


Close Relationship between Systemic Arterial and Portal Venous Pressure in an Animal Model with Healthy Liver
 , and
, and
Abstract
:1. Introduction
2. Results
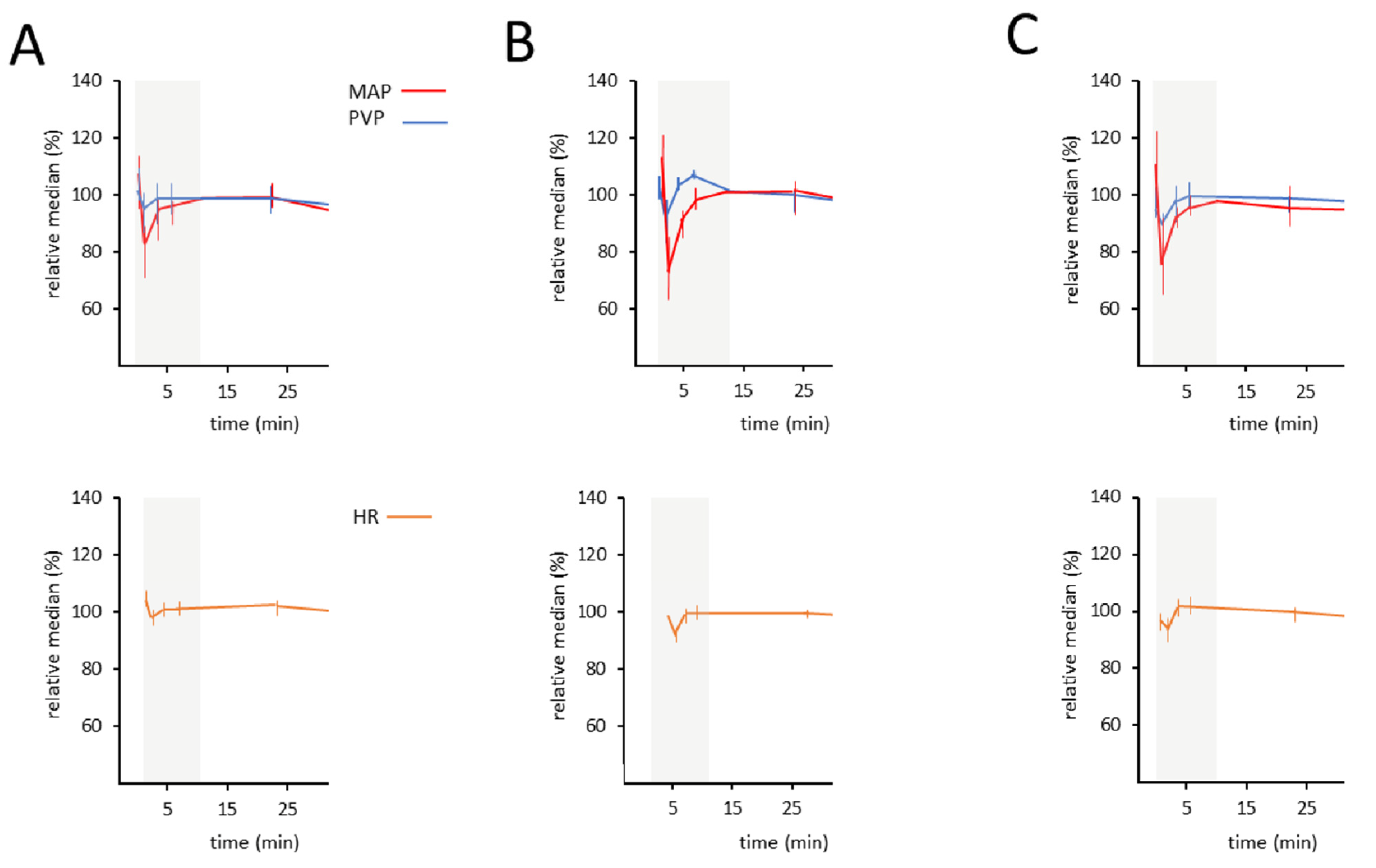
2.1. Time-Dependent Course of MAP and PVP in Three Groups of Healthy Rats
2.2. Correlation between MAP and PVP
2.3. Evaluation of Time Interval 10–30 min (Excluding the “Dip”)
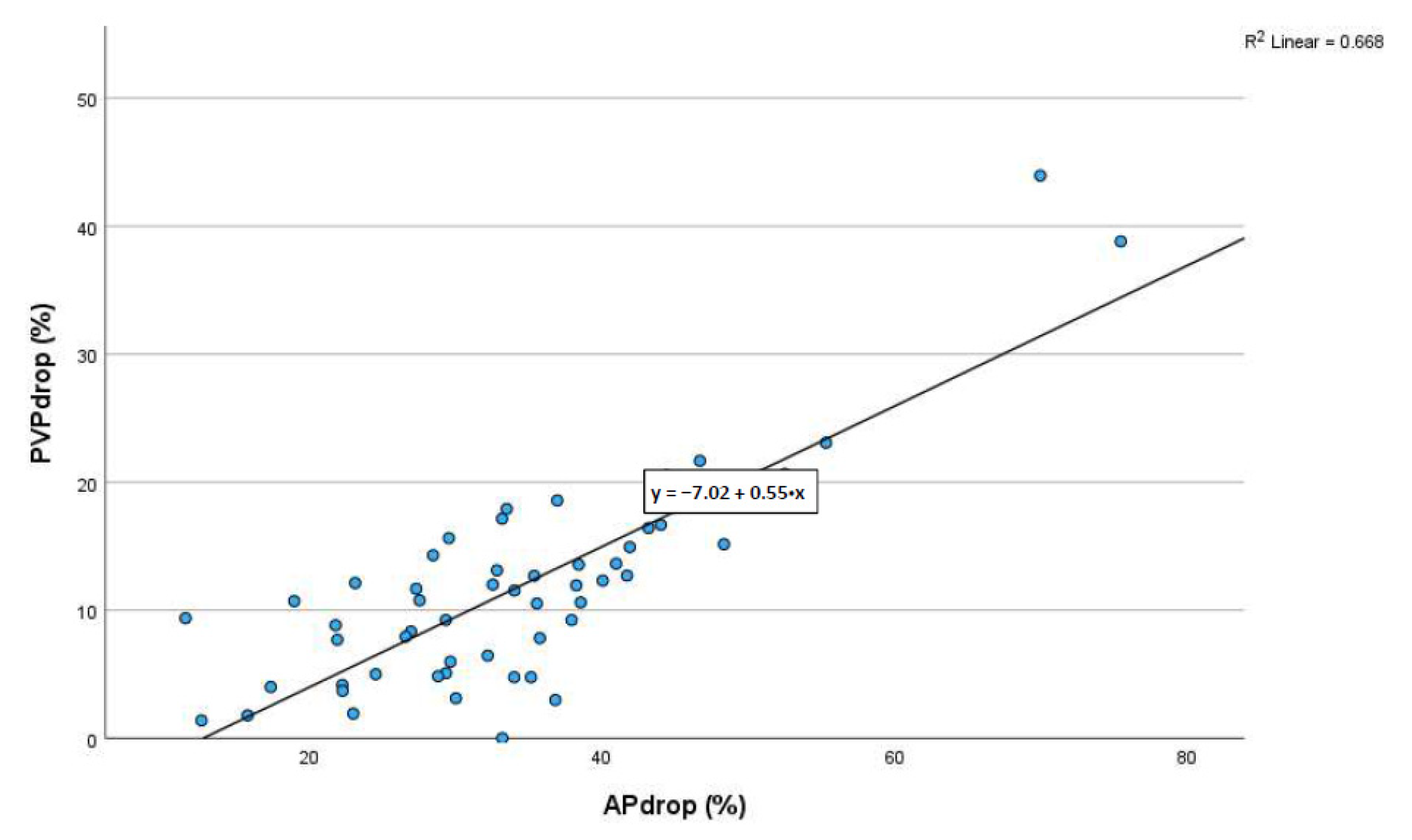
