

Relationship of Cognition and Alzheimer’s Disease with Gastrointestinal Tract Disorders: A Large-Scale Genetic Overlap and Mendelian Randomisation Analysis
 ,
,
Abstract
:1. Introduction
2. Results
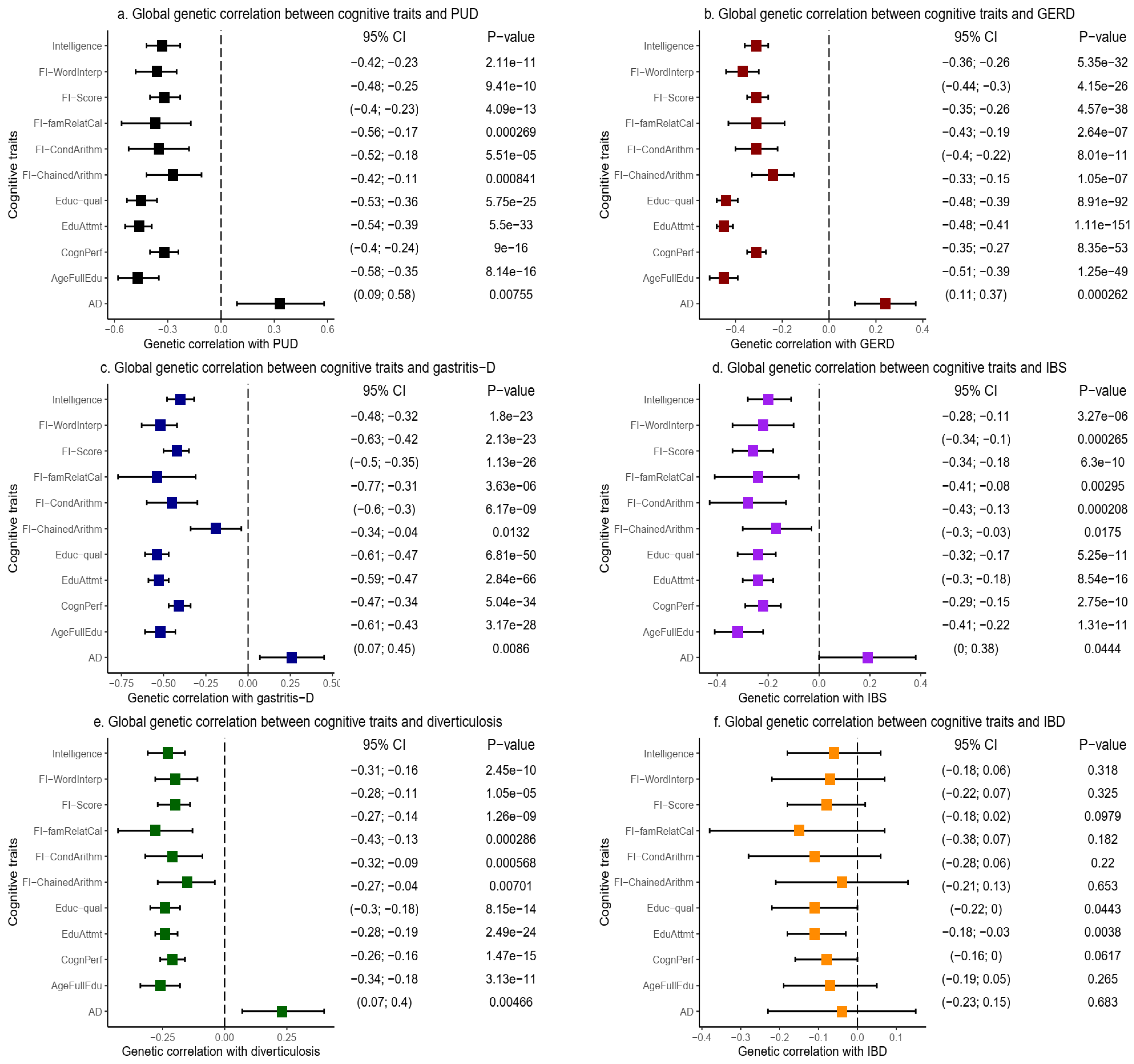
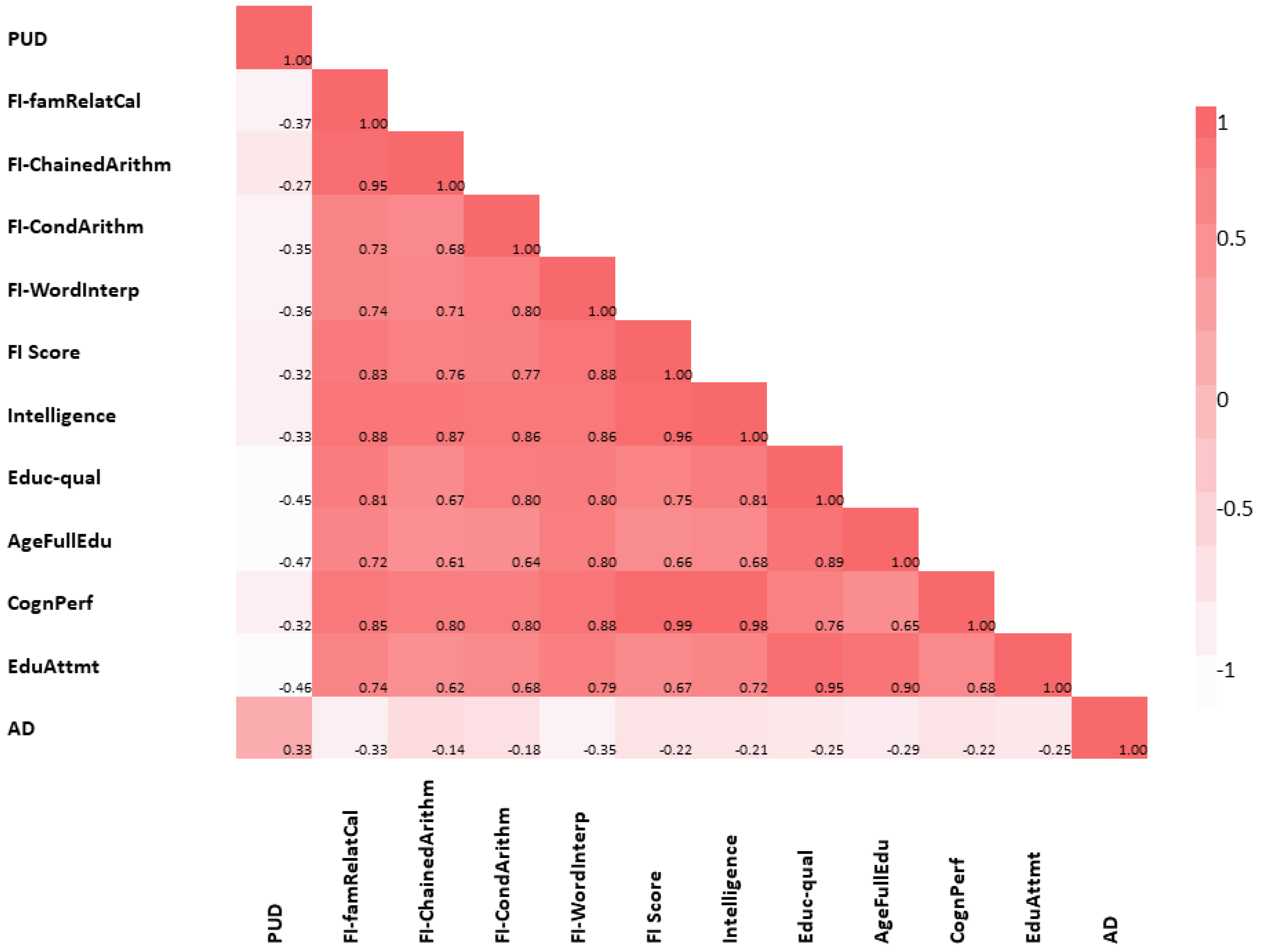
2.1. Global Genetic Correlation of Cognitive Traits with GIT Disorders
2.2. Local Genetic Correlation of Cognitive Traits and AD with GIT Disorders
2.3. Results of Causal Relationship Assessment
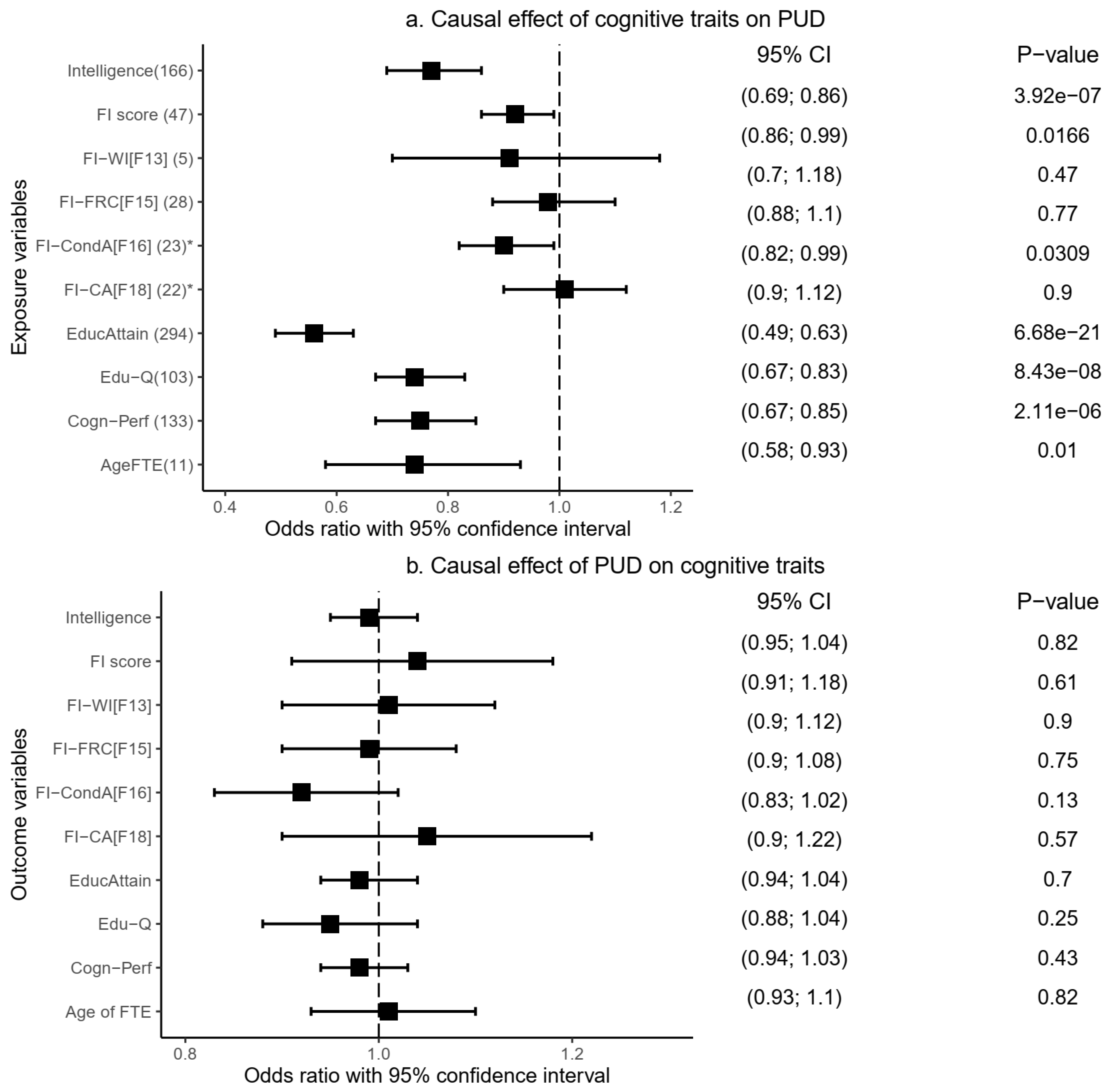
2.3.1. Causal Relationship of Peptic Ulcer Disease with Cognitive Traits
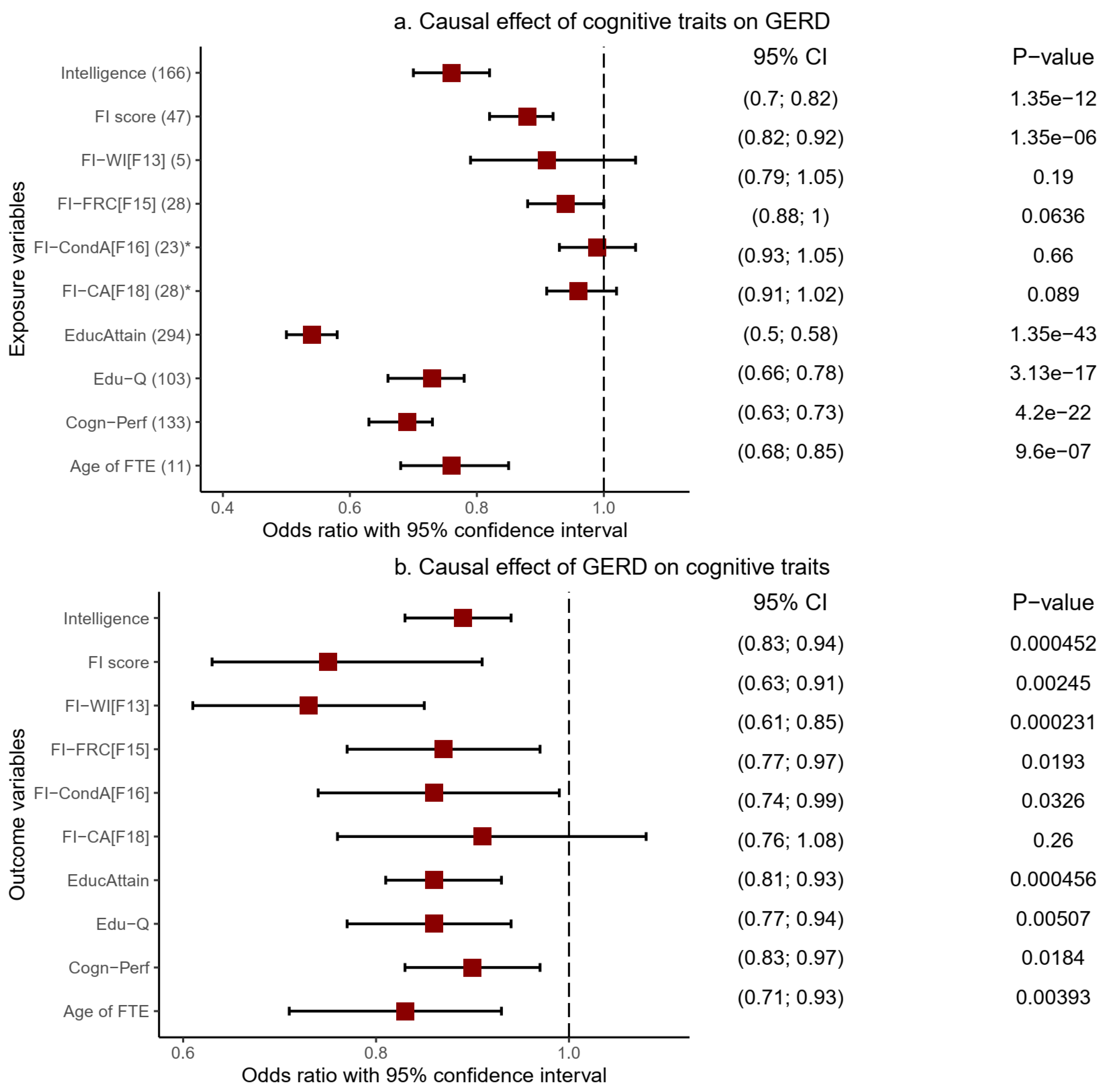
2.3.2. Causal Relationship of Gastroesophageal Reflux Disease with Cognitive Traits
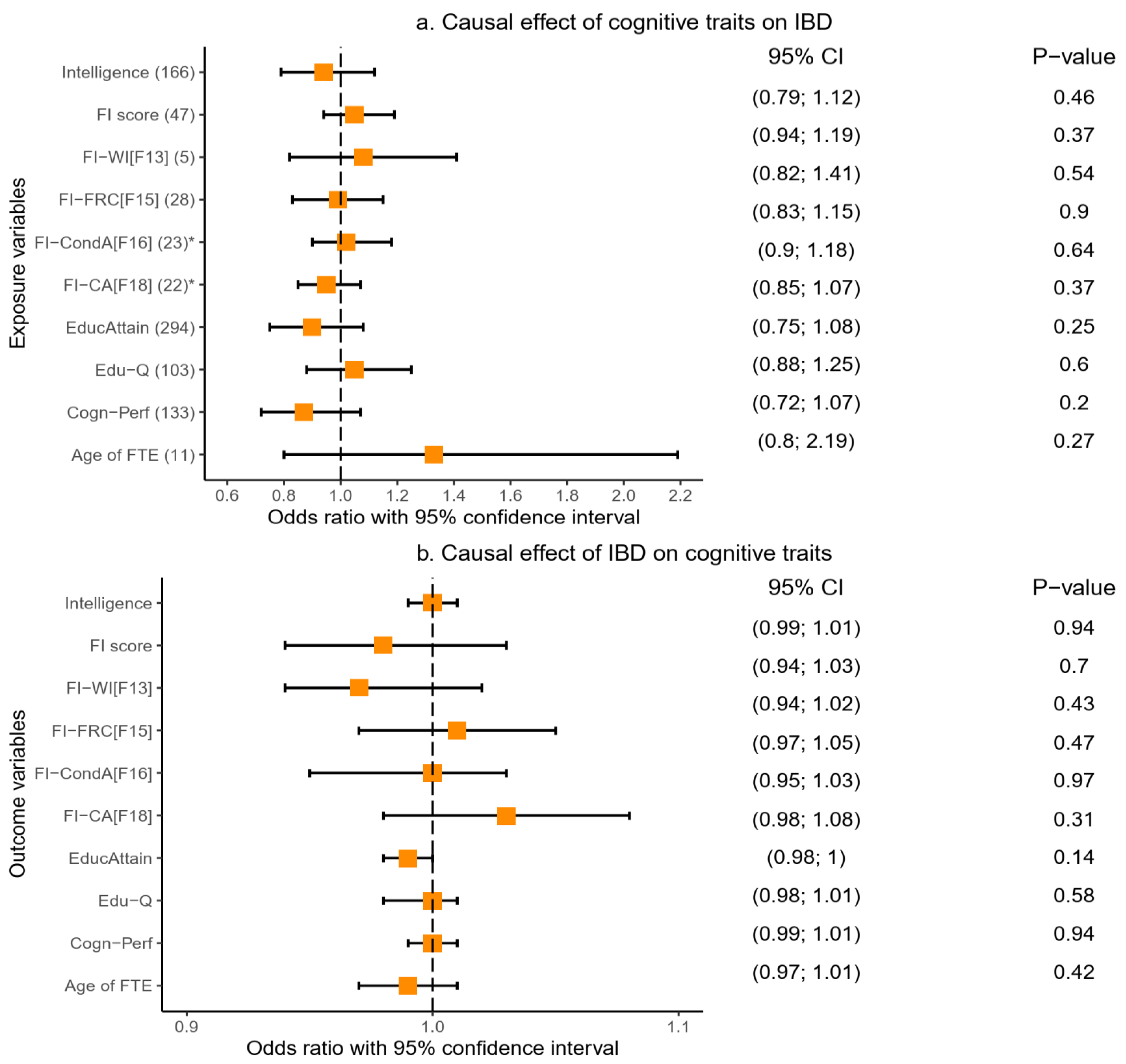
2.3.3. Causal Relationship of Inflammatory Bowel Disease with Cognitive Traits
2.4. Results of Gene-Level Genetic Overlap Analysis
3. Discussion
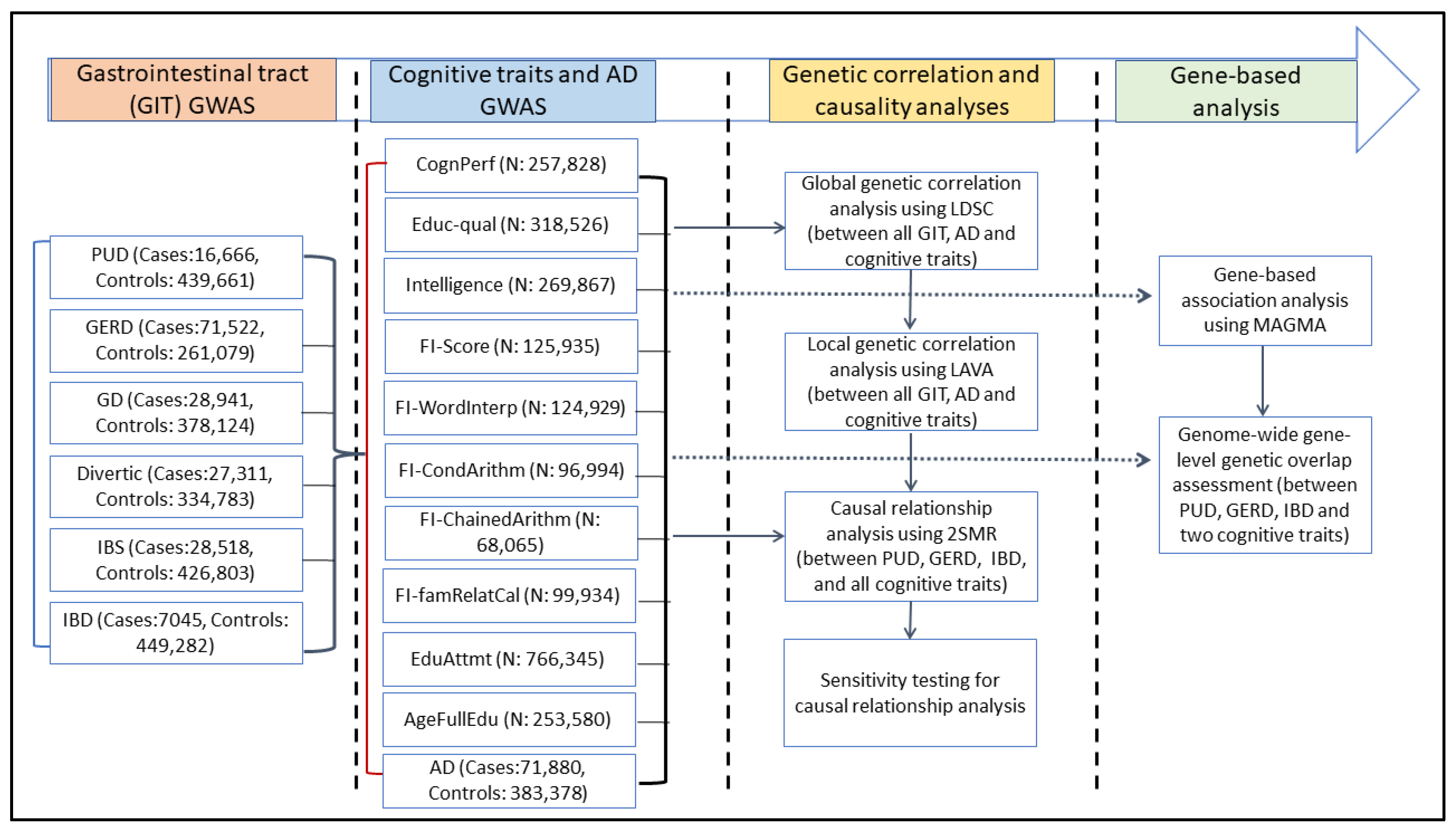
4. Materials and Methods
4.1. Data Sources
4.2. Genome-Wide (Global) Genetic Correlation Analysis
4.3. Local Genetic Correlation Analysis
4.4. Bidirectional Mendelian Randomisation Analysis
4.5. Gene-Level Genetic Overlap Assessment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khodabakhsh, P.; Bazrgar, M.; Dargahi, L.; Mohagheghi, F.; Taei, A.A.; Parvardeh, S.; Ahmadiani, A. Does Alzheimer’s disease stem in the gastrointestinal system? Life Sci. 2021, 287, 120088. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Dawson, T.M.; Kulkarni, S. Neurodegenerative disorders and gut-brain interactions. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Mitrea, L.; Nemes, S.A.; Szabo, K.; Teleky, B.E.; Vodnar, D.C. Guts Imbalance Imbalances the Brain: A Review of Gut Microbiota Association With Neurological and Psychiatric Disorders. Front. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.C.; Olson, C.A.; Hsiao, E.Y. Interactions between the microbiota, immune and nervous systems in health and disease. Nat. Neurosci. 2017, 20, 145–155. [Google Scholar] [CrossRef]
- Liu, S.; Gao, J.; Zhu, M.; Liu, K.; Zhang, H.-L. Gut Microbiota and Dysbiosis in Alzheimer’s Disease: Implications for Pathogenesis and Treatment. Mol. Neurobiol. 2020, 57, 5026–5043. [Google Scholar] [CrossRef]
- Lee, J.-G.; Cho, H.-J.; Jeong, Y.-M.; Lee, J.-S. Genetic Approaches Using Zebrafish to Study the Microbiota–Gut–Brain Axis in Neurological Disorders. Cells 2021, 10, 566. [Google Scholar] [CrossRef]
- dewuyi, E.O.; O’Brien, E.K.; Nyholt, D.R.; Porter, T.; Laws, S.M. A large-scale genome-wide cross-trait analysis reveals shared genetic architecture between Alzheimer’s disease and gastrointestinal tract disorders. Commun. Biol. 2022, 5, 1–14. [Google Scholar] [CrossRef]
- Jiang, C.; Li, G.; Huang, P.; Liu, Z.; Bin Zhao, B. The Gut Microbiota and Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 58, 1–15. [Google Scholar] [CrossRef]
- Doulberis, M.; Kotronis, G.; Gialamprinou, D.; Polyzos, S.A.; Papaefthymiou, A.; Katsinelos, P.; Kountouras, J. Alzheimer’s disease and gastrointestinal microbiota; impact of Helicobacter pylori infection involvement. Int. J. Neurosci. 2020, 131, 289–301. [Google Scholar] [CrossRef]
- Momtaz, Y.A.; Hamid, T.A.; Ibrahim, R. Gastritis May Boost Odds of Dementia. Am. J. Alzheimer’s Dis. Other Dementiasr 2014, 29, 452–456. [Google Scholar] [CrossRef]
