervention (n) | Control (n) | Reported Outcome | Country & Number of Centers |
|---|---|---|---|---|---|---|---|
| Ng et al. [28] | 2021 | Prednisone 1 mg/kg/d | 155 | 78 | 77 | Markwalder grading score (MGS) at 12 months | France (Multicentric) |
| Hutchinson et al. [29] | 2020 | Dexamethasone 8 mg 2× daily | 748 | 375 | 373 | Modified Rankin scale (mRS) at 6 months | United Kingdom (Multicentric) |
| Mebberson et al. [30] | 2019 | Dexamethasone 128 mg/2 weeks | 47 | 24 | 22 | Modified Rankin scale (mRS) at 6 months | Australia (Monocentric) |
| Jiang et al. [31] | 2018 | Atorvastatin 20 mg/day for 8 weeks | 196 | 98 | 98 | Markwalder grading score (MGS) at 12 months | China (Multicentric) |
| Prud´homme et al. [32] | 2016 | Dexamethasone 12 mg/day for 3 weeks | 20 | 10 | 10 | Mortality at 6 months | Canada (Monocentric) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vychopen, M.; Güresir, E.; Wach, J. Anti-Inflammatory Drug Therapy in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis of Prospective Randomized, Double-Blind and Placebo-Controlled Trials. Int. J. Mol. Sci. 2022, 23, 16198. https://doi.org/10.3390/ijms232416198
Vychopen M, Güresir E, Wach J. Anti-Inflammatory Drug Therapy in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis of Prospective Randomized, Double-Blind and Placebo-Controlled Trials. International Journal of Molecular Sciences. 2022; 23(24):16198. https://doi.org/10.3390/ijms232416198
Chicago/Turabian StyleVychopen, Martin, Erdem Güresir, and Johannes Wach. 2022. "Anti-Inflammatory Drug Therapy in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis of Prospective Randomized, Double-Blind and Placebo-Controlled Trials" International Journal of Molecular Sciences 23, no. 24: 16198. https://doi.org/10.3390/ijms232416198
APA StyleVychopen, M., Güresir, E., & Wach, J. (2022). Anti-Inflammatory Drug Therapy in Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis of Prospective Randomized, Double-Blind and Placebo-Controlled Trials. International Journal of Molecular Sciences, 23(24), 16198. https://doi.org/10.3390/ijms232416198