2.4. Correlation between the Maximum Dip in MAP and the Maximum Dip in PVP during the First 10 min
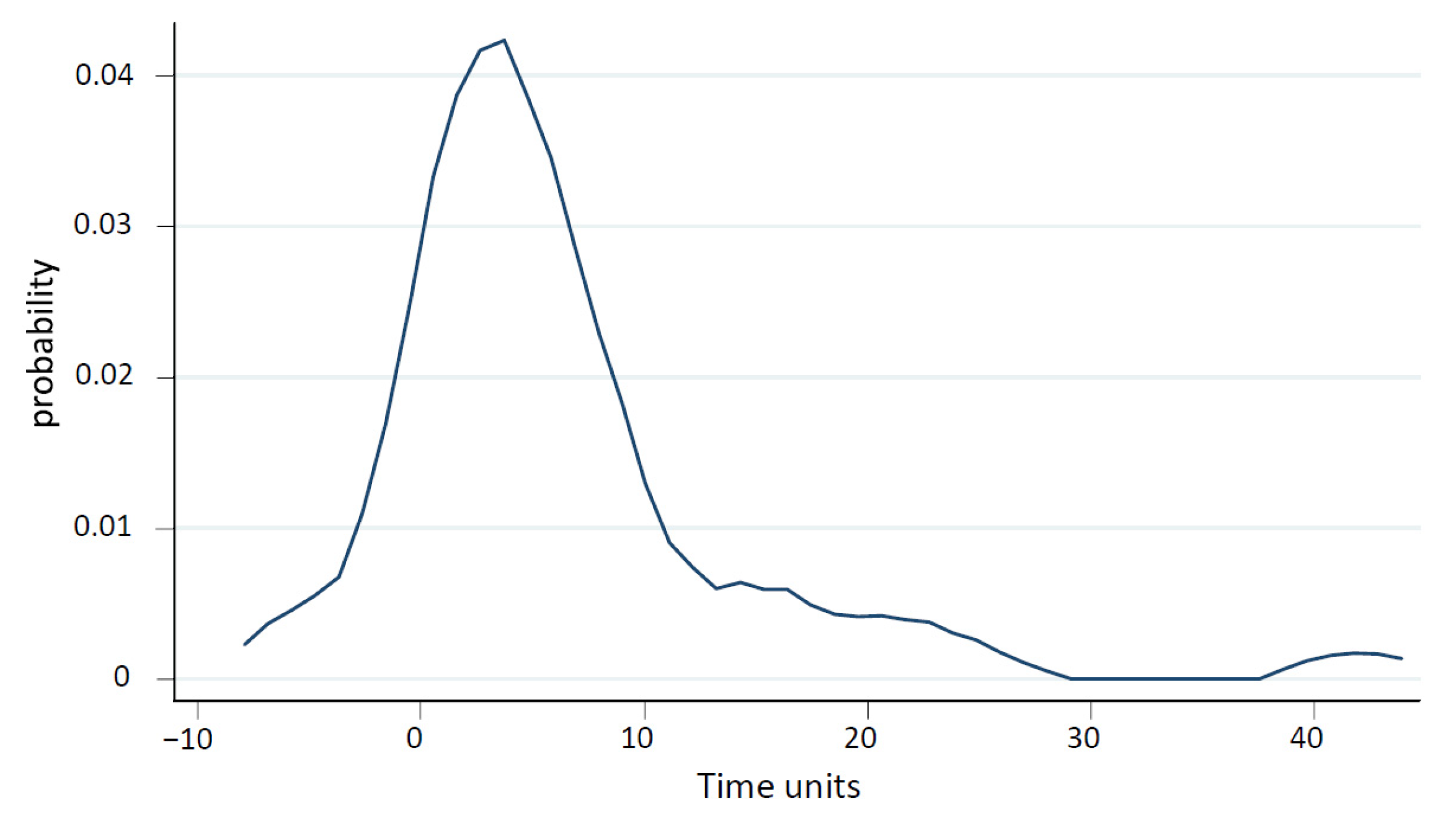
2.5. Quantifying the Time Lag between Pressure Change in MAP and PVP during the First 10 min
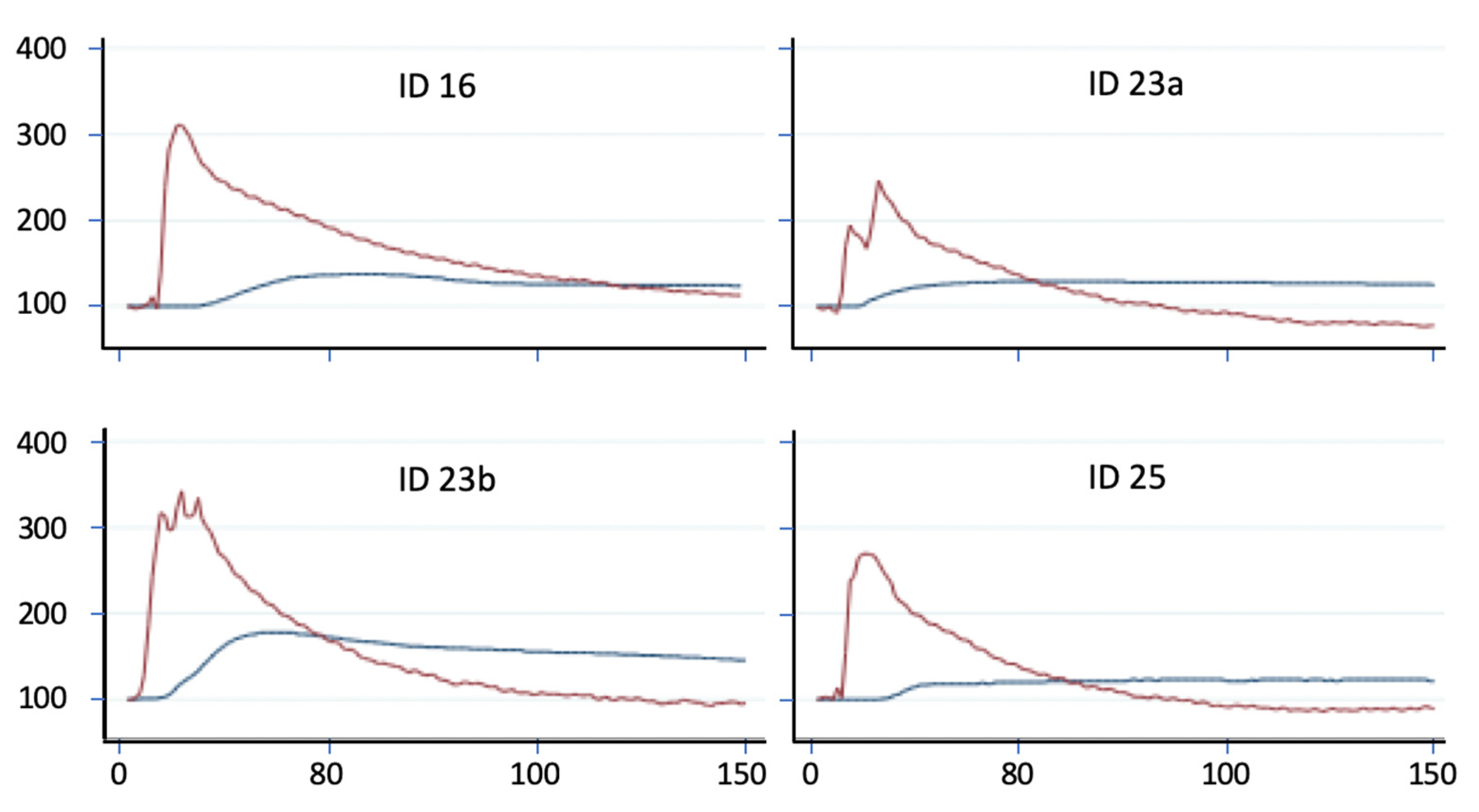
2.6. Elevation of MAP and Its Effect on PVP
3. Discussion
- There is high correlation between the maximal drop in MAP and the maximal drop in PVP. This further suggests a close relationship between the two circulatory systems;
- There is a distinct time lag between the lowest drop in MAP and the lowest drop in PVP. It totals up to 24 s as calculated for all groups (p = 0.0001). The difference among the groups is not statistically significant. These data imply a cause-and-effect relation between the drop in MAP and drop in PVP.