- Gau, S.-Y.; Lai, J.-N.; Yip, H.-T.; Wu, M.-C.; Wei, J.C.-C. Higher Dementia Risk in People With Gastroesophageal Reflux Disease: A Real-World Evidence. Front. Aging Neurosci. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Wang, H.E.; Bai, Y.-M.; Tsai, S.-J.; Su, T.-P.; Chen, T.-J.; Wang, Y.-P.; Chen, M.-H. Inflammatory bowel disease is associated with higher dementia risk: A nationwide longitudinal study. Gut 2020, 70, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Lin, C.-L.; Kao, C.-H. Irritable Bowel Syndrome Is Associated with an Increased Risk of Dementia: A Nationwide Population-Based Study. PLoS ONE 2016, 11, e0144589. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-C.; Chang, K.-H.; Lee, C.-Y.; Chong, L.-W.; Hsu, Y.-C.; Kao, C.-H.; Lin, C.-L. Association of Dementia and Peptic Ulcer Disease. Am. J. Alzheimer’s Dis. Other Dementiasr 2016, 31, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Li, Z.; Chen, P.; Zhang, A.; Zeng, Y.; Zhang, X.; Huang, Q.; Liu, D.; Qi, S.; Mao, C. Regular proton pump inhibitor use and incident dementia: Population-based cohort study. BMC Med. 2022, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Sommerville, N.R.; Liu, J.Y.H.; Ngan, M.P.; Poon, D.; Ponomarev, E.D.; Lu, Z.; Kung, J.S.C.; Rudd, J.A. Intra-gastrointestinal amyloid-β1–42 oligomers perturb enteric function and induce Alzheimer's disease pathology. J. Physiol. 2020, 598, 4209–4223. [Google Scholar] [CrossRef]
- Vonderwalde, I.; Finlayson-Trick, E. Gut amyloid-β induces cognitive deficits and Alzheimer's disease-related histopathology in a mouse model. J. Physiol. 2020, 599, 15–16. [Google Scholar] [CrossRef]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Cummings, J.; Lee, G.; Ritter, A.; Sabbagh, M.; Zhong, K. Alzheimer’s disease drug development pipeline: 2019. Alzheimer’s Dementia Transl. Res. Clin. Interv. 2019, 5, 272–293. [Google Scholar] [CrossRef]
- Hopkins, C.W.; Powell, N.; Norton, C.; Dumbrill, J.L.; Hayee, B.; Moulton, C.D. Cognitive Impairment in Adult Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Psychosom. 2021, 62, 387–403. [Google Scholar] [CrossRef]
- Jones, J.D.; Rahmani, E.; Garcia, E.; Jacobs, J.P. Gastrointestinal symptoms are predictive of trajectories of cognitive functioning in de novo Parkinson's disease. Park. Relat. Disord. 2020, 72, 7–12. [Google Scholar] [CrossRef]
- Hadjina, I.T.; Zivkovic, P.M.; Matetic, A.; Rusic, D.; Vilovic, M.; Bajo, D.; Puljiz, Z.; Tonkic, A.; Bozic, J. Impaired neurocognitive and psychomotor performance in patients with inflammatory bowel disease. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Dhiman, S.; Bodh, V.; Sharma, D.; Sharma, R.; Sharma, S.; Sharma, B. Cognitive dysfunction in ulcerative colitis patients in remission and its comparison with patients with irritable bowel syndrome and healthy controls. Indian J. Gastroenterol. 2021, 40, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.S.; Sanborn, V.; Gunstad, J.; Spitznagel, M.B. Poorer Cognitive Performance Is Associated with Gastrointestinal Symptoms in Otherwise Healthy Young Adults. Dig. Dis. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lanas, A.; Chan, F.K.L. Peptic ulcer disease. Lancet 2017, 390, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Han, M.-L.; Chen, J.-H.; Tsai, M.-K.; Liou, J.-M.; Chiou, J.-M.; Chiu, M.-J.; Chen, Y.-C. Association between Helicobacter pylori infection and cognitive impairment in the elderly. J. Formos. Med Assoc. 2018, 117, 994–1002. [Google Scholar] [CrossRef]
- Franceschi, F.; Ojetti, V.; Candelli, M.; Covino, M.; Cardone, S.; Potenza, A.; Simeoni, B.; Gabrielli, M.; Sabia, L.; Gasbarrini, G.; et al. Microbes and Alzheimer’ disease: Lessons from H. pylori and GUT microbiota. Eur. Rev. Med Pharmacol. Sci. 2019, 23, 426–430. [Google Scholar]
- Li, B.; He, Y.; Ma, J.; Huang, P.; Du, J.; Cao, L.; Wang, Y.; Xiao, Q.; Tang, H.; Chen, S. Mild cognitive impairment has similar alterations as Alzheimer's disease in gut microbiota. Alzheimer’s Dement. 2019, 15, 1357–1366. [Google Scholar] [CrossRef]
- Wu, Y.; Murray, G.K.; Byrne, E.M.; Sidorenko, J.; Visscher, P.M.; Wray, N.R. GWAS of peptic ulcer disease implicates Helicobacter pylori infection, other gastrointestinal disorders and depression. Nat. Commun. 2021, 12, 1–17. [Google Scholar] [CrossRef]
- Tegeler, C.; O'Sullivan, J.L.; Bucholtz, N.; Goldeck, D.; Pawelec, G.; Steinhagen-Thiessen, E.; Demuth, I. The inflammatory markers CRP, IL-6, and IL-10 are associated with cognitive function—Data from the Berlin Aging Study II. Neurobiol. Aging 2016, 38, 112–117. [Google Scholar] [CrossRef]
- Berrill, J.W.; Gallacher, J.; Hood, K.; Green, J.T.; Matthews, S.B.; Campbell, A.; Smith, A. An observational study of cognitive function in patients with irritable bowel syndrome and inflammatory bowel disease. Neurogastroenterol. Motil. 2013, 25, 918-e704. [Google Scholar] [CrossRef]
- Lam, N.C.-Y.; Yeung, H.-Y.; Li, W.-K.; Lo, H.-Y.; Yuen, C.-F.; Chang, R.C.-C.; Ho, Y.-S. Cognitive impairment in Irritable Bowel Syndrome (IBS): A systematic review. Brain Res. 2019, 1719, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M.; Holmes, M.V.; Smith, G.D. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 2018, 362, k601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulik-Sullivan, B.K.; Loh, P.R.; Finucane, H.K.; Ripke, S.; Yang, J.; Schizophrenia Working Group of the Psychiatric Genomics Consortium; Patterson, N.; Daly, M.J.; Price, A.L.; Neale, B.M. LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat. Genet. 2015, 47, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Werme, J.; van der Sluis, S.; Posthuma, D.; de Leeuw, C.A. An integrated framework for local genetic correlation analysis. Nat. Genet. 2022, 54, 274–282. [Google Scholar] [CrossRef]
- Anderson, E.L.; Howe, L.D.; Wade, K.H.; Ben-Shlomo, Y.; Hill, W.D.; Deary, I.J.; Sanderson, E.C.; Zheng, J.; Korologou-Linden, R.; Stergiakouli, E.; et al. Education, intelligence and Alzheimer’s disease: Evidence from a multivariable two-sample Mendelian randomization study. Leuk. Res. 2020, 49, 1163–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tillmann, T.; Vaucher, J.; Okbay, A.; Pikhart, H.; Peasey, A.; Kubinova, R.; Pajak, A.; Tamosiunas, A.; Malyutina, S.; Hartwig, F.P.; et al. Education and coronary heart disease: Mendelian randomisation study. BMJ 2017, 358, j3542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sand, J.R.; Troelsen, F.S.; Horváth-Puhó, E.; Henderson, V.W.; Sørensen, H.T.; Erichsen, R. Risk of dementia in patients with inflammatory bowel disease: A Danish population-based study. Aliment. Pharmacol. Ther. 2022, 56, 831–843. [Google Scholar] [CrossRef]
- Sun, Y.; Geng, J.; Chen, X.; Chen, H.; Wang, X.; Chen, J.; Li, X.; Hesketh, T. Association Between Inflammatory Bowel Disease and Dementia: A Longitudinal Cohort Study. Inflamm. Bowel Dis. 2021. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Nugent, Z.; Shaffer, S.; Singh, H.; Marrie, R.A. Comorbidity before and after a diagnosis of inflammatory bowel disease. Aliment. Pharmacol. Ther. 2021, 54, 637–651. [Google Scholar] [CrossRef]
- Savage, J.E.; Jansen, P.R.; Stringer, S.; Watanabe, K.; Bryois, J.; de Leeuw, C.A.; Nagel, M.; Awasthi, S.; Barr, P.B.; Coleman, J.R.I.; et al. Faculty Opinions recommendation of Genome-wide association meta-analysis in 269,867 individuals identifies new genetic and functional links to intelligence. Nat. Genet. 2018, 50, 912–919. [Google Scholar] [CrossRef]