4. Materials and Methods
4.1. Animal Preparation and Ethics Statement
4.2. Experimental Protocol
4.3. Data Processing and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PDE-5 | Phosphodiesterase-5 |
| PDE-5-I | Phosphodiesterase-5 inhibitor |
| NO | Nitric oxide |
| cGMP | Cyclic guanosine monophosphate |
| ISMN | Isosorbid monohydrate |
| ISDN | Isosorbid dinitrate |
| MAP | Mean arterial pressure |
| PVP | Portal venous pressure |
| PH | Portal hypertension |
| ACE inhibitors | Angiotensin-converting enzyme inhibitors |
| AT-1 receptors | Angiotensin-1 receptors |
| HVPG | Hepato-venous pressure gradient |
References
- Turco, L.; Garcia-Tsao, G. Portal Hypertension: Pathogenesis and Diagnosis. Clin. Liver Dis. 2019, 23, 573–587. [Google Scholar] [CrossRef]
- Berzigotti, A.; Seijo, S.; Reverter, E.; Bosch, J. Assessing portal hypertension in liver diseases. Expert. Rev. Gastroenterol. Hepatol. 2013, 7, 141–155. [Google Scholar] [CrossRef]
- Bosch, J.; Pizcueta, P.; Feu, F.; Fernández, M.; García-Pagán, J.C. Pathophysiology of portal hypertension. Gastroenterol. Clin. N. Am. 1992, 21, 1–14. [Google Scholar] [CrossRef]
- Bosch, J.; Abraldes, J.G.; Berzigotti, A.; García-Pagan, J.C. The clinical use of HVPG measurements in chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 573–582. [Google Scholar] [CrossRef]
- Bosch, J. Vascular deterioration in cirrhosis: The big picture. J. Clin. Gastroenterol. 2007, 41, S247–S253. [Google Scholar] [CrossRef]
- Jakab, S.S.; Garcia-Tsao, G. Evaluation and Management of Esophageal and Gastric Varices in Patients with Cirrhosis. Clin. Liver Dis. 2020, 24, 335–350. [Google Scholar] [CrossRef]
- De Franchis, R.; Dell’Era, A.; Primignani, M. Diagnosis and monitoring of portal hypertension. Dig. Liver Dis. 2008, 40, 312–317. [Google Scholar] [CrossRef] [PubMed]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, S.M.; Waldman, B. The Circulatory System in Liver Disease. Crit. Care Clin. 2016, 32, 331–342. [Google Scholar] [CrossRef]
- García-Pagán, J.-C.; Gracia-Sancho, J.; Bosch, J. Functional aspects on the pathophysiology of portal hypertension in cirrhosis. J. Hepatol. 2012, 57, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Greuter, T.; Shah, V.H. Hepatic sinusoids in liver injury, inflammation, and fibrosis: New pathophysiological insights. J. Gastroenterol. 2016, 51, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, M. Molecular pathophysiology of portal hypertension. Hepatology 2015, 61, 1406–1415. [Google Scholar] [CrossRef]
- Bosch, J.; Groszmann, R.J.; Shah, V.H. Evolution in the understanding of the pathophysiological basis of portal hypertension: How changes in paradigm are leading to successful new treatments. J. Hepatol. 2015, 62, S121–S130. [Google Scholar] [CrossRef] [Green Version]
- Gracia-Sancho, J.; Maeso-Díaz, R.; Bosch, J. Pathophysiology and a Rational Basis of Therapy. Dig. Dis. 2015, 33, 508–514. [Google Scholar] [CrossRef]
- Iwakiri, Y. Pathophysiology of portal hypertension. Clin. Liver Dis. 2014, 18, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Iwakiri, Y.; Shah, V.; Rockey, D.C. Vascular pathobiology in chronic liver disease and cirrhosis—Current status and future directions. J. Hepatol. 2014, 61, 912–924. [Google Scholar] [CrossRef] [Green Version]
- Bosch, J.; Iwakiri, Y. The portal hypertension syndrome: Etiology, classification, relevance, and animal models. Hepatol. Int. 2018, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Thabut, D.; Shah, V. Intrahepatic angiogenesis and sinusoidal remodeling in chronic liver disease: New targets for the treatment of portal hypertension? J. Hepatol. 2010, 53, 976–980. [Google Scholar] [CrossRef] [Green Version]
- Vallance, P.; Moncada, S. Hyperdynamic circulation in cirrhosis: A role for nitric oxide? Lancet 1991, 337, 776–778. [Google Scholar] [CrossRef] [PubMed]
- Møller, S.; Bendtsen, F. The pathophysiology of arterial vasodilatation and hyperdynamic circulation in cirrhosis. Liver Int. 2018, 38, 570–580. [Google Scholar] [CrossRef] [Green Version]