- Lee, J.J.; Wedow, R.; Okbay, A.; Kong, E.; Maghzian, O.; Zacher, M.; Nguyen-Viet, T.A.; Bowers, P.; Sidorenko, J.; Karlsson Linnér, R.R.; et al. Gene discovery and polygenic prediction from a genome-wide association study of educational attainment in 1.1 million individuals. Nat. Genet. 2018, 50, 1112–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Stringer, S.; Frei, O.; Mirkov, M.U.; de Leeuw, C.; Polderman, T.J.C.; van der Sluis, S.; Andreassen, O.A.; Neale, B.M.; Posthuma, D. A global overview of pleiotropy and genetic architecture in complex traits. Nat. Genet. 2019, 51, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Gharahkhani, P.; Law, M.H.; Ong, J.-S.; Han, X.; Olsen, C.M.; Neale, R.E.; Lai, J.; Vaughan, T.L.; Gockel, I.; et al. Gastroesophageal reflux GWAS identifies risk loci that also associate with subsequent severe esophageal diseases. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jansen, I.E.; Savage, J.E.; Watanabe, K.; Bryois, J.; Williams, D.; Steinberg, S.; Sealock, J.; Karlsson, I.; Hägg, S.; Athanasiu, L.; et al. Genome-wide meta-analysis identifies new loci and functional pathways influencing Alzheimer’s disease risk. Nat. Genet. 2019, 51, 404–413. [Google Scholar] [CrossRef]
- Sekula, P.; Fabiola Del Greco, M.; Pattaro, C.; Köttgen, A. Mendelian Randomization as an Approach to Assess Causality Using Observational Data. J. Am. Soc. Nephrol. 2016, 27, 3253–3265. [Google Scholar] [CrossRef] [Green Version]
- Wooldridge, J.M. Chapter 15: Instrumental Variables Estimation and Two-stage Least Squares. In Introductory econometrics; South-Western Publishing: Nashville, TN, USA, 2009. [Google Scholar]
- Bowden, J.; Davey Smith, G.; Haycock, P.C.; Burgess, S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet. Epidemiol. 2016, 40, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Davey Smith, G.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef] [Green Version]
- Verbanck, M.; Chen, C.-Y.; Neale, B.; Do, R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat. Genet. 2018, 50, 693–698. [Google Scholar] [CrossRef]
- Yang, Y.; The International Headache Genetics Consortium; Zhao, H.; I. Boomsma, D.; Ligthart, L.; Belin, A.C.; Smith, G.D.; Esko, T.; Freilinger, T.M.; Hansen, T.F.; et al. Molecular genetic overlap between migraine and major depressive disorder. Eur. J. Hum. Genet. 2018, 26, 1202–1216. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Nyholt, D.R. Gene-based analyses reveal novel genetic overlap and allelic heterogeneity across five major psychiatric disorders. Hum. Genet. 2016, 136, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Adewuyi, E.O.; Mehta, D.; International Endogene Consortium (IEC); Sapkota, Y.; Yoshihara, K.; Nyegaard, M.; Steinthorsdottir, V.; Morris, A.P.; Fassbender, A.; Rahmioglu, N.; et al. Genetic overlap analysis of endometriosis and asthma identifies shared loci implicating sex hormones and thyroid signalling pathways. Hum. Reprod. 2021, 37, 366–383. [Google Scholar] [CrossRef] [PubMed]
- Adewuyi, E.O.; Mehta, D.; Sapkota, Y.; Auta, A.; Yoshihara, K.; Nyegaard, M.; Griffiths, L.R.; Montgomery, G.W.; Chasman, D.I.; Nyholt, D.R.; et al. Genetic analysis of endometriosis and depression identifies shared loci and implicates causal links with gastric mucosa abnormality. Hum. Genet. 2020, 140, 529–552. [Google Scholar] [CrossRef]
- Adewuyi, E.O.; Sapkota, Y.; International Endogene Consortium (IEC) International Endogene Consortium (IEC); 23andMe Research Team 23andMe Research Team; International Headache Genetics Consortium (IHGC) International Headache Genetics Consortium (IHGC); Auta, A.; Yoshihara, K.; Nyegaard, M.; Griffiths, L.R.; Montgomery, G.W.; et al. Shared Molecular Genetic Mechanisms Underlie Endometriosis and Migraine Comorbidity. Genes 2020, 11, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanha, H.M.; Nyholt, D.R. The International Headache Genetics Consortium Genetic analyses identify pleiotropy and causality for blood proteins and highlight Wnt/β-catenin signalling in migraine. Nat. Commun. 2022, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- de Leeuw, C.A.; Mooij, J.M.; Heskes, T.; Posthuma, D. MAGMA: Generalized Gene-Set Analysis of GWAS Data. PLoS Comput. Biol. 2015, 11, e1004219. [Google Scholar] [CrossRef]
- Watanabe, K.; Taskesen, E.; van Bochoven, A.; Posthuma, D. Functional mapping and annotation of genetic associations with FUMA. Nat. Commun. 2017, 8, 1–11. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phenotype Class | Phenotype Name | Sample Size | Global h2SNP (observed scale) | Global h2SNP SE | Atlas or Source ID (Study and Year) | Ancestry |
|---|---|---|---|---|---|---|
| Cognitive traits | Cognitive performance | 257,828 | 0.20 | 0.01 | 4067 (Lee et al., 2018) | European |
| Intelligence | 269,867 | 0.20 | 0.01 | 3785 (Savage et al., 2018) | ||
| Fluid intelligence (FI) score | 125,935 | 0.22 | 0.01 | 3413 (Watanabe et al., 2019) | ||
| FI test–FI3: word interpolation | 124,929 | 0.07 | 0.01 | 3402 (Watanabe et al., 2019) | ||
| FI test–FI6: conditional arithmetic | 96,994 | 0.05 | 0.01 | 3404 (Watanabe et al., 2019) | ||
| FI test–FI8: chained arithmetic | 68,065 | 0.07 | 0.01 | 3406 (Watanabe et al., 2019) | ||
| FI test–FI5: family relationship calculation | 99,934 | 0.03 | 0.01 | 3403 (Watanabe et al., 2019) | ||
| Educational attainment | 766,345 | 0.11 | 0.00 | 4066 (Lee et al., 2018) | ||
| Education–Qualifications | 318,526 | 0.11 | 0.00 | 3409 (Watanabe et al., 2019) | ||
| Age completed full-time education | 253,580 | 0.05 | 0.00 | 3203 (Watanabe et al., 2019) | ||
| Alzheimer’s disease (AD) | AD | 455,258 | 0.01 | 0.00 | (Jansen et al., 2019) | |
| Gastrointestinal tract (GIT) disorders | Peptic ulcer disease (PUD) | 456,327 | 0.01 | 0.00 | (Wu et al., 2021) | |
| Gastroesophageal reflux disease (GERD) | 332,601 | 0.07 | 0.00 | (An et al., 2019) | ||
| Gastritis-duodenitis (GD) | 407,065 | 0.02 | 0.00 | Phecode 535 (Lee lab) | ||
| Diverticulosis | 362,094 | 0.04 | 0.00 | Phecode 562 (Lee lab) | ||
| Irritable bowel syndrome (IBS) | 455,321 | 0.01 | 0.00 | (Wu et al., 2021) | ||
| Inflammatory bowel disease (IBD) | 456,327 | 0.01 | 0.00 | (Wu et al., 2021) |
| Locus | Chr | Start | Stop | Phenotype 1 | Phenotype 2 | Parameter | R2 | p |
|---|---|---|---|---|---|---|---|---|
| 1 | 3 | 47588462 | 50387742 | GERD | Educational attainment | −0.87 | 0.76 | 3.14 × 10−9 |
| 3 | 47588462 | 50387742 | GERD | FI-Score | −0.98 | 0.96 | 6.63 × 10−7 | |
| 3 | 47588462 | 50387742 | GERD | Intelligence | −0.83 | 0.69 | 8.72 × 10−7 | |
| 3 | 47588462 | 50387742 | GERD | Educational qualification | −0.76 | 0.58 | 3.68 × 10−6 | |
| 3 | 47588462 | 50387742 | GERD | Cognitive performance | −0.82 | 0.67 | 5.26 × 10−6 | |
| 3 | 47588462 | 50387742 | GERD | Age of fulltime education | −0.95 | 0.91 | 2.69 × 10−5 | |
| 3 | 47588462 | 50387742 | IBD | Educational qualification | 0.85 | 0.72 | 5.81 × 10−8 | |
| 3 | 47588462 | 50387742 | IBD | Cognitive performance | 0.89 | 0.80 | 2.83 × 10−7 | |
| 3 | 47588462 | 50387742 | IBD | Educational attainment | 0.70 | 0.49 | 4.57 × 10−7 | |
| 3 | 47588462 | 50387742 | IBD | Intelligence | 0.75 | 0.56 | 3.45 × 10−6 | |
| 2 | 6 | 27261036 | 28666364 | GERD | Cognitive performance | −0.78 | 0.61 | 4.50 × 10−6 |
| 3 | 6 | 31106494 | 31250556 | Diverticulosis | Age of fulltime education | −1.00 | 1.00 | 2.29 × 10−5 |
| 4 | 6 | 32454578 | 32539567 | IBD | AD | 1.00 | 1.00 | 4.80 × 10−7 |
| 6 | 32454578 | 32539567 | IBD | Educational attainment | 0.77 | 0.59 | 1.14 × 10−5 | |
| 6 | 32454578 | 32539567 | Diverticulosis | Educational qualification | −1.00 | 1.00 | 4.81 × 10−10 | |
| 6 | 32454578 | 32539567 | Diverticulosis | Educational attainment | −1.00 | 1.00 | 5.02 × 10−9 | |
| 6 | 32454578 | 32539567 | Diverticulosis | Age of fulltime education | −1.00 | 1.00 | 1.51 × 10−7 | |
| 6 | 32454578 | 32539567 | Diverticulosis | AD | −0.92 | 0.85 | 8.93 × 10−6 | |
| 5 | 6 | 32539568 | 32586784 | IBD | AD | 0.99 | 0.98 | 1.10 × 10−8 |
| 6 | 6 | 98173004 | 99678876 | GERD | Educational attainment | −0.60 | 0.36 | 1.65 × 10−6 |