- Bolognesi, M.; Di Pascoli, M.; Verardo, A.; Gatta, A. Splanchnic vasodilation and hyperdynamic circulatory syndrome in cirrhosis. World J. Gastroenterol. 2014, 20, 2555–2563. [Google Scholar] [CrossRef]
- Hennenberg, M.; Trebicka, J.; Sauerbruch, T.; Heller, J. Mechanisms of extrahepatic vasodilation in portal hypertension. Gut 2008, 57, 1300–1314. [Google Scholar] [CrossRef]
- Iwakiri, Y.; Groszmann, R.J. The hyperdynamic circulation of chronic liver diseases: From the patient to the molecule. Hepatology 2006, 43, S121–S131. [Google Scholar] [CrossRef]
- Iwakiri, Y.; Kim, M.Y. Nitric oxide in liver diseases. Trends Pharmacol. Sci. 2015, 36, 524–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwakiri, Y.; Trebicka, J. Portal hypertension in cirrhosis: Pathophysiological mechanisms and therapy. JHEP Rep. 2021, 3, 100316. [Google Scholar] [CrossRef]
- Kreisel, W.; Lazaro, A.; Trebicka, J.; Perdekamp, M.G.; Schmitt-Graeff, A.; Deibert, P. Cyclic GMP in Liver Cirrhosis—Role in Pathophysiology of Portal Hypertension and Therapeutic Implications. Int. J. Mol. Sci. 2021, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Pascal, J.P.; Cales, P. Propranolol in the prevention of first upper gastrointestinal tract hemorrhage in patients with cirrhosis of the liver and esophageal varices. N. Engl. J. Med. 1987, 317, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Abraldes, J.G.; Garcia-Tsao, G. The Design of Clinical Trials in Portal Hypertension. Semin. Liver Dis. 2017, 37, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.G.; Mendoza, Y.P.; Bosch, J. Beta-blockers in cirrhosis: Evidence-based indications and limitations. JHEP Rep. 2020, 2, 100063. [Google Scholar] [CrossRef] [Green Version]
- Baiges, A.; Hernández-Gea, V.; Bosch, J. Pharmacologic prevention of variceal bleeding and rebleeding. Hepatol. Int. 2018, 12, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Deibert, P.; Schumacher, Y.-O.; Ruecker, G.; Opitz, O.G.; Blum, H.E.; Rössle, M.; Kreisel, W. Effect of vardenafil, an inhibitor of phosphodiesterase-5, on portal haemodynamics in normal and cirrhotic liver—Results of a pilot study. Aliment. Pharmacol. Ther. 2006, 23, 121–128. [Google Scholar] [CrossRef]
- Schaffner, D.; Lazaro, A.; Deibert, P.; Hasselblatt, P.; Stoll, P.; Fauth, L.; Baumstark, M.W.; Merfort, I.; Schmitt-Graeff, A.; Kreisel, W. Analysis of the nitric oxide-cyclic guanosine monophosphate pathway in experimental liver cirrhosis suggests phosphodiesterase-5 as potential target to treat portal hypertension. World J. Gastroenterol. 2018, 24, 4356–4368. [Google Scholar] [CrossRef] [PubMed]
- Kreisel, W.; Deibert, P.; Kupcinskas, L.; Sumskiene, J.; Appenrodt, B.; Roth, S.; Neagu, M.; Rössle, M.; Zipprich, A.; Caca, K.; et al. The phosphodiesterase-5-inhibitor udenafil lowers portal pressure in compensated preascitic liver cirrhosis. A dose-finding phase-II-study. Dig. Liver Dis. 2015, 47, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Kreisel, W.; Schaffner, D.; Lazaro, A.; Trebicka, J.; Merfort, I.; Schmitt-Graeff, A.; Deibert, P. Phosphodiesterases in the Liver as Potential Therapeutic Targets of Cirrhotic Portal Hypertension. Int. J. Mol. Sci. 2020, 21, 6223. [Google Scholar] [CrossRef]
- Sauerbruch, T.; Trebicka, J. Future therapy of portal hypertension in liver cirrhosis—A guess. F1000Prime Rep. 2014, 6, 95. [Google Scholar] [CrossRef] [Green Version]
- Sauerbruch, T.; Schierwagen, R.; Trebicka, J. Managing portal hypertension in patients with liver cirrhosis. F1000Research 2018, 7, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Berzigotti, A.; Bosch, J. Pharmacologic management of portal hypertension. Clin. Liver Dis. 2014, 18, 303–317. [Google Scholar] [CrossRef]
- Brusilovskaya, K.; Königshofer, P.; Schwabl, P.; Reiberger, T. Vascular Targets for the Treatment of Portal Hypertension. Semin. Liver Dis. 2019, 39, 483–501. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Trebicka, J.; Chalasani, N.; D’Amico, G.; Rockey, D.C.; Shah, V.H.; Bosch, J.; Garcia-Tsao, G. Prioritization of Therapeutic Targets and Trial Design in Cirrhotic Portal Hypertension. Hepatology 2019, 69, 1287–1299. [Google Scholar] [CrossRef] [Green Version]