| 6 | 98173004 | 99678876 | PUD | Cognitive performance | −0.69 | 0.47 | 5.90 × 10−7 | |
| 6 | 98173004 | 99678876 | PUD | Intelligence | −0.57 | 0.32 | 1.51 × 10−5 | |
| 6 | 98173004 | 99678876 | PUD | FI-Score | −0.64 | 0.41 | 1.91 × 10−5 | |
| 7 | 11 | 112755447 | 113889019 | GERD | Educational attainment | −0.87 | 0.75 | 1.34 × 10−6 |
| 8 | 13 | 58245844 | 59751795 | GERD | Educational attainment | −0.65 | 0.42 | 7.79 × 10−6 |
| 13 | 58245844 | 59751795 | GERD | Cognitive performance | −0.83 | 0.69 | 1.12 × 10−5 | |
| 9 | 14 | 22760701 | 23985936 | GD | Cognitive performance | −0.81 | 0.66 | 1.05 × 10−5 |
| 14 | 22760701 | 23985936 | GD | Age of fulltime education | −1.00 | 1.00 | 4.22 × 10−5 | |
| 10 | 15 | 96864279 | 98025684 | GD | Educational qualification | −0.60 | 0.36 | 3.49 × 10−5 |
| 11 | 16 | 27443062 | 29043177 | IBD | FI Chained arithmetic | −0.77 | 0.59 | 1.30 × 10−7 |
| 12 | 16 | 53393883 | 54866095 | GD | Cognitive performance | −0.72 | 0.51 | 1.23 × 10−5 |
| 16 | 53393883 | 54866095 | GERD | Intelligence | −0.52 | 0.27 | 3.22 × 10−6 | |
| 16 | 53393883 | 54866095 | GERD | Cognitive performance | −0.57 | 0.33 | 7.08 × 10−6 | |
| 13 | 17 | 45883902 | 47516224 | GERD | Cognitive performance | −0.80 | 0.65 | 1.16 × 10−5 |
| 14 | 19 | 45040933 | 45893307 | GERD | AD | −0.40 | 0.16 | 3.78 × 10−5 |
| Phenotype 1 | Phenotype 2 | N. Sig. | CI97.5 = 1 | Percentage |
|---|---|---|---|---|
| GERD | Cognitive performance | 5 | 4 | 80% |
| GERD | Educational attainment | 4 | 2 | 50% |
| GERD | Intelligence | 2 | 1 | 50% |
| IBD | Educational attainment | 2 | 1 | 50% |
| Diverticulosis | Age of fulltime education | 2 | 2 | 100% |
| IBD | AD | 2 | 2 | 100% |
| GD | Cognitive performance | 2 | 2 | 100% |
| GERD | FI-Score | 1 | 1 | 100% |
| GERD | Educational qualification | 1 | 1 | 100% |
| GERD | Age of fulltime education | 1 | 1 | 100% |
| IBD | Educational qualification | 1 | 1 | 100% |
| IBD | Cognitive performance | 1 | 1 | 100% |
| IBD | Intelligence | 1 | 1 | 100% |
| Diverticulosis | Educational qualification | 1 | 1 | 100% |
| Diverticulosis | Educational attainment | 1 | 1 | 100% |
| Diverticulosis | AD | 1 | 1 | 100% |
| PUD | Cognitive performance | 1 | 0 | 0% |
| PUD | Intelligence | 1 | 0 | 0% |
| PUD | FI-Score | 1 | 0 | 0% |
| GD | Age of fulltime education | 1 | 1 | 100% |
| GD | Educational qualification | 1 | 0 | 0% |
| IBD | FI-Chained arithmetic | 1 | 1 | 100% |
| GERD | AD | 1 | 0 | 0% |
| Exposure (nSNPs) | Outcome | MR-PRESSO RESULTS | MR-Egger Intercept | |||||
|---|---|---|---|---|---|---|---|---|
| Global test P | Raw OR | p | Cor-OR | p | Intercept | p | ||
| Cognitive traits (exposure) and PUD (outcome) | ||||||||
| Age of fulltime education (11) | PUD | 0.11 | 0.74 | 2.6 × 10−2 | - | - | 0.035 | 0.13 |
| Educational qualification (103) | PUD | 0.001 | 0.73 | 5.26 × 10−7 | - | - | −0.01 | 0.06 |
| Intelligence (166) | PUD | 0.002 | 0.77 | 7.84 × 10−6 | 0.76 | 1.90 × 10−6 | −0.0042 | 0.43 |
| FI Chained arithmetic (22) * | PUD | 0.0048 | 1.01 | 0.91 | - | - | −0.0035 | 0.8 |
| FI Cond arithmetic (23) * | PUD | 0.26 | 0.9 | 4.2 × 10−2 | - | - | −0.015 | 0.5 |
| FI−famRelatCal (28) | PUD | 0.09 | 0.98 | 0.78 | - | - | −0.0028 | 0.76 |
| Fluid intelligence score (47) | PUD | 0.144 | 0.92 | 2.0 × 10−2 | - | - | −0.0025 | 0.81 |
| FI−Word interpolation (5) | PUD | 0.071 | 0.91 | 0.51 | - | - | 0.1008 | 0.6 |
| Cognitive performance (133) | PUD | 0.0052 | 0.74 | 5.40 × 10−6 | 0.77 | 9.55 × 10−6 | 0.00077 | 0.89 |
| Educational attainment (294) | PUD | <0.001 | 0.56 | 1.90 × 10−18 | 0.55 | 3.85 × 10−19 | −0.0017 | 0.6 |
| PUD (exposure) and cognitive traits (outcome) | ||||||||
| PUD (7) | Age of fulltime education | 0.063 | 1.01 | 0.83 | - | - | −0.0043 | 0.86 |