- Garbuzenko, D.V. Contemporary concepts of the medical therapy of portal hypertension under liver cirrhosis. World J. Gastroenterol. 2015, 21, 6117–6126. [Google Scholar] [CrossRef] [PubMed]
- Garbuzenko, D.V.; Arefyev, N.O.; Kazachkov, E.L. Antiangiogenic therapy for portal hypertension in liver cirrhosis: Current progress and perspectives. World J. Gastroenterol. 2018, 24, 3738–3748. [Google Scholar] [CrossRef]
- Kravetz, D.; Bosch, J.; Arderiu, M.; Pilar Pizcueta, M.; Rodés, J. Hemodynamic effects of blood volume restitution following a hemorrhage in rats with portal hypertension due to cirrhosis of the liver: Influence of the extent of portal-systemic shunting. Hepatology 1989, 9, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, B. Effects of blood volume restitution following a portal hypertensive–related bleeding in anesthetized cirrhotic rats. Hepatology 2001, 33, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Halverscheid, L.; Deibert, P.; Schmidt, R.; Blum, H.E.; Dunkern, T.; Pannen, B.H.; Kreisel, W. Phosphodiesterase-5 inhibitors have distinct effects on the hemodynamics of the liver. BMC Gastroenterol. 2009, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, J.O.; Gladwin, M.T.; Weitzberg, E. Strategies to increase nitric oxide signalling in cardiovascular disease. Nat. Rev. Drug Discov. 2015, 14, 623–641. [Google Scholar] [CrossRef]
- Murad, F. Nitric Oxide and Cyclic GMP in Cell Signaling and Drug Development. N. Engl. J. Med. 2006, 355, 2003–2011. [Google Scholar] [CrossRef]
- Boyer, J.L.; Chatterjee, C.; Iber, F.L.; Basu, A.K. Effect of Plasma-Volume Expansion on Portal Hypertension. N. Engl. J. Med. 1966, 275, 750–755. [Google Scholar] [CrossRef]
- Van Limmen, J.; Wyffels, P.; Berrevoet, F.; Vanlander, A.; Coeman, L.; Wouters, P.; De Hert, S.; De Baerdemaeker, L. Effects of propofol and sevoflurane on hepatic blood flow: A randomized controlled trial. BMC Anesthesiol. 2020, 20, 241. [Google Scholar] [CrossRef]
- Ge, P.S.; Runyon, B.A. The changing role of beta-blocker therapy in patients with cirrhosis. J. Hepatol. 2014, 60, 643–653. [Google Scholar] [CrossRef] [Green Version]
- Idéo, G.; Bellati, G.; Fesce, E.; Grimoldi, D. Nadolol can prevent the first gastrointestinal bleeding in cirrhotics: A prospective, randomized study. Hepatology 1988, 8, 6–9. [Google Scholar] [CrossRef]
- Lebrec, D.; Poynard, T.; Capron, J.P.; Hillon, P.; Geoffroy, P.; Roulot, D.; Chaput, J.C.; Rueff, B.; Benhamou, J.P. Nadolol for prophylaxis of gastrointestinal bleeding in patients with cirrhosis. A randomized trial. J. Hepatol. 1988, 7, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Lebrec, D.; Poynard, T.; Hillon, P.; Benhamou, J.P. Propranolol for prevention of recurrent gastrointestinal bleeding in patients with cirrhosis: A controlled study. N. Engl. J. Med. 1981, 305, 1371–1374. [Google Scholar] [CrossRef] [PubMed]
- Westaby, D.; Melia, W.M.; Macdougall, B.R.; Hegarty, J.E.; Gimson, A.E.; Williams, R. B1 selective adrenoreceptor blockade for the long term management of variceal bleeding. A prospective randomised trial to compare oral metoprolol with injection sclerotherapy in cirrhosis. Gut 1985, 26, 421–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westaby, D.; Bihari, D.J.; Gimson, A.E.; Crossley, I.R.; Williams, R. Selective and non-selective beta receptor blockade in the reduction of portal pressure in patients with cirrhosis and portal hypertension. Gut 1984, 25, 121–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripathi, D.; Hayes, P.C. Beta-blockers in portal hypertension: New developments and controversies. Liver Int. 2014, 34, 655–667. [Google Scholar] [CrossRef]
- Bosch, J. Carvedilol: The β-blocker of choice for portal hypertension? Gut 2013, 62, 1529–1530. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, T.Y.; Sohn, J.H.; Um, S.H.; Seo, Y.S.; Baik, S.K.; Kim, M.Y.; Jang, J.Y.; Jeong, S.W.; Lee, B.; et al. A Randomized, Multi-Center, Open-Label Study to Evaluate the Efficacy of Carvedilol vs. Propranolol to Reduce Portal Pressure in Patients with Liver Cirrhosis. Am. J. Gastroenterol. 2016, 111, 1582–1590. [Google Scholar] [CrossRef]