| PUD (7) | Educational qualification | 2.0 × 10−4 | 0.94 | 0.3 | 0.97 | 0.18 | 0.013 | 0.61 |
| PUD (7) | Intelligence | 0.0098 | 0.99 | 0.83 | 0.99 | 0.8 | 0.0098 | 0.49 |
| PUD (7) | FI Chained arithmetic | 0.22 | 1.05 | 0.59 | - | - | −0.0077 | 0.86 |
| PUD (7) | FI Cond arithmetic | 0.82 | 0.92 | 0.066 | - | - | −0.014 | 0.64 |
| PUD (7) | FI−famRelatCal | 0.41 | 0.99 | 0.76 | - | - | 0.0027 | 0.91 |
| PUD (7) | Fluid intelligence score | 0.0164 | 1.04 | 0.63 | 1.04 | 0.48 | 0.035 | 0.37 |
| PUD (7) | FI−Word interpolation | 0.548 | 1.01 | 0.88 | - | - | 0.0069 | 0.83 |
| PUD (7) | Cognitive performance | 0.0176 | 0.98 | 0.47 | 0.998 | 0.93 | 0.014 | 0.32 |
| PUD (7) | Educational attainment | <2.0 × 10−4 | 0.98 | 0.73 | 0.97 | 0.32 | 0.015 | 0.33 |
| Exposure (nSNPs) | Outcome | MR-PRESSO RESULTS | MR-Egger Intercept | |||||
|---|---|---|---|---|---|---|---|---|
| Global Test P | Raw OR | p | Cor-OR | p | Intercept | p | ||
| Cognitive traits (exposure) and GERD (outcome) | ||||||||
| Age of fulltime education (11) | GERD | 0.26 | 0.76 | 6.24 × 10−4 | - | - | −0.0045 | 0.70 |
| Educational qualification (103) | GERD | <2 × 10−4 | 0.72 | 2.94 × 10−14 | 0.72 | 2.23 × 10−13 | −0.0061 | 0.18 |
| Intelligence (166) | GERD | <2 × 10−4 | 0.75 | 8.67 × 10−12 | 0.76 | 3.75 × 10−11 | 0.0065 | 0.08 |
| FI Chained arithmetic (22) * | GERD | 0.23 | 0.96 | 0.1 | - | - | −0.0052 | 0.35 |
| FI Cond arithmetic (23) * | GERD | 0.041 | 0.99 | 0.65 | - | - | −0.012 | 0.017 |
| FI−famRelatCal (28) | GERD | 0.018 | 0.94 | 7.46 × 10−2 | - | - | −0.0031 | 0.57 |
| Fluid intelligence score (47) | GERD | <2 × 10−4 | 0.88 | 1.53 × 10−5 | 0.87 | 3.43 × 10−7 | 0.016 | 0.04 |
| FI−Word interpolation (5) | GERD | 0.036 | 0.91 | 0.26 | 0.85 | 2.31 × 10−2 | 0.021 | 0.84 |
| Cognitive performance (133) | GERD | <2 × 10−4 | 0.69 | 4.86 × 10−17 | 0.67 | 9.48 × 10−20 | 0.0056 | 0.12 |
| Educational attainment (294) | GERD | <0.001 | 0.54 | 6.94 × 10−34 | 0.53 | 8.56 × 10−45 | −0.0036 | 0.12 |
| GERD (exposure) and cognitive traits (outcome) | ||||||||
| GERD (19) | Age of fulltime education | 2 × 10−4 | 0.83 | 9.89 × 10−3 | 0.80 | 2.77 × 10−3 | −0.02 | 0.26 |
| GERD (19) | Educational qualification | <2 × 10−4 | 0.86 | 3.84 × 10−2 | 0.90 | 1.18 × 10−2 | −0.012 | 0.37 |
| GERD (19) | Intelligence | <2 × 10−4 | 0.89 | 2.51 × 10−3 | 0.91 | 2.29 × 10−3 | −0.01 | 0.22 |
| GERD (19) | FI Chained arithmetic | 0.56 | 0.91 | 0.25 | - | - | −0.026 | 0.22 |
| GERD (19) | FI Cond arithmetic | 0.49 | 0.86 | 0.046 | - | - | −0.027 | 0.13 |
| GERD (19) | FI−famRelatCal | 0.62 | 0.87 | 2.26 × 10−2 | - | - | −0.0095 | 0.52 |
| GERD (19) | Fluid intelligence score | <2 × 10−4 | 0.75 | 7.23 × 10−3 | 0.79 | 1.15 × 10−2 | −0.032 | 0.15 |
| GERD (19) | FI−Word interpolation | 0.19 | 0.73 | 1.70 × 10−3 | - | - | −0.041 | 0.04 |
| GERD (19) | Cognitive performance | <2 × 10−4 | 0.90 | 2.99 × 10−2 | 0.95 | 0.11 | −0.016 | 0.13 |
| GERD (19) | Educational attainment | <2 × 10−4 | 0.87 | 2.53 × 10−3 | 0.88 | 3.05 × 10−4 | −0.0077 | 0.41 |
| Exposure (nSNPs) | Outcome | MR-PRESSO RESULTS | MR-Egger Intercept | |||||
|---|---|---|---|---|---|---|---|---|
| Global Test P | Raw OR | p | Cor-OR | p | Intercept | p | ||
| Cognitive traits (exposure) and IBD (outcome) | ||||||||
| Age of fulltime education (11) | IBD | 2 × 10−4 | 1.33 | 0.30 | 1.06 | 0.73 | −0.019 | 0.72 |
| Educational qualification (103) | IBD | <2 × 10−4 | 1.05 | 0.61 | 0.98 | 0.81 | −0.024 | 0.023 |
| Intelligence (166) | IBD | 4 × 10−4 | 0.94 | 0.46 | 0.96 | 0.61 | −0.0094 | 0.26 |
| FI Chained arithmetic (22) * | IBD | 0.60 | 0.95 | 0.34 | - | - | 0.00088 | 0.94 |
| FI Cond arithmetic (23) * | IBD | 0.66 | 1.03 | 0.60 | - | - | 0.0065 | 0.60 |
| FI−famRelatCal (28) | IBD | 0.23 | 0.99 | 0.89 | - | - | 0.0051 | 0.70 |