- Reiberger, T.; Ulbrich, G.; Ferlitsch, A.; Payer, B.A.; Schwabl, P.; Pinter, M.; Heinisch, B.B.; Trauner, M.; Kramer, L.; Peck-Radosavljevic, M. Vienna Hepatic Hemodynamic Lab. Carvedilol for primary prophylaxis of variceal bleeding in cirrhotic patients with haemodynamic non-response to propranolol. Gut 2013, 62, 1634–1641. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, G.; Malizia, G.; Bosch, J. Beta-blockers in 2016: Still the safest and most useful drugs for portal hypertension? Hepatology 2016, 63, 1771–1773. [Google Scholar] [CrossRef] [Green Version]
- Krag, A.; Wiest, R.; Albillos, A.; Gluud, L.L. The window hypothesis: Haemodynamic and non-haemodynamic effects of β-blockers improve survival of patients with cirrhosis during a window in the disease. Gut 2012, 61, 967–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albillos, A.; Lledó, J.L.; Bañares, R.; Rossi, I.; Iborra, J.; Calleja, J.L.; Garrido, A.; Escartin, P.; Bosch, J. Hemodynamic effects of alpha-adrenergic blockade with prazosin in cirrhotic patients with portal hypertension. Hepatology 1994, 20, 611–617. [Google Scholar] [PubMed]
- Albillos, A.; Lledó, J.L.; Rossi, I.; Pérez-Páramo, M.; Tabuenca, M.J.; Bañares, R.; Iborra, J.; Garrido, A.; Escartín, P.; Bosch, J. Continuous prazosin administration in cirrhotic patients: Effects on portal hemodynamics and on liver and renal function. Gastroenterology 1995, 109, 1257–1265. [Google Scholar] [CrossRef]
- Blei, A.T.; Garcia-Tsao, G.; Groszmann, R.J.; Kahrilas, P.; Ganger, D.; Morse, S.; Fung, H.L. Hemodynamic evaluation of isosorbide dinitrate in alcoholic cirrhosis. Pharmacokinetic-hemodynamic interactions. Gastroenterology 1987, 93, 576–583. [Google Scholar] [CrossRef]
- Navasa, M.; Chesta, J.; Bosch, J.; Rodés, J. Reduction of portal pressure by isosorbide-5-mononitrate in patients with cirrhosis: Effects on splanchnic and systemic hemodynamics and liver function. Gastroenterology 1989, 96, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, D.; Therapondos, G.; Lui, H.F.; Johnston, N.; Webb, D.J.; Hayes, P.C. Chronic administration of losartan, an angiotensin II receptor antagonist, is not effective in reducing portal pressure in patients with preascitic cirrhosis. Am. J. Gastroenterol. 2004, 99, 390–394. [Google Scholar] [CrossRef]
- Tandon, P.; Abraldes, J.G.; Berzigotti, A.; Garcia-Pagan, J.C.; Bosch, J. Renin–angiotensin–aldosterone inhibitors in the reduction of portal pressure: A systematic review and meta-analysis. J. Hepatol. 2010, 53, 273–282. [Google Scholar] [CrossRef]
- Agasti, A.K.; Mahajan, A.U.; Phadke, A.Y.; Nathani, P.J.; Sawant, P. Comparative randomized study on efficacy of losartan versus propranolol in lowering portal pressure in decompensated chronic liver disease. J. Dig. Dis. 2013, 14, 266–271. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Rodríguez-Vilarrupla, A.; Graupera, M.; Zafra, C.; García-Calderó, H.; García-Pagán, J.C.; Bosch, J. Simvastatin treatment improves liver sinusoidal endothelial dysfunction in CCl4 cirrhotic rats. J. Hepatol. 2007, 46, 1040–1046. [Google Scholar] [CrossRef]
- Bosch, J.; Abraldes, J.G.; Fernández, M.; García-Pagán, J.C. Hepatic endothelial dysfunction and abnormal angiogenesis: New targets in the treatment of portal hypertension. J. Hepatol. 2010, 53, 558–567. [Google Scholar] [CrossRef] [Green Version]
- Ramírez, G.; Briceño, J.; Rojas, A. Statins and portal hypertension: A new pharmacological challenge. Curr. Vasc. Pharmacol. 2012, 10, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Hennenberg, M.; Laleman, W.; Shelest, N.; Biecker, E.; Schepke, M.; Nevens, F.; Sauerbruch, T.; Heller, J. Atorvastatin lowers portal pressure in cirrhotic rats by inhibition of RhoA/Rho-kinase and activation of endothelial nitric oxide synthase. Hepatology 2007, 46, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Pollo-Flores, P.; Soldan, M.; Santos, U.C.; Kunz, D.G.; Mattos, D.E.; da Silva, A.C.; Marchiori, R.C.; da Rezende, G.F.M. Three months of simvastatin therapy vs. placebo for severe portal hypertension in cirrhosis: A randomized controlled trial. Dig. Liver Dis. 2015, 47, 957–963. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Villanueva, C.; Aracil, C.; Turnes, J.; Hernandez-Guerra, M.; Genesca, J.; Rodriguez, M.; Castellote, J.; García-Pagán, J.C.; Torres, F.; et al. BLEPS Study Group. Addition of Simvastatin to Standard Therapy for the Prevention of Variceal Rebleeding Does Not Reduce Rebleeding but Increases Survival in Patients with Cirrhosis. Gastroenterology 2016, 150, 1160–1170.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colle, I.; De Vriese, A.S.; Van Vlierberghe, H.; Lameire, N.H.; DeVos, M. Systemic and splanchnic haemodynamic effects of sildenafil in an in vivo animal model of cirrhosis support for a risk in cirrhotic patients. Liver Int. 2004, 24, 63–68. [Google Scholar] [CrossRef]
- Tandon, P.; Inayat, I.; Tal, M.; Spector, M.; Shea, M.; Groszmann, R.J.; Garcia-Tsao, G. Sildenafil has no effect on portal pressure but lowers arterial pressure in patients with compensated cirrhosis. Clin. Gastroenterol. Hepatol. 2010, 8, 546–549. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.-C.; Yang, Y.-Y.; Huang, Y.-T.; Lee, F.-Y.; Hou, M.-C.; Lin, H.-C.; Lee, S.-D. Administration of a low dose of sildenafil for 1 week decreases intrahepatic resistance in rats with biliary cirrhosis: The role of NO bioavailability. Clin. Sci. 2010, 119, 45–55. [Google Scholar] [CrossRef]
- Uschner, F.E.; Glückert, K.; Klein, S.; Magdaleno, F.; Schierwagen, R.; Trebicka, J. FRI-247—Udenafil decreases portal pressure and improves erectile dysfunction in liver cirrhosis. J. Hepatol. 2018, 68, S471. [Google Scholar] [CrossRef]
- Uschner, F.E.; Glückert, K.; Paternostro, R.; Gnad, T.; Schierwagen, R.; Mandorfer, M.; Magdaleno, F.; Ortiz, C.; Schwarzkopf, K.; Kamath, P.; et al. Combination of phosphodiesterase-5-inhibitors and beta blockers improves experimental portal hypertension and erectile dysfunction. Liver Int. 2020, 40, 2228–2241. [Google Scholar] [CrossRef]



 PVPmean,
PVPmean,  MAPmean.
PVPmean, MAPmean.
MAPmean.
PVPmean, MAPmean.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group One NaCl 0.9% n = 15 | Group Two Sildenafil (0.1 mg/kg) n = 18 | Group Three Sildenafil (1 mg/kg) n = 18 | |
|---|---|---|---|
| Weight (g) | 375.25 ± 14.60 | 371.55 ± 20.42 | 377.72 ± 18.99 |
| MAP mean (mmHg) | 85.55 ± 13.79 | 87.20 ± 15.02 | 79.69 ± 13.75 |
| PVP mean (mmHg) | 6.42 ± 0.59 | 6.59 ± 0.55 | 6.26 ± 0.63 |
| Evaluation Time Interval 10–30 min | |
|---|---|
| Observed time | 10 min–30 min |
| Group one (NaCl 0.9%) | 0.485 **, † [0.464, 0.505] |
| Group two (sildenafil 0.1 mg/kg) | 0.550 ***, † [0.541, 0.560] |
| Group three (sildenafil 1 mg/kg) | 0.651 ***, † [0.632, 0.670] |
| Group | n | Mean MAP Drop (%) | Mean PVP Drop (%) |
|---|---|---|---|
| Total | 51 | 35.0 (31.6, 38,3) | 11.8 (9.4, 14.1) |
| Group one (NaCl) | 15 | 28.6 † (23.3, 34.0) | 10.0 (6.6, 13.4) |
| Group two (sildenafil 0.1 mg/kg) | 18 | 39.3 † (33.1, 45.5) | 14.1 (9.8, 18.3) |
| Group three (sildenafil 1 mg/kg) | 18 | 35.8 (30.2, 41.5) | 11.1 (6.2, 16.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazaro, A.; Stoll, P.; von Elverfeldt, D.; Kreisel, W.; Deibert, P. Close Relationship between Systemic Arterial and Portal Venous Pressure in an Animal Model with Healthy Liver. Int. J. Mol. Sci. 2023, 24, 9963. https://doi.org/10.3390/ijms24129963
Lazaro A, Stoll P, von Elverfeldt D, Kreisel W, Deibert P. Close Relationship between Systemic Arterial and Portal Venous Pressure in an Animal Model with Healthy Liver. International Journal of Molecular Sciences. 2023; 24(12):9963. https://doi.org/10.3390/ijms24129963
Chicago/Turabian StyleLazaro, Adhara, Patrick Stoll, Dominik von Elverfeldt, Wolfgang Kreisel, and Peter Deibert. 2023. "Close Relationship between Systemic Arterial and Portal Venous Pressure in an Animal Model with Healthy Liver" International Journal of Molecular Sciences 24, no. 12: 9963. https://doi.org/10.3390/ijms24129963
APA StyleLazaro, A., Stoll, P., von Elverfeldt, D., Kreisel, W., & Deibert, P. (2023). Close Relationship between Systemic Arterial and Portal Venous Pressure in an Animal Model with Healthy Liver. International Journal of Molecular Sciences, 24(12), 9963. https://doi.org/10.3390/ijms24129963