| Fluid intelligence score (47) | IBD | 0.006 | 1.06 | 0.36 | 1.02 | 0.70 | 0.0032 | 0.87 |
| FI−Word interpolation (5) | IBD | 0.36 | 1.08 | 0.59 | - | - | 0.30 | 0.13 |
| Cognitive performance (133) | IBD | 4 × 10−4 | 0.88 | 0.20 | 0.87 | 0.11 | 0.0053 | 0.55 |
| Educational attainment (294) | IBD | 0.0018 | 0.90 | 0.25 | 0.85 | 0.067 | −0.0051 | 0.32 |
| IBD (exposure) and cognitive traits (outcome) | ||||||||
| IBD (25) | Age of fulltime education | 0.091 | 0.99 | 0.43 | - | - | −0.00060 | 0.90 |
| IBD (25) | Educational qualification | 0.0046 | 1.00 | 0.60 | 0.99 | 0.23 | 0.0014 | 0.68 |
| IBD (25) | Intelligence | 0.006 | 1.00 | 0.94 | 1.00 | 0.61 | 0.00086 | 0.73 |
| IBD (25) | FI Chained arithmetic | 0.077 | 1.03 | 0.31 | - | - | −0.0066 | 0.51 |
| IBD (25) | FI Cond arithmetic | 0.178 | 1.00 | 0.97 | - | - | 0.0073 | 0.34 |
| IBD (25) | FI−famRelatCal | 0.027 | 1.01 | 0.48 | - | - | 0.0071 | 0.35 |
| IBD (25) | Fluid intelligence score | 0.0012 | 0.99 | 0.72 | - | - | 0.0055 | 0.45 |
| IBD (25) | FI−Word interpolation | 0.24 | 0.98 | 0.43 | - | - | 0.0013 | 0.85 |
| IBD (25) | Cognitive performance | 2 × 10−4 | 1.00 | 0.94 | 1.00 | 0.70 | 5.0 × 10−5 | 0.99 |
| IBD (25) | Educational attainment | 0.0228 | 0.99 | 0.15 | 0.99 | 1.29 × 10−2 | 0.00068 | 0.63 |
| Discovery Set | Target Set | No. of Genes Overlapping the Discovery and the Target Sets at pgene < 0.05 | Proportion of Gene Overlap | Binomial Test | |||||
|---|---|---|---|---|---|---|---|---|---|
| PUD, GERD, IBD or AD | Total no. of Discovery Set (PUD, GERD, IBD or AD) Genes | No. of Discovery Set Genes at pgene < 0.05 | Cognitive Traits | Total No. of Target set (Cognitive Traits) Genes | No. of Target Set Genes at pgene < 0.05 | Expected | Observed | p Value | |
| PUD | 18,650 | 1511 | Educational attainment | 18,650 | 6761 | 625 | 0.081 | 0.092 | 3.85 × 10−4 * |
| Cognitive performance | 18,650 | 5273 | 489 | 0.081 | 0.093 | 1.18 × 10−3 | |||
| GERD | 18,729 | 3290 | Educational attainment | 18,729 | 6832 | 1752 | 0.176 | 0.255 | 2.20 × 10−16 |
| Cognitive performance | 18,729 | 5285 | 1336 | 0.176 | 0.253 | 2.20 × 10−16 | |||
| IBD | 18,650 | 1920 | Educational attainment | 18,650 | 6761 | 811 | 0.103 | 0.20 | 3.95 × 10−6 |
| Cognitive performance | 18,650 | 5273 | 636 | 0.103 | 0.121 | 2.13 × 10−5 | |||
| AD | 18,865 | 1813 | Educational attainment | 18,865 | 6720 | 753 | 0.096 | 0.112 | 7.79 × 10−6 |
| Cognitive performance | 18,865 | 5212 | 591 | 0.096 | 0.113 | 1.94 × 10−5 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adewuyi, E.O.; O’Brien, E.K.; Porter, T.; Laws, S.M. Relationship of Cognition and Alzheimer’s Disease with Gastrointestinal Tract Disorders: A Large-Scale Genetic Overlap and Mendelian Randomisation Analysis. Int. J. Mol. Sci. 2022, 23, 16199. https://doi.org/10.3390/ijms232416199
Adewuyi EO, O’Brien EK, Porter T, Laws SM. Relationship of Cognition and Alzheimer’s Disease with Gastrointestinal Tract Disorders: A Large-Scale Genetic Overlap and Mendelian Randomisation Analysis. International Journal of Molecular Sciences. 2022; 23(24):16199. https://doi.org/10.3390/ijms232416199
Chicago/Turabian StyleAdewuyi, Emmanuel O., Eleanor K. O’Brien, Tenielle Porter, and Simon M. Laws. 2022. "Relationship of Cognition and Alzheimer’s Disease with Gastrointestinal Tract Disorders: A Large-Scale Genetic Overlap and Mendelian Randomisation Analysis" International Journal of Molecular Sciences 23, no. 24: 16199. https://doi.org/10.3390/ijms232416199
APA StyleAdewuyi, E. O., O’Brien, E. K., Porter, T., & Laws, S. M. (2022). Relationship of Cognition and Alzheimer’s Disease with Gastrointestinal Tract Disorders: A Large-Scale Genetic Overlap and Mendelian Randomisation Analysis. International Journal of Molecular Sciences, 23(24), 16199. https://doi.org/10.3390/ijms232416199